
Morphometric Study of the Initial Ventricular Indices to Predict the Complications and Outcome of Aneurysmal Subarachnoid Hemorrhage
 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Methods
2.1. Patient Population
2.2. SAH Management
2.3. Data Management
2.4. Study Endpoints and Statistical Analyses
3. Results
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Erixon, H.O.; Sorteberg, A.; Sorteberg, W.; Eide, P.K. Predictors of shunt dependency after aneurysmal subarachnoid hemorrhage: Results of a single-center clinical trial. Acta Neurochir. 2014, 156, 2059–2069. [Google Scholar] [CrossRef]
- Paluzzi, A.; Belli, A.; Bain, P.; Viva, L. Brain ‘imaging’ in the Renaissance. J. R. Soc. Med. 2007, 100, 540–543. [Google Scholar] [CrossRef] [Green Version]
- LeMay, M. Radiologic changes of the aging brain and skull. Am. J. Neuroradiol. 1984, 143, 383–389. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Evans, W.J. An encephalographic ratio for estimating ventricular enlargement and cerebral atrophy. Arch. Neurol. Psychiatry 1942, 47, 931–937. [Google Scholar] [CrossRef]
- Nakajima, M.; Yamada, S.; Miyajima, M.; Ishii, K.; Kuriyama, N.; Kazui, H.; Kanemoto, H.; Suehiro, T.; Yoshiyama, K.; Kameda, M.; et al. Guidelines for Management of Idiopathic Normal Pressure Hydrocephalus (Third Edition): Endorsed by the Japanese Society of Normal Pressure Hydrocephalus. Neurol. Med. Chir. 2021, 61, 63–97. [Google Scholar] [CrossRef] [PubMed]
- Karypidou, E.; Megagiannis, P.; Papaoikonomou, D.; Pelteki, N.; Gkatzima, O.; Tsolaki, M. Callosal Angle and Evans Index predict beta amyloid and tau protein in patients with dementia. Hell. J. Nucl. Med. 2019, 22, 51–58. [Google Scholar] [PubMed]
- Andreasen, N.C.; Olsen, S.A.; Dennert, J.W.; Smith, M.R. Ventricular enlargement in schizophrenia: Relationship to positive and negative symptoms. Am. J. Psychiatry 1982, 139, 297–302. [Google Scholar] [CrossRef] [PubMed]
- van Asch, C.J.; van der Schaaf, I.C.; Rinkel, G.J. Acute hydrocephalus and cerebral perfusion after aneurysmal subarachnoid hemorrhage. Am. J. Neuroradiol. 2010, 31, 67–70. [Google Scholar] [CrossRef] [Green Version]
- Dupont, S.; Rabinstein, A.A. Extent of acute hydrocephalus after subarachnoid hemorrhage as a risk factor for poor functional outcome. Neurol. Res. 2013, 35, 107–110. [Google Scholar] [CrossRef]
- Said, M.; Gumus, M.; Herten, A.; Dinger, T.F.; Chihi, M.; Darkwah Oppong, M.; Deuschl, C.; Wrede, K.H.; Kleinschnitz, C.; Sure, U.; et al. Subarachnoid Hemorrhage Early Brain Edema Score (SEBES) as a radiographic marker of clinically relevant intracranial hypertension and unfavorable outcome after subarachnoid hemorrhage. Eur. J. Neurol. 2021, 28, 4051–4059. [Google Scholar] [CrossRef]
- Darkwah Oppong, M.; Buffen, K.; Pierscianek, D.; Herten, A.; Ahmadipour, Y.; Dammann, P.; Rauschenbach, L.; Forsting, M.; Sure, U.; Jabbarli, R. Secondary hemorrhagic complications in aneurysmal subarachnoid hemorrhage: When the impact hits hard. J. Neurosurg. 2019, 132, 79–86. [Google Scholar] [CrossRef] [PubMed]
- Jabbarli, R.; Oppong, M.D.; Dammann, P.; Wrede, K.H.; El Hindy, N.; Ozkan, N.; Muller, O.; Forsting, M.; Sure, U. Time Is Brain! Analysis of 245 Cases with Decompressive Craniectomy due to Subarachnoid Hemorrhage. World Neurosurg. 2017, 98, 689–694.e2. [Google Scholar] [CrossRef] [PubMed]
- Hahn, F.J.; Rim, K. Frontal ventricular dimensions on normal computed tomography. Am. J. Roentgenol. 1976, 126, 593–596. [Google Scholar] [CrossRef] [Green Version]
- Pelicci, L.J.; Bedrick, A.D.; Cruse, R.P.; Vannucci, R.C. Frontal ventricular dimensions of the brain in infants and children. Arch. Neurol. 1979, 36, 852–853. [Google Scholar] [CrossRef]
- Brinkman, S.D.; Sarwar, M.; Levin, H.S.; Morris, H.H., 3rd. Quantitative indexes of computed tomography in dementia and normal aging. Radiology 1981, 138, 89–92. [Google Scholar] [CrossRef]
- Huckman, M.S.; Fox, J.; Topel, J. The validity of criteria for the evaluation of cerebral atrophy by computed tomography. Radiology 1975, 116, 85–92. [Google Scholar] [CrossRef] [PubMed]
- Teasdale, G.M.; Drake, C.G.; Hunt, W.; Kassell, N.; Sano, K.; Pertuiset, B.; De Villiers, J.C. A universal subarachnoid hemorrhage scale: Report of a committee of the World Federation of Neurosurgical Societies. J. Neurol. Neurosurg. Psychiatry 1988, 51, 1457. [Google Scholar] [CrossRef] [Green Version]
- Fisher, C.M.; Kistler, J.P.; Davis, J.M. Relation of cerebral vasospasm to subarachnoid hemorrhage visualized by computerized tomographic scanning. Neurosurgery 1980, 6, 1–9. [Google Scholar] [CrossRef]
- Ahn, S.H.; Savarraj, J.P.; Pervez, M.; Jones, W.; Park, J.; Jeon, S.B.; Kwon, S.U.; Chang, T.R.; Lee, K.; Kim, D.H.; et al. The Subarachnoid Hemorrhage Early Brain Edema Score Predicts Delayed Cerebral Ischemia and Clinical Outcomes. Neurosurgery 2018, 83, 137–145. [Google Scholar] [CrossRef]
- van Swieten, J.C.; Koudstaal, P.J.; Visser, M.C.; Schouten, H.J.; van Gijn, J. Interobserver agreement for the assessment of handicap in stroke patients. Stroke 1988, 19, 604–607. [Google Scholar] [CrossRef] [Green Version]
- Rass, V.; Helbok, R. Early Brain Injury after Poor-Grade Subarachnoid Hemorrhage. Curr. Neurol. Neurosci. Rep. 2019, 19, 78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schneider, U.C.; Xu, R.; Vajkoczy, P. Inflammatory Events Following Subarachnoid Hemorrhage (SAH). Curr. Neuropharmacol. 2018, 16, 1385–1395. [Google Scholar] [CrossRef] [PubMed]
- DiSabato, D.J.; Quan, N.; Godbout, J.P. Neuroinflammation: The devil is in the details. J. Neurochem. 2016, 139 (Suppl. S2), 136–153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gilhus, N.E.; Deuschl, G. Neuroinflammation—A common thread in neurological disorders. Nat. Rev. Neurol. 2019, 15, 429–430. [Google Scholar] [CrossRef] [PubMed]
- Jin, J.; Duan, J.; Du, L.; Xing, W.; Peng, X.; Zhao, Q. Inflammation and immune cell abnormalities in intracranial aneurysm subarachnoid hemorrhage (SAH): Relevant signaling pathways and therapeutic strategies. Front. Immunol. 2022, 13, 1027756. [Google Scholar] [CrossRef] [PubMed]
- Minami, N.; Tani, E.; Maeda, Y.; Yamaura, I.; Fukami, M. Effects of inhibitors of protein kinase C and calpain in experimental delayed cerebral vasospasm. J. Neurosurg. 1992, 76, 111–118. [Google Scholar] [CrossRef] [PubMed]
- Mathiesen, T.; Andersson, B.; Loftenius, A.; von Holst, H. Increased interleukin-6 levels in cerebrospinal fluid following subarachnoid hemorrhage. J. Neurosurg. 1993, 78, 562–567. [Google Scholar] [CrossRef] [Green Version]
- Geraghty, J.R.; Lung, T.J.; Hirsch, Y.; Katz, E.A.; Cheng, T.; Saini, N.S.; Pandey, D.K.; Testai, F.D. Systemic Immune-Inflammation Index Predicts Delayed Cerebral Vasospasm After Aneurysmal Subarachnoid Hemorrhage. Neurosurgery 2021, 89, 1071–1079. [Google Scholar] [CrossRef]
- Guresir, E.; Lampmann, T.; Bele, S.; Czabanka, M.; Czorlich, P.; Gempt, J.; Goldbrunner, R.; Hurth, H.; Hermann, E.; Jabbarli, R.; et al. Fight INflammation to Improve outcome after aneurysmal Subarachnoid HEmorRhage (FINISHER) trial: Study protocol for a randomized controlled trial. Int. J. Stroke 2022, 18, 17474930221093501. [Google Scholar] [CrossRef]
- Monsour, M.; Croci, D.M.; Agazzi, S. Microclots in subarachnoid hemorrhage: An underestimated factor in delayed cerebral ischemia? Clin. Neurol. Neurosurg. 2022, 219, 107330. [Google Scholar] [CrossRef]
- Gusdon, A.M.; Savarraj, J.P.J.; Shihabeddin, E.; Paz, A.; Assing, A.; Ko, S.B.; McCullough, L.D.; Choi, H.A. Time Course of Peripheral Leukocytosis and Clinical Outcomes After Aneurysmal Subarachnoid Hemorrhage. Front. Neurol. 2021, 12, 694996. [Google Scholar] [CrossRef] [PubMed]
- Gomis, P.; Graftieaux, J.P.; Sercombe, R.; Hettler, D.; Scherpereel, B.; Rousseaux, P. Randomized, double-blind, placebo-controlled, pilot trial of high-dose methylprednisolone in aneurysmal subarachnoid hemorrhage. J. Neurosurg. 2010, 112, 681–688. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Czorlich, P.; Sauvigny, T.; Ricklefs, F.; Abboud, T.; Nierhaus, A.; Vettorazzi, E.; Reuter, D.A.; Regelsberger, J.; Westphal, M.; Schmidt, N.O. Impact of dexamethasone in patients with aneurysmal subarachnoid haemorrhage. Eur. J. Neurol. 2017, 24, 645–651. [Google Scholar] [CrossRef]
- Mohney, N.; Williamson, C.A.; Rothman, E.; Ball, R.; Sheehan, K.M.; Pandey, A.S.; Fletcher, J.J.; Jacobs, T.L.; Thompson, B.G.; Rajajee, V. A Propensity Score Analysis of the Impact of Dexamethasone Use on Delayed Cerebral Ischemia and Poor Functional Outcomes After Subarachnoid Hemorrhage. World Neurosurg. 2018, 109, e655–e661. [Google Scholar] [CrossRef]
- Heiss, J.D.; Papavassiliou, E.; Merrill, M.J.; Nieman, L.; Knightly, J.J.; Walbridge, S.; Edwards, N.A.; Oldfield, E.H. Mechanism of dexamethasone suppression of brain tumor-associated vascular permeability in rats. Involvement of the glucocorticoid receptor and vascular permeability factor. J. Clin. Invest. 1996, 98, 1400–1408. [Google Scholar] [CrossRef]
- Lauzier, D.C.; Jayaraman, K.; Yuan, J.Y.; Diwan, D.; Vellimana, A.K.; Osbun, J.W.; Chatterjee, A.R.; Athiraman, U.; Dhar, R.; Zipfel, G.J. Early Brain Injury after Subarachnoid Hemorrhage: Incidence and Mechanisms. Stroke 2023. [Google Scholar] [CrossRef]
- Lolansen, S.D.; Rostgaard, N.; Barbuskaite, D.; Capion, T.; Olsen, M.H.; Norager, N.H.; Vilhardt, F.; Andreassen, S.N.; Toft-Bertelsen, T.L.; Ye, F.; et al. Posthemorrhagic hydrocephalus associates with elevated inflammation and CSF hypersecretion via activation of choroidal transporters. Fluids Barriers CNS 2022, 19, 62. [Google Scholar] [CrossRef]
- Rubinos, C.; Kwon, S.B.; Megjhani, M.; Terilli, K.; Wong, B.; Cespedes, L.; Ford, J.; Reyes, R.; Kirsch, H.; Alkhachroum, A.; et al. Predicting Shunt Dependency from the Effect of Cerebrospinal Fluid Drainage on Ventricular Size. Neurocrit. Care 2022, 37, 670–677. [Google Scholar] [CrossRef] [PubMed]
- Weigl, C.; Bruendl, E.; Schoedel, P.; Schebesch, K.M.; Brawanski, A.; Kieninger, M.; Bele, S. III. Ventricle diameter increase during ventricular drainage challenge—A predictor of shunt dependency after subarachnoid hemorrhage. J. Clin. Neurosci. 2020, 72, 198–201. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Number of Cases (% *) or Mean (±SD) |
|---|---|
| Ventricular measurements | |
| Bifrontal ratio: A/a | 0.339 (±0.057) |
| Bicaudate ratio: B/b | 0.166 (±0.081) |
| Ventricular ratio: B/A | 0.517 (±0.214) |
| Third ventricle ratio: C/c | 0.062 (±0.046) |
| Evans’ index: A/D | 0.275 (±0.046) |
| Huckman’s index: A + B (cm) | 5.419 (±1.244) |
| Demographic characteristics | |
| Age (years) | 54.7 (±13.9) |
| Sex (female) | 497 (66.7%) |
| SAH characteristics | |
| WFNS (grade 4–5) | 360 (48.3%) |
| SEBES (grade 3–4) | 386 (52.1%) |
| Fisher’s scale (grade 3–4) | 638 (90.1%) |
| Clipping | 302 (40.5%) |
| Presence of IVH | 390 (52.4%) |
| Acute hydrocephalus | 570 (76.5%) |
| Neurologic complications during SAH | |
| Aneurysm rebleeding | 49 (6.6%) |
| DIND | 193 (31.3%) |
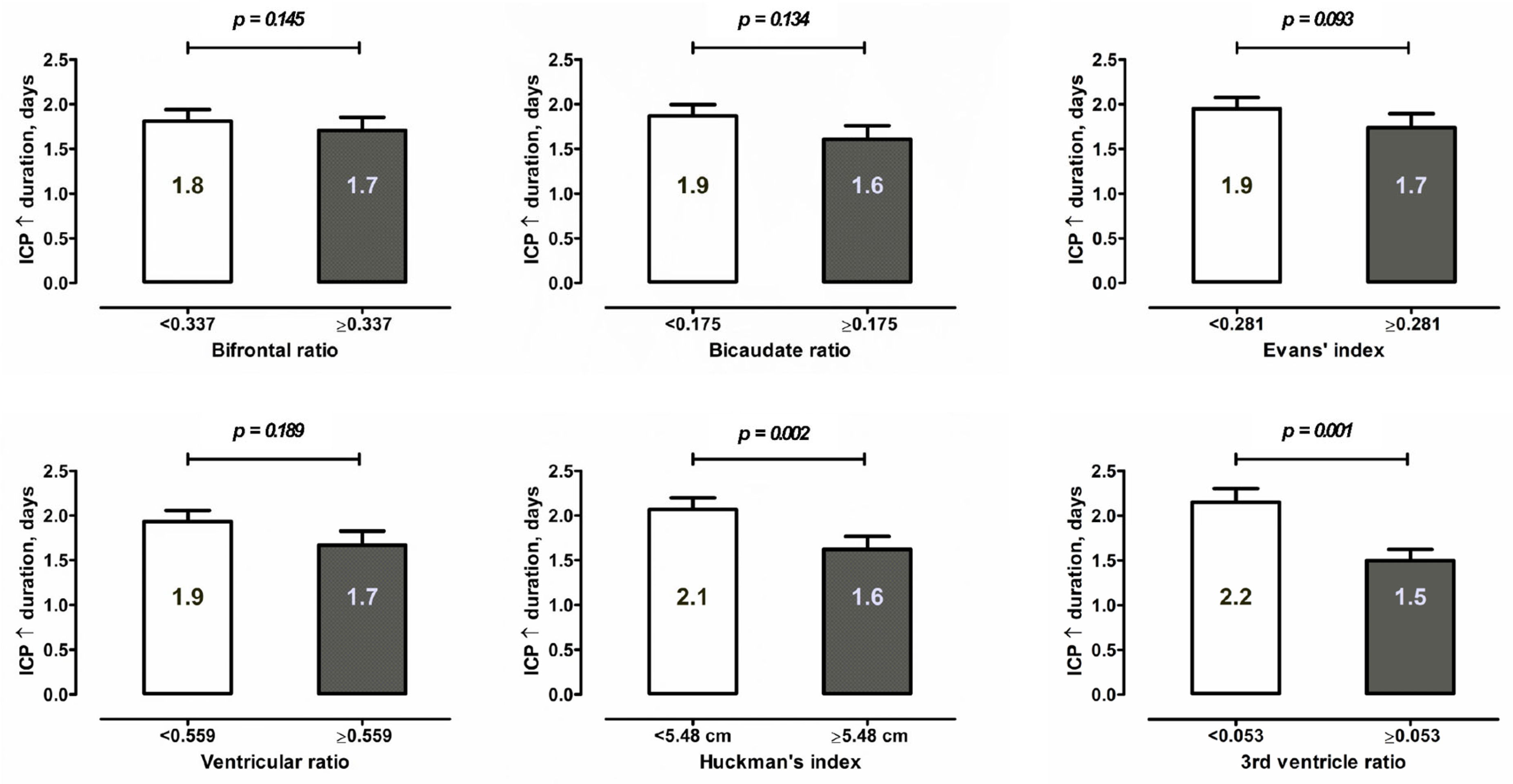
| Pathologic ICP increase | 368 (49.9%) |
| Decompressive craniectomy | 228 (30.6%) |
| TCD vasospasm | 340 (53.0%) |
| Early angiographic vasospasms (within 72 h) | 57 (9.7%) |
| Endovascular treatment of vasospasm | 171 (23.0%) |
| Epileptic seizures | 68 (9.1%) |
| Systemic complications during SAH | |
| Systemic infections | 310 (46.3%) |
| Acute coronary syndrome | 20 (3.1%) |
| Acute kidney failure | 9 (1.4%) |
| Primary study endpoints | |
| Cerebral infarction (s) | 380 (51.4%) |
| In-hospital mortality | 159 (21.3%) |
| Unfavorable outcome at 6 months (mRS > 3) | 296 (42.9%) |
| Ventricular Ratio/Index | aOR (95% CI) | p-Value |
|---|---|---|
| Cerebral infarction | ||
| Age >55 years | 1.39 (0.97–1.99) | 0.073 |
| WFNS grade 4–5 | 2.57 (1.82–3.62) | <0.0001 |
| SEBES 3–4 | 1.61 (1.13–2.28) | 0.008 |
| Fisher’s grade 3–4 | 1.50 (0.84–2.69) | 0.174 |
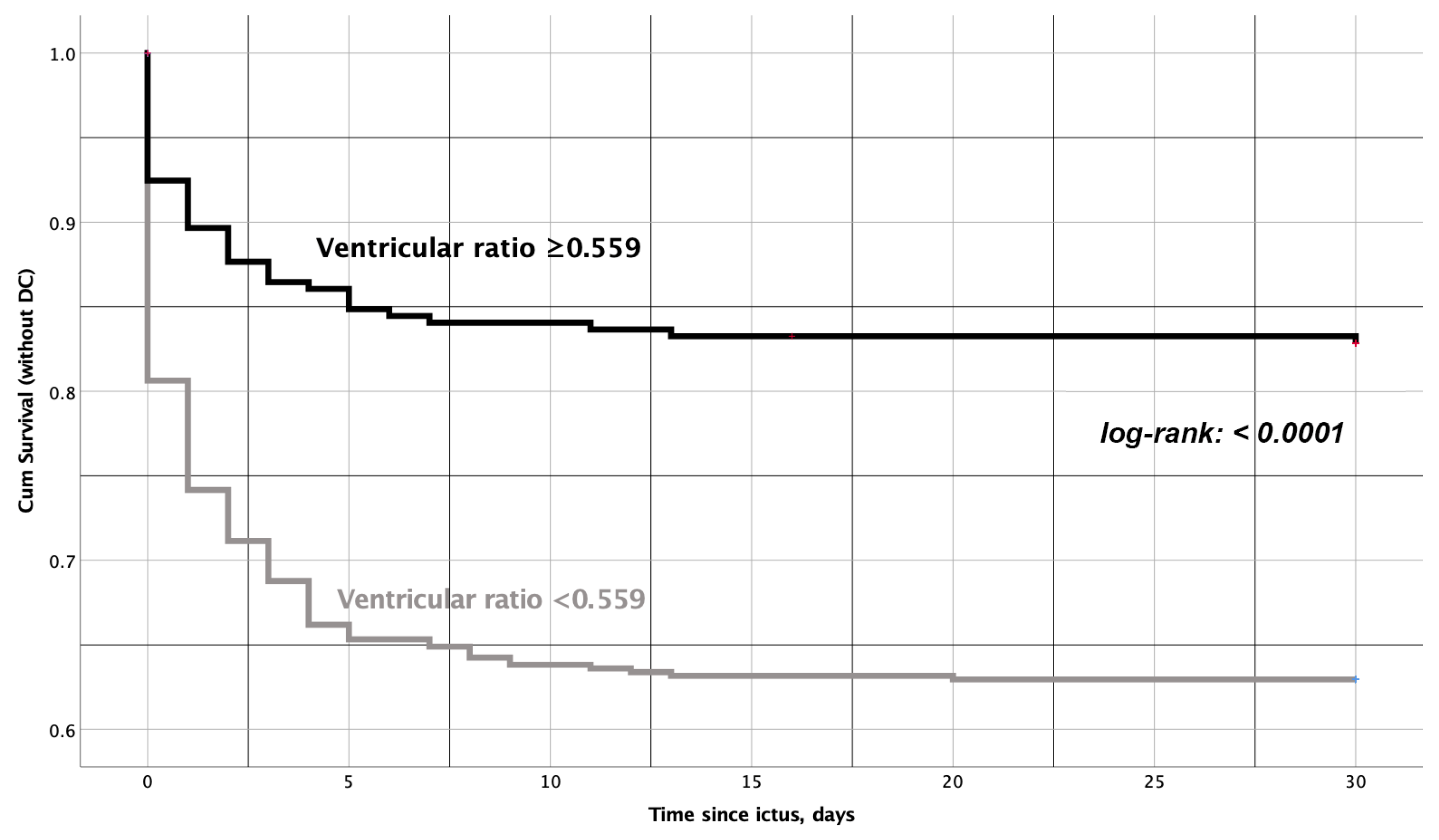
| Ventricular ratio ≥0.559 | 1.54 (1.07–2.19) | 0.017 |
| In-hospital mortality | ||
| Age >55 years | 1.81 (1.17–2.79) | 0.007 |
| WFNS grade 4–5 | 3.57 (2.28–5.58) | <0.0001 |
| SEBES 3–4 | 1.49 (0.96–2.31) | 0.074 |
| Fisher’s grade 3–4 | 4.12 (0.96–17.67) | 0.057 |
| Bicaudate ratio ≥0.175 | 1.61 (1.06–2.44) | 0.025 |
| Unfavorable outcome at 6 months after SAH * | ||
| Age >55 years | 2.75 (1.78–4.23) | <0.0001 |
| WFNS grade 4–5 | 7.03 (4.69–10.56) | <0.0001 |
| SEBES 3–4 | 1.73 (1.12–2.69) | 0.013 |
| Fisher’s grade 3–4 | 4.68 (1.57–13.97) | 0.006 |
| Evans’ index ≥0.281 | 1.67 (1.10–2.53) | 0.017 |
| Ventricular ratio ≥0.559 | 1.73 (1.12–2.65) | 0.013 |
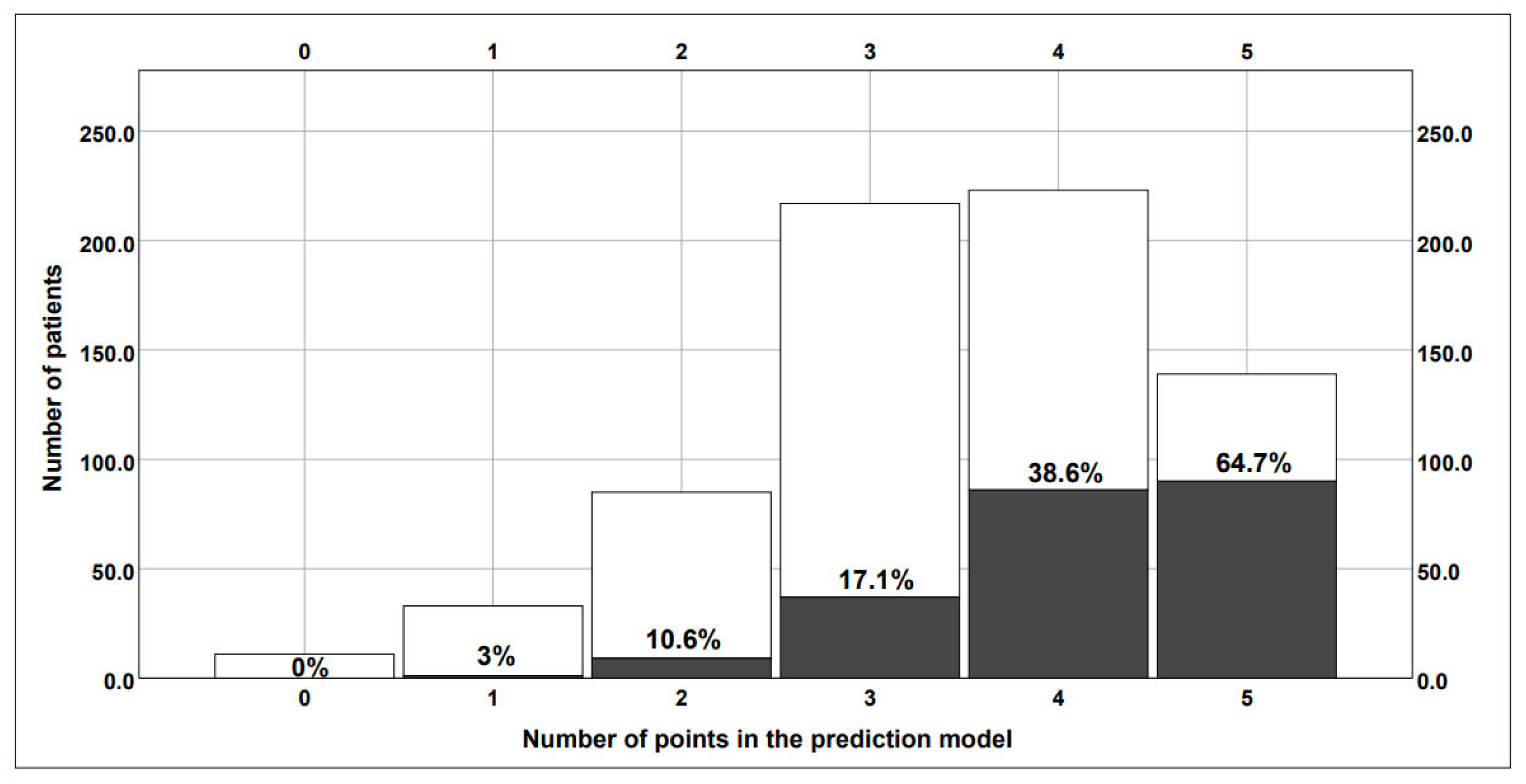
| Parameter | Score Weight |
|---|---|
| WFNS grade 4–5 | 1 |
| SEBES 3–4 | 1 |
| Fisher’s grade 3–4 | 2 |
| Ventricular ratio <0.559 | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Said, M.; Gümüs, M.; Rodemerk, J.; Chihi, M.; Rauschenbach, L.; Dinger, T.F.; Darkwah Oppong, M.; Ahmadipour, Y.; Dammann, P.; Wrede, K.H.; et al. Morphometric Study of the Initial Ventricular Indices to Predict the Complications and Outcome of Aneurysmal Subarachnoid Hemorrhage. J. Clin. Med. 2023, 12, 2585. https://doi.org/10.3390/jcm12072585
Said M, Gümüs M, Rodemerk J, Chihi M, Rauschenbach L, Dinger TF, Darkwah Oppong M, Ahmadipour Y, Dammann P, Wrede KH, et al. Morphometric Study of the Initial Ventricular Indices to Predict the Complications and Outcome of Aneurysmal Subarachnoid Hemorrhage. Journal of Clinical Medicine. 2023; 12(7):2585. https://doi.org/10.3390/jcm12072585
Chicago/Turabian StyleSaid, Maryam, Meltem Gümüs, Jan Rodemerk, Mehdi Chihi, Laurèl Rauschenbach, Thiemo F. Dinger, Marvin Darkwah Oppong, Yahya Ahmadipour, Philipp Dammann, Karsten H. Wrede, and et al. 2023. "Morphometric Study of the Initial Ventricular Indices to Predict the Complications and Outcome of Aneurysmal Subarachnoid Hemorrhage" Journal of Clinical Medicine 12, no. 7: 2585. https://doi.org/10.3390/jcm12072585