
Osteoid Osteoma, a Diagnostic Problem: A Series of Atypical and Mimicking Presentations and Review of the Recent Literature

Abstract
:1. Introduction
2. Materials and Methods
3. Results
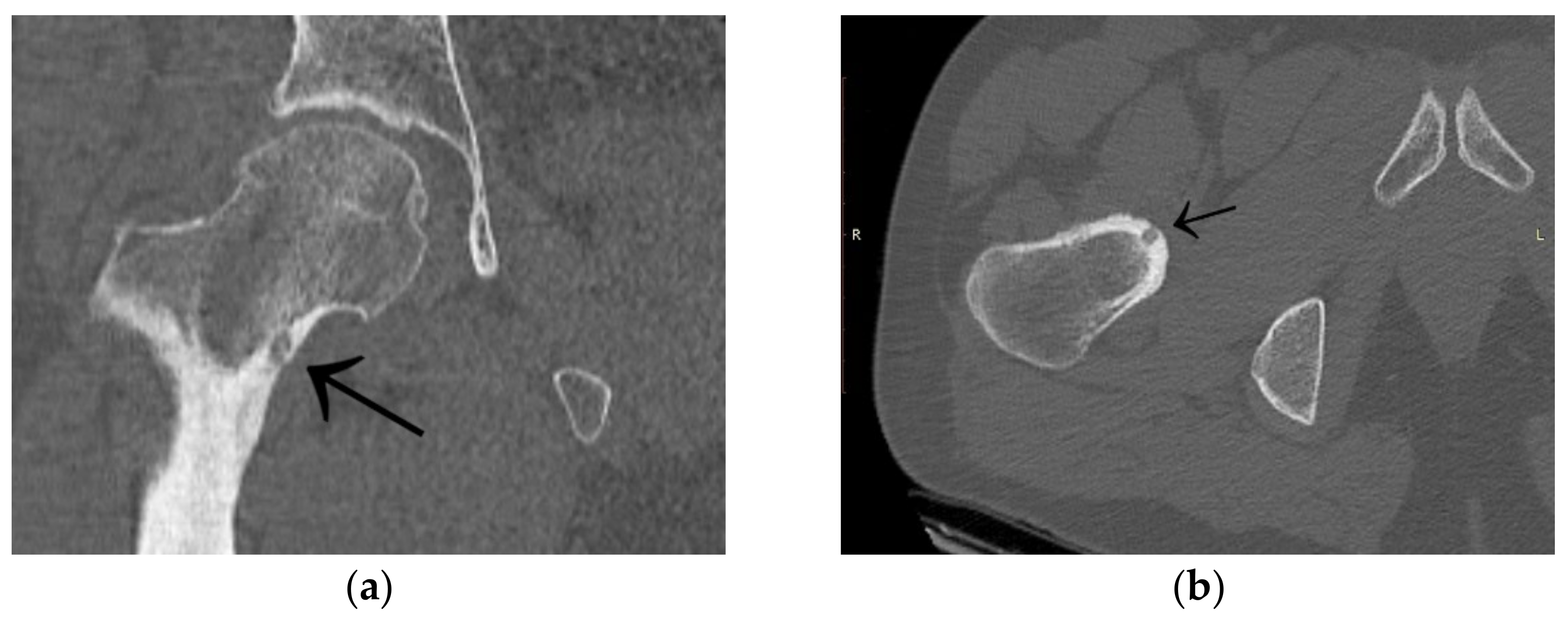
3.1. Case 1: OO Masking as Femoroacetabular Impingement (FAI)
3.2. Case 2: Example of an Incorrect Therapeutic Path of OO
3.3. Case 3: OO Masking as Lyme Disease and Leukaemia
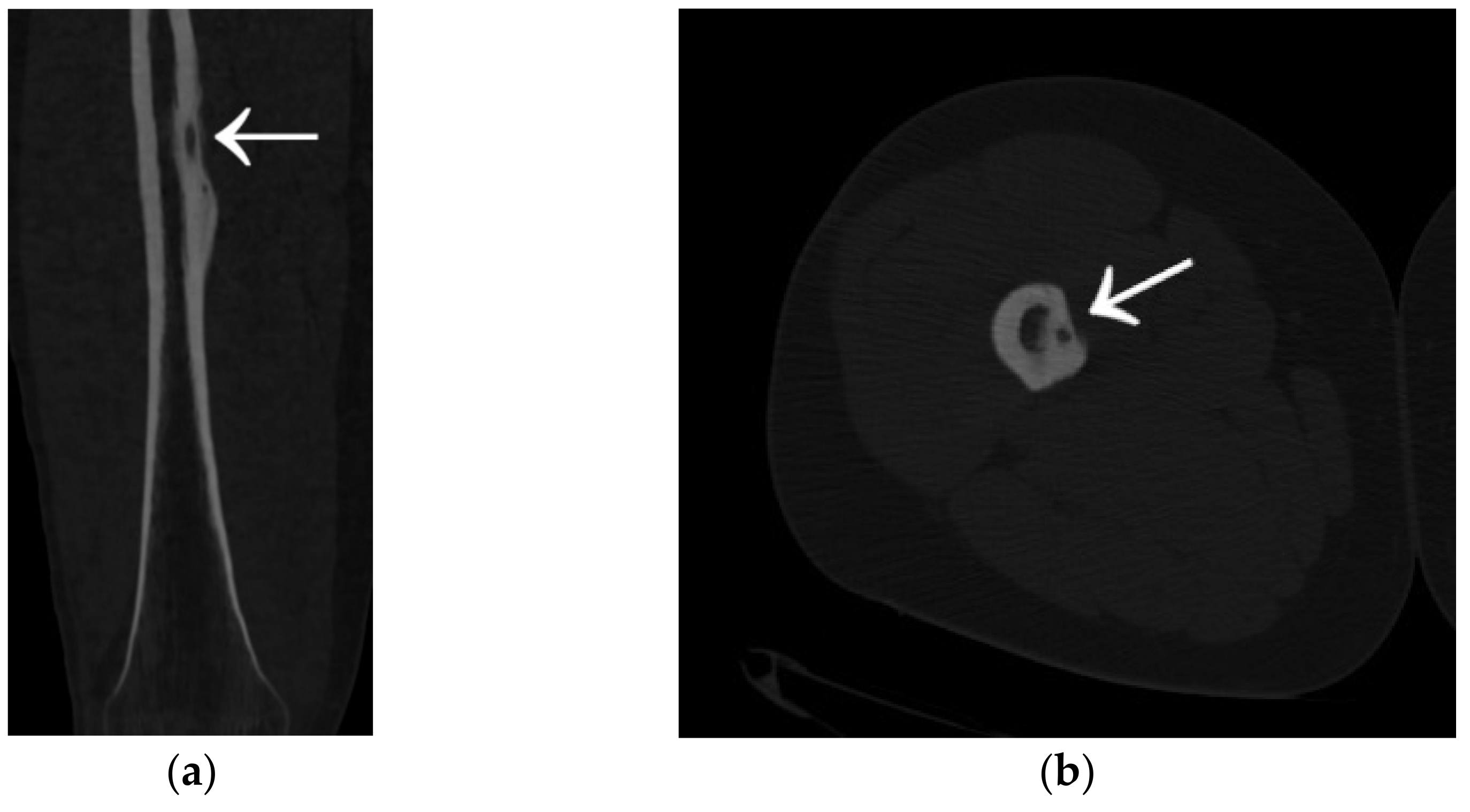
3.4. Case 4: OO Masking as a Fatigue Fracture
3.5. Case 5: OO Masking as Tuberculosis and Juvenile Idiopathic Arthritis
3.6. Case 6: OO Masking as Chronic Hip Arthritis
3.7. Case 7: OO Masking as a Meniscus Injury
3.8. Case 8: OO Masking as Juvenile Idiopathic Arthritis
3.9. Other Unusual Cases
4. Atypical Osteoid Osteomas: Presentation and Diagnosis
4.1. Osteoid Osteoma in Unusual Locations
4.2. Mimicking Rheumatologic and Inflammatory Diseases
4.3. Presentation of Osteoid Osteoma Localised Intraarticularly
4.4. Presentation of Osteoid Osteoma Localised in the Axial Skeleton
4.5. Similarity to Other Tumors
5. Diseases Masking as Osteoid Osteoma
5.1. Benign Tumors Resembling Osteoid Osteoma
5.2. Other Conditions Mimicking Osteoid Osteoma
6. Treatment of Atypical Osteoid Osteomas
7. Conclusions
Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bianchi, G.; Zugaro, L.; Palumbo, P.; Candelari, R.; Paci, E.; Floridi, C.; Giovagnoni, A. Interventional Radiology’s Osteoid Osteoma Management: Percutaneous Thermal Ablation. J. Clin. Med. 2022, 11, 723. [Google Scholar] [CrossRef]
- Arrigoni, F.; Bruno, F.; Gianneramo, C.; Palumbo, P.; Zugaro, L.; Zoccali, C.; Barile, A.; Masciocchi, C. Evolution of the imaging features of osteoid osteoma treated with RFA or MRgFUS during a long-term follow-up: A pictorial review with clinical correlations. Radiol. Med. 2020, 125, 578–584. [Google Scholar] [CrossRef]
- Baumhoer, D.; Jundt, G.; Lenze, U.; Reisinger, C.; Hirschmann, A. Enthesopathy of the pectoralis major tendon mimicking osteoid osteoma. A case report with an unfortunate series of events. Muscles Ligaments Tendons J. 2015, 5, 223–226. [Google Scholar] [CrossRef]
- Maselli, F.; Storari, L.; Lorusso, M.; Mourad, F.; Pennella, D.; Barbari, V.; Salomon, M.; Brindisino, F. Osteoid Osteoma in an Adult Wheelchair Basketball Player Mimicking Musculoskeletal Shoulder Pain: Red Flag or a Red Herring? Tomography 2022, 8, 389–401. [Google Scholar] [CrossRef] [PubMed]
- Mungo, D.V.; Zhang, X.; O’Keefe, R.J.; Rosier, R.N.; Puzas, J.E.; Schwarz, E.M. COX-1 and COX-2 expression in osteoid osteomas. J. Orthop. Res. 2002, 20, 159–162. [Google Scholar] [CrossRef]
- Acanfora, C.; Grassi, E.; Giacobbe, G.; Ferrante, M.; Granata, V.; Barile, A.; Cappabianca, S. Post-Procedural Follow-Up of the Interventional Radiology’s Management of Osteoid Osteomas and Osteoblastomas. J. Clin. Med. 2022, 11, 1987. [Google Scholar] [CrossRef]
- Malghem, J.; Lecouvet, F.; Kirchgesner, T.; Acid, S.; Vande Berg, B. Osteoid osteoma of the hip: Imaging features. Skelet. Radiol. 2020, 49, 1709–1718. [Google Scholar] [CrossRef] [PubMed]
- Van Straaten, A.; Clockaerts, S.; Vanhoenacker, F. Osteoid Osteoma of the Hallux: A Diagnostic Challenge. J. Belg. Soc. Radiol. 2021, 105, 36. [Google Scholar] [CrossRef]
- Cobianchi Bellisari, F.; Palumbo, P.; Masciocchi, C.; Zoccali, C.; Barile, A.; Arrigoni, F. Needleless Ablation of Osteoid Osteoma and Osteoblastoma: The Emergent Role of MRgFUS. J. Clin. Med. 2021, 11, 128. [Google Scholar] [CrossRef]
- Parmeggiani, A.; Martella, C.; Ceccarelli, L.; Miceli, M.; Spinnato, P.; Facchini, G. Osteoid osteoma: Which is the best mininvasive treatment option? Eur. J. Orthop. Surg. Traumatol. 2021, 31, 1611–1624. [Google Scholar] [CrossRef]
- Park, J.H.; Jung, H.W.; Jang, W.Y. Excision of Intramedullary Osteoid Osteomas in the Posterior Tibial Area via Medulloscopy: A Case Report. Medicina 2021, 57, 163. [Google Scholar] [CrossRef] [PubMed]
- Iwai, T.; Oebisu, N.; Hoshi, M.; Takada, N.; Nakamura, H. Finite Element Analysis Could Predict and Prevent a Pathological Femoral Shaft Fracture after En Bloc Resection of a Large Osteoid Osteoma. Children 2022, 9, 158. [Google Scholar] [CrossRef] [PubMed]
- De Cataldo, C.; Bruno, F.; Necozione, S.; Novello, M.; Palumbo, P.; Zugaro, L.; Barile, A.; Masciocchi, C.; Arrigoni, F. Weakening or Structural Strengthening? An Evaluation of Bone Density after MRgFUS Ablation for Treatment of Benign Bone Lesions. J. Clin. Med. 2021, 11, 182. [Google Scholar] [CrossRef] [PubMed]
- Westlake, B.; Mazzi, J.; Tedesco, N. Osteoid Osteoma Treatment with Microwave Ablation: A Report of Two Cases. Medicina 2021, 57, 470. [Google Scholar] [CrossRef]
- Ciftdemir, M.; Tuncel, S.A.; Usta, U. Atypical osteoid osteomas. Eur. J. Orthop. Surg. Traumatol. 2015, 25, 17–27. [Google Scholar] [CrossRef] [PubMed]
- Carneiro, B.C.; Da Cruz, I.A.N.; Ormond Filho, A.G.; Silva, I.P.; Guimarães, J.B.; Silva, F.D.; Nico, M.A.C.; Stump, X.M.G.R.G. Osteoid osteoma: The great mimicker. Insights Into Imaging 2021, 12, 32. [Google Scholar] [CrossRef]
- Liu, E.H.; Stone, N.; Alowami, S.O.; Thoma, A. Proximal Phalanx Osteoid Osteoma: A Case Report and Literature Review. Plast. Reconstr. Surg. Glob. Open 2017, 5, e1332. [Google Scholar] [CrossRef] [PubMed]
- Roessner, A.; Schoeder, V.; Smolle, M.; Haybäck, J. Osteoidbildende Knochentumoren: Morphologie und aktuelle translationale Zellbiologie [Osteoid-forming bone tumors: Morphology and current translational cell biology]. Pathologe 2020, 41, 123–133. (In German) [Google Scholar] [CrossRef]
- Seemann, R.; Böning, G.; Schwabe, P.; Teichgräber, U.; Gebauer, B.; Streitparth, F. Osteoid osteoma: Treatment outcome and long-term follow-up after MRI-guided laser ablation. Ann. Transl. Med. 2022, 10, 240. [Google Scholar] [CrossRef]
- Vlaic, J.; Lamot, L.; Simunic, S.; Harjacek, M.; Bojic, D. Unusual localization and presentation of osteoid osteoma mimicking juvenile spondyloarthritis: A case report. BMC Musculoskelet. Disord. 2019, 20, 17. [Google Scholar] [CrossRef]
- Becce, F.; Theumann, N.; Rochette, A.; Larousserie, F.; Campagna, R.; Cherix, S.; Guillou, L.; Mouhsine, E.; Anract, P.; Drapé, J.L.; et al. Osteoid osteoma and osteoid osteoma-mimicking lesions: Biopsy findings, distinctive MDCT features and treatment by radiofrequency ablation. Eur. Radiol. 2010, 20, 2439–2446. [Google Scholar] [CrossRef]
- Laredo, J.D.; Hamze, B.; Jeribi, R. Percutaneous biopsy of osteoid osteomas prior to percutaneous treatment using two different biopsy needles. Cardiovasc. Interv. Radiol. 2009, 32, 998–1003. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, R.T.; Jakobs, T.F.; Kubisch, C.H.; Trumm, C.G.; Weber, C.; Duerr, H.R.; Helmberger, T.K.; Reiser, M.F. Radiofrequency ablation in the treatment of osteoid osteoma-5-year experience. Eur. J. Radiol. 2010, 73, 374–379. [Google Scholar] [CrossRef]
- Wałejko, S.; Napora, J.; Mazurek, T. Osteoid osteoma mimicking tuberculosis and juvenile idiopathic arthritis—A case report. Chir. Narz. Ruchu Ortop. Pol. 2022, 87, 32–35. [Google Scholar] [CrossRef]
- Kuhaimi, T.A.; Alenezi, G.; Alawaji, A.; Alshaikh, M.; Bauones, S. Intra-articular hip joint osteoid osteoma: Challenging diagnosis and percutaneous radiofrequency ablation treatment. Radiol. Case Rep. 2021, 16, 3315–3320. [Google Scholar] [CrossRef] [PubMed]
- Glanzmann, M.C.; Imhoff, A.B.; Schwyzer, H.K. Osteoid osteoma of the shoulder and elbow: From diagnosis to minimally invasive removal. Int. Orthop. 2013, 37, 2403–2408. [Google Scholar] [CrossRef] [Green Version]
- Miyazaki, M.; Aoki, J.; Miyazaki, A.; Nakajima, T.; Koyama, Y.; Shinozaki, T.; Endo, K. Percutaneous radiofrequency ablation of osteoid osteoma using cool-tip electrodes without the cooling system. Jpn. J. Radiol. 2011, 29, 138–143. [Google Scholar] [CrossRef]
- Tepelenis, K.; Skandalakis, G.P.; Papathanakos, G.; Kefala, M.A.; Kitsouli, A.; Barbouti, A.; Tepelenis, N.; Varvarousis, D.; Vlachos, K.; Kanavaros, P.; et al. Osteoid Osteoma: An Updated Review of Epidemiology, Pathogenesis, Clinical Presentation, Radiological Features, and Treatment Option. Vivo 2021, 35, 1929–1938. [Google Scholar] [CrossRef]
- Chai, J.W.; Hong, S.H.; Choi, J.Y.; Koh, Y.H.; Lee, J.W.; Choi, J.A.; Kang, H.S. Radiologic diagnosis of osteoid osteoma: From simple to challenging findings. Radiographics 2010, 30, 737–749. [Google Scholar] [CrossRef]
- Daghighi, M.H.; Mahmoudpour, M.; Akhavi Milani, A. Osteoid osteoma of the second metatarsal bone diagnosed on MRI: A case report and literature review. Radiol. Case Rep. 2021, 17, 423–426. [Google Scholar] [CrossRef]
- Smolle, M.A.; Gilg, M.M.; Machacek, F.; Smerdelj, M.; Tunn, P.U.; Mavcic, B.; Lujic, N.; Sopta, J.; Repsa, L.; Igrec, J.; et al. Osteoid osteoma of the foot: Presentation, treatment and outcome of a multicentre cohort. Wien. Klin. Wochenschr. 2022, 134, 434–441. [Google Scholar] [CrossRef]
- Bhure, U.; Roos, J.E.; Strobel, K. Osteoid osteoma: Multimodality imaging with focus on hybrid imaging. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 1019–1036. [Google Scholar] [CrossRef] [PubMed]
- Cinka, H.; Coskun, H.S.; Ozturk, M.; Say, F.; Baris, Y.S. Osteoid Osteoma of the Distal Phalanx of the Foot: An Atypical Location. J. Am. Podiatr. Med Assoc. 2019, 109, 334–337. [Google Scholar] [CrossRef] [PubMed]
- Bellemans, M.; de Saint-Aubin de Somerhausen, N.; Lê, P.Q. Osteoid Osteoma: A Unique Presentation in a Child’s Lesser Toe. Case Rep. Orthop. 2021, 2021, 8876584. [Google Scholar] [CrossRef] [PubMed]
- Daher, J.C.; Boushnak, M.O.; Al Najjar, E.N.; Tannoury, E.H.; Moucharafieh, R.C. Osteoid Osteoma of the Distal Phalanx: A Rare Condition. Cureus 2021, 13, e19077. [Google Scholar] [CrossRef]
- Ekmekci, P.; Bostanci, S.; Erdoğan, N.; Akçaboy, B.; Gürgey, E. A painless subungual osteoid osteoma. Dermatol. Surg. 2001, 27, 764–765. [Google Scholar] [CrossRef]
- Noordin, S.; Allana, S.; Hilal, K.; Nadeem, N.; Lakdawala, R.; Sadruddin, A.; Uddin, N. Osteoid osteoma: Contemporary management. Orthop. Rev. 2018, 10, 7496. [Google Scholar] [CrossRef] [Green Version]
- Wałejko, S.; Mazurek, T.; Żychliński, M. Bifocal osteoid osteoma of the talus treated with thermal ablation and navigation 3D—Case report. Chir. Narz. Ruchu Ortop. Pol. 2020, 85, 25–28. [Google Scholar] [CrossRef]
- Güner, M.D.; Kamburoğlu, H.O.; Bektaş, U.; Ay, Ş. Osteoid osteoma of the lunatum mimicking Kienböck’s disease. Case Rep. Plast. Surg. Hand Surg. 2015, 2, 19–21. [Google Scholar] [CrossRef] [Green Version]
- Salva-Coll, G.; Terrades-Cladera, X. Osteoid osteoma of the hamate presenting as a midcarpal synovitis. J. Wrist Surg. 2015, 4, 61–64. [Google Scholar] [CrossRef] [Green Version]
- El Haj, N.I.; Hafidi, S.; Karam, R.; Boubia, S.; Karkouri, M.; Ridai, M. Osteoid osteoma of the rib: A report of an extremely rare condition. Int. J. Surg. Case Rep. 2022, 94, 107139. [Google Scholar] [CrossRef]
- Ellingsen, T.; Nalley, A.; Oda, D.; Dodson, T.B.; Lee, P.P. Osteoblastoma and Osteoid Osteoma of the Mandible: Review of the Literature and Report of Two Cases. Case Rep. Dent. 2022, 2022, 7623855. [Google Scholar] [CrossRef]
- Somma, F.; Stoia, V.; D’Angelo, R.; Fiore, F. Imaging-guided radiofrequency ablation of osteoid osteoma in typical and atypical sites: Long term follow up. PLoS ONE 2021, 16, e0248589. [Google Scholar] [CrossRef]
- Bhambhu, V.; Patel, P.G.; Mehendiratta, D.; Dalvie, S. Complete Surgical Excision with Pre-operative Localization of Lesion Under CT-Guidance of Osteoid Osteoma of the Sacrum—A Case Report. J. Orthop. Case Rep. 2020, 10, 56–60. [Google Scholar] [CrossRef] [PubMed]
- Amin, Z.H.F.; Al-Rasheedi, R.S.; Sairafi, M.H.; Alrashidi, Y. Osteoid osteoma of scapular glenoid: A case report. Int. J. Surg. Case Rep. 2020, 77, 143–146. [Google Scholar] [CrossRef]
- Sharma, S.; Rajnish, R.K.; Prakash, M.; Agarwal, S.; Dhillon, M.S. Patellar Osteoid Osteoma as a Cause of Intractable Anterior Knee Pain—A Case Report and Systematic Review of Literature. J. Orthop. Case Rep. 2020, 10, 29–34. [Google Scholar]
- Christodoulou, A.; Ploumis, A.; Karkavelas, G.; Terzidis, I.; Tsagias, I. A rare case of juxtaarticular osteoid osteoma of the calcaneus initially misdiagnosed as juvenile chronic arthritis. Arthritis Rheum. 2003, 48, 776–779. [Google Scholar] [CrossRef]
- Traore, S.Y.; Dumitriu, D.I.; Docquier, P.L. Intra-articular osteoid osteoma mimicking juvenile arthritis. Case Rep. Orthop. 2014, 2014, 912609. [Google Scholar] [CrossRef]
- Turkmen, I.; Alpan, B.; Soylemez, S.; Ozkan, F.U.; Unay, K.; Ozkan, K. Osteoid osteoma of the great toe mimicking osteomyelitis: A case report and review of the literature. Case Rep. Orthop. 2013, 2013, 234048. [Google Scholar] [CrossRef] [Green Version]
- Abd El Baky, H.; Thomas, R.D.; Kuechle, J.; Abdul-Aziz, R. Acetabula Osteoid Osteoma Mimicking Juvenile Idiopathic Arthritis and Chronic Recurrent Multifocal Osteomyelitis. Case Rep. Rheumatol. 2020, 2020, 8810735. [Google Scholar] [CrossRef]
- Shah, J.; Gandhi, D.; Chauhan, A.; Gupta, S. Imaging Review of Pediatric Benign Osteocytic Tumors and Latest Updates on Management. J. Clin. Med. 2021, 10, 2823. [Google Scholar] [CrossRef]
- Allen, S.D.; Saifuddin, A. Imaging of intra-articular osteoid osteoma. Clin. Radiol. 2003, 58, 845–852. [Google Scholar] [CrossRef]
- Seniaray, N.; Jain, A. Osteoid Osteoma Mimicking Inflammatory Synovitis. Indian J. Nucl. Med. 2017, 32, 194–197. [Google Scholar] [CrossRef] [Green Version]
- Challawar, N.S.; Shah, H.H. Intra-articular osteoid osteoma of the distal humerus: A diagnostic challenge. BMJ Case Rep. 2014, 2014, bcr2013202943. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zeng, H.; He, H.; Tong, X.; Wang, Z.; Luo, R.; Liu, Q. Osteoid Osteoma of the Proximal Femur: Pitfalls in Diagnosis and Performance of Open Surgical Resection. Front. Surg. 2022, 9, 922317. [Google Scholar] [CrossRef]
- van den Bekerom, M.P.; van Hooft, M.A.; Eygendaal, D. Osteoid osteoma of the elbow mimicking hemophilic arthropathy. World J. Clin. Cases 2014, 2, 104–107. [Google Scholar] [CrossRef]
- Song, M.H.; Yoo, W.J.; Cho, T.J.; Chung, C.Y.; Park, M.S.; Cheon, J.E.; Choi, I.H. Clinical and radiological features and skeletal sequelae in childhood intra-/juxta-articular versus extra-articular osteoid osteoma. BMC Musculoskelet. Disord. 2015, 16, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dai, L.; Zhang, X.; Mei, Y.; Gao, G.; Huang, H.; Wang, C.; Ju, X.; Xu, Y.; Wang, J. Arthroscopic Excision of Intra-Articular Osteoid Osteoma of the Hip: A Case Series. Arthroscopy 2021, 37, 3104–3112. [Google Scholar] [CrossRef] [PubMed]
- Gao, G.; Wu, R.; Liu, R.; Ao, Y.; Wang, J.; Xu, Y. Hip arthroscopy has good clinical outcomes in the treatment of osteoid osteoma of the acetabulum. BMC Musculoskelet. Disord. 2021, 22, 491. [Google Scholar] [CrossRef]
- Tomasevich, K.; Lindsay, A. Osteoid osteoma of the femoral neck mistaken as a synovial herniation pit. Radiol. Case Rep. 2021, 16, 3844–3849. [Google Scholar] [CrossRef]
- Bedard, T.; Mohammed, M.; Serinelli, S.; Damron, T.A. Atypical Enostoses-Series of Ten Cases and Literature Review. Medicina 2020, 56, 534. [Google Scholar] [CrossRef]
- Chen, Y.L.; Jiang, W.Y.; Ma, W.H. Osteoid osteoma: Lower back pain combined with scoliosis. J. Int. Med Res. 2020, 48, 300060520903873. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, Q.; Liu, W.; Xu, H.; Cui, L.; Li, Y.; Shan, H.; Huang, Z.; Ma, K.; Niu, X. Avoiding Misdiagnosis and Missed Diagnosis for Appropriately Treating Spinal Osteoid Osteomas: A Single-Center Experience. Orthop. Surg. 2022, 14, 868–875. [Google Scholar] [CrossRef] [PubMed]
- Ishikura, Y.; Yoshida, R.; Yoshizako, T.; Kishimoto, K.; Ishikawa, N.; Maruyama, R.; Kitagaki, H. Osteoid osteoma of the rib with strong F-18 fluoro-deoxyglucose uptake mimicking osteoblastoma: A case report with literature review. Acta Radiol. Open 2021, 10, 20584601211022497. [Google Scholar] [CrossRef]
- Izzo, A.; Zugaro, L.; Fascetti, E.; Bruno, F.; Zoccali, C.; Arrigoni, F. Management of Osteoblastoma and Giant Osteoid Osteoma with Percutaneous Thermoablation Techniques. J. Clin. Med. 2021, 10, 5717. [Google Scholar] [CrossRef]
- De Salvo, S.; Pavone, V.; Coco, S.; Dell’Agli, E.; Blatti, C.; Testa, G. Benign Bone Tumors: An Overview of What We Know Today. J. Clin. Med. 2022, 11, 699. [Google Scholar] [CrossRef] [PubMed]
- Georgiev, G.P.; Slavchev, S.A.; Dimitrova, I.N. Osteoid Osteoma of the Middle Phalanx of the Third Finger in a Child Mimicking a Malignancy. Folia Medica 2018, 60, 314–317. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lam, S.W.; Cleven, A.H.G.; Kroon, H.M.; Briaire-de Bruijn, I.H.; Szuhai, K.; Bovée, J.V.M.G. Utility of FOS as diagnostic marker for osteoid osteoma and osteoblastoma. Virchows Arch. 2020, 476, 455–463. [Google Scholar] [CrossRef] [Green Version]
- Ramnath, R.R.; Rosenthal, D.I.; Cates, J.; Gebhardt, M.; Quinn, R.H. Intracortical chondroma simulating osteoid osteoma treated by radiofrequency. Skelet. Radiol. 2002, 31, 597–602. [Google Scholar] [CrossRef]
- Cao, X.; Ren, Q.; Li, X.; Tian, Y.; Wang, Z. Correction to: Epiphyseal enchondroma masking as osteoid osteoma: A case report. Eur. J. Med. Res. 2021, 26, 53. [Google Scholar] [CrossRef]
- Yeh, Y.L.; Yeh, S.I.; Cheng, C.T. Intramuscular hemangioma causing periosteal reaction and cortical hypertrophy misdiagnosed as osteoid osteoma. Int. J. Surg. Case Rep. 2017, 34, 106–109. [Google Scholar] [CrossRef]
- Tilahun, T. Vaginal Leech Infestation: A Rare Cause of Hypovolumic Shock in Postmenopausal Woman. Ethiop. J. Health Sci. 2015, 25, 377–380. [Google Scholar] [CrossRef] [Green Version]
- Patel, A.; Davies, M.; James, S.; Azzopardi, C.; Botchu, R. A Rare Presentation of Osteoid Osteoma in a 77-Year-Old Patient, Treated with Computer Tomography-Guided Percutaneous Radiofrequency Ablation. Indian J. Radiol. Imaging 2021, 31, 735–739. [Google Scholar] [CrossRef]
- Erol, B.; Topkar, M.O.; Tokyay, A.; Sofulu, O.; Caliskan, E.; Okay, E. Minimal invasive intralesional excision of extremity-located osteoid osteomas in children. J. Pediatr. Orthop. B 2017, 26, 552–559. [Google Scholar] [CrossRef] [PubMed]
- Gryglewski, K.; Napora, J.; Wałejko, S.; Mazurek, T. Recent advances on diagnosis and treatment of osteoid osteoma. Chir. Narzadow Ruchu Ortop. Pol. 2022, 87, 25–31. [Google Scholar] [CrossRef]
- Jäckle, K.; Lippross, S.; Michel, T.E.; Kowallick, J.T.; Dullin, C.; Lüders, K.A.; Lorenz, H.M.; Tsaknakis, K.; Hell, A.K. A Preclinical Pilot Study on the Effects of Thermal Ablation on Lamb Growth Plates. Children 2022, 9, 878. [Google Scholar] [CrossRef]
- Mallepally, A.R.; Mahajan, R.; Pacha, S.; Rustagi, T.; Marathe, N.; Chhabra, H.S. Spinal osteoid osteoma: Surgical resection and review of literature. Surg. Neurol. Int. 2020, 11, 308. [Google Scholar] [CrossRef]
- Erdogan, O.; Gurkan, V. Hand osteoid osteoma: Evaluation of diagnosis and treatment. Eur. J. Med. Res. 2019, 24, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gökalp, M.A.; Gözen, A.; Ünsal, S.Ş.; Önder, H.; Güner, S. An Alternative Surgical Method for Treatment of Osteoid Osteoma. Med. Sci. Monit. 2016, 22, 580–586. [Google Scholar] [CrossRef]
- Ayas, M.S.; Gül, O.; Okutan, A.E.; Kerimoğlu, S.; Yıldız, M.; Turhan, A.U.; Aynacı, O. Effectiveness and reliability of traditional open surgery in atypical localizations of osteoid osteoma. Jt. Dis. Relat. Surg. 2020, 31, 541–547. [Google Scholar] [CrossRef] [PubMed]
- Gomes, A.R.; Quatrin, F.Y.; Becker, N.M.; Zanella, R.C.; Rocha, T.M.S. Resection of Bone Tumor Guided by Gamma Probe and Evaluation of Postoperative Pain. Rev. Bras. De Ortop. 2020, 55, 115–120. [Google Scholar] [CrossRef] [Green Version]
- Goyal, T.; Pandita, N.; Paul, S. Arthroscopic excision of intra-articular sub-periosteal osteoid osteoma of elbow: A case report. SICOT J. 2018, 4, 25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marwan, Y.A.; Abatzoglou, S.; Esmaeel, A.A.; Alqahtani, S.M.; Alsulaimani, S.A.; Tanzer, M.; Turcotte, R.E. Hip arthroscopy for the management of osteoid osteoma of the acetabulum: A systematic review of the literature and case report. BMC Musculoskelet. Disord. 2015, 16, 318. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Plečko, M.; Mahnik, A.; Dimnjaković, D.; Bojanić, I. Arthroscopic removal as an effective treatment option for intra-articular osteoid osteoma of the knee. World J. Orthop. 2021, 12, 505–514. [Google Scholar] [CrossRef] [PubMed]





















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Feature of OO | Typical | Atypical |
|---|---|---|
| Type of bone | Long | Short, irregular |
| Bone location | Diaphyseal; metaphyseal | Epiphyseal; intraarticular |
| Most commonly affected bones | Femur, tibia, humerus | Other |
| Nidus quantity | 1 | >1 |
| Nidus size | <10 mm | >10 mm |
| Nidus location | Cortical, subcortical | Intramedullary |
| Age of patient | <30 yrs. | >30 yrs. |
| Occurrence of pain | Night pain, awakening, rarely post-exercise | Day pain |
| Characteristics of pain | Responding to NSAIDs | Non-responding to NSAIDs |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Napora, J.; Wałejko, S.; Mazurek, T. Osteoid Osteoma, a Diagnostic Problem: A Series of Atypical and Mimicking Presentations and Review of the Recent Literature. J. Clin. Med. 2023, 12, 2721. https://doi.org/10.3390/jcm12072721
Napora J, Wałejko S, Mazurek T. Osteoid Osteoma, a Diagnostic Problem: A Series of Atypical and Mimicking Presentations and Review of the Recent Literature. Journal of Clinical Medicine. 2023; 12(7):2721. https://doi.org/10.3390/jcm12072721
Chicago/Turabian StyleNapora, Justyna, Szymon Wałejko, and Tomasz Mazurek. 2023. "Osteoid Osteoma, a Diagnostic Problem: A Series of Atypical and Mimicking Presentations and Review of the Recent Literature" Journal of Clinical Medicine 12, no. 7: 2721. https://doi.org/10.3390/jcm12072721