
Short Interpregnancy Interval Following a Multifetal Pregnancy: Maternal and Neonatal Outcomes


Abstract
:1. Introduction
2. Material and Methods
Statistical Analysis
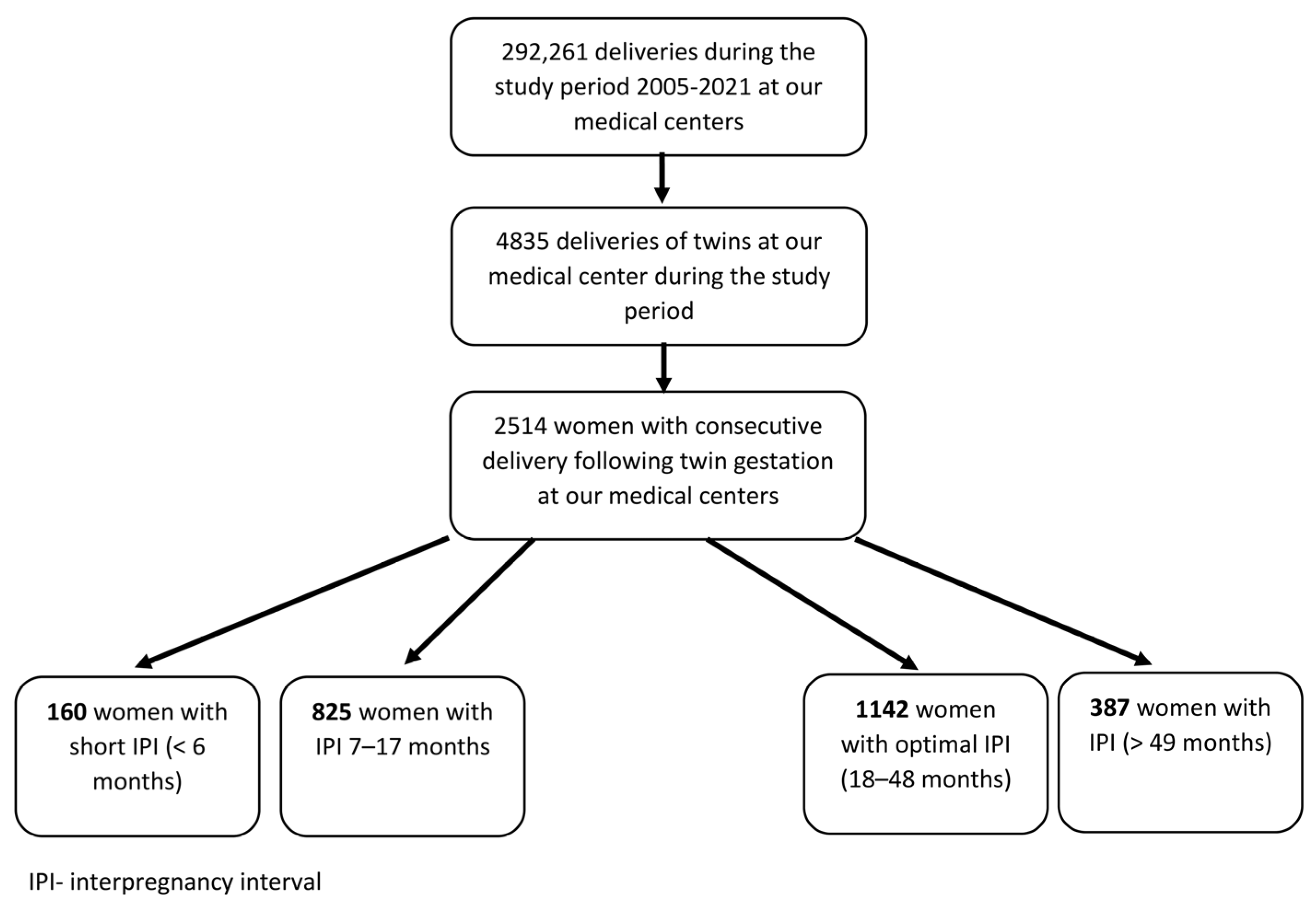
3. Results
4. Discussion
4.1. Clinical Implications
4.2. Research Implications
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fell, D.B.; Joseph, K.S. Temporal trends in the frequency of twins and higher-order multiple births in Canada and the United States. BMC Pregnancy Childbirth 2012, 12, 103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grisaru-Granovsky, S.; Gordon, E.S.; Haklai, Z.; Samueloff, A.; Schimmel, M.M. Effect of interpregnancy interval on adverse perinatal outcomes—A national study. Contraception 2009, 80, 512–518. [Google Scholar] [CrossRef] [PubMed]
- Hutcheon, J.A.; Nelson, H.D.; Stidd, R.; Moskosky, S.; Ahrens, K.A. Short interpregnancy intervals and adverse maternal outcomes in high-resource settings: An updated systematic review. Paediatr. Perinat. Epidemiol. 2019, 33, O48–O59. [Google Scholar] [CrossRef] [Green Version]
- Zhu, B.-P.; Rolfs, R.T.; Nangle, B.E.; Horan, J.M. Effect of the interval between pregnancies on perinatal outcomes. N. Engl. J. Med. 1999, 340, 589–594. [Google Scholar] [CrossRef] [PubMed]
- Tessema, G.A.; Marinovich, M.L.; Håberg, S.E.; Gissler, M.; Mayo, J.A.; Nassar, N.; Ball, S.; Betrán, A.P.; Gebremedhin, A.T.; de Klerk, N.; et al. Interpregnancy intervals and adverse birth outcomes in high-income countries: An international cohort study. PLoS ONE 2021, 16, e0255000. [Google Scholar] [CrossRef]
- Rawlings, J.S.; Rawlings, V.B.; Read, J.A. Prevalence of low birth weight and preterm delivery in relation to the interval between pregnancies among white and black women. N. Engl. J. Med. 1995, 332, 69–74. [Google Scholar] [CrossRef]
- Nisha, M.K.; Alam, A.; Islam, M.T.; Huda, T.; Raynes-Greenow, C. Risk of adverse pregnancy outcomes associated with short and long birth intervals in Bangladesh: Evidence from six Bangladesh Demographic and Health Surveys, 1996–2014. BMJ Open 2019, 9, e024392. [Google Scholar] [CrossRef]
- Goodnight, W.; Newman, R.; Society of Maternal–Fetal Medicine. Optimal nutrition for improved twin pregnancy outcome. Obstet. Gynecol. 2009, 114, 1121–1134. [Google Scholar] [CrossRef] [Green Version]
- Luke, B. Improving multiple pregnancy outcomes with nutritional interventions. Clin. Obstet. Gynecol. 2004, 47, 146–162. [Google Scholar] [CrossRef]
- Conde-Agudelo, A.; Rosas-Bermúdez, A.; Kafury-Goeta, A.C. Effects of birth spacing on maternal health: A systematic review. Am. J. Obstet. Gynecol. 2007, 196, 297–308. [Google Scholar] [CrossRef]
- Conde-Agudelo, A.; Rosas-Bermúdez, A.; Kafury-Goeta, A.C. Birth spacing and risk of adverse perinatal outcomes: A meta-analysis. JAMA 2006, 295, 1809–1823. [Google Scholar] [CrossRef] [PubMed]
- Gupta, P.M.; Freedman, A.A.; Kramer, M.R.; Goldenberg, R.L.; Willinger, M.; Stoll, B.J.; Silver, R.M.; Dudley, D.J.; Parker, C.B.; Hogue, C.J. Interpregnancy interval and risk of stillbirth: A population-based case control study. Ann. Epidemiol. 2019, 35, 35–41. [Google Scholar] [CrossRef] [PubMed]
- Hanley, G.E.; Hutcheon, J.A.; Kinniburgh, B.A.; Lee, L. Interpregnancy Interval and Adverse Pregnancy Outcomes: An Analysis of Successive Pregnancies. Obstet. Gynecol. 2017, 129, 408–415. [Google Scholar] [CrossRef] [PubMed]
- Louis, J.M.; Bryant, A.; Ramos, D.; Stuebe, A.; Blackwell, S.C.; American College of Obstetricians and Gynecologists. Interpregnancy care. Am. J. Obstet. Gynecol. 2019, 220, B2–B18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ball, S.J.; Pereira, G.; Jacoby, P.; de Klerk, N.; Stanley, F.J. Re-evaluation of link between interpregnancy interval and adverse birth outcomes: Retrospective cohort study matching two intervals per mother. BMJ 2014, 349, g4333. [Google Scholar] [CrossRef] [Green Version]
- Shachar, B.Z.; Mayo, J.A.; Lyell, D.J.; Baer, R.J.; Jeliffe-Pawlowski, L.L.; Stevenson, D.K.; Shaw, G.M. Interpregnancy interval after live birth or pregnancy termination and estimated risk of preterm birth: A retrospective cohort study. BJOG 2016, 123, 2009–2017. [Google Scholar] [CrossRef]
- Marinovich, M.L.; Regan, A.K.; Gissler, M.; Magnus, M.C.; Håberg, S.E.; Mayo, J.A.; Shaw, G.; Bell, J.; Nassar, N.; Ball, S.; et al. Associations between interpregnancy interval and preterm birth by previous preterm birth status in four high-income countries: A cohort study. BJOG 2021, 128, 1134–1143. [Google Scholar] [CrossRef]
- Congdon, J.L.; Baer, R.J.; Arcara, J.; Feuer, S.K.; Gómez, A.M.; Karasek, D.; Oltman, S.P.; Pantell, M.S.; Ryckman, K.; Jelliffe-Pawlowski, L. Interpregnancy Interval and Birth Outcomes: A Propensity Matching Study in the California Population. Matern. Child Health J. 2022, 26, 1115–1125. [Google Scholar] [CrossRef]
- Conde-Agudelo, A.; Rosas-Bermudez, A.; Castaño, F.; Norton, M.H. Effects of birth spacing on maternal, perinatal, infant, and child health: A systematic review of causal mechanisms. Stud. Fam. Plann. 2012, 43, 93–114. [Google Scholar] [CrossRef]
- Weiss, A.; Sela, H.Y.; Rotem, R.; Grisaru-Granovsky, S.; Rottenstreich, M. Recurrent short interpregnancy interval: Maternal and neonatal outcomes. Eur. J. Obstet. Gynecol. Reprod. Biol. 2021, 264, 299–305. [Google Scholar] [CrossRef]
- Jena, B.H.; Biks, G.A.; Gete, Y.K.; Gelaye, K.A. Incidence of preterm premature rupture of membranes and its association with inter-pregnancy interval: A prospective cohort study. Sci. Rep. 2022, 12, 5714. [Google Scholar] [CrossRef]
- Beyerlein, A.; Schiessl, B.; Lack, N.; von Kries, R. Optimal Gestational weight gain ranges for the avoidance of adverse birth weight outcomes: A novel approach. Am. J. Clin. Nutr. 2009, 90, 1552–1558. [Google Scholar] [CrossRef] [Green Version]
- Luke, B.; Hediger, M.L.; Nugent, C.; Newman, R.B.; Mauldin, J.G.; Witter, F.R.; O’Sullivan, M.J. Body mass index—Specific weight gains associated with optimal birth weights in twin pregnancies. J. Reprod. Med. 2003, 48, 217–224. [Google Scholar]
- Hinkle, S.N.; Hediger, M.L.; Kim, S.; Albert, P.S.; Grobman, W.; Newman, R.B.; Wing, D.A.; Grewal, J.; Zhang, C.; Louis, G.M.B.; et al. Maternal weight gain and associations with longitudinal fetal growth in dichorionic twin pregnancies: A prospective cohort study. Am. J. Clin. Nutr. 2017, 106, 1449–1455. [Google Scholar] [CrossRef] [Green Version]
- Luke, B.; Min, S.J.; Gillespie, B.; Avni, M.; Witter, F.R.; Newman, R.B.; Mauldin, J.G.; Salman, F.A.; O’Sullivan, M.J. The importance of early weight gain in the intrauterine growth and birth weight of twins. Am. J. Obstet. Gynecol. 1998, 179, 1155–1161. [Google Scholar] [CrossRef]
- Weiss, A.; Lang Ben Nun, E.; Sela, H.Y.; Rotem, R.; Grisaru-Granovsky, S.; Rottenstreich, M. Twin pregnancy following a short interpregnancy interval: Maternal and neonatal outcomes. Eur. J. Obstet. Gynecol. Reprod. Biol. 2022, 276, 185–190. [Google Scholar] [CrossRef]
- Smith, G.C.S.; Pell, J.P.; Dobbie, R. Interpregnancy interval and risk of preterm birth and neonatal death: Retrospective cohort study. BMJ 2003, 327, 313. [Google Scholar] [CrossRef] [Green Version]
- Blumenfeld, Y.J.; Baer, R.J.; Druzin, M.L.; El-Sayed, Y.Y.; Lyell, D.J.; Faucett, A.M.; Shaw, G.M.; Currier, R.J.; Jelliffe-Pawlowski, L.L. Association between maternal characteristics, abnormal serum aneuploidy analytes, and placental abruption. Am. J. Obstet. Gynecol. 2014, 211, 144.e1–144.e9. [Google Scholar] [CrossRef]
- Dewey, K.G.; Cohen, R.J. Does birth spacing affect maternal or child nutritional status? A systematic literature review. Matern. Child. Nutr. 2007, 3, 151–173. [Google Scholar] [CrossRef]


{kind=link}
| Optimal IPI (18–48 Months) n = 1142 | Short IPI (0–6 Months) n = 160 | p Value | |
|---|---|---|---|
| Maternal age, years | 32.1 ± 4.6 | 30 ± 5.3 | <0.01 |
| Previous miscarriages | 301 (27.3%) | 43 (29.9%) | 0.52 |
| Previous miscarriages ≥ 3 | 34 (3.1%) | 8 (5.6%) | 0.12 |
| Gravidity | 4.4 ± 2.5 | 4.4 ± 2.9 | 0.99 |
| Parity | 4 ± 2.2 | 3.9 ± 2.4 | 0.57 |
| Interpregnancy pregnancy interval, months | 29.9 ± 8.4 | 4.1 ± 1.2 | <0.01 |
| Smoking | 21 (2%) | 4 (3%) | 0.45 |
| Previous cesarean delivery in twin pregnancy | 576 (51.3%) | 52 (33.2%) | <0.01 |
| Previous cesarean delivery, any | 588 (51.5%) | 54 (33.8%) | <0.01 |
| Fertility Treatments | 118 (10.7%) | 2 (1.4%) | <0.01 |
| Obesity (BMI ≥ 30) | 52 (17.7%) | 5 (17.2%) | 0.95 |
| Induction of labor | 94 (8.9%) | 19 (12.8%) | 0.13 |
| Trial of labor after cesarean | 390 (35.4%) | 33 (22.9%) | <0.01 |
| Meconium-stained amniotic fluid | 144 (13.1%) | 20 (13.9%) | 0.78 |
| Epidural analgesia | 543 (48%) | 84 (54.5%) | 0.13 |
| Optimal IPI (18–48 Months) n = 1142 | Short IPI (0–6 Months) n = 160 | p Value | |
|---|---|---|---|
| Hypertensive disorders of pregnancy | 14 (1.3%) | 2 (1.4%) | 0.91 |
| Diabetes (pre-gestational + gestational) | 62 (5.7%) | 4 (3.1%) | 0.20 |
| Anemia (Hb < 11 gr%) on admission to labor | 91 (11.4%) | 20 (20%) | 0.01 |
| Placental abruption | 23 (2.1%) | 7 (5.3%) | 0.03 |
| Gestational age at delivery | 39.2 ± 1.6 | 38.9 ± 1.9 | 0.05 |
| Gestational age at delivery < 37 week | 47 (4.3%) | 14 (9.7%) | <0.01 |
| Gestational age at delivery < 34 week | 8 (0.7%) | 3 (1.9%) | 0.13 |
| Gestational age at delivery < 32 week | 3 (0.3%) | 1 (0.6%) | 0.44 |
| Gestational age at delivery < 28 week | 1 (0.1%) | 0 (0%) | 0.71 |
| Spontaneous preterm birth (<37 weeks) | 29 (2.6%) | 7 (4.9%) | 0.13 |
| Indicated preterm birth (<7 weeks) | 18 (1.6%) | 7 (4.9%) | 0.01 |
| Unplanned cesarean | 65 (5.9%) | 8 (5.6%) | 0.87 |
| Elective cesarean | 189 (17.2%) | 21 (14.6%) | 0.44 |
| Postpartum hemorrhage | 81 (7.4%) | 5 (3.8%) | 0.12 |
| Blood products transfusion | 15 (1.9%) | 1 (1%) | 0.53 |
| Maternal ICU admissions | 1 (0.1%) | 0 (0%) | 0.72 |
| Placenta Accreta/Percreta | 1 (0.1%) | 0 (0%) | 0.72 |
| Prolonged hospital stays * | 16 (2%) | 3 (3%) | 0.52 |
| Composite adverse maternal outcome ** | 131 (11.5%) | 22 (13.8%) | 0.40 |
| Optimal IPI (18–48 Months) n = 1142 | Short IPI (0–6 Months) n = 160 | p Value | |
|---|---|---|---|
| Birthweight | 3361.5 ± 490.5 | 3283.4 ± 509.7 | 0.06 |
| Birthweight ≥ 4000 g | 83 (7.5%) | 6 (4.2%) | 0.14 |
| LGA | 164 (14.9%) | 20 (13.9%) | 0.75 |
| SGA | 94 (8.5%) | 10 (6.9%) | 0.52 |
| 5-Minute Apgar score < 7 | 13 (1.1%) | 1 (0.6%) | 0.56 |
| Perinatal death | 34 (3.1%) | 9 (6.3%) | 0.05 |
| NICU admission | 1 (0.1%) | 0 (0%) | 0.72 |
| Composite adverse neonatal outcome * | 252 (22.1%) | 33 (20.6%) | 0.68 |
| p-Value | aOR | 95% CI | ||
|---|---|---|---|---|
| Previous preterm delivery(<37 weeks) | <0.01 | 3.02 | 1.55 | 5.88 |
| Anemia (Hb < 11 gr%) on admission to labor | 0.01 | 2.54 | 1.26 | 5.13 |
| Short IPI (<6 months) following multifetal pregnancy | 0.03 | 2.39 | 1.12 | 5.11 |
| Previous cesarean delivery, any | 0.17 | 3.12 | 0.62 | 15.65 |
| Hypertensive disorders of pregnancy | 0.21 | 2.21 | 0.63 | 7.73 |
| Previous miscarriages ≥ 3 | 0.36 | 1.35 | 0.71 | 2.59 |
| p Value | aOR | 95%CI | ||
|---|---|---|---|---|
| Composite Adverse Maternal Outcome * | ||||
| Previous cesarean delivery | <0.01 | 1.72 | 1.21 | 2.46 |
| Short IPI | 0.14 | 1.47 | 0.89 | 2.42 |
| Gravidity | 0.45 | 0.92 | 0.74 | 1.14 |
| Parity | 0.69 | 0.95 | 0.74 | 1.22 |
| Fertility Treatments | 0.94 | 1.02 | 0.58 | 1.79 |
| Composite Adverse Neonatal Outcome ** | ||||
| Diabetes (pre-gestational + gestational) | <0.01 | 8.64 | 4.95 | 15.08 |
| Previous cesarean delivery | <0.01 | 1.99 | 1.41 | 2.80 |
| Anemia (Hb < 11 gr%) on admission to labor | 0.01 | 1.85 | 1.17 | 2.92 |
| Maternal age, years | 0.43 | 0.99 | 0.95 | 1.02 |
| Short IPI | 0.52 | 1.19 | 0.70 | 2.04 |
| Hypertensive disorders of pregnancy | 0.88 | 1.10 | 0.32 | 3.74 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Weiss, A.; Sela, H.Y.; Grisaru-Granovsky, S.; Rottenstreich, M. Short Interpregnancy Interval Following a Multifetal Pregnancy: Maternal and Neonatal Outcomes. J. Clin. Med. 2023, 12, 2576. https://doi.org/10.3390/jcm12072576
Weiss A, Sela HY, Grisaru-Granovsky S, Rottenstreich M. Short Interpregnancy Interval Following a Multifetal Pregnancy: Maternal and Neonatal Outcomes. Journal of Clinical Medicine. 2023; 12(7):2576. https://doi.org/10.3390/jcm12072576
Chicago/Turabian StyleWeiss, Ari, Hen Y. Sela, Sorina Grisaru-Granovsky, and Misgav Rottenstreich. 2023. "Short Interpregnancy Interval Following a Multifetal Pregnancy: Maternal and Neonatal Outcomes" Journal of Clinical Medicine 12, no. 7: 2576. https://doi.org/10.3390/jcm12072576