
Incidence of Healthcare-Associated Infections in a Neonatal Intensive Care Unit before and during the COVID-19 Pandemic: A Four-Year Retrospective Cohort Study
 , , , , ,
, , , , ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Setting
2.2. Data Collection
2.3. Statistical Analysis
3. Results
3.1. Characteristics of Patients
3.2. Occurrence of HAIs
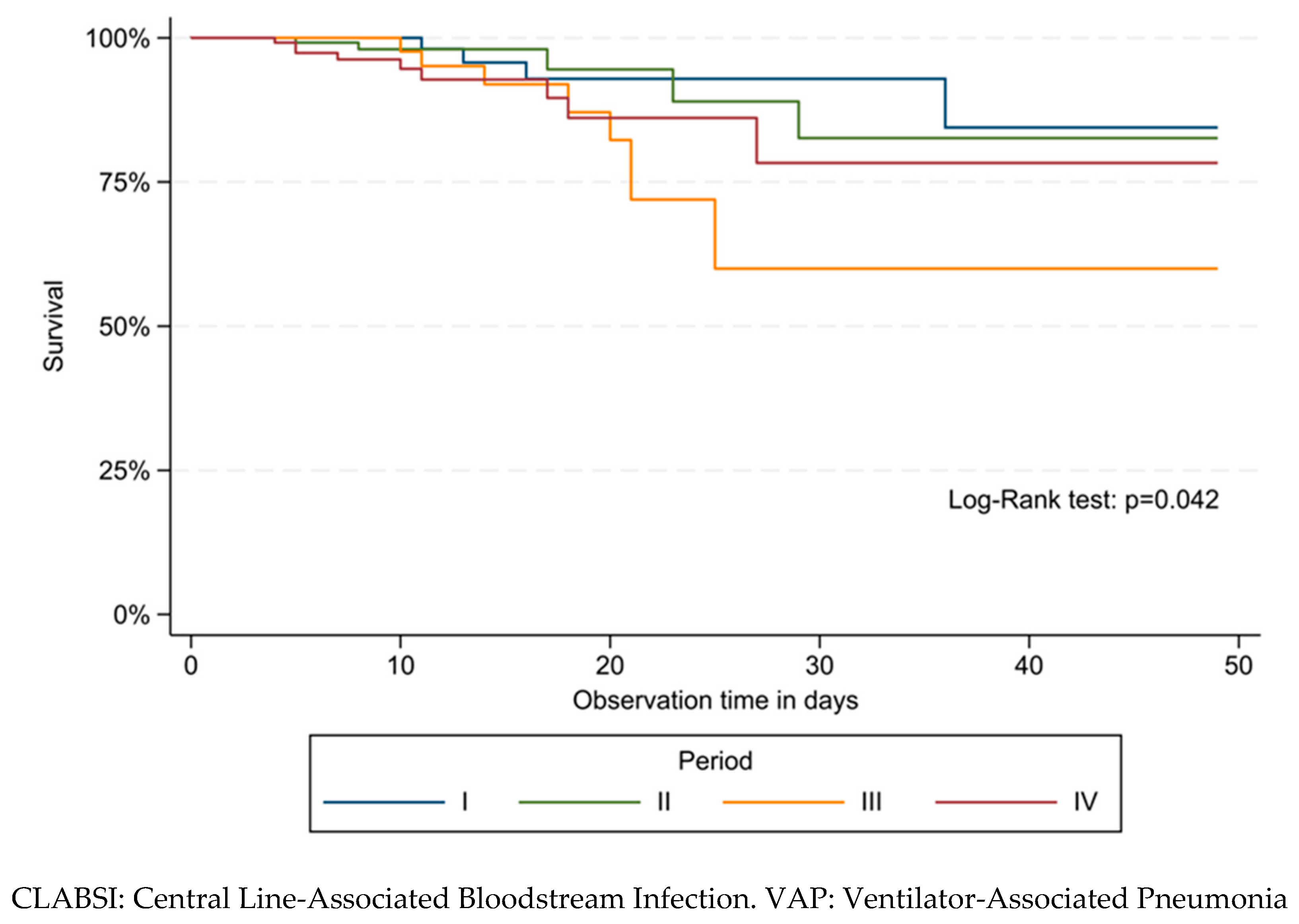
3.3. Survival Analysis for First HAI
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kumar, S.; Shankar, B.; Arya, S.; Deb, M.; Chellani, H. Healthcare Associated Infections in Neonatal Intensive Care Unit and Its Correlation with Environmental Surveillance. J. Infect. Public Health 2018, 11, 275–279. [Google Scholar] [CrossRef]
- Graham, P.L. Simple Strategies to Reduce Healthcare Associated Infections in the Neonatal Intensive Care Unit: Line, Tube, and Hand Hygiene. Clin. Perinatol. 2010, 37, 645–653. [Google Scholar] [CrossRef]
- Sass, L.; Karlowicz, M.G. Healthcare-Associated Infections in the Neonate. Princ. Pract. Pediatr. Infect. Dis. 2018, 560–566. [Google Scholar] [CrossRef]
- Scamardo, M.S.; Dolce, P.; Esposito, E.P.; Raimondi, F.; Triassi, M.; Zarrilli, R. Trends, Risk Factors and Outcomes of Healthcare-Associated Infections in a Neonatal Intensive Care Unit in Italy during 2013–2017. Ital. J. Pediatr 2020, 46, 34. [Google Scholar] [CrossRef] [Green Version]
- Quattrocolo, F.; D’Ambrosio, A.; Corcione, S.; Stillo, M.; Blanco, V.; Gualano, M.; Villa, G.; Voglino, G.; Clemente, S.; Camussi, E.; et al. Studio di Prevalenza Italiano Sulle Infezioni Correlate All’Assistenza e Sull’uso di Antibiotici Negli Ospedali per Acuti-Protocollo ECDC; Dipartimento Scienze della Salute Pubblica e Pediatriche, Università di Torino: Turin, Italy, 2018. [Google Scholar]
- Baccolini, V.; Migliara, G.; Isonne, C.; Dorelli, B.; Barone, L.C.; Giannini, D.; Marotta, D.; Marte, M.; Mazzalai, E.; Alessandri, F.; et al. The Impact of the COVID-19 Pandemic on Healthcare-Associated Infections in Intensive Care Unit Patients: A Retrospective Cohort Study. Antimicrob. Resist. Infect. Control. 2021, 10, 87. [Google Scholar] [CrossRef] [PubMed]
- Ng, Q.X.; Ong, N.Y.; Lee, D.Y.X.; Yau, C.E.; Lim, Y.L.; Kwa, A.L.H.; Tan, B.H. Trends in Pseudomonas aeruginosa (P. Aeruginosa) Bacteremia during the COVID-19 Pandemic: A Systematic Review. Antibiotics 2023, 12, 409. [Google Scholar] [CrossRef] [PubMed]
- Kharrat, A.; Neish, A.; Diambomba, Y.; Jain, A. Non-COVID Co-Morbidity: Potential Indirect Consequences of the SARS-CoV-2 Pandemic in a Neonatal Intensive Care Unit. J. Hosp. Infect. 2021, 109, 65–67. [Google Scholar] [CrossRef]
- Griffin, I.; Benarba, F.; Peters, C.; Oyelese, Y.; Murphy, T.; Contreras, D.; Gagliardo, C.; Nwaobasi-Iwuh, E.; Dipentima, M.C.; Schenkman, A. The Impact of COVID-19 Infection on Labor and Delivery, Newborn Nursery, and Neonatal Intensive Care Unit: Prospective Observational Data from a Single Hospital System. Am. J. Perinatol. 2020, 37, 1022–1030. [Google Scholar] [CrossRef] [PubMed]
- Conti, M.G.; Natale, F.; Stolfi, I.; Pedicino, R.; Boscarino, G.; Ajassa, C.; Cardilli, V.; Ciambra, G.L.; Guadalupi, L.; Favata, P.; et al. Consequences of Early Separation of Maternal-Newborn Dyad in Neonates Born to Sars-Cov-2 Positive Mothers: An Observational Study. Int. J. Environ. Res. Public Health 2021, 18, 5899. [Google Scholar] [CrossRef]
- Isonne, C.; Baccolini, V.; Migliara, G.; Ceparano, M.; Alessandri, F.; Ceccarelli, G.; Tellan, G.; Pugliese, F.; de Giusti, M.; de Vito, C.; et al. Comparing the Occurrence of Healthcare-Associated Infections in Patients with and without COVID-19 Hospitalized during the Pandemic: A 16-Month Retrospective Cohort Study in a Hospital Intensive Care Unit. J. Clin. Med. 2022, 11, 1446. [Google Scholar] [CrossRef]
- Ceparano, M.; Baccolini, V.; Migliara, G.; Isonne, C.; Renzi, E.; Tufi, D.; de Vito, C.; de Giusti, M.; Trancassini, M.; Alessandri, F.; et al. Acinetobacter baumannii Isolates from COVID-19 Patients in a Hospital Intensive Care Unit: Molecular Typing and Risk Factors. Microorganisms 2022, 10, 722. [Google Scholar] [CrossRef]
- Deiana, G.; Arghittu, A.; Gentili, D.; Dettori, M.; Palmieri, A.; Masia, M.D.; Azara, A.; Castiglia, P. Impact of the COVID-19 Pandemic on the Prevalence of HAIs and the Use of Antibiotics in an Italian University Hospital. Healthcare 2022, 10, 1597. [Google Scholar] [CrossRef] [PubMed]
- Cena, L.; Biban, P.; Janos, J.; Lavelli, M.; Langfus, J.; Tsai, A.; Youngstrom, E.A.; Stefana, A. The Collateral Impact of COVID-19 Emergency on Neonatal Intensive Care Units and Family-Centered Care: Challenges and Opportunities. Front. Psychol. 2021, 12, 630594. [Google Scholar] [CrossRef] [PubMed]
- Indrio, F.; Salatto, A.; Amato, O.; Bartoli, F.; Capasso, L.; Corvaglia, L.; Maffei, G.; Mosca, F.; Pettoello Mantovani, M.; Raimondi, F.; et al. COVID-19 Pandemic in the Neonatal Intensive Care Unit: Any Effect on Late-Onset Sepsis and Necrotizing Enterocolitis? Eur. J. Pediatr. 2022, 181, 853–857. [Google Scholar] [CrossRef]
- Magiorakos, A.P.; Srinivasan, A.; Carey, R.B.; Carmeli, Y.; Falagas, M.E.; Giske, C.G.; Harbarth, S.; Hindler, J.F.; Kahlmeter, G.; Olsson-Liljequist, B.; et al. Multidrug-Resistant, Extensively Drug-Resistant and Pandrug-Resistant Bacteria: An International Expert Proposal for Interim Standard Definitions for Acquired Resistance. Clin. Microbiol. Infect. 2012, 18, 268–281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Becker, K.; Skov, R.L.; von Eiff, C. Staphylococcus, Micrococcus, and Other Catalase-Positive Cocci. Man. Clin. Microbiol. 2021, 354–382. [Google Scholar]
- Horan, T.C.; Andrus, M.; Dudeck, M.A. CDC/NHSN Surveillance Definition of Health Care-Associated Infection and Criteria for Specific Types of Infections in the Acute Care Setting. Am. J. Infect. Control. 2008, 36, 309–332. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention National Healthcare Safety Network (NHSN). Patient Safety Component Manual; NHSN: Atlanta, GA, USA, 2023. [Google Scholar]
- Prakash Yadav, C. An Overview of Statistical Models for Recurrent Events Analysis: A Review. Epidemiology 2018, 8, 354. [Google Scholar] [CrossRef]
- Talbot, D.; Massamba, V.K. A Descriptive Review of Variable Selection Methods in Four Epidemiologic Journals: There Is Still Room for Improvement. Eur. J. Epidemiol. 2019, 34, 725–730. [Google Scholar] [CrossRef] [PubMed]
- Rosenthal, V.D.; Myatra, S.N.; Divatia, J.V.; Biswas, S.; Shrivastava, A.; Al-Ruzzieh, M.A.; Ayaad, O.; Bat-Erdene, A.; Bat-Erdene, I.; Narankhuu, B.; et al. The Impact of COVID-19 on Health Care–Associated Infections in Intensive Care Units in Low- and Middle-Income Countries: International Nosocomial Infection Control Consortium (INICC) Findings. Int. J. Infect. Dis. 2022, 118, 83–88. [Google Scholar] [CrossRef] [PubMed]
- Shekerdemian, L.S.; Mahmood, N.R.; Wolfe, K.K.; Riggs, B.J.; Ross, C.E.; McKiernan, C.A.; Heidemann, S.M.; Kleinman, L.C.; Sen, A.I.; Hall, M.W.; et al. Characteristics and Outcomes of Children with Coronavirus Disease 2019 (COVID-19) Infection Admitted to US and Canadian Pediatric Intensive Care Units. JAMA Pediatr. 2020, 174, 868–873. [Google Scholar] [CrossRef]
- Thomas Stelfox, H.; Bates, D.W.; Redelmeier, D.A. Safety of Patients Isolated for Infection Control. JAMA 2003, 290, 1899–1905. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Casafont, C.; Fabrellas, N.; Rivera, P.; Olivé-Ferrer, M.C.; Querol, E.; Venturas, M.; Prats, J.; Cuzco, C.; Frías, C.E.; Pérez-Ortega, S.; et al. Experiences of Nursing Students as Healthcare Aid during the COVID-19 Pandemic in Spain: A Phemonenological Research Study. Nurse Educ. Today 2021, 97, 104711. [Google Scholar] [CrossRef] [PubMed]
- Rogowski, J.A.; Staiger, D.; Patrick, T.; Horbar, J.; Kenny, M.; Lake, E.T. Nurse Staffing and Nicu Infection Rates. JAMA Pediatr. 2013, 167, 444–450. [Google Scholar] [CrossRef] [Green Version]
- Raven, J.H.; Tolhurst, R.J.; Tang, S.; van den Broek, N. What Is Quality in Maternal and Neonatal Health Care? Midwifery 2012, 28, e676–e683. [Google Scholar] [CrossRef] [PubMed]
- Orsi, G.B.; d’Ettorre, G.; Panero, A.; Chiarini, F.; Vullo, V.; Venditti, M. Hospital-Acquired Infection Surveillance in a Neonatal Intensive Care Unit. Am. J. Infect. Control. 2009, 37, 201–203. [Google Scholar] [CrossRef] [PubMed]
- Auriti, C.; Ronchetti, M.P.; Pezzotti, P.; Marrocco, G.; Quondamcarlo, A.; Seganti, G.; Bagnoli, F.; de Felice, C.; Buonocore, G.; Arioni, C.; et al. Determinants of Nosocomial Infection in 6 Neonatal Intensive Care Units: An Italian Multicenter Prospective Cohort Study. Infect. Control. Hosp. Epidemiol. 2010, 31, 926–933. [Google Scholar] [CrossRef]
- Kraus-Haas, M.; Mielke, M.; Simon, A. Update on Outbreaks Reported from Neonatal Intensive Care Units: Serratia Marcescens, Klebsiella Pneumoniae, Acinetobacter baumannii, and Pseudomonas aeruginosa. Bundesgesundheitsblatt Gesundh. Gesundh. 2015, 58, 308–322. [Google Scholar] [CrossRef] [Green Version]
- Morillo, Á.; González, V.; Aguayo, J.; Carreño, C.; Torres, M.J.; Jarana, D.; Artacho, M.J.; Jiménez, F.; Conde, M.; Aznar, J. Brote Epidémico Por Serratia Marcescens En Una Unidad de Cuidados Intensivos Neonatales. Enferm. Infecc. Microbiol. Clin. 2016, 34, 645–651. [Google Scholar] [CrossRef]
- Hocevar, S.N.; Edwards, J.R.; Horan, T.C.; Morrell, G.C.; Iwamoto, M.; Lessa, F.C. Device-Associated Infections among Neonatal Intensive Care Unit Patients: Incidence and Associated Pathogens Reported to the National Healthcare Safety Network, 2006–2008. Infect. Control. Hosp. Epidemiol. 2012, 33, 1200–1206. [Google Scholar] [CrossRef]
- Cailes, B.; Kortsalioudaki, C.; Buttery, J.; Pattnayak, S.; Greenough, A.; Matthes, J.; Bedford Russell, A.; Kennea, N.; Heath, P.T. Epidemiology of UK Neonatal Infections: The NeonIN Infection Surveillance Network. Arch. Dis. Child Fetal Neonatal. Ed. 2018, 103, F547–F553. [Google Scholar] [CrossRef]
- Viswanathan, R.; Singh, A.K.; Mukherjee, S.; Mukherjee, R.; Das, P.; Basu, S. An Outbreak of Neonatal Sepsis Presenting with Exanthematous Rash Caused by Klebsiella Pneumoniae. Epidemiol. Infect. 2011, 139, 226–228. [Google Scholar] [CrossRef] [PubMed]
- Fabbri, G.; Panico, M.; Dallolio, L.; Suzzi, R.; Ciccia, M.; Sandri, F.; Farruggia, P. Outbreak of Ampicillin/Piperacillin-Resistant Klebsiella pneumoniae in a Neonatal Intensive Care Unit (NICU): Investigation and Control Measures. Int. J. Environ. Res. Public Health 2013, 10, 808–815. [Google Scholar] [CrossRef] [Green Version]
- Cristina, M.L.; Sartini, M.; Spagnolo, A.M. Serratia marcescens Infections in Neonatal Intensive Care Units (NICUs). Int. J. Environ. Res. Public Health 2019, 16, 610. [Google Scholar] [CrossRef] [Green Version]
- Yeo, K.T.; Octavia, S.; Lim, K.; Lin, C.; Lin, R.; Thoon, K.C.; Tee, N.W.S.; Yung, C.F. Serratia Marcescens in the Neonatal Intensive Care Unit: A Cluster Investigation Using Molecular Methods. J. Infect. Public Health 2020, 13, 1006–1011. [Google Scholar] [CrossRef] [PubMed]
- Mohzari, Y.; Aljobair, F.; Alrashed, A.; Asdaq, S.M.B.; Alshuraim, R.A.; Asfour, S.S.; Al-Mouqdad, M.M.; Bamogaddam, R.F.; Al-Anazi, D.; Zeilinger, C.E.; et al. Safety and Efficacy of Daptomycin in Neonates with Coagulase-Negative Staphylococci: Case Series Analysis. Antibiotics 2021, 10, 168. [Google Scholar] [CrossRef] [PubMed]
- Polin, R.A.; Denson, S.; Brady, M.T.; Papile, L.A.; Baley, J.E.; Carlo, W.A.; Cummings, J.J.; Kumar, P.; Tan, R.C.; Watterberg, K.L.; et al. Epidemiology and Diagnosis of Health Care—Associated Infections in the NICU. Pediatrics 2012, 129, e1104–e1109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hooven, T.A.; Polin, R.A. Healthcare-Associated Infections in the Hospitalized Neonate: A Review. Early Hum. Dev. 2014, 90, S4. [Google Scholar] [CrossRef] [PubMed]
- Kusari, A.; Han, A.M.; Virgen, C.A.; Matiz, C.; Rasmussen, M.; Friedlander, S.F.; Eichenfield, D.Z. Evidence-Based Skin Care in Preterm Infants. Pediatr. Dermatol. 2019, 36, 16–23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Collins, A.; Weitkamp, J.H.; Wynn, J.L. Why Are Preterm Newborns at Increased Risk of Infection? Arch. Dis. Child Fetal Neonatal. Ed. 2018, 103, F391–F394. [Google Scholar] [CrossRef]
- Levy, O. Innate Immunity of the Newborn: Basic Mechanisms and Clinical Correlates. Nat. Rev. Immunol. 2007, 7, 379–390. [Google Scholar] [CrossRef]
- Sampah, M.E.S.; Hackam, D.J. Prenatal Immunity and Influences on Necrotizing Enterocolitis and Associated Neonatal Disorders. Front. Immunol. 2021, 12, 650709. [Google Scholar] [CrossRef] [PubMed]
- Rangelova, V.R.; Raycheva, R.D.; Kevorkyan, A.K.; Krasteva, M.B.; Kalchev, Y.I. Ventilator-Associated Pneumonia in Neonates Admitted to a Tertiary Care NICU in Bulgaria. Front. Pediatr. 2022, 10, 909217. [Google Scholar] [CrossRef]
- Borghesi, A.; Stronati, M. Strategies for the Prevention of Hospital-Acquired Infections in the Neonatal Intensive Care Unit. J. Hosp. Infect. 2008, 68, 293–300. [Google Scholar] [CrossRef]
- Mohammed, D.; el Seifi, O.S. Bacterial Nosocomial Infections in Neonatal Intensive Care Unit, Zagazig University Hospital, Egypt. Egypt. Pediatr. Assoc. Gaz. 2014, 62, 72–79. [Google Scholar] [CrossRef] [Green Version]
- Dal-Bó, K.; Da Silva, R.M.; Sakae, T. Nosocomial Infections in a Neonatal Intensive Care Unit in South Brazil. Rev. Bras. De Ter. Intensiv. 2012, 24, 381–385. [Google Scholar] [CrossRef]
- Tzialla, C.; Borghesi, A.; Serra, G.; Stronati, M.; Corsello, G. Antimicrobial Therapy in Neonatal Intensive Care Unit. Ital. J. Pediatr. 2015, 41, 27. [Google Scholar] [CrossRef] [Green Version]
- Migliara, G.; di Paolo, C.; Barbato, D.; Baccolini, V.; Salerno, C.; Nardi, A.; Alessandri, F.; Giordano, A.; Tufi, D.; Marinelli, L.; et al. Multimodal Surveillance of Healthcare Associated Infections in an Intensive Care Unit of a Large Teaching Hospital. Ann. Ig 2019, 31, 399–413. [Google Scholar] [CrossRef]
- Angelozzi, A.; Caminada, S.; Dorelli, B.; Sindoni, A.; Baccolini, V.; di Paolo, C.; Mele, A.; Salvatori, L.M.; Alessandri, F.; Marzuillo, C.; et al. Knowledge, Attitude, Barriers, Professional Behaviour and Possible Interventions: A Survey on Healthcareassociated Infections among the Healthcare Workers of an Intensive Care Unit in a Large Teaching Hospital in Rome. Ann. Ig 2021, 33, 628–643. [Google Scholar] [CrossRef] [PubMed]
- Allegranzi, B.; Pittet, D. Role of Hand Hygiene in Healthcare-Associated Infection Prevention. J. Hosp. Infect. 2009, 73, 305–315. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Period | |||||
|---|---|---|---|---|---|
| I | II | III | IV | ||
| 1 March 2018 to 28 February 2019 | 1 March 2019 to 29 February 2020 | 1 March 2020 to 28 February 2021 | 1 March 2021 to 28 February 2022 | p-Value * | |
| Patients, N | 133 | 148 | 90 | 132 | |
| Total observation time, patient days | 2038 | 1999 | 1629 | 1925 | |
| Length of NICU stay in days, mean (SD) | 15.3 (15.8) | 13.5 (15.6) | 18.1 (21.7) | 14.6 (15.6) | 0.470 |
| Sex, N (%) | 0.440 | ||||
| Female | 61 (45.9) | 74 (50.0) | 38 (42.2) | 54 (40.9) | |
| Male | 72 (54.1) | 74 (50.0) | 52 (57.8) | 78 (59.1) | |
| Gestational age in weeks, mean (SD) (N = 499) | 32.9 (4.3) | 33.5 (4.0) | 32.8 (4.2) | 33.6 (3.7) | 0.300 |
| Birth weight in grams, mean (SD) | 1919.9 (885.4) | 2056.1 (871.6) | 1866.6 (881.1) | 2025.7 (764.1) | 0.180 |
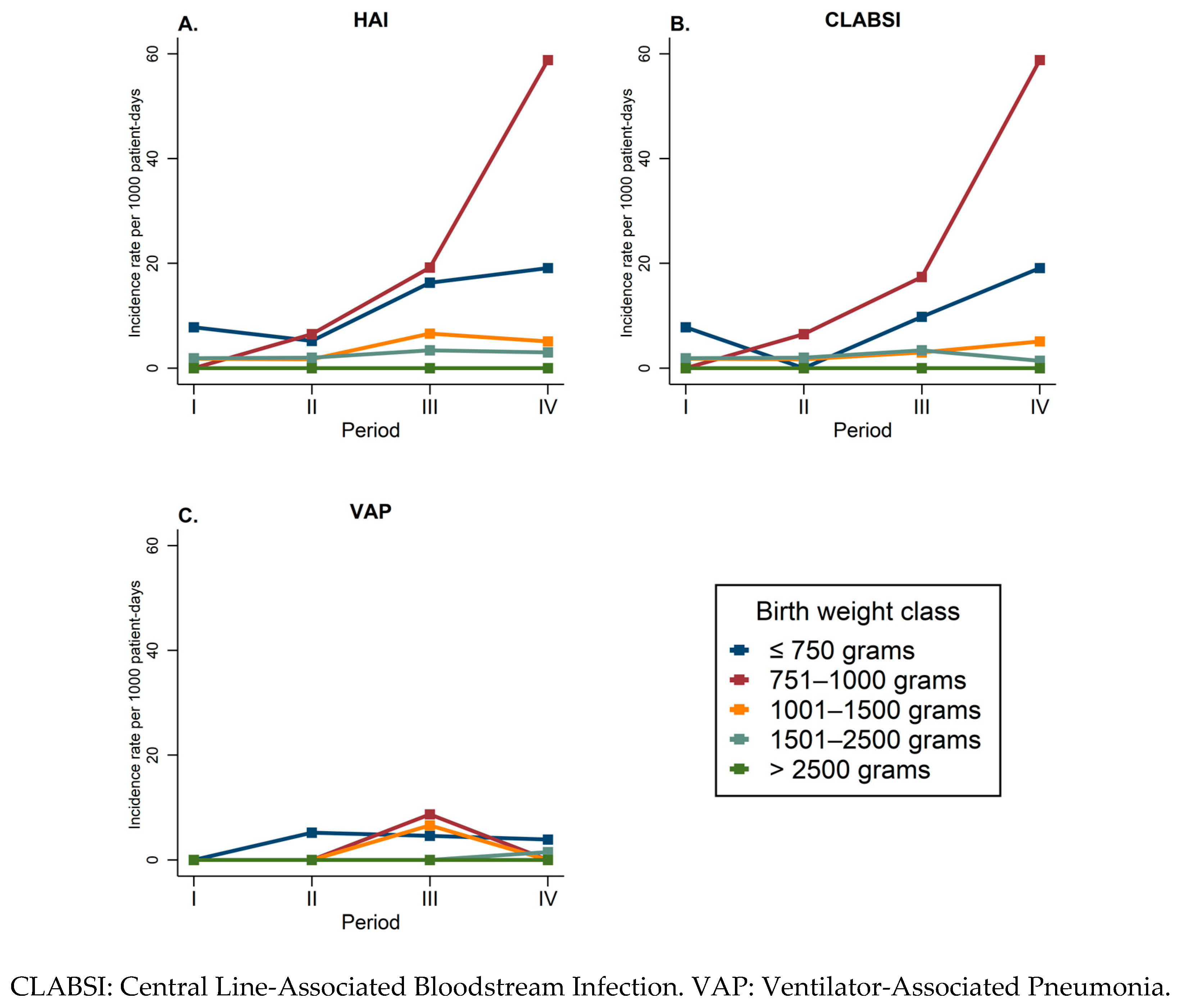
| Birth weight class, N (%) | 0.450 | ||||
| ≤750 g | 7 (5.3) | 6 (4.1) | 9 (10.0) | 8 (6.1) | |
| 751–1000 g | 8 (6.0) | 8 (5.4) | 6 (6.7) | 1 (0.8) | |
| 1001–1500 g | 32 (24.1) | 29 (19.6) | 19 (21.1) | 27 (20.5) | |
| 1501–2500 g | 56 (42.1) | 63 (42.6) | 36 (40.0) | 61 (46.2) | |
| >2500 g | 30 (22.6) | 42 (28.4) | 20 (22.2) | 35 (26.5) | |
| Delivery, N (%) | 0.810 | ||||
| Spontaneous | 23 (17.4) | 26 (17.8) | 12 (13.5) | 20 (15.4) | |
| Cesarean section | 109 (82.6) | 120 (82.2) | 77 (86.5) | 110 (84.6) | |
| Preterm birth, N (%) | 105 (78.9) | 114 (77.0) | 74 (82.2) | 106 (80.3) | 0.800 |
| Twin pregnancy, N (%) | 22 (16.5) | 26 (17.6) | 25 (27.8) | 33 (25.0) | 0.094 |
| Respiratory distress syndrome, N (%) | 60 (45.1) | 79 (53.4) | 55 (61.1) | 83 (62.9) | 0.018 |
| Use of central line, N (%) | 93 (69.9) | 96 (64.9) | 53 (58.9) | 62 (47.0) | <0.001 |
| Cumulative days of central line, mean (SD) (N = 304) | 11.9 (10.1) | 13.3 (16.5) | 19.6 (21.4) | 13.9 (14.8) | 0.350 |
| Use of mechanical ventilation, N (%) | 34 (25.6) | 38 (25.7) | 21 (23.3) | 13 (9.8) | 0.003 |
| Cumulative days of mechanical ventilation, mean (SD) (N = 106) | 7.6 (8.5) | 8.6 (15.3) | 14.7 (20.4) | 10.8 (11.7) | 0.370 |
| Use of ampicillin, N (%) | 107 (80.5) | 116 (78.4) | 67 (74.4) | 97 (73.5) | 0.510 |
| Cumulative days of ampicillin use, mean (SD) (N = 387) | 6.9 (2.8) | 6.8 (3.1) | 6.4 (2.7) | 6.0 (2.7) | 0.093 |
| Use of netilmicin, N (%) | 102 (76.7) | 102 (68.9) | 61 (67.8) | 94 (71.2) | 0.420 |
| Cumulative days of netilmicin use, mean (SD) (N = 359) | 5.3 (2.2) | 5.5 (2.5) | 5.8 (2.5) | 4.6 (2.3) | <0.001 |
| Use of fluconazole, N (%) | 18 (13.5) | 14 (9.5) | 15 (16.7) | 9 (6.8) | 0.091 |
| Cumulative days of fluconazole use, mean (SD) (N = 56) | 17.3 (12.0) | 30.1 (19.5) | 34.2 (19.1) | 22.2 (16.4) | 0.043 |
| NICU deaths, N (%) | 5 (3.8) | 7 (4.7) | 2 (2.2) | 4 (3.0) | 0.760 |
| NICU mortality, rate × 1000 patient days (95% CI) | 2.5 (1.0–5.9) | 3.5 (1.7–7.3) | 1.2 (0.3–4.9) | 2.1 (0.8–5.5) | |
| Period | |||||
|---|---|---|---|---|---|
| I | II | III | IV | ||
| 1 March 2018 to 28 February 2019 | 1 March 2019 to 29 February 2020 | 1 March 2020 to 28 February 2021 | 1 March 2021 to 28 February 2022 | p-Value * | |
| Patients, N | 133 | 148 | 90 | 132 | |
| Patients with at least one HAI, N (%) | 4 (3.0) | 5 (3.4) | 10 (11.1) | 9 (6.8) | 0.034 |
| Patients with at least one CLABSI, N (%) | 4 (3.0) | 4 (2.7) | 8 (8.9) | 8 (6.1) | 0.100 |
| Patients with at least one VAP, N (%) | 0 (0.0) | 1 (0.7) | 5 (5.6) | 2 (1.5) | 0.007 |
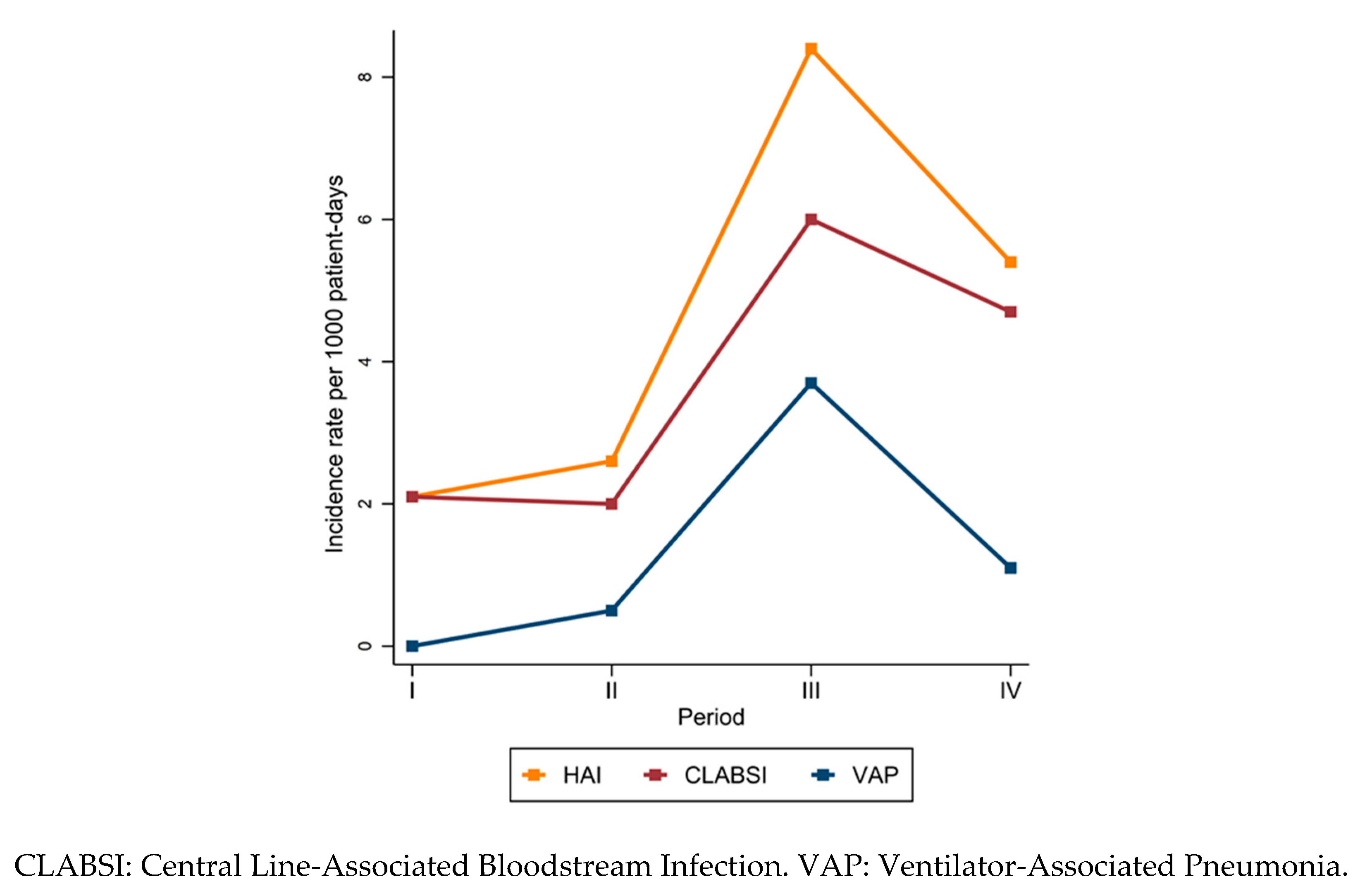
| HAIs, N | 4 | 5 | 16 | 11 | |
| Type of HAI, N (%) | 0.130 | ||||
| CLABSI | 4 (100.0) | 4 (80.0) | 8 (50.0) | 9 (81.8) | |
| VAP | 0 (0.0) | 1 (20.0) | 8 (50.0) | 2 (18.2) | |
| Incidence rate for first HAI × 1000 patient days (95% CI) | 2.1 (0.8–5.5) | 2.6 (1.1–6.3) | 8.4 (4.5–15.6) | 5.4 (2.8–10.4) | |
| Incidence rate for recurrent HAIs × 1000 patient days (95% CI) | 2.0 (0.7–5.2) | 2.5 (1.0–6.0) | 9.4 (5.5–16.0) | 5.6 (3.1–10.3) | |
| aHR | 95% CI | p-Value | |
|---|---|---|---|
| Period | |||
| II (1 March 2019 to 29 February 2020) | Ref. | ||
| I (1 March 2018 to 28 February 2019) | 1.62 | 0.34–7.67 | 0.544 |
| III (1 March 2020 to 28 February 2021) | 4.88 | 1.33–17.97 | 0.017 |
| IV (1 March 2021 to 28 February 2022) | 6.45 | 1.53–27.24 | 0.011 |
| Sex | |||
| Female | Ref. | ||
| Male | 1.08 | 0.49–2.37 | 0.843 |
| Delivery | |||
| Spontaneous | Ref. | ||
| Cesarean section | 0.73 | 0.27–1.96 | 0.537 |
| Birth weight, grams | 0.99 | 0.98–0.99 | 0.030 |
| Respiratory distress syndrome | |||
| No | Ref. | ||
| Yes | 1.86 | 0.76–4.52 | 0.172 |
| Mechanical ventilation use, days | 1.04 | 1.02–1.06 | <0.001 |
| Previous use of netilmicin | |||
| No | Ref. | ||
| Yes | 5.23 | 0.65–42.40 | 0.121 |
| Previous use of fluconazole | |||
| No | Ref. | ||
| Yes | 0.89 | 0.33–2.44 | 0.828 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ceparano, M.; Sciurti, A.; Isonne, C.; Baccolini, V.; Migliara, G.; Marzuillo, C.; Natale, F.; Terrin, G.; Villari, P.; The Collaborating Group. Incidence of Healthcare-Associated Infections in a Neonatal Intensive Care Unit before and during the COVID-19 Pandemic: A Four-Year Retrospective Cohort Study. J. Clin. Med. 2023, 12, 2621. https://doi.org/10.3390/jcm12072621
Ceparano M, Sciurti A, Isonne C, Baccolini V, Migliara G, Marzuillo C, Natale F, Terrin G, Villari P, The Collaborating Group. Incidence of Healthcare-Associated Infections in a Neonatal Intensive Care Unit before and during the COVID-19 Pandemic: A Four-Year Retrospective Cohort Study. Journal of Clinical Medicine. 2023; 12(7):2621. https://doi.org/10.3390/jcm12072621
Chicago/Turabian StyleCeparano, Mariateresa, Antonio Sciurti, Claudia Isonne, Valentina Baccolini, Giuseppe Migliara, Carolina Marzuillo, Fabio Natale, Gianluca Terrin, Paolo Villari, and The Collaborating Group. 2023. "Incidence of Healthcare-Associated Infections in a Neonatal Intensive Care Unit before and during the COVID-19 Pandemic: A Four-Year Retrospective Cohort Study" Journal of Clinical Medicine 12, no. 7: 2621. https://doi.org/10.3390/jcm12072621