
Acute Coronary Syndrome, Stroke, and Mortality after Community-Acquired Pneumonia: Systematic Review and Meta-Analysis

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Roger, V.L. Epidemiology of Myocardial Infarction. Med. Clin. N. Am. 2007, 91, 537–552. [Google Scholar] [CrossRef] [Green Version]
- Writing Group Members; Mozaffarian, D.; Benjamin, E.J.; Go, A.S.; Arnett, D.K.; Blaha, M.J.; Cushman, M.; Das, S.R.; De Ferranti, S.; Després, J.-P.; et al. Executive Summary: Heart Disease and Stroke Statistics—2016 Update: A Report from the American Heart Association. Circulation 2016, 133, 447–454. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nichols, M.; Townsend, N.; Scarborough, P.; Rayner, M. Cardiovascular disease in Europe 2014: Epidemiological update. Eur. Heart J. 2014, 35, 2950–2959. [Google Scholar] [CrossRef] [Green Version]
- Storms, A.D.; Chen, J.; Jackson, L.A.; Nordin, J.; Naleway, A.L.; Glanz, J.M.; Jacobsen, S.J.; Weintraub, E.S.; Klein, N.P.; Gargiullo, P.M.; et al. Rates and risk factors associated with hospitalization for pneumonia with ICU admission among adults. BMC Pulm. Med. 2017, 17, 208. [Google Scholar] [CrossRef] [Green Version]
- Birnbaum, H.G.; Morley, M.; Greenberg, P.E.; Cifaldi, M.; Colice, G.L. Economic burden of pneumonia in an employed population. Arch. Intern. Med. 2001, 161, 2725–2731. [Google Scholar] [CrossRef] [PubMed]
- Johnson, N.B.; Hayes, L.D.; Brown, K.; Hoo, E.C.; Ethier, K.A.; Centers for Disease Control and Prevention (CDC). CDC National Health Report: Leading causes of morbidity and mortality and associated behavioral risk and protective factors—United States, 2005–2013. MMWR Suppl. 2014, 63, 3–27. [Google Scholar]
- Bruns, A.H.W.; Oosterheert, J.J.; Cucciolillo, M.C.; El Moussaoui, R.; Groenwold, R.H.H.; Prins, J.M.; Hoepelman, A.I.M. Cause-specific long-term mortality rates in patients recovered from community-acquired pneumonia as compared with the general Dutch population. Clin. Microbiol. Infect. 2011, 17, 763–768. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Park, S.J.; Choi, S.; Seo, W.-W.; Lee, Y.J. Hospitalization for acute coronary syndrome increases the long-term risk of pneumonia: A population-based cohort study. Sci. Rep. 2021, 11, 9696. [Google Scholar] [CrossRef]
- Armstrong, J.R.; Mosher, B.D. Aspiration Pneumonia After Stroke: Intervention and prevention. Neurohospitalist 2011, 1, 85–93. [Google Scholar] [CrossRef]
- Singanayagam, A.; Elder, D.H.J.; Chalmers, J.D. Is community-acquired pneumonia an independent risk factor for cardiovascular disease? Eur. Respir. J. 2012, 39, 187–196. [Google Scholar] [CrossRef] [Green Version]
- Restrepo, M.I.; Reyes, L.F. Pneumonia as a cardiovascular disease. Respirology 2018, 23, 250–259. [Google Scholar] [CrossRef] [Green Version]
- Corrales-Medina, V.F.; Suh, K.N.; Rose, G.; Chirinos, J.A.; Doucette, S.; Cameron, D.W.; Fergusson, D.A. Cardiac Complications in Patients with Community-Acquired Pneumonia: A Systematic Review and Meta-Analysis of Observational Studies. PLOS Med. 2011, 8, e1001048. [Google Scholar] [CrossRef] [Green Version]
- Tralhão, A.; Póvoa, P. Cardiovascular Events after Community-Acquired Pneumonia: A Global Perspective with Systematic Review and Meta-Analysis of Observational Studies. J. Clin. Med. 2020, 9, 414. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.T.; Green, S. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions, Version 5.1.0; Updated March 2011; The Cochrane Collaboration and John Wiley & Sons Ltd.: Glasgow, UK, 2011; Available online: http://handbook-5-1.cochrane.org/ (accessed on 2 February 2023).
- Moher, D.; Liberati, M.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Shea, B.J.; Reeves, B.C.; Wells, G.; Thuku, M.; Hamel, C.; Moran, J.; Moher, D.; Tugwell, P.; Welch, V.; Kristjansson, E.; et al. AMSTAR 2: A critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ 2017, 358, j4008. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wells, G.A.; Shea, B.; O’Connell, D.; Pereson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses; Ottawa Hospital Research Institute: Ottawa, ON, Canada, 2013; Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 28 July 2022).
- Corrales-Medina, V.F.; Alvarez, K.N.; Weissfeld, L.A.; Angus, D.C.; Chirinos, J.A.; Chang, C.-C.H.; Newman, A.; Loehr, L.; Folsom, A.R.; Elkind, M.S.; et al. Association Between Hospitalization for Pneumonia and Subsequent Risk of Cardiovascular Disease. JAMA 2015, 313, 264–274. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Corrales-Medina, V.F.; Musher, D.M.; Wells, G.A.; Chirinos, J.A.; Chen, L.; Fine, M.J. Cardiac complications in patients with community-acquired pneumonia: Incidence, timing, risk factors, and association with short-term mortality. Circulation 2012, 125, 773–781. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnstone, J.; Eurich, D.T.; Majumdar, S.R.; Jin, Y.; Marrie, T.J. Long-term morbidity and mortality after hospitalization with community-acquired pneumonia: A population-based cohort study. Medicine 2008, 8, 329–334. [Google Scholar] [CrossRef]
- Viasus, D.; Garcia-Vidal, C.; Manresa, F.; Dorca, J.; Gudiol, F.; Carratalà, J. Risk stratification and prognosis of acute cardiac events in hospitalized adults with community-acquired pneumonia. J. Infect. 2013, 66, 27–33. [Google Scholar] [CrossRef] [PubMed]
- Lazo, B.D. Complicaciones Cardiovasculares en Pacientes Hospitalizados por Neumonía en el Hospital Casimiro Ulloa-2014. Physician Degree Thesis, Faculty of Human Medicine, Ricardo Palma University, Lima, Peru, 2016. Available online: https://repositorio.urp.edu.pe/handle/20.500.14138/539 (accessed on 1 February 2023).
- Musher, D.M.; Rueda, A.M.; Kaka, A.S.; Mapara, S.M. The Association between Pneumococcal Pneumonia and Acute Cardiac Events. Clin. Infect. Dis. 2007, 45, 158–165. [Google Scholar] [CrossRef] [Green Version]
- Ramirez, J.; Aliberti, S.; Mirsaeidi, M.; Peyrani, P.; Filardo, G.; Amir, A.; Moffett, B.; Gordon, J.; Blasi, F.; Bordon, J. Acute myocardial infarction in hospitalized patients with community-acquired pneumonia. Clin. Infect. Dis. 2008, 47, 182–187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mortensen, E.M.; Coley, C.M.; Singer, D.E.; Marrie, T.J.; Obrosky, D.S.; Kapoor, W.N.; Fine, M.J. Causes of death for patients with community-acquired pneumonia: Results from the Pneumonia Patient Outcomes Research Team cohort study. Arch. Intern. Med. 2002, 162, 1059–1064. [Google Scholar] [CrossRef]
- Fuertes, J.A.G.; Molina, J.P.; Dominguez, I.J.; Mugica, M.B.L.; Mora, M.C.B.; Gomez, A.M.A.; Sierra, L.T.; Beristain, J.L.L. Acute Pneumonia and PSI: Is it posible to prevent a cardiovascular event? Eur. Respir. J. 2020, 56, 1776. [Google Scholar] [CrossRef]
- Baskaran, V.; Mckeever, T.; Shen, L.W. Incidence of Cardiac Complications after Hospitalization for Community Acquired Pneumonia: A Large Population-based Cohort Study. Eur. Respir. J. 2020, 56, 1772. [Google Scholar] [CrossRef]
- Kang, Y.; Fang, X.Y.; Wang, D.; Wang, X.J. Factors associated with acute myocardial infarction in older patients after hospitalization with community-acquired pneumonia: A cross-sectional study. BMC Geriatr. 2021, 21, 113. [Google Scholar] [CrossRef]
- Pieralli, F.; Vannucchi, V.; Nozzoli, C.; Augello, G.; Dentali, F.; De Marzi, G.; Uomo, G.; Risaliti, F.; Morbidoni, L.; Mazzone, A.; et al. Acute cardiovascular events in patients with community acquired pneumonia: Results from the observational prospective FADOI-ICECAP study. BMC Infect. Dis. 2021, 25, 116. [Google Scholar] [CrossRef]
- Huang, X.; Zhang, J.; Huang, X.; Zeng, M.; Chen, Y. Predictors of 30-day mortality in elderly patients with community acquired pneumonia. Eur. Respir. J. 2015, 46, PA2571. [Google Scholar] [CrossRef]
- Campos, C.C.; Liapikou, A.; Martin-Loeches, I.; Garcia-Vidal, C.; Gabarrus, A.; Ceccato, A.; Mensa, J.; Marco, F. Twenty-year Trend in Mortality among Hospitalized Patients with Pneumococcal Community-Acquired Pneumonia. Eur. Respir. J. 2018, 52, PA2626. [Google Scholar] [CrossRef] [Green Version]
- Allen, S.C. Lobar pneumonia in Northern Zambia: Clinical study of 502 adult patients. Thorax 1984, 39, 612–616. [Google Scholar] [CrossRef] [Green Version]
- Esposito, A.L. Community-acquired bacteremic pneumococcal pneumonia. Effect of age on manifestations and outcome. Arch. Intern. Med. 1984, 144, 945–948. [Google Scholar] [CrossRef] [PubMed]
- Marrie, T.J.; Durant, H.; Yates, L. Community-acquired pneumonia requiring hospitalization: 5-year prospective study. Rev. Infect. Dis. 1989, 11, 586–599. [Google Scholar] [CrossRef] [PubMed]
- Ortqvist, A.; Hedlund, J.; Grillner, L.; Jalonen, E.; Kallings, I.; Leinonen, M.; Kalin, M. Aetiology, outcome and prognostic factors in community-acquired pneumonia requiring hospitalization. Eur. Respir. J. 1990, 3, 1105–1113. [Google Scholar] [CrossRef] [PubMed]
- Venkatesan, P.; Gladman, J.; Macfarlane, J.T.; Barer, D.; Berman, P.; Kinnear, W.; Finch, R.G. A hospital study of community acquired pneumonia in the elderly. Thorax 1990, 45, 254–258. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fine, M.J.; Smith, D.N.; Singer, D.E. Hospitalization decision in patients with community-acquired pneumonia: A prospective cohort study. Am. J. Med. 1990, 89, 713–721. [Google Scholar] [CrossRef]
- Leroy, O.; Santre, C.; Beuscart, C.; Georges, H.; Guery, B.; Jacquier, J.M.; Beaucaire, G. A five-year study of severe community-acquired pneumonia with emphasis on prognosis in patients admitted to an intensive care unit. Intensive Care Med. 1995, 21, 24–31. [Google Scholar] [CrossRef]
- Janssens, J.P.; Gauthey, L.; Herrmann, F.; Tkatch, L.; Michel, J.P. Community-acquired pneumonia in older patients. J. Am. Geriatr. Soc. 1996, 44, 539–544. [Google Scholar] [CrossRef]
- The British Thoracic Society Research Committee and The Public Health Laboratory Service. The aetiology, management and outcome of severe community-acquired pneumonia on the intensive care unit. Respir. Med. 1992, 86, 7–13. [Google Scholar] [CrossRef]
- Fine, M.J.; Stone, R.A.; Singer, D.E.; Coley, C.M.; Marrie, T.J.; Lave, J.R.; Hough, L.J.; Obrosky, D.S.; Schulz, R.; Ricci, E.M.; et al. Processes and outcomes of care for patients with community-acquired pneumonia: Results from the Pneumonia Patient Outcomes Research Team (PORT) cohort study. Arch Intern. Med. 1999, 159, 970–980. [Google Scholar] [CrossRef] [Green Version]
- Musher, D.M.; Alexandraki, I.; Graviss, E.A.; Yanbeiy, N.; Eid, A.; Inderias, L.A.; Phan, H.M.; Solomon, E. Bacteremic and nonbacteremic pneumococcal pneumonia. A prospective study. Medicine 2000, 79, 210–221. [Google Scholar] [CrossRef]
- Fernández-Sabé, N.; Carratalà, J.; Rosón, B.; Dorca, J.; Verdaguer, R.; Manresa, F.; Gudiol, F. Community-acquired pneumonia in very elderly patients: Causative organisms, clinical characteristics, and outcomes. Medicine 2003, 82, 159–169. [Google Scholar] [CrossRef]
- Fine, M.J.; Stone, R.A.; Lave, J.R.; Hough, L.J.; Obrosky, D.S.; Mor, M.K.; Kapoor, W.N. Implementation of an evidence-based guideline to reduce duration of intravenous antibiotic therapy and length of stay for patients hospitalized with community-acquired pneumonia: A randomized controlled trial. Am. J. Med. 2003, 115, 343–351. [Google Scholar] [CrossRef]
- Martínez-Moragón, E.; García Ferrer, L.; Serra Sanchis, B.; Fernández Fabrellas, E.; Gómez Belda, A.; Julve Pardo, R. La neumonía adquirida en la comunidad de los ancianos: Diferencias entre los que viven en residencias y en domicilios particulares [Community-acquired pneumonia among the elderly: Differences between patients living at home and in nursing homes]. Arch. Bronconeumol. 2004, 40, 547–552. (In Spanish) [Google Scholar] [CrossRef]
- Menéndez, R.; Torres, A.; Zalacaín, R.; Aspa, J.; Martín-Villasclaras, J.J.; Borderías, L.; Benítez-Moya, J.M.; Ruiz-Manzano, J.; de Castro, F.R.; Blanquer, J.; et al. Guidelines for the treatment of community-acquired pneumonia: Predictors of adherence and outcome. Am. J. Respir. Crit. Care Med. 2005, 172, 757–762. [Google Scholar] [CrossRef]
- Querol-Ribelles, J.M.; Tenías, J.M.; Querol-Borrás, J.M.; Labrador, T.; Nieto, A.; González-Granda, D.; Martínez, I. Levofloxacin versus ceftriaxone plus clarithromycin in the treatment of adults with community-acquired pneumonia requiring hospitalization. Int. J. Antimicrob. Agents 2005, 25, 75–83. [Google Scholar] [CrossRef] [PubMed]
- Díaz, A.; Alvarez, M.; Callejas, C.; Rosso, R.; Schnettler, K.; Saldías, F. Cuadro clínico y factores pronósticos de la neumonía adquirida en la comunidad grave en adultos hospitalizados en la unidad de cuidados intensivos [Clinical picture and prognostic factors for severe community-acquired pneumonia in adults admitted to the intensive care unit]. Arch. Bronconeumol. 2005, 41, 20–26. (In Spanish) [Google Scholar] [CrossRef]
- Marrie, T.J.; Huang, J.Q. Low-risk patients admitted with community-acquired pneumonia. Am. J. Med. 2005, 118, 1357–1363. [Google Scholar] [CrossRef]
- McAlister, F.A.; Majumdar, S.R.; Blitz, S.; Rowe, B.H.; Romney, J.; Marrie, T.J. The relation between hyperglycemia and outcomes in 2,471 patients admitted to the hospital with community-acquired pneumonia. Diabetes Care. 2005, 28, 810–815. [Google Scholar] [CrossRef] [Green Version]
- Becker, T.; Moldoveanu, A.; Cukierman, T.; Gerstein, H.C. Clinical outcomes associated with the use of subcutaneous insulin-by-glucose sliding scales to manage hyperglycemia in hospitalized patients with pneumonia. Diabetes Res. Clin. Pract. 2007, 78, 392–397. [Google Scholar] [CrossRef]
- Cabré, M.; Serra-Prat, M.; Force, L.; Palomera, E.; Pallarés, R. Functional status as a risk factor for mortality in very elderly patients with pneumonia. Med. Clin. 2008, 131, 167–170. [Google Scholar] [CrossRef] [PubMed]
- Mandal, P.; Chalmers, J.D.; Choudhury, G.; Akram, A.R.; Hill, A.T. Vascular complications are associated with poor outcome in community-acquired pneumonia. QJM 2011, 104, 489–495. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perry, T.W.; Pugh, M.J.V.; Waterer, G.W.; Nakashima, B.; Orihuela, C.J.; Copeland, L.A.; Restrepo, M.I.; Anzueto, A.; Mortensen, E.M. Incidence of cardiovascular events after hospital admission for pneumonia. Am. J. Med. 2011, 124, 244–251. [Google Scholar] [CrossRef] [Green Version]
- Griffin, A.T.; Wiemken, T.L.; Arnold, F.W. Risk factors for cardiovascular events in hospitalized patients with community-acquired pneumonia. Int. J. Infect. Dis. 2013, 17, e1125–e1129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aliberti, S.; Ramirez, J.; Cosentini, R.; Valenti, V.; Voza, A.; Rossi, P.; Stolz, D.; Legnani, D.; Pesci, A.; Richeldi, L.; et al. Acute myocardial infarction versus other cardiovascular events in community-acquired pneumonia. ERJ Open Res. 2015, 1, 00020–02015. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cangemi, R.; Calvieri, C.; Falcone, M.; Bucci, T.; Bertazzoni, G.; Scarpellini, M.G.; Barillà, F.; Taliani, G.; Violi, F.; Battaglia, S.; et al. Relation of Cardiac Complications in the Early Phase of Community-Acquired Pneumonia to Long-Term Mortality and Cardiovascular Events. Am. J. Cardiol. 2015, 116, 647–651. [Google Scholar] [CrossRef]
- Chen, P.C.; Liao, W.I.; Wang, Y.C.; Chang, W.C.; Hsu, C.W.; Chen, Y.H.; Tsai, S.H. An Elevated Glycemic Gap is Associated With Adverse Outcomes in Diabetic Patients With Community-Acquired Pneumonia. Medicine 2015, 94, e1456. [Google Scholar] [CrossRef]
- Violi, F.; Cangemi, R.; Falcone, M.; Taliani, G.; Pieralli, F.; Vannucchi, V.; Nozzoli, C.; Venditti, M.; Chirinos, J.A.; Corrales-Medina, V.F.; et al. Cardiovascular Complications and Short-term Mortality Risk in Community-Acquired Pneumonia. Clin. Infect. Dis. 2017, 64, 1486–1493. [Google Scholar] [CrossRef] [Green Version]
- Eurich, D.T.; Marrie, T.J.; Minhas-Sandhu, J.K.; Majumdar, S.R. Risk of heart failure after community acquired pneumonia: Prospective controlled study with 10 years of follow-up. BMJ 2017, 356, j413. [Google Scholar] [CrossRef] [Green Version]
- Cilli, A.; Cakin, O.; Aksoy, E.; Kargin, F.; Adiguzel, N.; Karakurt, Z.; Ergan, B.; Mersin, S.; Bozkurt, S.; Ciftci, F.; et al. Acute cardiac events in severe community-acquired pneumonia: A multicenter study. Clin. Respir. J. 2018, 12, 2212–2219. [Google Scholar] [CrossRef]
- Postma, D.F.; Spitoni, C.; van Werkhoven, C.H.; van Elden, L.J.R.; Oosterheert, J.J.; Bonten, M.J.M. Cardiac events after macrolides or fluoroquinolones in patients hospitalized for community-acquired pneumonia: Post-hoc analysis of a cluster-randomized trial. BMC Infect. Dis. 2019, 19, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pieralli, F.; Biondo, B.; Vannucchi, V.; Falcone, M.; Antonielli, E.; De Marzi, G.; Casati, C.; Maddaluni, L.; Nozzoli, C.; Olivotto, I. Performance of the CHA2DS2-VASc score in predicting new onset atrial fibrillation during hospitalization for community-acquired pneumonia. Eur. J. Intern. Med. 2019, 62, 24–28. [Google Scholar] [CrossRef] [PubMed]
- Cangemi, R.; Calvieri, C.; Taliani, G.; Pignatelli, P.; Morelli, S.; Falcone, M.; Pastori, D.; Violi, F.; SIXTUS Study Group. Left Atrium Dilatation and Left Ventricular Hypertrophy Predispose to Atrial Fibrillation in Patients With Community-Acquired Pneumonia. Am. J. Cardiol. 2019, 124, 723–728. [Google Scholar] [CrossRef]
- Corrales-Medina, V.F.; Taljaard, M.; Yende, S.; Kronmal, R.; Dwivedi, G.; Newman, A.B.; Elkind, M.S.; Lyles, M.F.; Chirinos, J.A. Intermediate and long-term risk of new-onset heart failure after hospitalization for pneumonia in elderly adults. Am. Heart J. 2015, 170, 306–312. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Corrales-Medina, V.F.; Taljaard, M.; Fine, M.J.; Dwivedi, G.; Perry, J.J.; Musher, D.M.; Chirinos, J.A. Risk stratification for cardiac complications in patients hospitalized for community-acquired pneumonia. Mayo Clin. Proc. 2014, 89, 60–68. [Google Scholar] [CrossRef]
- Fonseca, A.; Sá Marques, M.; Silva, E.; Shiang, T.; Vanzeller, M.; Ribeiro, C. Community acquired pneumonia: An increased risk for subsequent cardiovascular events? Eur. Respir. J. 2020, 56, 1775. [Google Scholar] [CrossRef]
- Meier, C.R.; Jick, S.S.; Derby, L.E.; Vasilakis, C.; Jick, H. Acute respiratory-tract infections and risk of first-time acute myocardial infarction. Lancet 1998, 351, 1467–1471. [Google Scholar] [CrossRef] [PubMed]
- Smeeth, L.; Thomas, S.L.; Hall, A.J.; Hubbard, R.; Farrington, P.; Vallance, P. Risk of Myocardial Infarction and Stroke after Acute Infection or Vaccination. N. Engl. J. Med. 2004, 351, 2611–2618. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clayton, T.C.; Thompson, M.; Meade, T.W. Recent respiratory infection and risk of cardiovascular disease: Case-control study through a general practice database. Eur. Heart J. 2008, 29, 96–103. [Google Scholar] [CrossRef] [Green Version]
- Nuñez-Delgado, R.D.P.; Tapia-Pérez, R.F.; Cachicatari-Vargas, E.; Chirinos-Lazo, R.M. Neumonía adquirida en la comunidad como factor de riesgo para enfermedades cardiovasculares. Rev. Cuerpo Med. HNAAA 2022, 15, 35–41. [Google Scholar] [CrossRef]
- Wang, C.-C.; Peng, C.-L.; Wang, G.-J.; Sung, F.-C.; Kao, C.-H. Pneumococcal pneumonia and the risk of acute coronary syndrome: A population-based cohort study. Int. J. Cardiol. 2013, 168, 4480–4481. [Google Scholar] [CrossRef]
- Koivula, I.; Stén, M.; Mäkelä, P.H. Prognosis after community-acquired pneumonia in the elderly: A population-based 12-year follow-up study. Arch. Intern. Med. 1999, 159, 1550–1555. [Google Scholar] [CrossRef] [Green Version]
- Yende, S.; D’Angelo, G.; Kellum, J.A.; Weissfeld, L.; Fine, J.; Welch, R.D.; Kong, L.; Carter, M.; Angus, D.C. Inflammatory Markers at Hospital Discharge Predict Subsequent Mortality after Pneumonia and Sepsis. Am. J. Respir. Crit. Care Med. 2008, 177, 1242–1247. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chung, W.-S.; Hsu, W.-H.; Lin, C.-L.; Kao, C.-H. Mycoplasma pneumonia increases the risk of acute coronary syndrome: A nationwide population-based cohort study. Qjm Int. J. Med. 2015, 108, 697–703. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, L.-F.; Chen, H.-P.; Huang, Y.-S.; Huang, K.-Y.; Chou, P.; Lee, C.-C. Pneumococcal Pneumonia and the Risk of Stroke: A Population-Based Follow-Up Study. PLoS ONE 2012, 7, e51452. [Google Scholar] [CrossRef]
- Corrales-Medina, V.F.; Serpa, J.; Rueda, A.M.; Giordano, T.P.; Bozkurt, B.; Madjid, M.; Tweardy, D.; Musher, D.M. Acute Bacterial Pneumonia is Associated With the Occurrence of Acute Coronary Syndromes. Medicine 2009, 88, 154–159. [Google Scholar] [CrossRef]
- O’Meara, E.S.; White, M.; Siscovick, D.S.; Lyles, M.F.; Kuller, L.H. Hospitalization for Pneumonia in the Cardiovascular Health Study: Incidence, Mortality, and Influence on Longer-Term Survival. J. Am. Geriatr. Soc. 2005, 53, 1108–1116. [Google Scholar] [CrossRef]
- Baskaran, V.; Quammie, S.; Lawrence, H.; Ashton, D.; Lim, W.S.; McKeever, T. Meta-analysis of Acute Coronary Syndrome in Patients with Community-Acquired Pneumonia. Eur. Respir. J. 2020, 56 (Suppl. 64), 1778. [Google Scholar] [CrossRef]
- Haynes, R.B.; Devereaux, P.; Guyatt, G.H. Clinical expertise in the era of evidence-based medicine and patient choice. ACP J. Club 2002, 136, A11–A14. [Google Scholar] [CrossRef]
- Balshem, H.; Helfand, M.; Schünemann, H.J.; Oxman, A.D.; Kunz, R.; Brozek, J.; Vist, G.E.; Falck-Ytter, Y.; Meerpohl, J.; Norris, S.; et al. GRADE guidelines: 3. Rating the quality of evidence. J. Clin. Epidemiol. 2011, 64, 401–406. [Google Scholar] [CrossRef]
- Jager, K.; Zoccali, C.; MacLeod, A.; Dekker, F. Confounding: What it is and how to deal with it. Kidney Int. 2008, 73, 256–260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kahlert, J.; Gribsholt, S.B.; Gammelager, H.; Dekkers, O.; Luta, G. Control of confounding in the analysis pase—An overview for clinicians. Clin. Epidemiol. 2017, 9, 195–204. [Google Scholar] [CrossRef] [Green Version]
- Anderson, R.; Feldman, C. Review manuscript: Mechanisms of platelet activation by the pneumococcus and the role of platelets in community-acquired pneumonia. J. Infect. 2017, 75, 473–485. [Google Scholar] [CrossRef] [Green Version]
- Anderson, R.; Nel, J.G.; Feldman, C. Multifaceted Role of Pneumolysin in the Pathogenesis of Myocardial Injury in Community-Acquired Pneumonia. Int. J. Mol. Sci. 2018, 19, 1147. [Google Scholar] [CrossRef] [Green Version]
- Arroyo, A.B.; Fernández-Pérez, M.P.; del Monte, A.; Águila, S.; Méndez, R.; Hernández-Antolín, R.; García-Barber, N.; Reyes-García, A.M.D.L.; González-Jiménez, P.; Arcas, M.I.; et al. miR-146a is a pivotal regulator of neutrophil extracellular trap formation promoting thrombosis. Haematologica 2021, 106, 1636–1646. [Google Scholar] [CrossRef] [PubMed]
- Brissac, T.; Shenoy, A.T.; Patterson, L.A.; Orihuela, C.J. Cell Invasion and Pyruvate Oxidase-Derived H2O2 are Critical for Streptococcus pneumoniae-Mediated Cardiomyocyte Killing. Infect. Immun. 2017, 86, e00569-17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cangemi, R.; Pignatelli, P.; Carnevale, R.; Bartimoccia, S.; Nocella, C.; Falcone, M.; Taliani, G.; Violi, F.; Battaglia, S.; Bertazzoni, G.; et al. Low-grade endotoxemia, gut permeability and platelet activation in community-acquired pneumonia. J. Infect. 2016, 73, 107–114. [Google Scholar] [CrossRef]
- Feldman, C.; Normark, S.; Normark, B.H.; Anderson, R. Pathogenesis and prevention of risk of cardiovascular events in patients with pneumococcal community-acquired pneumonia. J. Intern. Med. 2019, 285, 635–652. [Google Scholar] [CrossRef] [Green Version]
- Borenstein, M.; Hedges, L.V.; Higgins, J.P.; Rothstein, H.R. Introduction to Meta-Analysis, 1st ed.; John Wiley & Sons: Hoboken, NJ, USA, 2009; Available online: https://onlinelibrary.wiley.com/doi/book/10.1002/9780470743386 (accessed on 1 February 2023).
- Lin, L.; Chu, H. Meta-analysis of Proportions Using Generalized Linear Mixed Models. Epidemiology 2020, 31, 713–717. [Google Scholar] [CrossRef]
- Barker, T.H.; Migliavaca, C.B.; Stein, C.; Colpani, V.; Falavigna, M.; Aromataris, E.; Munn, Z. Conducting proportional meta-analysis in different types of systematic reviews: A guide for synthesisers of evidence. BMC Med. Res. Methodol. 2021, 21, 189. [Google Scholar] [CrossRef]
- Munn, Z.; Moola, S.; Lisy, K.; Riitano, D.; Tufanaru, C. Methodological guidance for systematic reviews of observational epidemiological studies reporting prevalence and cumulative incidence data. Int. J. Evid. -Based Healthc. 2015, 13, 147–153. [Google Scholar] [CrossRef]
- Barendregt, J.J.; Doi, S.; Lee, Y.Y.; Norman, R.E.; Vos, T. Meta-analysis of prevalence. J. Epidemiol. Community Health 2013, 67, 974–978. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thompson, S.G.; Sharp, S.J. Explaining heterogeneity in meta-analysis: A comparison of methods. Stat. Med. 1999, 18, 2693–2708. [Google Scholar] [CrossRef]
- Ioannidis, J.P.; Patsopoulos, N.; Evangelou, E. Heterogeneity in Meta-Analyses of Genome-Wide Association Investigations. PLoS ONE 2007, 2, e841. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study, Year (Region) | Participants, Study Design, Sample Characteristics | Exposition | Outcome | Adjustment Factors | OR/RR/HR (95% CI) |
|---|---|---|---|---|---|
| Meier [1], UK, 1986 | N = 9571. Cases (MI) 1922, controls (no MI) 7649. Two separate analyses: case-control and case-crossover study. Follow-up: 3 y. Both sexes. Age ≤75 years. Deaths among cases 285. Deaths among controls NR. | Acute RTI | First MI | Smoking and BMI | AOR = for first-time MI at 1–5, 6–10, 11–15, or 16–30 days after ARTI were 3.6 (2.2–5.7), 2.3 (1.3–4.2), 1.8 (1.0–3.3), and 1.0 (0.7–1.6). RR = 2.7 (1.6–4.7) for MI at 10 days after ARTI. |
| Smeeth [2], UK; 2004a | N = 65,746. First MI 53709. ARTI 20,921. ARTI and first MI 3254. Mean follow-up 5.6 y. Both sexes. Median age at MI 72.3 y. Case-series method. | Acute RTI | First MI | Age | AOR = for first MI at 1–3, 4–7, 8–14, 15–28, 29–91 days since ARTI were 4.95 (4.43–5.53), 3.20 (2.84–3.60), 2.81 (2.54–3.09), 1.95 (1.79–2.12), 1.95 (1.79–2.12), respectively. |
| Smeeth [2], UK; 2004b | N = 66,637 patients. First stroke 50,766. ARTI 22,400. ARTI and first stroke 3060. Mean follow-up 5.3 y. Both sexes. Median age at stroke 78.3 y. Case-series method. | Acute RTI | First stroke | Age | AOR = for first stroke at 1–3, 4–7, 8–14, 15–28, 29–91 days since ARTI were 3.19 (2.81–3.62), 2.34 (2.05–2.66), 2.09 (1.89–2.32), 1.68 (1.54–1.82), 1.33 (1.26–1.40), respectively. |
| Clayton [3], UK, 2008a | Cases (MI) 11,155. Controls (no MI) 11,155. Mean follow-up 1 y. Both sexes. Median age at MI 79 ± 14 y. Case-control study. | Acute RTI | First MI | Angina, smoking, DM, HT, PVD, family history of CAD, hyperlipidemia, previous stroke. | AOR = for first MI 2.10 (1.38–3.21), 1.93 (1.42–2.63), 1.16 (0.92–1.47), 1.08 (0.94–1.23), during the 1–7, 8–28, 29–91, 92–365 days following infection, respectively. |
| Clayton [3], UK, 2008b | Cases (stroke) 9208. Controls (no stroke) 9208. Mean follow-up 1 y. Both sexes. Median age at stroke 74 ± 13 y. Case-control study. | Acute RTI | First stroke | Smoking, DM, HT, PVD, previous MI, UTI | AOR = for stroke 1.92 (1.24–2.97), 1.76 (1.27–2.45), 1.09 (0.88–1.36), 1.08 (0.94–1.24), during the 1–7, 8–28, 29–91, 92–365 days following infection, respectively. |
| Nuñez-Delgado [4], Peru, 2022a | N = 693 (CAP 231, no CAP 462). Ambispective cohort. Follow-up: 2 y. CAP and MI 107, no CAP and MI 0. Both sexes. Age >30 years. Mean age 64.1 ± 13.7 years. | CAP | ACS (MI) | Smoking, HT, DM, hypercholesterolemia | ARR = 3.98 (2.98–5.33) for ACS. |
| Nuñez-Delgado [4], Peru, 2022b | N = 693 (CAP 231, no CAP 462). Ambispective cohort. Follow-up: 2 y. CAP and HF 75, no CAP and HF 0. Both sexes. Age >30 years. Mean age 64.1 ± 13.7 years. | CAP | HF | Smoking, HT, DM, hypercholesterolemia | ARR = 9.65 (8.45–11.0) for HF. |
| Nuñez-Delgado [4], Peru, 2022c | N = 693 (CAP 231, no CAP 462). Ambispective cohort. Follow-up: 2 years. CAP and arrhythmia 119, no CAP and arrhythmia 0. Both sexes. Age > 30 years. Mean age 64.1 ± 13.7 years. | CAP | Arrhythmias (AF, PSVT) | Smoking, HT, DM, hypercholesterolemia | ARR = 10.7 (8.64–13.2) for arrhythmias. |
| Wang [5], Taiwan, 2013 | CAP 20,111, no CAP 80,444. Prospective cohort study. CAP and ACS 1044, no CAP and ACS 332. Both sexes. Age ≥20 years. Follow-up 14 y. | CAP | First episode of ACS. | Age, sex, comorbidities (HT, DM, dyslipidemia, COPD). | ARR 1.92 (1.70–2.17) for ACS. ARR 3.90 (2.46–6.18) within 3 months; ARR = 2.43 (1.75–3.38) within 1 year, ARR 1.74 (1.51–2.00) >1 year. AHR = 1.47 (1.24–1.73) for ACS in the following 14 years. AHR = 1.18 (1.02–1.37) for ACS in males. |
| Koivula [6], Finland, 1999a | N = 4167. CAP 122. Follow-up 9.2 y. Prospective observational (cohort) study. No CAP 4045. Both sexes. Age ≥60 y. Deaths 1979. Mean follow-up 9.2 y. | CAP | Total mortality, cardiovascular mortality | Age, sex, and multiple comorbidities. | ARR 2.1 (1.3–3.4) for pneumonia-related mortality. ARR 1.5 (1.2–1.9) for total mortality. ARR 1.4 (1.0–1.9) for cardiovascular mortality. |
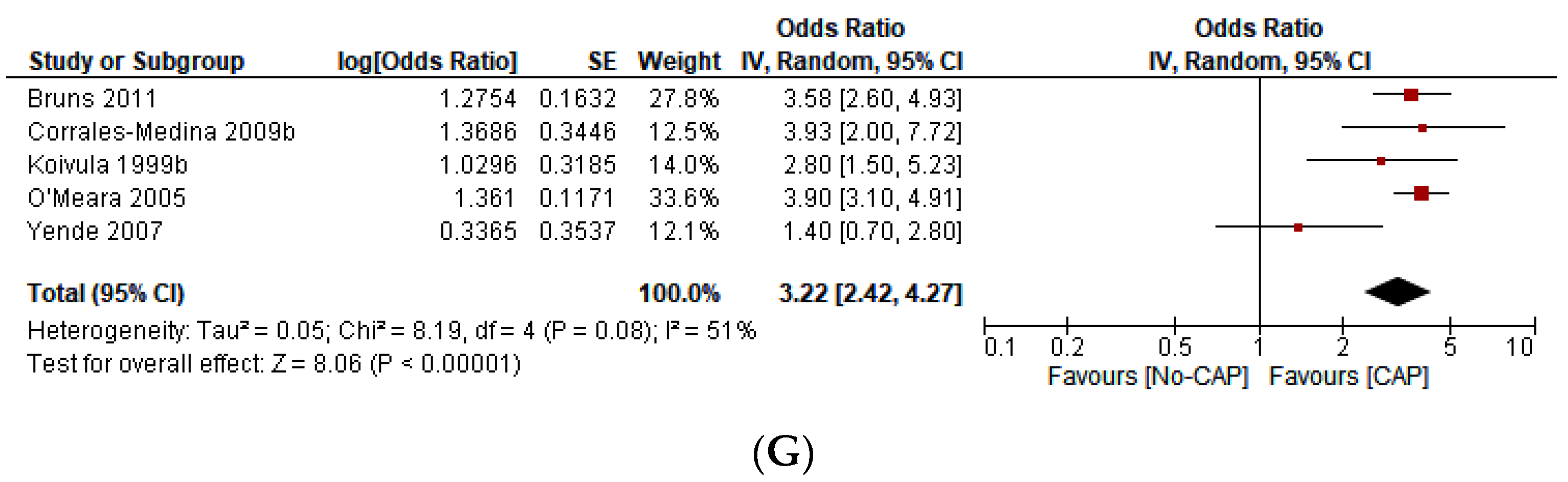
| Koivula [6], Finland, 1999b | N = 4167. PCAP 53. Follow-up 9.2 y. Prospective observational (cohort) study. No CAP 4045. Both sexes. Age ≥60 y. Deaths 1979. Mean follow-up 9.2 y. | PCAP | Total mortality, cardiovascular mortality | Age, sex, and multiple comorbidities. | RR 2.8 (1.5–5.3) for pneumonia-related mortality. ARR 1.6 (1.1–2.2) for total mortality. ARR 1.6 (1.0–2.4) for cardiovascular mortality. |
| Bruns [7], Netherlands, 2011 | N = 712. Patients discharged from hospital after an episode of CAP 356. Death in CAP 187, death in no CAP 85. Follow-up: 7 y. Both sexes. Age ≥18 y. Mean age of the CAP patients. Follow-up 7 y. 66.0 ± 16.1 years. Prospective cohort study. | CAP | Mortality rate | Age, sex, PSI | AOR 3.58 (2.60–4.94) for long-term mortality rate. |
| Yende [8], USA, 2007 | N = 3075, 106 subjects hospitalized for CAP. Follow-up: 5.2 y. Prospective cohort study. Deaths: 361. Both sexes. Age 70–79 y. Mean age 73.6 ± 2.9 y. | CAP | Mortality | Age, sex, race, site, smoking, DM, CHD, eGFR, FEV1, albuminemia, cognitive function, functional status, TNF, IL-6. | AOR 1.4 (0.7–3.0) for mortality at 0–30 days. AOR 3.5 (1.5–8.1) for mortality at 31–365 days. AOR 5.6 (2.8–11.2) for mortality at >365 days. |
| Chung [9], Taiwan, 2015. | N = 12,152 newly diagnosed MP. No MP 48,600 individuals. Nationwide longitudinal cohort study. Follow-up up to >12 months. Both sexes. ACS and MP 350. ACS and no MP 106. | MP | New ACS (unstable angina and MI). | Sex, age, comorbidities and follow-up time. | AHR 1.37(1.10–1.70) for ACS. AHR 1.49 (1.06–2.08) for ACS in females. AHR 1.29 (0.97–1.71) for ACS in males. AHR 1.48 (1.01–2.16) for ACS in ≤64 y. AHR 1.34 (1.02–1.74) for ACS in >65 y. |
| Chen [10], Taiwan, 2012. | Hospitalized patients. PCAP 745, no PCAP 1490. Cohort study. PCAP and stroke 80, no PCAP and stroke 73. Follow-up: 2 y. Both sexes. Age > 18 y. In both cohorts >60% were ≥65 y. | PCAP | Stroke | Patient characteristics, comorbidities, geographic region, urbanization, level of residence, and socioeconomic status. | AHR 3.65 (2.25–5.90) for stroke in the first year. AHR 0.91 (0.53–1.59) for stroke in the second year. AHR 5.00 (1.78–14.07) for stroke in the first year in those with comorbidities. AHR 3.23(1.86–5.62) for stroke in the first year in those without comorbidities. |
| Corrales-Medina [11], USA, 2015a | Community-based prospective cohort. CHS cohort. Age ≥ 65 years, CAP 591, no CAP 1182. Both sexes. CVD * events 173. Follow-up up to 10 y. | CAP | Incident CVD (MI, stroke, and fatal CHD) | Age, sex, race, HT, DM, total cholesterol, HDL, LDL, smoking, alcohol abuse, AF, CKD, CRP, CVD, FEV1, daily living activities, modified MMS score. | AHR 4.07 (2.86–5.27) for CVD at 0–30 d. AHR 2.94 (2.18–3.70) for CVD at 31–90 d. AHR 2.10 (1.59–2.60) for CVD at 91 d-1 y. AHR 1.86 (1.18–2.55) for CVD at 9–10 y. |
| Corrales-Medina [11], USA, 2015b | Community-based prospective cohort. ARIC cohort. Age 45–64 years, CAP 680, no CAP 1360. Both sexes. CVD * events 45. Follow-up up to 10 y. | CAP | Incident CVD (MI, stroke, and fatal CHD) | Age, sex, race, HT, DM, total cholesterol, HDL, LDL, smoking, alcohol abuse, AF, CKD, Q waves in ECG, PAD, FEV1 | AHR 2.38 (1.12–3.63) for CVD at 0–30 d. AHR 2.40 (1.23–3.47) for CVD at 31–90 d. AHR 2.19 (1.20–3.19) for CVD at 91 d-1 y. AHR 1.88 (1.10–2.66) for CVD at 9–10 y. |
| Corrales-Medina [12], USA, 2009a | Case-control study. CAP patients (144 S. pneumoniae, 62 H. influenzae) 206. Controls 395. ACS: 22 cases among CAP patients and 6 among 395 controls. Both sexes. Follow-up 475 d. | PCAP or HCAP | ACS | CHD equivalent (CHD, or cerebrovascular disease, or PVD, HF, ≥2 coronary risk factors (DM, HT, dyslipidemia, smoking, family history of CHD). | AOR 8.52 (3.35–22.23) for ACS. |
| Corrales-Medina [12], USA, 2009b | Case-control study. CAP patients (144 S. pneumoniae, 62 H. influenzae) 206. Controls 395. Thirty-day mortality: 26 cases among CAP patients and 14 among 395 controls. Both sexes. Follow-up 475 d. | PCAP or HCAP | Thirty-day mortality | CHD equivalent (CHD, or cerebrovascular disease, or PVD, HF, ≥2 coronary risk factors (DM, HT, dyslipidemia, smoking, family history of CHD). | AOR 3.93 (2.00–22.7.71) for 30-day mortality. |
| O’Meara [13], USA, 2005 | CHS. N = 5888 men and women aged ≥65. CAP 582. No CAP: 5306. Median follow-up 10.7 years. Prospective cohort. | CAP | Total mortality | * Age, sex, and race. ** Age, sex, and race, Baseline history of CVD, DM, smoking, and measures of lung, physical, and cognitive function. | * ARR 4.9 (4.1–6.0) for total mortality during the first year after hospitalization. * ARR 2.6 (2.2–3.1) for total mortality after the first year after hospitalization. ** ARR 3.9 (3.1–4.8) for total mortality during the first year after hospitalization. ** ARR 2.0 (1.6–2.4) for total mortality after the first year after hospitalization. |
| Author | Study Design | Tool | Selection | Comparability | Outcome | Total | Conclusion |
|---|---|---|---|---|---|---|---|
| Meier [1], UK, 1986 | CC | NOS | *** | ** | ** | 7 | Low risk |
| Smeeth [2], UK; 2004 | CC | NOS | *** | ** | ** | 7 | Low risk |
| Clayton [3], UK, 2008 | CC | NOS | *** | ** | ** | 7 | Low risk |
| Nuñez-Delgado [4], Peru, 2022 | CS | NOS | *** | ** | *** | 8 | Low risk |
| Wang [5], Taiwan, 2013 | CC | NOS | *** | ** | ** | 7 | Low risk |
| Koivula [6], Finland, 1999 | CS | NOS | *** | ** | *** | 8 | Low risk |
| Bruns [7], Netherlands, 2011 | CS | NOS | *** | ** | ** | 7 | Low risk |
| Yende [8], USA, 2007 | CC | NOS | *** | ** | ** | 7 | Low risk |
| Chung [9], Taiwan, 2015. | CS | NOS | *** | ** | *** | 8 | Low risk |
| Chen [10], Taiwan, 2012. | CS | NOS | *** | ** | ** | 7 | Low risk |
| Corrales-Medina [11], USA, 2015 | CS | NOS | **** | ** | *** | 9 | Low risk |
| Corrales-Medina [12], USA, 2009 | CC | NOS | *** | ** | *** | 8 | Low risk |
| O’Meara [13], 2005, USA | CS | NOS | *** | ** | ** | 7 | Low risk |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Meregildo-Rodriguez, E.D.; Asmat-Rubio, M.G.; Rojas-Benites, M.J.; Vásquez-Tirado, G.A. Acute Coronary Syndrome, Stroke, and Mortality after Community-Acquired Pneumonia: Systematic Review and Meta-Analysis. J. Clin. Med. 2023, 12, 2577. https://doi.org/10.3390/jcm12072577
Meregildo-Rodriguez ED, Asmat-Rubio MG, Rojas-Benites MJ, Vásquez-Tirado GA. Acute Coronary Syndrome, Stroke, and Mortality after Community-Acquired Pneumonia: Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2023; 12(7):2577. https://doi.org/10.3390/jcm12072577
Chicago/Turabian StyleMeregildo-Rodriguez, Edinson Dante, Martha Genara Asmat-Rubio, Mayra Janett Rojas-Benites, and Gustavo Adolfo Vásquez-Tirado. 2023. "Acute Coronary Syndrome, Stroke, and Mortality after Community-Acquired Pneumonia: Systematic Review and Meta-Analysis" Journal of Clinical Medicine 12, no. 7: 2577. https://doi.org/10.3390/jcm12072577