
Machine Learning for Onset Prediction of Patients with Intracerebral Hemorrhage
 , ,
, ,
Abstract
:1. Introduction
2. Methods
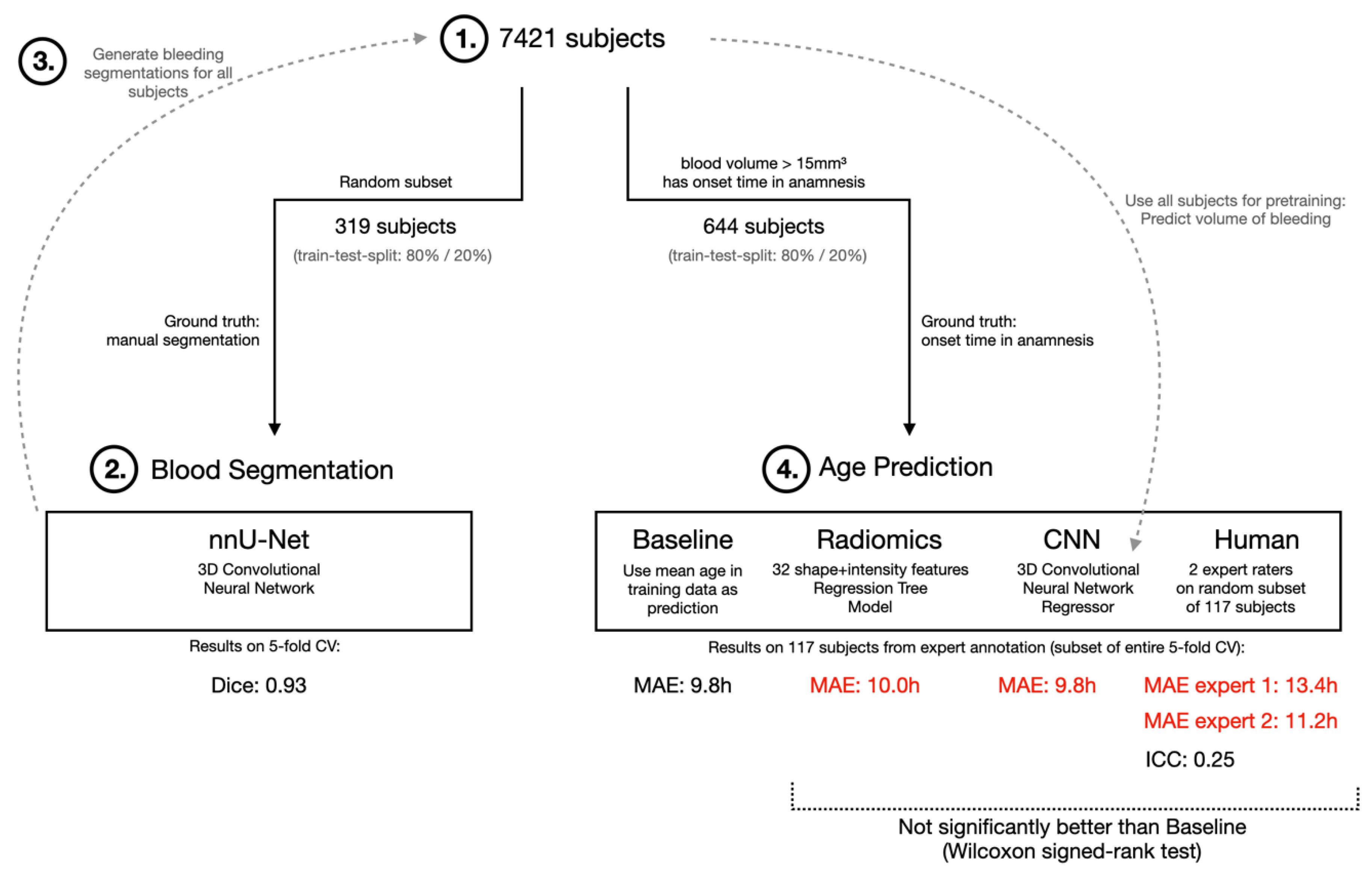
2.1. Study Design
2.2. Data Processing, Classifier Training and Image Assessment
2.3. Statistics
3. Results
3.1. Study Cohort
3.2. Onset Estimation of Classifiers and Human Raters
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AI | Artificial intelligence |
| CI | Confidence interval |
| CT | Computed tomography |
| GCS | Glasgow coma scale |
| ICH | Intracerebral hemorrhage |
| ICC | Intraclass correlation coefficient |
| INR | International normalized ratio |
| IVH | Intraventricular hemorrhage |
| mRS | Modified ranking scale |
| MAE | Mean absolute error |
| MRI | Magnetic resonance imaging |
| OAC | Oral anticoagulants |
| PACS | Picture Archiving and Communication System |
| HU | Hounsfield Unit |
| RIS | Radiological Information System |
References
- Qureshi, A.I.; Mendelow, A.D.; Hanley, D.F. Intracerebral haemorrhage. Lancet 2009, 373, 1632–1644. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caceres, J.A.; Goldstein, J.N. Intracranial hemorrhage. Emerg. Med. Clin. N. Am. 2012, 30, 771–794. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elliott, J.; Smith, M. The acute management of intracerebral hemorrhage: A clinical review. Anesth. Analg. 2010, 110, 1419–1427. [Google Scholar] [CrossRef] [PubMed]
- Broderick, J.P.; Brott, T.G.; Duldner, J.E.; Tomsick, T.; Huster, G. Volume of intracerebral hemorrhage. A powerful and easy-to-use predictor of 30-day mortality. Stroke 1993, 24, 987–993. [Google Scholar] [CrossRef] [Green Version]
- Fogelholm, R.; Murros, K.; Rissanen, A.; Avikainen, S. Long term survival after primary intracerebral haemorrhage: A retrospective population based study. J. Neurol. Neurosurg. Psychiatry 2005, 76, 1534–1538. [Google Scholar] [CrossRef] [Green Version]
- Hemphill, J.C., 3rd; Bonovich, D.C.; Besmertis, L.; Manley, G.T.; Johnston, S.C. The ICH score: A simple, reliable grading scale for intracerebral hemorrhage. Stroke 2001, 32, 891–897. [Google Scholar] [CrossRef] [Green Version]
- van Asch, C.J.; Luitse, M.J.; Rinkel, G.J.; van der Tweel, I.; Algra, A.; Klijn, C.J. Incidence, case fatality, and functional outcome of intracerebral haemorrhage over time, according to age, sex, and ethnic origin: A systematic review and meta-analysis. Lancet Neurol. 2010, 9, 167–176. [Google Scholar] [CrossRef]
- Russell, M.W.; Boulanger, L.; Joshi, A.V.; Neumann, P.J.; Menzin, J. The economic burden of intracerebral hemorrhage: Evidence from managed care. Manag. Care Interface 2006, 19, 24–28, 34. [Google Scholar]
- Smeds, M.; Skrifvars, M.B.; Reinikainen, M.; Bendel, S.; Hoppu, S.; Laitio, R.; Ala-Kokko, T.; Curtze, S.; Sibolt, G.; Martinez-Majander, N.; et al. One-year healthcare costs of patients with spontaneous intracerebral hemorrhage treated in the intensive care unit. Eur. Stroke J. 2022, 7, 267–279. [Google Scholar] [CrossRef]
- Thomas, S.M.; Reindorp, Y.; Christophe, B.R.; Connolly, E.S., Jr. Systematic Review of Resource Use and Costs in the Hospital Management of Intracerebral Hemorrhage. World Neurosurg. 2022, 164, 41–63. [Google Scholar] [CrossRef]
- Soyland, M.H.; Tveiten, A.; Eltoft, A.; Oygarden, H.; Varmdal, T.; Indredavik, B.; Mathiesen, E.B. Wake-up stroke and unknown-onset stroke; occurrence and characteristics from the nationwide Norwegian Stroke Register. Eur. Stroke J. 2022, 7, 143–150. [Google Scholar] [CrossRef] [PubMed]
- Sporns, P.B.; Schwake, M.; Schmidt, R.; Kemmling, A.; Minnerup, J.; Schwindt, W.; Cnyrim, C.; Zoubi, T.; Heindel, W.; Niederstadt, T.; et al. Computed Tomographic Blend Sign Is Associated With Computed Tomographic Angiography Spot Sign and Predicts Secondary Neurological Deterioration After Intracerebral Hemorrhage. Stroke 2017, 48, 131–135. [Google Scholar] [CrossRef] [PubMed]
- Inoue, Y.; Miyashita, F.; Koga, M.; Minematsu, K.; Toyoda, K. Unclear-onset intracerebral hemorrhage: Clinical characteristics, hematoma features, and outcomes. Int. J. Stroke 2017, 12, 961–968. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.Y.; Bae, H.J. Spontaneous Intracerebral Hemorrhage: Management. J. Stroke 2017, 19, 28–39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qureshi, A.I. Antihypertensive Treatment of Acute Cerebral Hemorrhage (ATACH): Rationale and design. Neurocrit. Care 2007, 6, 56–66. [Google Scholar] [CrossRef] [PubMed]
- Qureshi, A.I.; Palesch, Y.Y. Antihypertensive Treatment of Acute Cerebral Hemorrhage (ATACH) II: Design, methods, and rationale. Neurocrit. Care 2011, 15, 559–576. [Google Scholar] [CrossRef] [Green Version]
- Anderson, C.S.; Heeley, E.; Huang, Y.; Wang, J.; Stapf, C.; Delcourt, C.; Lindley, R.; Robinson, T.; Lavados, P.; Neal, B.; et al. Rapid blood-pressure lowering in patients with acute intracerebral hemorrhage. N. Engl. J. Med. 2013, 368, 2355–2365. [Google Scholar] [CrossRef]
- Luzzi, S.; Elia, A.; Del Maestro, M.; Morotti, A.; Elbabaa, S.K.; Cavallini, A.; Galzio, R. Indication, Timing, and Surgical Treatment of Spontaneous Intracerebral Hemorrhage: Systematic Review and Proposal of a Management Algorithm. World Neurosurg. 2019, 124, e769–e778. [Google Scholar] [CrossRef]
- Sprigg, N.; Flaherty, K.; Appleton, J.P.; Al-Shahi Salman, R.; Bereczki, D.; Beridze, M.; Christensen, H.; Ciccone, A.; Collins, R.; Czlonkowska, A.; et al. Tranexamic acid for hyperacute primary IntraCerebral Haemorrhage (TICH-2): An international randomised, placebo-controlled, phase 3 superiority trial. Lancet 2018, 391, 2107–2115. [Google Scholar] [CrossRef] [Green Version]
- Sporns, P.B.; Schwake, M.; Kemmling, A.; Minnerup, J.; Schwindt, W.; Niederstadt, T.; Schmidt, R.; Hanning, U. Comparison of Spot Sign, Blend Sign and Black Hole Sign for Outcome Prediction in Patients with Intracerebral Hemorrhage. J. Stroke 2017, 19, 333–339. [Google Scholar] [CrossRef] [Green Version]
- Sporns, P.B.; Kemmling, A.; Minnerup, J.; Hanning, U.; Heindel, W. Imaging-based outcome prediction in patients with intracerebral hemorrhage. Acta Neurochir. 2018, 160, 1663–1670. [Google Scholar] [CrossRef] [PubMed]
- Sporns, P.B.; Kemmling, A.; Schwake, M.; Minnerup, J.; Nawabi, J.; Broocks, G.; Wildgruber, M.; Fiehler, J.; Heindel, W.; Hanning, U. Triage of 5 Noncontrast Computed Tomography Markers and Spot Sign for Outcome Prediction After Intracerebral Hemorrhage. Stroke 2018, 49, 2317–2322. [Google Scholar] [CrossRef] [PubMed]
- Nawabi, J.; Kniep, H.; Elsayed, S.; Friedrich, C.; Sporns, P.; Rusche, T.; Bohmer, M.; Morotti, A.; Schlunk, F.; Duhrsen, L.; et al. Imaging-Based Outcome Prediction of Acute Intracerebral Hemorrhage. Transl. Stroke Res. 2021, 12, 958–967. [Google Scholar] [CrossRef] [PubMed]
- Reyes, M.; Meier, R.; Pereira, S.; Silva, C.A.; Dahlweid, F.M.; von Tengg-Kobligk, H.; Summers, R.M.; Wiest, R. On the Interpretability of Artificial Intelligence in Radiology: Challenges and Opportunities. Radiol. Artif. Intell. 2020, 2, e190043. [Google Scholar] [CrossRef]
- Richardson, M.L.; Garwood, E.R.; Lee, Y.; Li, M.D.; Lo, H.S.; Nagaraju, A.; Nguyen, X.V.; Probyn, L.; Rajiah, P.; Sin, J.; et al. Noninterpretive Uses of Artificial Intelligence in Radiology. Acad. Radiol. 2021, 28, 1225–1235. [Google Scholar] [CrossRef]
- Weikert, T.; Winkel, D.J.; Bremerich, J.; Stieltjes, B.; Parmar, V.; Sauter, A.W.; Sommer, G. Automated detection of pulmonary embolism in CT pulmonary angiograms using an AI-powered algorithm. Eur. Radiol. 2020, 30, 6545–6553. [Google Scholar] [CrossRef]
- Rao, B.; Zohrabian, V.; Cedeno, P.; Saha, A.; Pahade, J.; Davis, M.A. Utility of Artificial Intelligence Tool as a Prospective Radiology Peer Reviewer—Detection of Unreported Intracranial Hemorrhage. Acad. Radiol. 2021, 28, 85–93. [Google Scholar] [CrossRef]
- Rava, R.A.; Seymour, S.E.; LaQue, M.E.; Peterson, B.A.; Snyder, K.V.; Mokin, M.; Waqas, M.; Hoi, Y.; Davies, J.M.; Levy, E.I.; et al. Assessment of an Artificial Intelligence Algorithm for Detection of Intracranial Hemorrhage. World Neurosurg. 2021, 150, e209–e217. [Google Scholar] [CrossRef]
- Voter, A.F.; Meram, E.; Garrett, J.W.; Yu, J.J. Diagnostic Accuracy and Failure Mode Analysis of a Deep Learning Algorithm for the Detection of Intracranial Hemorrhage. J. Am. Coll. Radiol. 2021, 18, 1143–1152. [Google Scholar] [CrossRef]
- Sporns, P.B.; Psychogios, M.N.; Boulouis, G.; Charidimou, A.; Li, Q.; Fainardi, E.; Dowlatshahi, D.; Goldstein, J.N.; Morotti, A. Neuroimaging of Acute Intracerebral Hemorrhage. J. Clin. Med. 2021, 10, 1086. [Google Scholar] [CrossRef]
- Barras, C.D.; Tress, B.M.; Christensen, S.; MacGregor, L.; Collins, M.; Desmond, P.M.; Skolnick, B.E.; Mayer, S.A.; Broderick, J.P.; Diringer, M.N.; et al. Density and shape as CT predictors of intracerebral hemorrhage growth. Stroke 2009, 40, 1325–1331. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nawabi, J.; Elsayed, S.; Morotti, A.; Speth, A.; Liu, M.; Kniep, H.; McDonough, R.; Broocks, G.; Faizy, T.; Can, E.; et al. Perihematomal Edema and Clinical Outcome in Intracerebral Hemorrhage Related to Different Oral Anticoagulants. J. Clin. Med. 2021, 10, 2234. [Google Scholar] [CrossRef] [PubMed]
- Sporns, P.B.; Psychogios, M.N.; Fullerton, H.J.; Lee, S.; Naggara, O.; Boulouis, G. Neuroimaging of Pediatric Intracerebral Hemorrhage. J. Clin. Med. 2020, 9, 1518. [Google Scholar] [CrossRef] [PubMed]
- Zimmer, S.; Meier, J.; Minnerup, J.; Wildgruber, M.; Broocks, G.; Nawabi, J.; Morotti, A.; Kemmling, A.; Psychogios, M.; Hanning, U.; et al. Prognostic Value of Non-Contrast CT Markers and Spot Sign for Outcome Prediction in Patients with Intracerebral Hemorrhage under Oral Anticoagulation. J. Clin. Med. 2020, 9, 1077. [Google Scholar] [CrossRef] [PubMed]
- Morotti, A.; Nawabi, J.; Schlunk, F.; Poli, L.; Costa, P.; Mazzacane, F.; Busto, G.; Scola, E.; Arba, F.; Brancaleoni, L.; et al. Characteristics of Early Presenters after Intracerebral Hemorrhage. J. Stroke 2022, 24, 425–428. [Google Scholar] [CrossRef]
- Morotti, A.; Boulouis, G.; Dowlatshahi, D.; Li, Q.; Barras, C.D.; Delcourt, C.; Yu, Z.; Zheng, J.; Zhou, Z.; Aviv, R.I.; et al. Standards for Detecting, Interpreting, and Reporting Noncontrast Computed Tomographic Markers of Intracerebral Hemorrhage Expansion. Ann. Neurol. 2019, 86, 480–492. [Google Scholar] [CrossRef]
- Nawabi, J.; Elsayed, S.; Kniep, H.; Sporns, P.; Schlunk, F.; McDonough, R.; Broocks, G.; Duhrsen, L.; Schon, G.; Gotz, T.; et al. Inter- and Intrarater Agreement of Spot Sign and Noncontrast CT Markers for Early Intracerebral Hemorrhage Expansion. J. Clin. Med. 2020, 9, 1020. [Google Scholar] [CrossRef] [Green Version]
- Guo, Y.; Guo, X.M.; Li, R.L.; Zhao, K.; Bao, Q.J.; Yang, J.C.; Zhang, Q.; Yang, M.F. Tranexamic Acid for Acute Spontaneous Intracerebral Hemorrhage: A Meta-Analysis of Randomized Controlled Trials. Front. Neurol. 2021, 12, 761185. [Google Scholar] [CrossRef]
- Broocks, G.; Leischner, H.; Hanning, U.; Flottmann, F.; Faizy, T.D.; Schon, G.; Sporns, P.; Thomalla, G.; Kamalian, S.; Lev, M.H.; et al. Lesion Age Imaging in Acute Stroke: Water Uptake in CT Versus DWI-FLAIR Mismatch. Ann. Neurol. 2020, 88, 1144–1152. [Google Scholar] [CrossRef]
- Nawabi, J.; Flottmann, F.; Kemmling, A.; Kniep, H.; Leischner, H.; Sporns, P.; Schon, G.; Hanning, U.; Thomalla, G.; Fiehler, J.; et al. Elevated early lesion water uptake in acute stroke predicts poor outcome despite successful recanalization—When “tissue clock” and “time clock” are desynchronized. Int. J. Stroke 2021, 16, 863–872. [Google Scholar] [CrossRef]
- Sporns, P.B.; Hohne, M.; Meyer, L.; Krogias, C.; Puetz, V.; Thierfelder, K.M.; Duering, M.; Kaiser, D.; Langner, S.; Brehm, A.; et al. Simplified Assessment of Lesion Water Uptake for Identification of Patients within 4.5 Hours of Stroke Onset: An Analysis of the MissPerfeCT Study. J. Stroke 2022, 24, 390–395. [Google Scholar] [CrossRef] [PubMed]
- Sporns, P.B.; Kemmling, A.; Minnerup, H.; Meyer, L.; Krogias, C.; Puetz, V.; Thierfelder, K.; Duering, M.; Kaiser, D.; Langner, S.; et al. CT Hypoperfusion-Hypodensity Mismatch to Identify Patients With Acute Ischemic Stroke Within 4.5 Hours of Symptom Onset. Neurology 2021, 97, e2088–e2095. [Google Scholar] [CrossRef] [PubMed]
- Thomalla, G.; Simonsen, C.Z.; Boutitie, F.; Andersen, G.; Berthezene, Y.; Cheng, B.; Cheripelli, B.; Cho, T.H.; Fazekas, F.; Fiehler, J.; et al. MRI-Guided Thrombolysis for Stroke with Unknown Time of Onset. N. Engl. J. Med. 2018, 379, 611–622. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Esteva, A.; Kuprel, B.; Novoa, R.A.; Ko, J.; Swetter, S.M.; Blau, H.M.; Thrun, S. Dermatologist-level classification of skin cancer with deep neural networks. Nature 2017, 542, 115–118. [Google Scholar] [CrossRef]
- Kornbluth, J.; Nekoovaght-Tak, S.; Ullman, N.; Carhuapoma, J.R.; Hanley, D.F.; Ziai, W. Early Quantification of Hematoma Hounsfield Units on Noncontrast CT in Acute Intraventricular Hemorrhage Predicts Ventricular Clearance after Intraventricular Thrombolysis. AJNR Am. J. Neuroradiol. 2015, 36, 1609–1615. [Google Scholar] [CrossRef] [Green Version]
- Ziya, A. Determination of bleeding time by hounsfield unit values in computed tomography scans of patients diagnosed with intracranial hemorrhage: Evaluation results of computed tomography scans of 666 patients. Clin. Neurol. Neurosurg. 2022, 217, 107258. [Google Scholar] [CrossRef]
- Xu, J.; Dai, F.; Wang, B.; Wang, Y.; Li, J.; Pan, L.; Liu, J.; Liu, H.; He, S. Predictive Value of CT Perfusion in Hemorrhagic Transformation after Acute Ischemic Stroke: A Systematic Review and Meta-Analysis. Brain Sci. 2023, 13, 156. [Google Scholar] [CrossRef]
- Tian, X.; Fang, H.; Lan, L.; Ip, H.L.; Abrigo, J.; Liu, H.; Zheng, L.; Fan, F.S.Y.; Ma, S.H.; Ip, B.; et al. Risk stratification in symptomatic intracranial atherosclerotic disease with conventional vascular risk factors and cerebral haemodynamics. Stroke Vasc. Neurol. 2023, 8, 77–85. [Google Scholar] [CrossRef]
- Lee, R.M. Morphology of cerebral arteries. Pharmacol. Ther. 1995, 66, 149–173. [Google Scholar] [CrossRef]
- Niederberger, E.; Gauvrit, J.Y.; Morandi, X.; Carsin-Nicol, B.; Gauthier, T.; Ferre, J.C. Anatomic variants of the anterior part of the cerebral arterial circle at multidetector computed tomography angiography. J. Neuroradiol. 2010, 37, 139–147. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Mean Absolute Error (MAE) in h | 95% Confidence Interval (CI) | |
|---|---|---|
| Rater 1 | 13.38 | 11.21, 15.74 |
| Rater 2 | 11.21 | 9.51, 12.90 |
| CNN | 9.77 | 8.52, 11.03 |
| Radiomics | 9.96 | 8.68, 11.32 |
| Mean of known onset in entire cohort | 9.81 | 8.62, 11.06 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rusche, T.; Wasserthal, J.; Breit, H.-C.; Fischer, U.; Guzman, R.; Fiehler, J.; Psychogios, M.-N.; Sporns, P.B. Machine Learning for Onset Prediction of Patients with Intracerebral Hemorrhage. J. Clin. Med. 2023, 12, 2631. https://doi.org/10.3390/jcm12072631
Rusche T, Wasserthal J, Breit H-C, Fischer U, Guzman R, Fiehler J, Psychogios M-N, Sporns PB. Machine Learning for Onset Prediction of Patients with Intracerebral Hemorrhage. Journal of Clinical Medicine. 2023; 12(7):2631. https://doi.org/10.3390/jcm12072631
Chicago/Turabian StyleRusche, Thilo, Jakob Wasserthal, Hanns-Christian Breit, Urs Fischer, Raphael Guzman, Jens Fiehler, Marios-Nikos Psychogios, and Peter B. Sporns. 2023. "Machine Learning for Onset Prediction of Patients with Intracerebral Hemorrhage" Journal of Clinical Medicine 12, no. 7: 2631. https://doi.org/10.3390/jcm12072631