
Endovascular Treatment for Acute Basilar Artery Occlusion: A Fragility Index Meta-Analysis
 , , , ,
, , , ,  , ,
, ,
Abstract
:1. Background
2. Methods
2.1. Standard Protocol Approvals, Registrations, and Patient Consents
2.2. Data Sources, Searches and Study Selection
2.3. Quality Control, Bias Assessment and Data Extraction
2.4. Outcomes
2.5. Statistical Analysis
3. Results
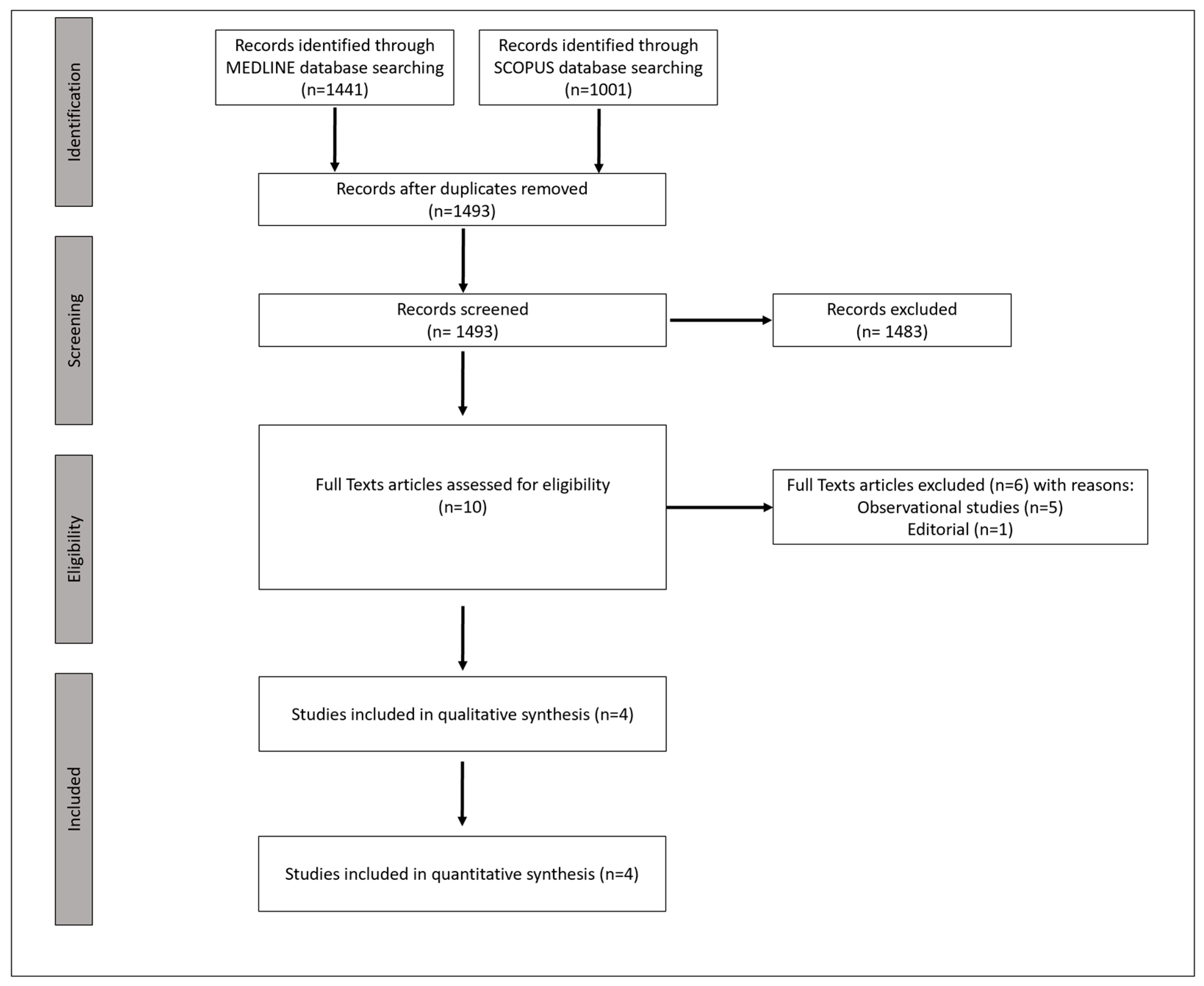
3.1. Literature Search and Included Studies
3.2. Quality Control of Included Studies
3.3. Quantitative Analyses
3.4. Primary Outcome
3.5. Secondary Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Trial Registration
References
- Tsivgoulis, G.; Safouris, A.; Katsanos, A.H.; Arthur, A.S.; Alexandrov, A.V. Mechanical thrombectomy for emergent large vessel occlusion: A critical appraisal of recent randomized controlled clinical trials. Brain Behav. 2016, 6, e00418. [Google Scholar] [CrossRef] [Green Version]
- Jadhav, A.P.; Desai, S.M.; Jovin, T.G. Indications for Mechanical Thrombectomy for Acute Ischemic Stroke: Current Guidelines and Beyond. Neurology 2021, 97, S126–S136. [Google Scholar] [CrossRef]
- Turc, G.; Bhogal, P.; Fischer, U.; Khatri, P.; Lobotesis, K.; Mazighi, M.; Schellinger, P.D.; Toni, D.; de Vries, J.; White, P.; et al. European Stroke Organisation (ESO)—European Society for Minimally Invasive Neurological Therapy (ESMINT) Guidelines on Mechanical Thrombectomy in Acute Ischaemic StrokeEndorsed by Stroke Alliance for Europe (SAFE). Eur. Stroke J. 2019, 4, 6–12. [Google Scholar] [CrossRef] [Green Version]
- Powers, W.J.; Rabinstein, A.A.; Ackerson, T.; Adeoye, O.M.; Bambakidis, N.C.; Becker, K.; Biller, J.; Brown, M.; Demaerschalk, B.M.; Hoh, B.; et al. Guidelines for the Early Management of Patients With Acute Ischemic Stroke: 2019 Update to the 2018 Guidelines for the Early Management of Acute Ischemic Stroke: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke 2019, 50, e344–e418. [Google Scholar]
- Albers, G.W.; Marks, M.P.; Kemp, S.; Christensen, S.; Tsai, J.P.; Ortega-Gutierrez, S.; McTaggart, R.A.; Torbey, M.T.; Kim-Tenser, M.; Leslie-Mazwi, T.; et al. Thrombectomy for Stroke at 6 to 16 Hours with Selection by Perfusion Imaging. New Engl. J. Med. 2018, 378, 708–718. [Google Scholar] [CrossRef] [PubMed]
- Nogueira, R.G.; Jadhav, A.P.; Haussen, D.C.; Bonafe, A.; Budzik, R.F.; Bhuva, P.; Yavagal, D.R.; Ribo, M.; Cognard, C.; Hanel, R.A.; et al. Thrombectomy 6 to 24 Hours after Stroke with a Mismatch between Deficit and Infarct. N. Engl. J. Med. 2018, 378, 11–21. [Google Scholar] [CrossRef]
- Sommer, P.; Posekany, A.; Serles, W.; Marko, M.; Scharer, S.; Fertl, E.; Ferrari, J.; Lang, W.; Vosko, M.; Szabo, S.; et al. Is Functional Outcome Different in Posterior and Anterior Circulation Stroke? Stroke 2018, 49, 2728–2732. [Google Scholar] [CrossRef] [PubMed]
- Schonewille, W.J.; Wijman, C.A.; Michel, P.; Rueckert, C.M.; Weimar, C.; Mattle, H.P.; Engelter, S.T.; Tanne, D.; Muir, K.W.; Molina, C.; et al. Treatment and outcomes of acute basilar artery occlusion in the Basilar Artery International Cooperation Study (BASICS): A prospective registry study. Lancet Neurol. 2009, 8, 724–730. [Google Scholar] [CrossRef]
- Katsanos, A.H.; Safouris, A.; Nikolakopoulos, S.; Mavridis, D.; Goyal, N.; Psychogios, M.N.; Magoufis, G.; Krogias, C.; Catanese, L.; Van Adel, B.; et al. Endovascular treatment for basilar artery occlusion: A systematic review and meta-analysis. Eur. J. Neurol. 2021, 28, 2106–2110. [Google Scholar] [CrossRef]
- Langezaal, L.C.; van der Hoeven, E.J.; Mont’Alverne, F.J.; de Carvalho, J.J.; Lima, F.O.; Dippel, D.W.; van der Lugt, A.; Lo, R.T.; Boiten, J.; Nijeholt, G.J.L.À.; et al. Endovascular Therapy for Stroke Due to Basilar-Artery Occlusion. New Engl. J. Med. 2021, 384, 1910–1920. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Dai, Q.; Ye, R.; Zi, W.; Liu, Y.; Wang, H.; Zhu, W.; Ma, M.; Yin, Q.; Li, M.; et al. Endovascular treatment versus standard medical treatment for vertebrobasilar artery occlusion (BEST): An open-label, randomised controlled trial. Lancet Neurol. 2020, 19, 115–122. [Google Scholar] [CrossRef]
- Tao, C.; Nogueira, R.G.; Zhu, Y.; Sun, J.; Han, H.; Yuan, G.; Wen, C.; Zhou, P.; Chen, W.; Zeng, G.; et al. Trial of Endovascular Treatment of Acute Basilar-Artery Occlusion. New Engl. J. Med. 2022, 387, 1361–1372. [Google Scholar] [CrossRef] [PubMed]
- Jovin, T.G.; Li, C.; Wu, L.; Wu, C.; Chen, J.; Jiang, C.; Shi, Z.; Gao, Z.; Song, C.; Chen, W.; et al. Trial of Thrombectomy 6 to 24 Hours after Stroke Due to Basilar-Artery Occlusion. New Engl. J. Med. 2022, 387, 1373–1384. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Moher, D. Updating guidance for reporting systematic reviews: Development of the PRISMA 2020 statement. J. Clin. Epidemiol. 2021, 134, 103–112. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials revisited. Contemp. Clin. Trials 2015, 45, 139–145. [Google Scholar] [CrossRef] [Green Version]
- Borenstein, M.; Higgins, J.P. Meta-analysis and subgroups. Prev. Sci. Off. J. Soc. Prev. Res. 2013, 14, 134–143. [Google Scholar] [CrossRef]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [Green Version]
- Atal, I.; Porcher, R.; Boutron, I.; Ravaud, P. Fragilty Index of Meta-Analyses. Available online: https://clinicalepidemio.fr/fragility_ma/ (accessed on 29 November 2022).
- Mun, K.T.; Bonomo, J.B.; Liebeskind, D.S.; Saver, J.L. Fragility Index Meta-Analysis of Randomized Controlled Trials Shows Highly Robust Evidential Strength for Benefit of <3 Hour Intravenous Alteplase. Stroke 2022, 53, 2069–2074. [Google Scholar]
- Deeks, J.J.; Higgins, J.P.; Altman, D.G. Chapter 10: Analysing Data and Undertaking Meta-Analyses. In Cochrane Handbook for Systematic Reviews of Interventions Version 6.3 (Updated February 2022). Cochrane. 2022. Available online: https://training.cochrane.org/handbook/current/chapter-10 (accessed on 29 November 2022).
- Wallace, B.C.; Dahabreh, I.J.; Trikalinos, T.A.; Lau, J.; Trow, P.; Schmid, C.H. Closing the Gap between Methodologists and End-Users: R as a Computational Back-End. J. Stat. Softw. 2012, 49, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Nogueira, R.G.; Tsivgoulis, G. Large Vessel Occlusion Strokes After the DIRECT-MT and SKIP Trials: Is the Alteplase Syringe Half Empty or Half Full? Stroke 2020, 51, 3182–3186. [Google Scholar] [CrossRef] [PubMed]
- Kohli, G.S.; Schartz, D.; Whyte, R.; Akkipeddi, S.M.; Ellens, N.R.; Bhalla, T.; Mattingly, T.K.; Bender, M.T. Endovascular thrombectomy with or without intravenous thrombolysis in acute basilar artery occlusion ischemic stroke: A meta-analysis. J. Stroke Cereb. Dis. 2022, 31, 28. [Google Scholar] [CrossRef] [PubMed]
- Strbian, D.; Sairanen, T.; Silvennoinen, H.; Salonen, O.; Kaste, M.; Lindsberg, P.J. Thrombolysis of basilar artery occlusion: Impact of baseline ischemia and time. Ann. Neurol. 2013, 73, 688–694. [Google Scholar] [CrossRef]
- Lee, Y.Y.; Yoon, W.; Kim, S.K.; Baek, B.H.; Kim, G.S.; Kim, J.T.; Park, M. Acute Basilar Artery Occlusion: Differences in Characteristics and Outcomes after Endovascular Therapy between Patients with and without Underlying Severe Atherosclerotic Stenosis. Am. J. Neuroradiol. 2017, 38, 1600–1604. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.S.; Lee, S.J.; Hong, J.M.; Alverne, F.; Lima, F.O.; Nogueira, R.G. Endovascular Treatment of Large Vessel Occlusion Strokes Due to Intracranial Atherosclerotic Disease. J. Stroke 2022, 24, 3–20. [Google Scholar] [CrossRef]
- Mutke, M.A.; Potreck, A.; Schmitt, N.; Seker, F.; Ringleb, P.A.; Nagel, S.; Möhlenbruch, M.A.; Bendszus, M.; Weyland, C.S.; Jesser, J. Exact Basilar Artery Occlusion Location Indicates Stroke Etiology and Recanalization Success in Patients Eligible for Endovascular Stroke Treatment. Clin. Neuroradiol. 2022; ahead of print. [Google Scholar] [CrossRef]
- Tornyos, D.; Bálint, A.; Kupó, P.; El Abdallaoui, O.E.A.; Komócsi, A. Antithrombotic Therapy for Secondary Prevention in Patients with Non-Cardioembolic Stroke or Transient Ischemic Attack: A Systematic Review. Life 2021, 11, 447. [Google Scholar]
- Tornyos, D.; Komócsi, A.; Bálint, A.; Kupó, P.; El Abdallaoui, O.E.A.; Szapáry, L.; Szapáry, L.B. Antithrombotic therapy for secondary prevention in patients with stroke or transient ischemic attack: A multiple treatment network meta-analysis of randomized controlled trials. PLoS ONE 2022, 17, e0273103. [Google Scholar] [CrossRef]
- Román, L.S.; Menon, B.K.; Blasco, J.; Hernández-Pérez, M.; Dávalos, A.; Majoie, C.B.L.M.; Campbell, B.C.V.; Guillemin, F.; Lingsma, H.; Anxionnat, R.; et al. Imaging features and safety and efficacy of endovascular stroke treatment: A meta-analysis of individual patient-level data. Lancet Neurol. 2018, 17, 895–904. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bouslama, M.; Haussen, D.C.; Aghaebrahim, A.; Grossberg, J.A.; Walker, G.; Rangaraju, S.; Horev, A.; Frankel, M.R.; Nogueira, R.G.; Jovin, T.G.; et al. Predictors of Good Outcome After Endovascular Therapy for Vertebrobasilar Occlusion Stroke. Stroke 2017, 48, 3252–3257. [Google Scholar] [CrossRef]
- Alexandre, A.; Valente, I.; Consoli, A.; Piano, M.; Renieri, L.; Gabrieli, J.; Russo, R.; Caragliano, A.; Ruggiero, M.; Saletti, A.; et al. Posterior Circulation Endovascular Thrombectomy for Large-Vessel Occlusion: Predictors of Favorable Clinical Outcome and Analysis of First-Pass Effect. Am. J. Neuroradiol. 2021, 42, 896–903. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Zhao, W.; Guo, Y.; Li, Y. Endovascular thrombectomy versus standard medical treatment for stroke patients with acute basilar artery occlusion: A systematic review and meta-analysis. J. Neurointerv. Surg. 2022, 14, 1173–1179. [Google Scholar] [CrossRef] [PubMed]
- Malik, A.; Drumm, B.; D’Anna, L.; Brooks, I.; Low, B.; Raha, O.; Shabbir, K.; Vittay, O.; Kwan, J.; Brown, Z.; et al. Mechanical thrombectomy in acute basilar artery stroke: A systematic review and Meta-analysis of randomized controlled trials. BMC Neurol. 2022, 22, 415. [Google Scholar]
- Xu, J.; Chen, X.; Chen, S.; Cao, W.; Zhao, H.; Ni, W.; Zhang, Y.; Gao, C.; Gu, Y.; Cheng, X.; et al. Endovascular treatment for basilar artery occlusion: A meta-analysis. Stroke Vasc. Neurol. 2022, 8, 1–3. [Google Scholar] [CrossRef]
- Lin, C.H.; Liebeskind, D.S.; Ovbiagele, B.; Lee, M.; Saver, J.L. Efficacy of endovascular therapy for basilar and vertebral artery occlusion: A systematic review and meta-analysis of randomized controlled trials. Eur. J. Intern. Med. 2022, 110, 22–28. [Google Scholar] [CrossRef]
- Abdalkader, M.; Finitsis, S.; Li, C.; Hu, W.; Liu, X.; Ji, X.; Huo, X.; Alemseged, F.; Qiu, Z.; Strbian, D.; et al. Endovascular versus Medical Management of Acute Basilar Artery Occlusion: A Systematic Review and Meta-Analysis of the Randomized Controlled Trials. J. Stroke 2023, 25, 81–91. [Google Scholar] [CrossRef] [PubMed]
- Yu, Y.; Lou, Y.; Cui, R.; Miao, Z.; Lou, X.; Ma, N. Endovascular treatment versus standard medical treatment for basilar artery occlusion: A meta-analysis of randomized controlled trials. J. Neurosurg. 2023; 1–9, Online ahead of print. [Google Scholar] [CrossRef]
- Li, F.; Sang, H.; Song, J.; Guo, Z.; Liu, S.; Luo, W.; Yuan, J.; Qiu, Z.; Huang, J.; Chen, L.; et al. One-Year Outcome After Endovascular Treatment for Acute Basilar Artery Occlusion. Stroke 2022, 53. [Google Scholar] [CrossRef]
- Pirson, F.A.V.; Boodt, N.; Brouwer, J.; Bruggeman, A.A.; Hartog, S.J.D.; Goldhoorn, R.-J.B.; Langezaal, L.C.; Staals, J.; van Zwam, W.H.; van der Leij, C.; et al. Endovascular Treatment for Posterior Circulation Stroke in Routine Clinical Practice: Results of the Multicenter Randomized Clinical Trial of Endovascular Treatment for Acute Ischemic Stroke in the Netherlands Registry. Stroke 2022, 53, 758–768. [Google Scholar] [CrossRef]
- Schonewille, W.J. Favorable Outcomes in Endovascular Therapy for Basilar-Artery Occlusion. New Engl. J. Med. 2022, 387, 1428–1429. [Google Scholar] [CrossRef]
- Singer, O.C.; Berkefeld, J.; Nolte, C.; Bohner, G.; Haring, H.-P.; Trenkler, J.; Gröschel, K.; Müller-Forell, W.; Niederkorn, K.; Deutschmann, H.; et al. Mechanical recanalization in basilar artery occlusion: The ENDOSTROKE study. Ann. Neurol. 2014, 77, 415–424. [Google Scholar] [CrossRef] [PubMed]
- Tao, C.; Qureshi, A.I.; Yin, Y.; Li, J.; Li, R.; Xu, P.; Sun, J.; Liao, G.; Yue, X.; Shi, H.; et al. Endovascular Treatment Versus Best Medical Management in Acute Basilar Artery Occlusion Strokes: Results from the ATTENTION Multicenter Registry. Circulation 2022, 146, 6–17. [Google Scholar] [CrossRef] [PubMed]
- Writing Group for the BASILAR Group; Zi, W.; Qiu, Z.; Wu, D.; Li, F.; Liu, H.; Liu, W.; Huang, W.; Shi, Z.; Bai, Y.; et al. Assessment of Endovascular Treatment for Acute Basilar Artery Occlusion via a Nationwide Prospective Registry. JAMA Neurol. 2020, 77, 561–573. [Google Scholar] [CrossRef] [PubMed]
- McGrath, S.; Sohn, H.; Steele, R.; Benedetti, A. Meta-analysis of the difference of medians. Biom. J. 2019, 62, 69–98. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Recruiting Centers | Period of Enrollment | Target Population | EVT and BMT | BMT Alone | ||
|---|---|---|---|---|---|---|---|
| N | Patients Characteristics | N | Patients Characteristics | ||||
| ATTENTION [12] | China | February 2021–January 2022 | BAO within 12 h, with NIHSS ≥ 10 and pre-stroke mRS and PC-ASPECTS selection stratified by age | 226 | Mean age: 66.0 ± 11.1 years; 66% males; median NIHSS: 24 (15–35); median PC-ASPECTS: 9 (8–10); median time from stroke onset to randomization: 5.1 (3.6–7.2) h; 31% with IVT pretreatment | 114 | Mean age: 67.3 ± 10.2 years; 72% males; median NIHSS: 24 (14–35); median PC-ASPECTS: 10 (8–10); median time from stroke onset to randomization: 4.9 (3.5–7.0) h; 34% with IVT pretreatment |
| BAOCHE [13] | China | August 2016–June 2021 | BAO between 6 to 24 h, age ≤ 80, with NIHSS ≥ 10 (later expanded to ≥6), pre-stroke mRS ≤ 1, PC-ASPECTS ≥ 6 | 110 | Mean age: 64.2 ± 9.6 years; 73% males; median NIHSS: 20 (15–29); median PC-ASPECTS: 8 (7–10); median time from stroke onset to randomization: 11.1 (8.5–14.4) h; 14% with IVT pretreatment | 107 | Mean age: 63.7 ± 9.8 years; 74% males; median NIHSS: 19 (12–30); median PC = ASPECTS: 8 (7–10); median time from stroke onset to randomization: 11.0 (8.2–14.0) h; 21% with IVT pretreatment |
| BASICS [10] | Interna tional | October 2011–December 2019 | BAO within 6 h, age ≤ 85 (later expanded to >85), with NIHSS ≥ 10 (later expanded to <10), pre-stroke mRS ≤ 2 | 154 | Mean age: 66.8 ± 13.1 years; 65% males; median NIHSS: 21 (NR); median PC-ASPECTS: 10 (10–10); median time from stroke onset to randomization: 4.4 (3.3–6.2) h *; 79% with IVT pretreatment | 146 | Mean age: 67.2 ± 11.9 years; 66% males; median NIHSS: 22 (NR); median PC-ASPECTS: 10 (10–10); median time from stroke onset to randomization: NR; 80% with IVT pretreatment |
| BEST [11] | China | April 2015–September 2017 | BAO, within 8 h, pre-stroke mRS ≤ 2 | 66 | Mean age: 62.0 ± 17.8 years; 73% males; median NIHSS: 32 (18–38); median PC-ASPECTS: 8 (7–9); median time from stroke onset to randomization: 4.1 (2.3–6) h; 27% with IVT pretreatment | 65 | Mean age: 65.7 ± 12.6 years; 80% males; median NIHSS: 26 (13–37); median PC-ASPECTS: 8 (7–9); median time from stroke onset to randomization: 4.6 (3.2–6.5) h; 32% with IVT pretreatment |
| Variable | Effect | Fragility Index | Interpretation | ||
|---|---|---|---|---|---|
| N of Studies | Risk Ratio (95% CI) | I2, p for Cochran Q | |||
| Primary Outcome | |||||
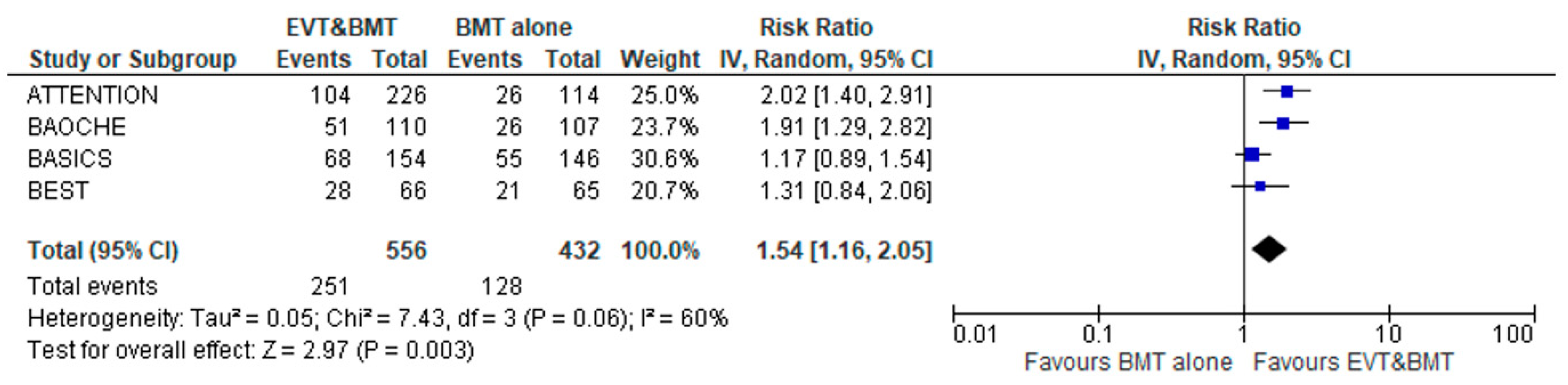
| Good Functional Outcome (mRS 0–3) | 4 | 1.54 (1.16–2.05) | 60%; 0.06 | 9 | Fragile/Somewhat Robust |
| Secondary Efficacy Outcomes | |||||
| Functional Independence (mRS 0–2) | 4 | 1.83 (1.08–3.08) | 79%; 0.02 | 4 | Highly Fragile/Not Robust |
| Reduced Disability | 4 | 1.96 (1.26–3.05) * | 59%; 0.06 | NA | NA |
| Secondary Safety Outcomes | |||||
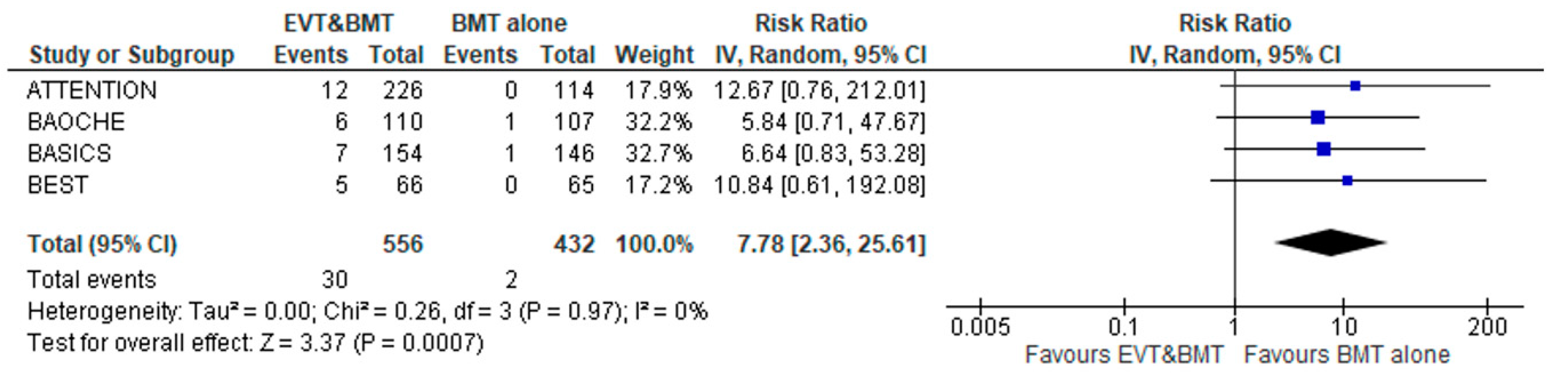
| Symptomatic Intracranial Hemorrhage | 4 | 7.78 (2.36–25.61) | 0%; 0.97 | 5 | Fragile/Somewhat Robust |
| Any Intracranial Hemorrhage | 4 | 2.85 (1.50–5.44) | 16%; 0.31 | 5 | Fragile/Somewhat Robust |
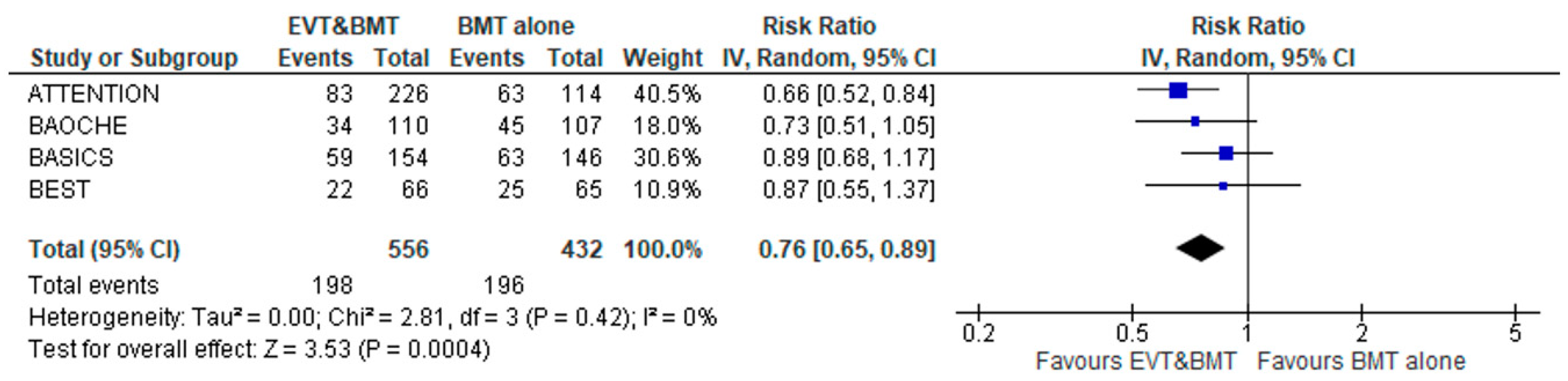
| All-cause mortality | 4 | 0.76 (0.65–0.89) | 0%; 0.42 | 9 | Fragile/Somewhat Robust |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Palaiodimou, L.; Eleftheriou, A.; Katsanos, A.H.; Safouris, A.; Magoufis, G.; Spiliopoulos, S.; Velonakis, G.; Vassilopoulou, S.; de Sousa, D.A.; Turc, G.; et al. Endovascular Treatment for Acute Basilar Artery Occlusion: A Fragility Index Meta-Analysis. J. Clin. Med. 2023, 12, 2617. https://doi.org/10.3390/jcm12072617
Palaiodimou L, Eleftheriou A, Katsanos AH, Safouris A, Magoufis G, Spiliopoulos S, Velonakis G, Vassilopoulou S, de Sousa DA, Turc G, et al. Endovascular Treatment for Acute Basilar Artery Occlusion: A Fragility Index Meta-Analysis. Journal of Clinical Medicine. 2023; 12(7):2617. https://doi.org/10.3390/jcm12072617
Chicago/Turabian StylePalaiodimou, Lina, Andreas Eleftheriou, Aristeidis H. Katsanos, Apostolos Safouris, Georgios Magoufis, Stavros Spiliopoulos, Georgios Velonakis, Sofia Vassilopoulou, Diana Aguiar de Sousa, Guillaume Turc, and et al. 2023. "Endovascular Treatment for Acute Basilar Artery Occlusion: A Fragility Index Meta-Analysis" Journal of Clinical Medicine 12, no. 7: 2617. https://doi.org/10.3390/jcm12072617