

Developing a Warning Model of Potentially Inappropriate Medications in Older Chinese Outpatients in Tertiary Hospitals: A Machine-Learning Study

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Setting and the Study Population
2.2. Data Collection
2.3. Evaluation Criteria
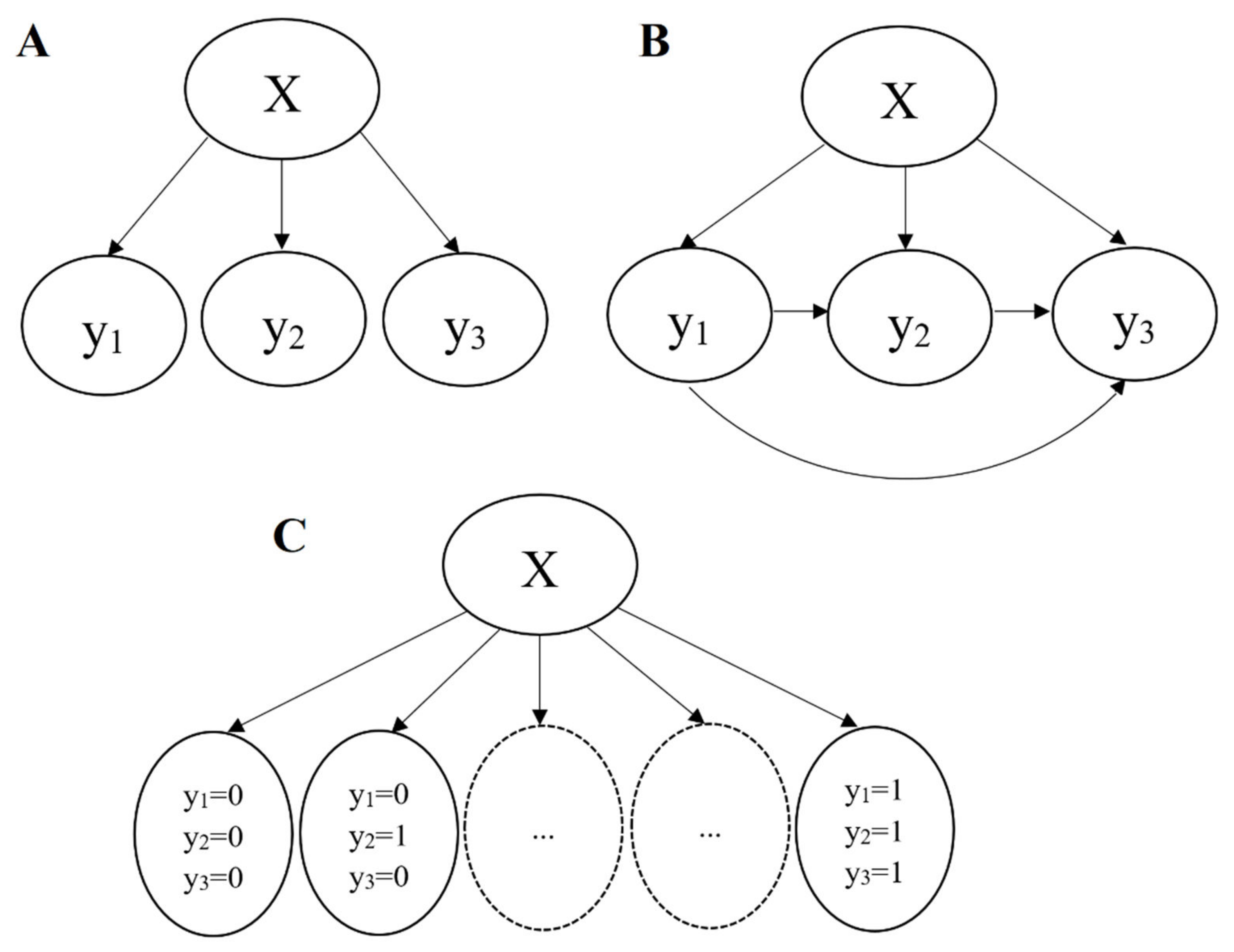
2.4. Multilabel Classification
2.5. Model Development
2.6. Model Evaluation Metrics
2.7. Statistical Analysis
3. Results
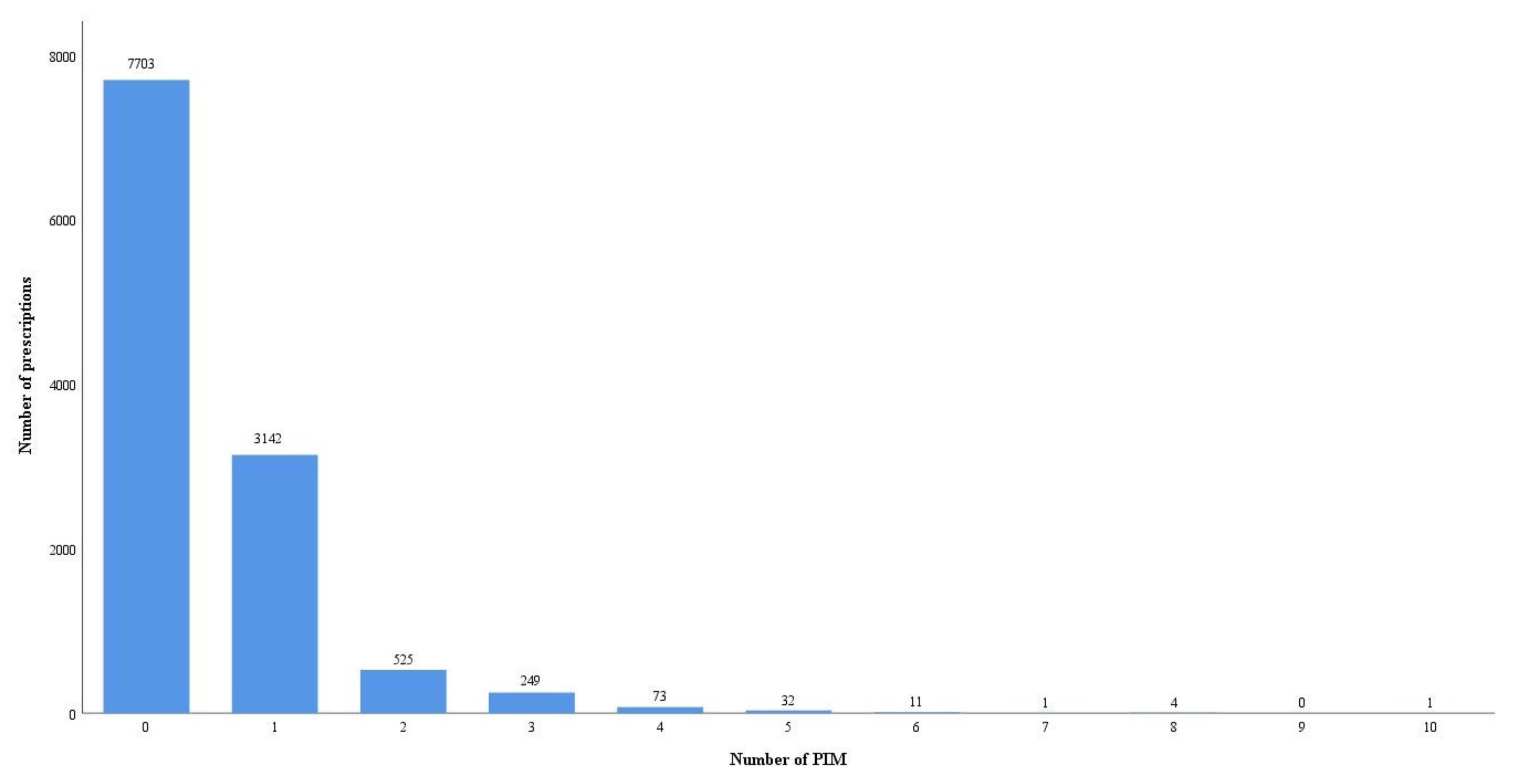
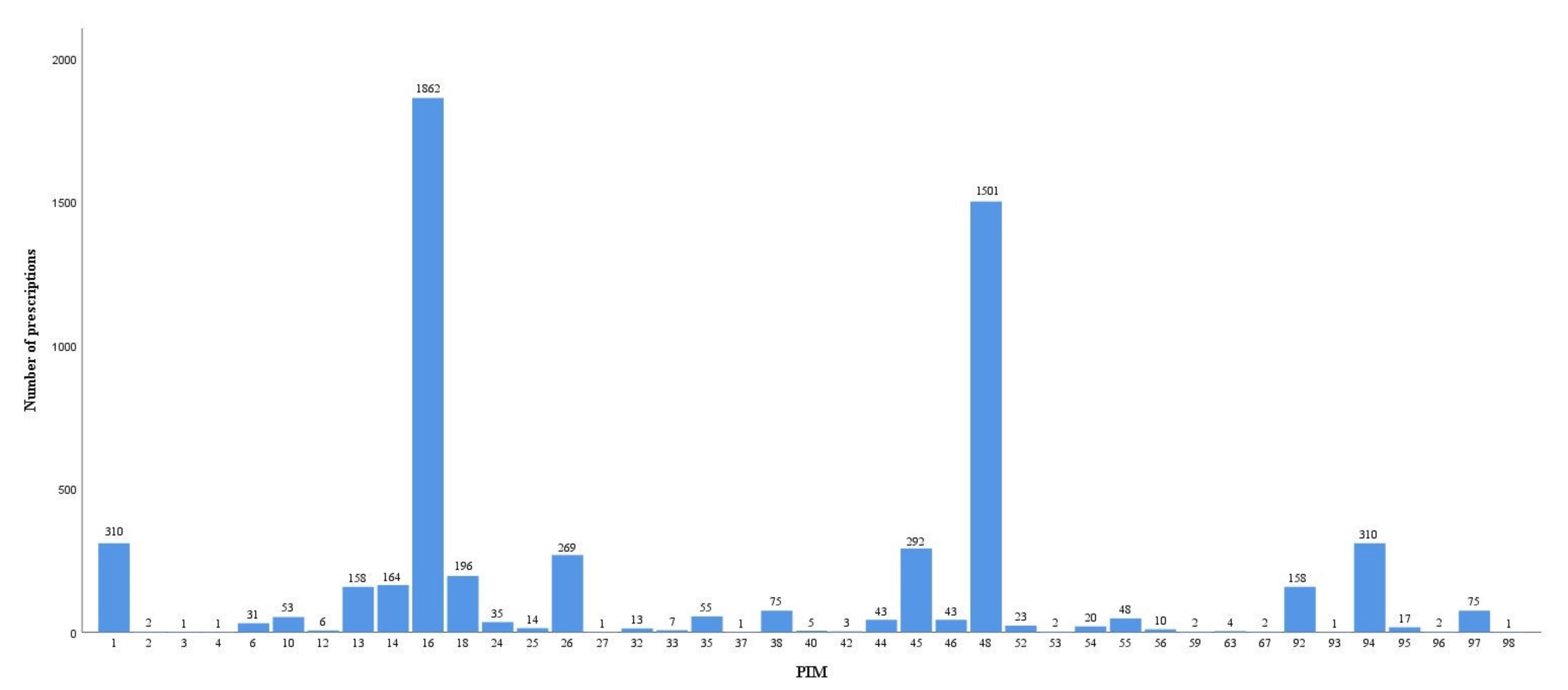
3.1. Study Population
- Potentially inappropriate medication
3.2. Model Performance
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kang, J.H.; Kim, H.; Kim, J.; Seo, J.H.; Cha, S.; Oh, H.; Kim, K.; Park, S.J.; Kim, E.; Kong, S.; et al. Interaction of genetic and environmental factors for body fat mass control: Observational study for lifestyle modification and genotyping. Sci. Rep. 2021, 11, 13180. [Google Scholar] [CrossRef]
- Wang, Y.; Zhou, C. Promoting social engagement of the elderly to cope with aging of the Chinese population. Biosci. Trends. 2020, 14, 310–313. [Google Scholar] [CrossRef]
- Endocrinology and Metabolism Branch of Chinese Association of Geriatric Research; Committee of Clinical Toxicology of Chinese Society of Toxicology. Expert consensus on risk management of polypharmacy in elderly. Chin. Gen. Pract. 2018, 21, 3533–3544. [Google Scholar]
- Sum, G.; Hone, T.; Atun, R.; Millett, C.; Suhrcke, M.; Mahal, A.; Koh, G.C.; Lee, J.T. Multimorbidity and out-of-pocket expenditure on medicines: A systematic review. BMJ Glob. Health. 2018, 3, e000505. [Google Scholar] [CrossRef] [Green Version]
- Dimitrow, M.S.; Airaksinen, M.S.; Kivelä, S.L.; Lyles, A.; Leikola, S.N. Comparison of prescribing criteria to evaluate the appropriateness of drug treatment in individuals aged 65 and older: A systematic review. J. Am. Geriatr. Soc. 2011, 59, 1521–1530. [Google Scholar] [CrossRef]
- Renom-Guiteras, A.; Meyer, G.; Thürmann, P.A. The EU (7)-PIM list: A list of potentially inappropriate medications for older people consented by experts from seven European countries. Eur. J. Clin. Pharmacol. 2015, 71, 861–875. [Google Scholar] [CrossRef] [Green Version]
- Hedna, K.; Hakkarainen, K.M.; Gyllensten, H.; Jönsson, A.K.; Petzold, M.; Hägg, S. Potentially inappropriate prescribing and adverse drug reactions in the elderly: A population-based study. Eur. J. Clin. Pharmacol. 2015, 71, 1525–1533. [Google Scholar] [CrossRef] [Green Version]
- Morin, L.; Laroche, M.L.; Texier, G.; Johnell, K. Prevalence of Potentially Inappropriate Medication Use in Older Adults Living in Nursing Homes: A Systematic Review. J. Am. Med. Dir. Assoc. 2016, 17, 862.e1–862.e9. [Google Scholar] [CrossRef] [Green Version]
- Nyborg, G.; Straand, J.; Brekke, M. Inappropriate prescribing for the elderly--a modern epidemic? Eur. J. Clin. Pharmacol. 2012, 68, 1085–1094. [Google Scholar] [CrossRef] [Green Version]
- Opondo, D.; Eslami, S.; Visscher, S.; de-Rooij, S.E.; Verheij, R.; Korevaar, J.C.; Abu-Hanna, A. Inappropriateness of medication prescriptions to elderly patients in the primary care setting: A systematic review. PLoS ONE 2012, 7, e43617. [Google Scholar] [CrossRef]
- Corsonello, A.; Pedone, C.; Incalzi, R.A. Age-related pharmacokinetic and pharmacodynamic changes and related risk of adverse drug reactions. Curr. Med. Chem. 2010, 17, 571–584. [Google Scholar] [CrossRef]
- Reich, O.; Rosemann, T.; Rapold, R.; Blozik, E.; Senn, O. Potentially inappropriate medication use in older patients in Swiss managed care plans: Prevalence, determinants and association with hospitalization. PLoS ONE 2014, 9, e105425. [Google Scholar] [CrossRef] [Green Version]
- Klarin, I.; Wimo, A.; Fastbom, J. The association of inappropriate drug use with hospitalisation and mortality: A population-based study of the very old. Drugs Aging 2005, 22, 69–82. [Google Scholar] [CrossRef]
- Lau, D.T.; Kasper, J.D.; Potter, D.E.; Lyles, A.; Bennett, R.G. Hospitalization and death associated with potentially inappropriate medication prescriptions among elderly nursing home residents. Arch. Intern. Med. 2005, 165, 68–74. [Google Scholar] [CrossRef]
- Muhlack, D.C.; Hoppe, L.K.; Weberpals, J.; Brenner, H.; Schöttker, B. The Association of Potentially Inappropriate Medication at Older Age With Cardiovascular Events and Overall Mortality: A Systematic Review and Meta-Analysis of Cohort Studies. J. Am. Med. Dir. Assoc. 2017, 18, 211–220. [Google Scholar] [CrossRef]
- 2019 American Geriatrics Society Beers Criteria Update Expert Panel. American Geriatrics Society 2019 Updated AGS Beers Criteria® for potentially inappropriate medication use in older adults. J. Am. Geriatr. Soc. 2019, 67, 674–694. [Google Scholar] [CrossRef]
- Kamal, H.; Lopez, V.; Sheth, S.A. Machine learning in acute ischemic stroke neuroimaging. Front. Neurol. 2018, 9, 945. [Google Scholar] [CrossRef]
- Lan, K.; Wang, D.T.; Fong, S.; Liu, L.S.; Wong, K.; Dey, N. A survey of data mining and deep learning in bioinformatics. J. Med. Syst. 2018, 42, 139. [Google Scholar] [CrossRef]
- Li, C.; Sun, L.; Peng, D.; Subramani, S.; Nicolas, S.C. A multi-label classification system for anomaly classification in electrocardiogram. Health Inf. Sci. Syst. 2022, 10, 19. [Google Scholar] [CrossRef]
- Tian, F.; Li, H.; Chen, Z.; Xu, T. Potentially inappropriate medications in Chinese older outpatients in tertiary hospitals according to Beers criteria: A cross-sectional study. Int. J. Clin. Pract. 2021, 75, e14348. [Google Scholar] [CrossRef]
- Boutell, M.; Luo, J.; Shen, X.; Brown, C. Learning multi-label scene classification. Pattern. Recognit. 2004, 37, 1757–1771. [Google Scholar] [CrossRef] [Green Version]
- Rokach, L.; Schclar, A.; Itach, E. Ensemble methods for multi-label classification. Expert Syst. Appl. 2014, 41, 7507–7523. [Google Scholar] [CrossRef] [Green Version]
- Read, J.; Pfahringer, B.; Holmes, G.; Frank, E. Classifier chains: A review and perspectives. J. Artif. Intell. Res. 2021, 70, 683–718. [Google Scholar] [CrossRef]
- 24 Yap, X.H.; Raymer, M. Multi-label classification and label dependence in in silico toxicity prediction. Toxicol. In Vitro 2021, 74, 105157. [Google Scholar] [CrossRef]
- Ren, Y.; Chakraborty, T.; Doijad, S.; Falgenhauer, L.; Falgenhauer, J.; Goesmann, A.; Schwengers, O.; Heider, D. Multi-label classification for multi-drug resistance prediction of Escherichia coli. Comput. Struct. Biotechnol. J. 2022, 20, 1264–1270. [Google Scholar] [CrossRef]
- Tsoumakas, G.; Vlahavas, I. Random k-Labelsets: An ensemble method for multilabel classification. In Machine Learning: ECML 2007; Kok, J.N., Koronacki, J., Mantaras, R.L.d., Matwin, S., Mladenič, D., Eds.; Springer: Berlin/Heidelberg, Germany, 2007; pp. 406–417. [Google Scholar]
- Elkafrawy, P.; Mausad, A.; Esmail, H. Experimental comparison of methods for multi-label classifcation in diferent application domains. Int. J. Comput. Appl. 2015, 114, 1–9. [Google Scholar]
- Ashraf, N.; Khan, L.; Butt, S.; Chang, H.T.; Sidorov, G.; Gelbukh, A. Multi-label emotion classification of Urdu tweets. Peer J. Comput. Sci. 2022, 8, e896. [Google Scholar] [CrossRef]
- Fick, D.M.; Mion, L.C.; Beers, M.H.; Waller, J.L. Health outcomes associated with potentially inappropriate medication use in older adults. Res. Nurs. Health 2008, 31, 42–51. [Google Scholar] [CrossRef]
- Hamaker, M.E.; Wildes, T.M.; Rostoft, S. Time to stop saying geriatric assessment is too time-consuming. J. Clin. Oncol. 2017, 35, 2871–2874. [Google Scholar] [CrossRef] [Green Version]
- Mulder-Wildemors, L.G.M.; Heringa, M.; Floor-Schreudering, A.; Jansen, P.A.F.; Bouvy, M.L. Reducing Inappropriate Drug Use in Older Patients by Use of Clinical Decision Support in Community Pharmacy: A Mixed-Methods Evaluation. Drugs Aging 2020, 37, 115–123. [Google Scholar] [CrossRef]
- Prasert, V.; Shono, A.; Chanjaruporn, F.; Ploylearmsang, C.; Boonnan, K.; Khampetdee, A.; Akazawa, M. Effect of a computerized decision support system on potentially inappropriate medication prescriptions for elderly patients in Thailand. J. Eval. Clin. Pract. 2019, 25, 514–520. [Google Scholar] [CrossRef]
- Frutos, E.; Kakazu, M.; Tajerian, M.; Gaiera, A.; Rubin, L.; Otero, C.; Luna, D. Clinical Decision Support System for PIM in Elderly Patients: Implementation and Initial Evaluation in Ambulatory Care. Stud. Health Technol. Inform. 2022, 294, 475–479. [Google Scholar]
- Syeda-Mahmood, T. Role of big data and machine learning in diagnostic decision support in radiology. J. Am. Coll. Radiol. 2018, 15, 569–576. [Google Scholar] [CrossRef]
- Takada, M.; Sugimoto, M.; Masuda, N.; Iwata, H.; Kuroi, K.; Yamashiro, H.; Ohno, S.; Ishiguro, H.; Inamoto, T.; Toi, M. Prediction of postoperative disease-free survival and brain metastasis for HER2-positive breast cancer patients treated with neoadjuvant chemotherapy plus trastuzumab using a machine learning algorithm. Breast. Cancer Res. Treat. 2018, 172, 611–618. [Google Scholar] [CrossRef]
- Becker, A.S.; Marcon, M.; Ghafoor, S.; Wurnig, M.C.; Frauenfelder, T.; Boss, A. Deep learning in mammography: Diagnostic accuracy of a multipurpose image analysis software in the detection of breast cancer. Investig. Radiol. 2017, 52, 434–440. [Google Scholar] [CrossRef]
- Egan, M.; Moride, Y.; Wolfson, C.; Monette, J. Long-term continuous use of benzodiazepines by older adults in Quebec: Prevalence, incidence and risk factors. J. Am. Geriatr. Soc. 2000, 48, 811–816. [Google Scholar] [CrossRef]
- Pourmand, A.; Lombardi, K.M.; Roberson, J.; Mazer-Amirshahi, M. Patterns of benzodiazepine administration and prescribing to older adults in U.S. emergency departments. Aging Clin. Exp. Res. 2020, 32, 2621–2628. [Google Scholar] [CrossRef]
- Béland, S.G.; Préville, M.; Dubois, M.F.; Lorrain, D.; Voyer, P.; Bossé, C.; Grenier, S.; Moride, Y.; Scientific Committee of the ESA Study. The association between length of benzodiazepine use and sleep quality in older population. Int. J. Geriatr. Psychiatry 2011, 26, 908–915. [Google Scholar] [CrossRef]
- Avidan, A.Y.; Palmer, L.A.; Doan, J.F.; Baran, R.W. Insomnia medication use and the probability of an accidental event in an older adult population. Drug. Healthc. Patient. Saf. 2010, 2, 225–232. [Google Scholar] [CrossRef] [Green Version]
- Schepis, T.S.; Simoni-Wastila, L.; McCabe, S.E. Prescription opioid and benzodiazepine misuse is associated with suicidal ideation in older adults. Int. J. Geriatr. Psychiatry 2019, 34, 122–129. [Google Scholar] [CrossRef] [Green Version]
- Praharaj, S.K.; Gupta, R.; Gaur, N. Clinical practice guideline on management of sleep disorders in the elderly. Indian J. Psychiatry 2018, 60, S383–S396. [Google Scholar] [CrossRef]
- Alessi, C.; Vitiello, M.V. Insomnia (primary) in older people: Non-drug treatments. BMJ. Clin. Evid. 2015, 2015, 2302. [Google Scholar]
- Barber, J.; McKeever, T.M.; McDowell, S.E.; Clayton, J.A.; Ferner, R.E.; Gordon, R.D.; Stowasser, M.; O’Shaughnessy, K.M.; Hall, I.P.; Glover, M. A systematic review and meta-analysis of thiazide-induced hyponatraemia: Time to reconsider electrolyte monitoring regimens after thiazide initiation? Br. J. Clin. Pharmacol. 2015, 79, 566–577. [Google Scholar] [CrossRef] [Green Version]
- Inaguma, D.; Kitagawa, W.; Hayashi, H.; Kanoh, T.; Kurata, K.; Kumon, S. Three cases of severe hyponatremia under taking selective serotonin reuptake inhibitor (SSRI). Nihon Jinzo Gakkai Shi 2000, 42, 644–648. [Google Scholar]
- Schouten, W.E.; Sepers, J.M. Hyponatraemia associated with the use of a selective serotonin-reuptake inhibitor in an older patient. Age Ageing 2001, 30, 94. [Google Scholar] [CrossRef] [Green Version]
- Finfgeld, D.L. SSRI-related hyponatremia among aging adults. J. Psychosoc. Nurs. Ment. Health Serv. 2003, 41, 12–16. [Google Scholar] [CrossRef]
- Nahshoni, E.; Weizman, A.; Shefet, D.; Pik, N. A case of hyponatremia associated with escitalopram. J. Clin. Psychiatry 2004, 65, 1722. [Google Scholar] [CrossRef] [Green Version]
- Jacob, S.; Spinler, S.A. Hyponatremia associated with selective serotonin-reuptake inhibitors in older adults. Ann. Pharmacother. 2006, 40, 1618–1622. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variable | Total (n = 11,741) | Training Set (n = 9392) | Testing Set (n = 2349) | p |
|---|---|---|---|---|
| PIM | ||||
| Yes | 4038 | 3204 | 834 | 0.410 |
| No | 7703 | 6188 | 1515 | |
| Gender | ||||
| Male | 7030 | 5607 | 1423 | 0.981 |
| Female | 4711 | 3785 | 926 | |
| Age (years) | 78.69 ± 8.29 (65–119) | 78.71 ± 8.29 (65–103) | 78.69 ± 8.29 (65–119) | 0.935 |
| Number of diseases | 2.84 ± 2.73 (1–19) | 2.86 ± 2.75 (1–19) | 2.80 ± 2.69 (1–18) | 0.335 |
| Number of medications | 3.39 ± 2.59 (1–23) | 3.40 ± 2.59 (1–18) | 3.40 ± 2.62 (1–23) | 0.975 |
| Problem Transformation Method | Classification Model | Accuracy | Precision | Recall | F1 | ss Acc | hm |
|---|---|---|---|---|---|---|---|
| BR | RF | 0.9332 | 0.7871 | 0.5415 | 0.6121 | 0.9293 | 0.0023 |
| LightGBM | 0.9293 | 0.6911 | 0.7005 | 0.6778 | 0.9285 | 0.0022 | |
| XGBoost | 0.9706 | 0.9000 | 0.8367 | 0.8624 | 0.9698 | 0.0008 | |
| CatBoost | 0.9762 | 0.9098 | 0.8685 | 0.8880 | 0.9753 | 0.0007 | |
| DF | 0.9617 | 0.8095 | 0.7796 | 0.7876 | 0.9600 | 0.0011 | |
| TabNet | 0.8966 | 0.6356 | 0.5449 | 0.5719 | 0.8923 | 0.0035 | |
| CC | RF | 0.9281 | 0.7994 | 0.5457 | 0.6208 | 0.9276 | 0.0025 |
| LightGBM | 0.9395 | 0.8137 | 0.7856 | 0.7859 | 0.9378 | 0.0018 | |
| XGBoost | 0.9715 | 0.9228 | 0.8712 | 0.8933 | 0.9706 | 0.0008 | |
| CatBoost | 0.9783 | 0.9218 | 0.8934 | 0.9069 | 0.9779 | 0.0006 | |
| DF | 0.9621 | 0.8194 | 0.8026 | 0.8090 | 0.9608 | 0.0011 | |
| TabNet | 0.8859 | 0.7043 | 0.5592 | 0.5939 | 0.8765 | 0.0039 | |
| LP | RF | 0.9204 | 0.7903 | 0.5491 | 0.6309 | 0.9195 | 0.0031 |
| LightGBM | 0.7220 | 0.3219 | 0.3779 | 0.3109 | 0.7088 | 0.0209 | |
| XGBoost | 0.9434 | 0.8523 | 0.5646 | 0.6252 | 0.9425 | 0.0020 | |
| CatBoost | 0.9447 | 0.7601 | 0.6224 | 0.6764 | 0.9442 | 0.0020 | |
| DF | 0.9421 | 0.7683 | 0.6556 | 0.7013 | 0.9413 | 0.0021 | |
| TabNet | 0.8889 | 0.5762 | 0.4474 | 0.4618 | 0.8710 | 0.0067 |
| No of PIM | Sample, n | Precision | Recall | F1 |
|---|---|---|---|---|
| 1 | 63 | 1.0000 | 0.9841 | 0.9920 |
| 2 | 0 | 0.0000 | 0.0000 | 0.0000 |
| 3 | 0 | 0.0000 | 0.0000 | 0.0000 |
| 4 | 0 | 0.0000 | 0.0000 | 0.0000 |
| 6 | 7 | 1.0000 | 0.8571 | 0.9231 |
| 10 | 9 | 1.0000 | 0.8889 | 0.9412 |
| 12 | 1 | 0.0000 | 0.0000 | 0.0000 |
| 13 | 33 | 1.0000 | 1.0000 | 1.0000 |
| 14 | 36 | 1.0000 | 1.0000 | 1.0000 |
| 16 | 358 | 1.0000 | 1.0000 | 1.0000 |
| 18 | 43 | 1.0000 | 1.0000 | 1.0000 |
| 24 | 9 | 1.0000 | 0.5556 | 0.7143 |
| 25 | 3 | 1.0000 | 1.0000 | 1.0000 |
| 26 | 61 | 1.0000 | 1.0000 | 1.0000 |
| 27 | 1 | 0.0000 | 0.0000 | 0.0000 |
| 32 | 3 | 1.0000 | 1.0000 | 1.0000 |
| 33 | 0 | 0.0000 | 0.0000 | 0.0000 |
| 35 | 9 | 1.0000 | 0.5556 | 0.7143 |
| 37 | 1 | 0.0000 | 0.0000 | 0.0000 |
| 38 | 17 | 1.0000 | 0.5882 | 0.7407 |
| 40 | 0 | 0.0000 | 0.0000 | 0.0000 |
| 42 | 0 | 0.0000 | 0.0000 | 0.0000 |
| 44 | 3 | 1.0000 | 0.6667 | 0.8000 |
| 45 | 65 | 0.8772 | 0.7692 | 0.8197 |
| 46 | 9 | 0.8182 | 1.0000 | 0.9000 |
| 48 | 299 | 1.0000 | 1.0000 | 1.0000 |
| 52 | 3 | 1.0000 | 1.0000 | 1.0000 |
| 53 | 1 | 0.0000 | 0.0000 | 0.0000 |
| 54 | 6 | 1.0000 | 1.0000 | 1.0000 |
| 55 | 11 | 1.0000 | 0.8182 | 0.9000 |
| 56 | 2 | 0.0000 | 0.0000 | 0.0000 |
| 59 | 0 | 0.0000 | 0.0000 | 0.0000 |
| 64 | 1 | 1.0000 | 1.0000 | 1.0000 |
| 67 | 1 | 0.0000 | 0.0000 | 0.0000 |
| 92 | 33 | 1.0000 | 1.0000 | 1.0000 |
| 93 | 0 | 0.0000 | 0.0000 | 0.0000 |
| 94 | 63 | 1.0000 | 0.9841 | 0.9920 |
| 95 | 3 | 1.0000 | 1.0000 | 1.0000 |
| 96 | 0 | 0.0000 | 0.0000 | 0.0000 |
| 97 | 15 | 1.0000 | 1.0000 | 1.0000 |
| 98 | 0 | 0.0000 | 0.0000 | 0.0000 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hu, Q.; Tian, F.; Jin, Z.; Lin, G.; Teng, F.; Xu, T. Developing a Warning Model of Potentially Inappropriate Medications in Older Chinese Outpatients in Tertiary Hospitals: A Machine-Learning Study. J. Clin. Med. 2023, 12, 2619. https://doi.org/10.3390/jcm12072619
Hu Q, Tian F, Jin Z, Lin G, Teng F, Xu T. Developing a Warning Model of Potentially Inappropriate Medications in Older Chinese Outpatients in Tertiary Hospitals: A Machine-Learning Study. Journal of Clinical Medicine. 2023; 12(7):2619. https://doi.org/10.3390/jcm12072619
Chicago/Turabian StyleHu, Qiaozhi, Fangyuan Tian, Zhaohui Jin, Gongchao Lin, Fei Teng, and Ting Xu. 2023. "Developing a Warning Model of Potentially Inappropriate Medications in Older Chinese Outpatients in Tertiary Hospitals: A Machine-Learning Study" Journal of Clinical Medicine 12, no. 7: 2619. https://doi.org/10.3390/jcm12072619