
Relationship of Glycated Hemoglobin A1c with All-Cause and Cardiovascular Mortality among Patients with Hypertension
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
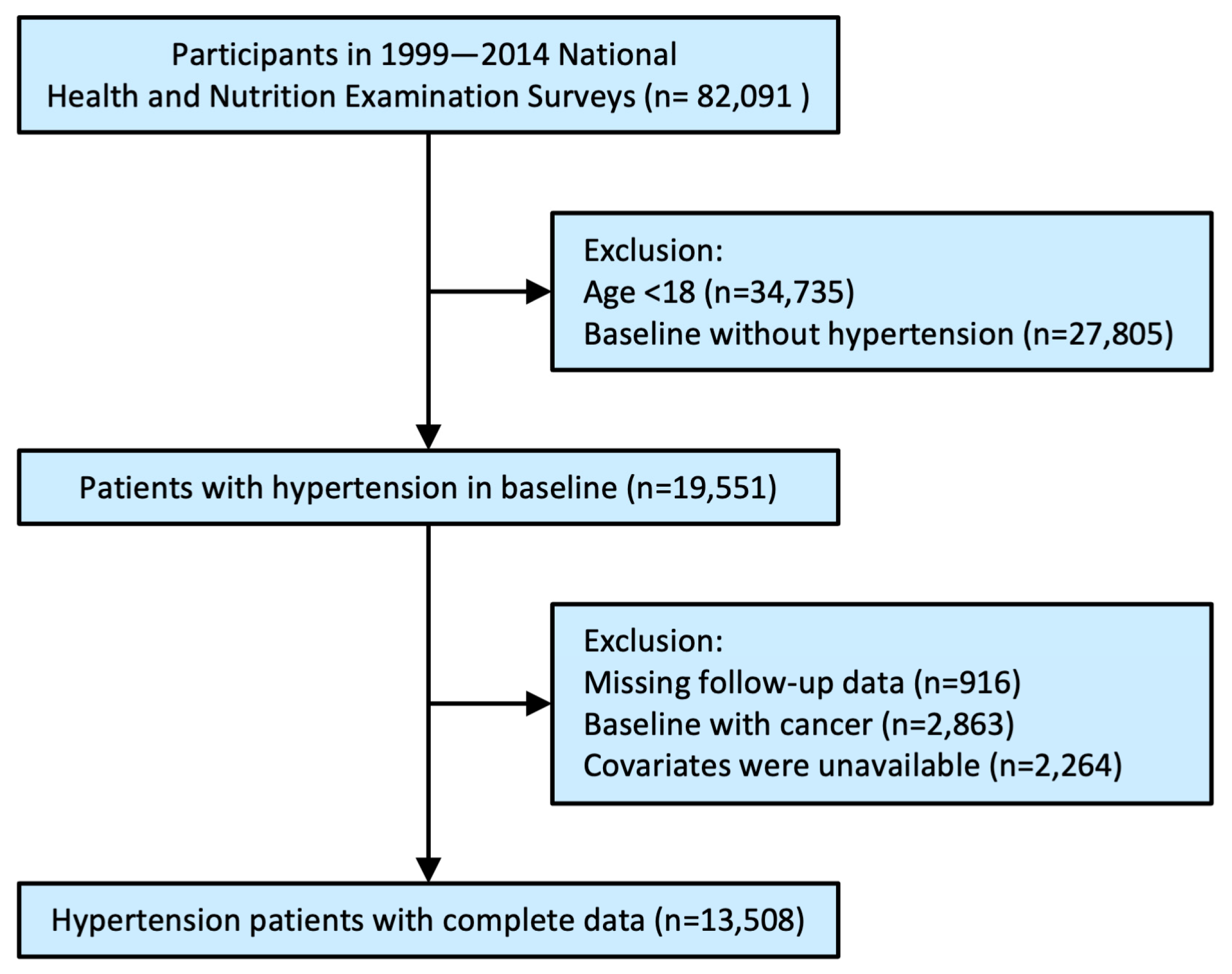
2.1. Study Population
2.2. Demographic Characteristics and Biochemical Covariates
2.3. Outcomes
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics
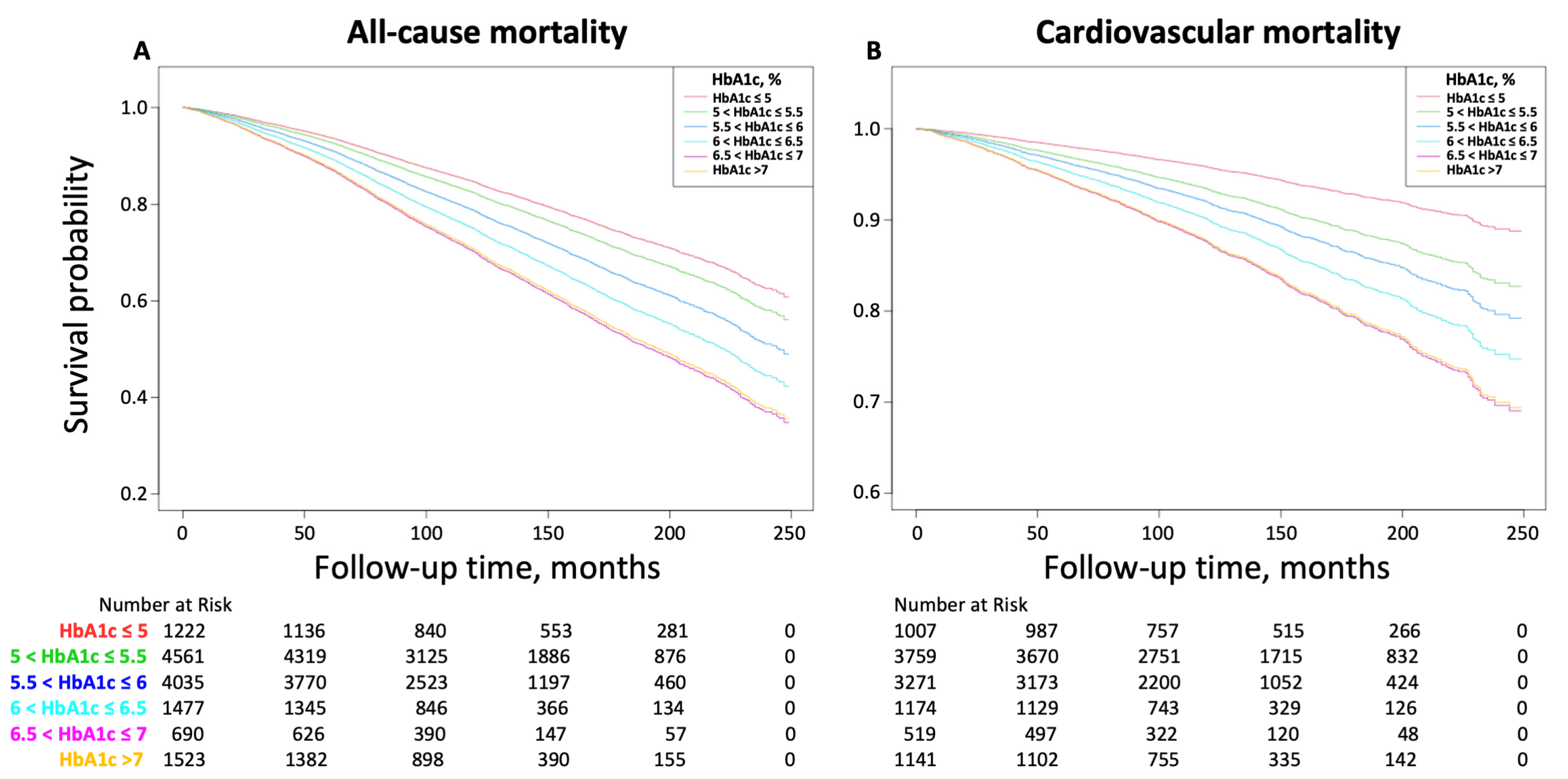
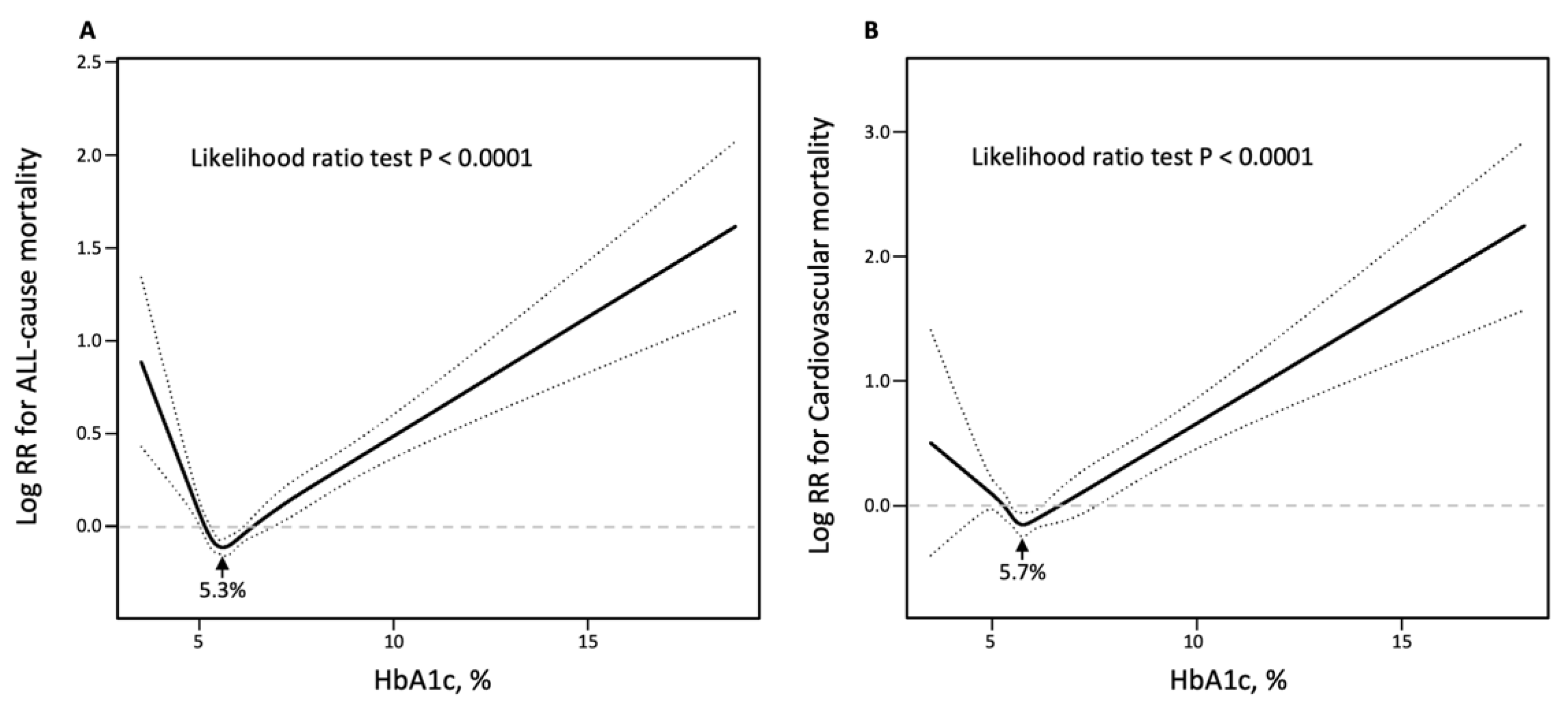
3.2. Relationship between HbA1c and All-Cause and Cardiovascular Mortality
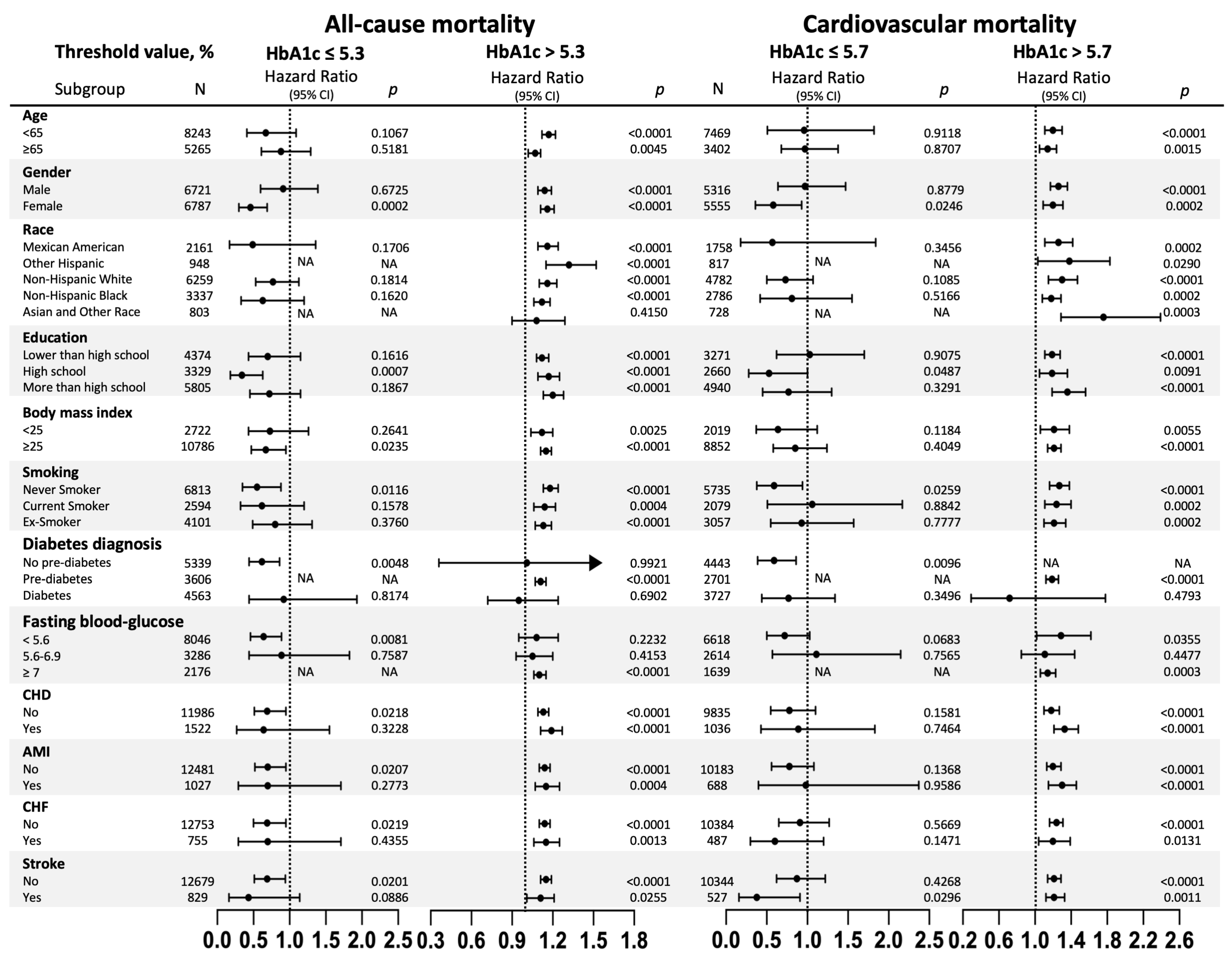
3.3. Subgroups Analysis of the Risk of All-Cause and Cardiovascular Mortality
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Collaborators GBDRF. Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1923–1994. [Google Scholar]
- Unger, T.; Borghi, C.; Charchar, F.; Khan, N.A.; Poulter, N.R.; Prabhakaran, D.; Ramirez, A.; Schlaich, M.; Stergiou, G.S.; Schutte, A.E.; et al. 2020 International Society of Hypertension Global Hypertension Practice Guidelines. Hypertension 2020, 75, 1334–1357. [Google Scholar] [CrossRef]
- Tsimihodimos, V.; Gonzalez-Villalpando, C.; Meigs, J.B.; Ferrannini, E. Hypertension and Diabetes Mellitus: Coprediction and Time Trajectories. Hypertension 2018, 71, 422–428. [Google Scholar] [CrossRef]
- Qiu, S.; Du, Z.; Li, W.; Chen, J.; Wu, H.; Liu, J.; Cai, M.; Wang, B.; Guo, H.; Sun, Z.; et al. Exploration and Validation of the Performance of Hemoglobin A1c in Detecting Diabetes in Community-Dwellers with Hypertension. Ann. Lab. Med. 2020, 40, 457–465. [Google Scholar] [CrossRef]
- Petrie, J.R.; Guzik, T.J.; Touyz, R.M. Diabetes, Hypertension, and Cardiovascular Disease: Clinical Insights and Vascular Mechanisms. Can. J. Cardiol. 2018, 34, 575–584. [Google Scholar] [CrossRef] [Green Version]
- American Diabetes. A Diagnosis and classification of diabetes mellitus. Diabetes Care 2010, 33, S62–S69. [Google Scholar] [CrossRef] [Green Version]
- Use of Glycated Haemoglobin (HbA1c) in the Diagnosis of Diabetes Mellitus: Abbreviated Report of a WHO Consultation; World Health Organization: Geneva, Switzerland, 2011.
- Menon, V.; Greene, T.; Pereira, A.A.; Wang, X.; Beck, G.J.; Kusek, J.W.; Collins, A.J.; Levey, A.S.; Sarnak, M.J. Glycosylated hemoglobin and mortality in patients with nondiabetic chronic kidney disease. J. Am. Soc. Nephrol. 2005, 16, 3411–3417. [Google Scholar] [CrossRef] [Green Version]
- Andersson, C.; van Gaal, L.; Caterson, I.D.; Weeke, P.; James, W.P.; Coutinho, W.; Finer, N.; Sharma, A.M.; Maggioni, A.P.; Torp-Pedersen, C.; et al. Relationship between HbA1c levels and risk of cardiovascular adverse outcomes and all-cause mortality in overweight and obese cardiovascular high-risk women and men with type 2 diabetes. Diabetologia 2012, 55, 2348–2355. [Google Scholar] [CrossRef] [Green Version]
- Inoue, K.; Nianogo, R.; Telesca, D.; Goto, A.; Khachadourian, V.; Tsugawa, Y.; Sugiyama, T.; Mayeda, E.R.; Ritz, B. Low HbA1c levels and all-cause or cardiovascular mortality among people without diabetes: The US National Health and Nutrition Examination Survey 1999–2015. Int. J. Epidemiol. 2021, 50, 1373–1383. [Google Scholar] [CrossRef]
- Mongraw-Chaffin, M.; Bertoni, A.G.; Golden, S.H.; Mathioudakis, N.; Sears, D.D.; Szklo, M.; Anderson, C.A.M. Association of Low Fasting Glucose and HbA1c with Cardiovascular Disease and Mortality: The MESA Study. J. Endocr. Soc. 2019, 3, 892–901. [Google Scholar] [CrossRef] [Green Version]
- Blaum, C.S.; Volpato, S.; Cappola, A.R.; Chaves, P.; Xue, Q.L.; Guralnik, J.M.; Fried, L.P. Diabetes, hyperglycaemia and mortality in disabled older women: The Women’s Health and Ageing Study I. Diabet. Med. 2005, 22, 543–550. [Google Scholar] [CrossRef] [Green Version]
- Anyanwagu, U.; Mamza, J.; Donnelly, R.; Idris, I. Relationship between HbA1c and all-cause mortality in older patients with insulin-treated type 2 diabetes: Results of a large UK Cohort Study. Age Ageing 2019, 48, 235–240. [Google Scholar] [CrossRef]
- Goode, K.M.; John, J.; Rigby, A.S.; Kilpatrick, E.S.; Atkin, S.L.; Bragadeesh, T.; Clark, A.L.; Cleland, J.G. Elevated glycated haemoglobin is a strong predictor of mortality in patients with left ventricular systolic dysfunction who are not receiving treatment for diabetes mellitus. Heart 2009, 95, 917–923. [Google Scholar] [CrossRef]
- Ford, E.S.; Giles, W.H.; Dietz, W.H. Prevalence of the metabolic syndrome among US adults: Findings from the third National Health and Nutrition Examination Survey. JAMA 2002, 287, 356–359. [Google Scholar] [CrossRef] [Green Version]
- Palmer, M.K.; Toth, P.P. Trends in Lipids, Obesity, Metabolic Syndrome, and Diabetes Mellitus in the United States: An NHANES Analysis (2003–2004 to 2013–2014). Obesity 2019, 27, 309–314. [Google Scholar] [CrossRef] [Green Version]
- American Diabetes. A 2 Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes-2018. Diabetes Care 2018, 41, S13–S27. [Google Scholar] [CrossRef] [Green Version]
- Huang, Y.Q.; Liu, L.; Huang, J.Y.; Chen, C.L.; Yu, Y.L.; Lo, K.; Feng, Y.Q. Prediabetes and risk for all-cause and cardiovascular mortality based on hypertension status. Ann. Transl. Med. 2020, 8, 1580. [Google Scholar] [CrossRef]
- James, P.A.; Oparil, S.; Carter, B.L.; Cushman, W.C.; Dennison-Himmelfarb, C.; Handler, J.; Lackland, D.T.; LeFevre, M.L.; MacKenzie, T.D.; Ortiz, E.; et al. 2014 evidence-based guideline for the management of high blood pressure in adults: Report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA 2014, 311, 507–520. [Google Scholar] [CrossRef] [Green Version]
- Yan, Y.Q.; Chen, J.; Huang, Y.Q. A Non-Linear Association of High-Density Lipoprotein Cholesterol with All-Cause and Cause-Specific Mortality in Diabetic Patients. Diabetes Metab. Syndr. Obes. 2021, 14, 2851–2862. [Google Scholar] [CrossRef]
- Cavero-Redondo, I.; Peleteiro, B.; Alvarez-Bueno, C.; Rodriguez-Artalejo, F.; Martinez-Vizcaino, V. Glycated haemoglobin A1c as a risk factor of cardiovascular outcomes and all-cause mortality in diabetic and non-diabetic populations: A systematic review and meta-analysis. BMJ Open 2017, 7, e015949. [Google Scholar] [CrossRef] [Green Version]
- Sakurai, M.; Saitoh, S.; Miura, K.; Nakagawa, H.; Ohnishi, H.; Akasaka, H.; Kadota, A.; Kita, Y.; Hayakawa, T.; NIPPON DATA90 Research Group. HbA1c and the risks for all-cause and cardiovascular mortality in the general Japanese population: NIPPON DATA90. Diabetes Care 2013, 36, 3759–3765. [Google Scholar] [CrossRef] [Green Version]
- Brewer, N.; Wright, C.S.; Travier, N.; Cunningham, C.W.; Hornell, J.; Pearce, N.; Jeffreys, M. A New Zealand linkage study examining the associations between A1C concentration and mortality. Diabetes Care 2008, 31, 1144–1149. [Google Scholar] [CrossRef] [Green Version]
- Creager, M.A.; Luscher, T.F.; Cosentino, F.; Beckman, J.A. Diabetes and vascular disease: Pathophysiology, clinical consequences, and medical therapy: Part I. Circulation 2003, 108, 1527–1532. [Google Scholar] [CrossRef] [Green Version]
- Brownlee, M. The pathobiology of diabetic complications: A unifying mechanism. Diabetes 2005, 54, 1615–1625. [Google Scholar] [CrossRef] [Green Version]
- Kalantar-Zadeh, K.; Block, G.; Horwich, T.; Fonarow, G.C. Reverse epidemiology of conventional cardiovascular risk factors in patients with chronic heart failure. J. Am. Coll. Cardiol. 2004, 43, 1439–1444. [Google Scholar] [CrossRef] [Green Version]
- Wright, R.J.; Frier, B.M. Vascular disease and diabetes: Is hypoglycaemia an aggravating factor? Diabetes Metab. Res. Rev. 2008, 24, 353–363. [Google Scholar] [CrossRef]
- Frier, B.M.; Schernthaner, G.; Heller, S.R. Hypoglycemia and cardiovascular risks. Diabetes Care 2011, 34, S132–S137. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total | HbA1c ≤ 5 | 5 < HbA1c ≤ 5.5 | 5.5 < HbA1c ≤ 6 | 6 < HbA1c ≤ 6.5 | 6.5 < HbA1c ≤ 7 | HbA1c > 7 | p | |
|---|---|---|---|---|---|---|---|---|
| N | 13,508 | 1222 | 4561 | 4035 | 1477 | 690 | 1523 | |
| Age, years | 58.55 ± 15.56 | 48.91 ± 17.38 | 55.77 ± 16.65 | 60.91 ± 14.38 | 63.97 ± 12.54 | 63.99 ± 12.18 | 60.67 ± 12.15 | <0.001 |
| Male, N (%) | 6787 (50.24) | 609 (49.84) | 2287 (50.14) | 2055 (50.93) | 778 (52.67) | 323 (46.81) | 735 (48.26) | 0.075 |
| Body mass index, kg/m2 | 30.45 ± 6.91 | 28.51 ± 6.52 | 29.23 ± 6.31 | 30.59 ± 6.93 | 32.00 ± 7.06 | 32.82 ± 7.47 | 32.71 ± 7.21 | <0.001 |
| Systolic blood pressure, mmHg | 135.80 ± 20.78 | 132.32 ± 20.94 | 135.38 ± 20.46 | 136.71 ± 20.92 | 136.13 ± 20.15 | 134.84 ± 19.71 | 137.53 ± 21.91 | <0.001 |
| Diastolic blood pressure, mmHg | 73.53 ± 14.05 | 75.53 ± 14.10 | 75.24 ± 13.71 | 73.53 ± 13.96 | 71.17 ± 13.79 | 69.39 ± 14.50 | 70.94 ± 14.17 | <0.001 |
| Race, N (%) | <0.001 | |||||||
| Mexican American | 2161 (16.00) | 132 (10.80) | 676 (14.82) | 621 (15.39) | 216 (14.62) | 126 (18.26) | 390 (25.61) | |
| Other Hispanic | 948 (7.02) | 64 (5.24) | 273 (5.99) | 291 (7.21) | 136 (9.21) | 57 (8.26) | 127 (8.34) | |
| Non-Hispanic White | 6259 (46.34) | 680 (55.65) | 2528 (55.43) | 1811 (44.88) | 536 (36.29) | 252 (36.52) | 452 (29.68) | |
| Non-Hispanic Black | 3337 (24.70) | 285 (23.32) | 867 (19.01) | 1046 (25.92) | 486 (32.90) | 206 (29.86) | 447 (29.35) | |
| Asian and other Race | 803 (5.94) | 61 (4.99) | 217 (4.76) | 266 (6.59) | 103 (6.97) | 49 (7.10) | 107 (7.03) | |
| Education, N (%) | <0.001 | |||||||
| Lower than high school | 4374 (32.38) | 274 (22.42) | 1310 (28.72) | 1304 (32.32) | 532 (36.02) | 273 (39.57) | 681 (44.71) | |
| High school | 3329 (24.64) | 285 (23.32) | 1102 (24.16) | 1053 (26.10) | 400 (27.08) | 168 (24.35) | 321 (21.08) | |
| More than high school | 5805 (42.97) | 663 (54.26) | 2149 (47.12) | 1678 (41.59) | 545 (36.90) | 249 (36.09) | 521 (34.21) | |
| Smoking, N (%) | <0.001 | |||||||
| Never Smoker | 6813 (50.44) | 620 (50.74) | 2306 (50.56) | 2051 (50.83) | 716 (48.48) | 339 (49.13) | 781 (51.28) | |
| Current Smoker | 2594 (19.20) | 286 (23.40) | 924 (20.26) | 771 (19.11) | 249 (16.86) | 109 (15.80) | 255 (16.74) | |
| Ex-Smoker | 4101 (30.36) | 316 (25.86) | 1331 (29.18) | 1213 (30.06) | 512 (34.66) | 242 (35.07) | 487 (31.98) | |
| Diabetes diagnosis, N (%) | <0.001 | |||||||
| No pre-diabetes | 5339 (39.52) | 1029 (84.21) | 3572 (78.32) | 738 (18.29) | 0 (0.00) | 0 (0.00) | 0 (0.00) | |
| Pre-diabetes | 4563 (33.78) | 150 (12.27) | 819 (17.96) | 2812 (69.69) | 782 (52.95) | 0 (0.00) | 0 (0.00) | |
| Diabetes | 3606 (26.70) | 43 (3.52) | 170 (3.73) | 485 (12.02) | 695 (47.05) | 690 (100.00) | 1523 (100.00) | |
| Coronary heart disease, N (%) | 1522 (11.27) | 64 (5.24) | 406 (8.90) | 467 (11.57) | 206 (13.95) | 116 (16.81) | 263 (17.27) | <0.001 |
| Acute myocardial infarction, N (%) | 1027 (7.60) | 36 (2.95) | 277 (6.07) | 308 (7.63) | 145 (9.82) | 84 (12.17) | 177 (11.62) | <0.001 |
| Chronic heart failure, N (%) | 755 (5.59) | 30 (2.45) | 194 (4.25) | 208 (5.15) | 111 (7.52) | 74 (10.72) | 138 (9.06) | <0.001 |
| Stroke, N (%) | 829 (6.14) | 58 (4.75) | 224 (4.91) | 252 (6.25) | 115 (7.79) | 54 (7.83) | 126 (8.27) | <0.001 |
| HbA1c, % | 5.98 ± 1.24 | 4.83 ± 0.22 | 5.33 ± 0.13 | 5.77 ± 0.14 | 6.26 ± 0.14 | 6.78 ± 0.14 | 8.76 ± 1.71 | <0.001 |
| Fasting blood glucose, mmol/L | 6.09 ± 2.54 | 5.00 ± 0.72 | 5.17 ± 0.75 | 5.50 ± 0.99 | 6.18 ± 1.41 | 7.12 ± 2.04 | 10.71 ± 4.73 | <0.001 |
| Creatinine, mg/dL | 85.73 ± 54.06 | 86.58 ± 76.68 | 83.23 ± 56.50 | 84.71 ± 35.56 | 87.07 ± 40.57 | 93.41 ± 77.70 | 90.48 ± 62.48 | <0.001 |
| Hemoglobin, g/L | 14.11 ± 1.55 | 14.10 ± 1.78 | 14.32 ± 1.51 | 14.11 ± 1.49 | 13.85 ± 1.52 | 13.79 ± 1.59 | 13.86 ± 1.58 | <0.001 |
| Triglyceride, mg/dL | 134.0 (90.0–202.0) | 116.0 (77.0–172.0) | 123.0 (84.0–185.0) | 134.0 (92.0–193.0) | 144.0 (99.0–212.0) | 154.0 (104.3–233.8) | 173.0 (114.5–266.5) | <0.001 |
| Total cholesterol, mg/dL | 200.13 ± 43.65 | 195.61 ± 40.24 | 203.31 ± 41.72 | 203.78 ± 43.61 | 193.48 ± 44.09 | 189.08 ± 46.87 | 196.06 ± 47.72 | <0.001 |
| HDL-C, mg/dL | 51.95 ± 15.92 | 55.38 ± 17.81 | 54.08 ± 16.84 | 52.32 ± 15.46 | 49.24 ± 13.76 | 47.65 ± 14.11 | 46.38 ± 12.96 | <0.001 |
| Antihypertensive drugs, N (%) | 8015 (59.34) | 508 (41.57) | 2212 (48.50) | 2506 (62.11) | 1091 (73.87) | 565 (81.88) | 1133 (74.39) | <0.001 |
| Hypoglycemic agents, N (%) | 2423 (17.94) | 22 (1.80) | 81 (1.78) | 312 (7.73) | 434 (29.38) | 421 (61.01) | 1153 (75.71) | <0.001 |
| Aspirin, N (%) | 322 (2.38) | 11 (0.90) | 50 (1.10) | 95 (2.35) | 62 (4.20) | 27 (3.91) | 77 (5.06) | <0.001 |
| Clopidogrel, N (%) | 438 (3.24) | 19 (1.55) | 104 (2.28) | 128 (3.17) | 66 (4.47) | 37 (5.36) | 84 (5.52) | <0.001 |
| Statin, N (%) | 3742 (27.70) | 129 (10.56) | 864 (18.94) | 1116 (27.66) | 628 (42.52) | 326 (47.25) | 679 (44.58) | <0.001 |
| All-cause mortality, N (%) | 3760 (27.84) | 278 (22.75) | 1154 (25.30) | 1089 (26.99) | 440 (29.79) | 245 (35.51) | 554 (36.38) | <0.001 |
| Cardiovascular mortality, N (%) | 1123 (10.33) | 63 (6.26) | 352 (9.36) | 325 (9.94) | 137 (11.67) | 74 (14.26) | 172 (15.07) | <0.001 |
| Model 1 HR (95% CI), p | Model 2 HR (95% CI), p | Model 3 HR (95% CI), p | |
|---|---|---|---|
| All-cause mortality | |||
| HbA1c | 1.13 (1.11, 1.16), <0.0001 | 1.15 (1.12, 1.18), <0.0001 | 1.11 (1.08, 1.15), <0.0001 |
| HbA1c threshold value | |||
| ≤threshold value 5.3 | 1.04 (0.77, 1.40), 0.8085 | 0.53 (0.40, 0.70), <0.0001 | 0.68 (0.51, 0.90), 0.0078 |
| >threshold value 5.3 | 1.10 (1.08, 1.13), <0.0001 | 1.19 (1.16, 1.22), <0.0001 | 1.14 (1.11, 1.18), <0.0001 |
| HbA1c categorical | |||
| HbA1c ≤ 5 | 0.86 (0.76, 0.98), 0.0256 | 1.32 (1.16, 1.51), <0.0001 | 1.27 (1.11, 1.45), 0.0004 |
| 5 < HbA1c ≤ 5.5 | Reference | Reference | Reference |
| 5.5 < HbA1c ≤ 6 | 1.23 (1.14, 1.34), <0.0001 | 0.98 (0.90, 1.06), 0.6200 | 0.96 (0.88, 1.05), 0.3660 |
| 6 < HbA1c ≤ 6.5 | 1.49 (1.33, 1.66), <0.0001 | 1.13 (1.01, 1.27), 0.0294 | 1.07 (0.95, 1.20), 0.2622 |
| 6.5 < HbA1c ≤ 7 | 1.82 (1.59, 2.09), <0.0001 | 1.31 (1.14, 1.51), 0.0001 | 1.08 (0.93, 1.27), 0.2988 |
| HbA1c > 7 | 1.79 (1.61, 1.98), <0.0001 | 1.73 (1.56, 1.92), <0.0001 | 1.45 (1.27, 1.66), <0.0001 |
| p for trend | <0.0001 | <0.0001 | <0.0001 |
| Cardiovascular mortality | |||
| HbA1c | 1.17 (1.13, 1.21), <0.0001 | 1.20 (1.15, 1.25), <0.0001 | 1.17 (1.11, 1.23), <0.0001 |
| HbA1c threshold value | |||
| ≤threshold value 5.7 | 1.80 (1.33, 2.45), 0.0002 | 0.76 (0.56, 1.03), 0.0776 | 0.77 (0.57, 1.05), 0.0969 |
| >threshold value 5.7 | 1.09 (1.04, 1.14), 0.0005 | 1.24 (1.18, 1.30), <0.0001 | 1.22 (1.16, 1.29), <0.0001 |
| HbA1c categorical | |||
| HbA1c ≤ 5 | 0.51 (0.39, 0.67), <0.0001 | 1.17 (0.89, 1.53), 0.2681 | 1.21 (0.92, 1.59), 0.1829 |
| 5 < HbA1c ≤ 5.5 | 0.81 (0.70, 0.95), 0.0078 | 1.13 (0.97, 1.32), 0.1080 | 1.22 (1.04, 1.42), 0.0135 |
| 5.5 < HbA1c ≤ 6 | Reference | Reference | Reference |
| 6 < HbA1c ≤ 6.5 | 1.25 (1.02, 1.53), 0.0290 | 1.24 (1.01, 1.51), 0.0386 | 1.19 (0.96, 1.46), 0.1051 |
| 6.5 < HbA1c ≤ 7 | 1.59 (1.23, 2.05), 0.0003 | 1.40 (1.09, 1.81), 0.0089 | 1.23 (0.93, 1.62), 0.1510 |
| HbA1c > 7 | 1.57 (1.30, 1.89), <0.0001 | 2.05 (1.70, 2.48), <0.0001 | 1.85 (1.47, 2.33), <0.0001 |
| p for trend | <0.0001 | <0.0001 | 0.0003 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zeng, R.; Zhang, Y.; Xu, J.; Kong, Y.; Tan, J.; Guo, L.; Zhang, M. Relationship of Glycated Hemoglobin A1c with All-Cause and Cardiovascular Mortality among Patients with Hypertension. J. Clin. Med. 2023, 12, 2615. https://doi.org/10.3390/jcm12072615
Zeng R, Zhang Y, Xu J, Kong Y, Tan J, Guo L, Zhang M. Relationship of Glycated Hemoglobin A1c with All-Cause and Cardiovascular Mortality among Patients with Hypertension. Journal of Clinical Medicine. 2023; 12(7):2615. https://doi.org/10.3390/jcm12072615
Chicago/Turabian StyleZeng, Ruixiang, Yuzhuo Zhang, Junpeng Xu, Yongjie Kong, Jiawei Tan, Liheng Guo, and Minzhou Zhang. 2023. "Relationship of Glycated Hemoglobin A1c with All-Cause and Cardiovascular Mortality among Patients with Hypertension" Journal of Clinical Medicine 12, no. 7: 2615. https://doi.org/10.3390/jcm12072615