
Management of Non-Culprit Lesions in STEMI Patients with Multivessel Disease
 , , ,
, , ,
Abstract
:1. Introduction
2. Angiography-Guided Complete Revascularization
3. Function-Guided Complete Revascularization
3.1. FFR-Guided Complete Revascularization
3.2. Angiography-Guided vs. FFR-Guided Revascularization
4. Imaging-Guided Complete Revascularization
Imaging Guidance for Percutaneous Coronary Intervention
5. Complete Revascularization in Cardiogenic Shock
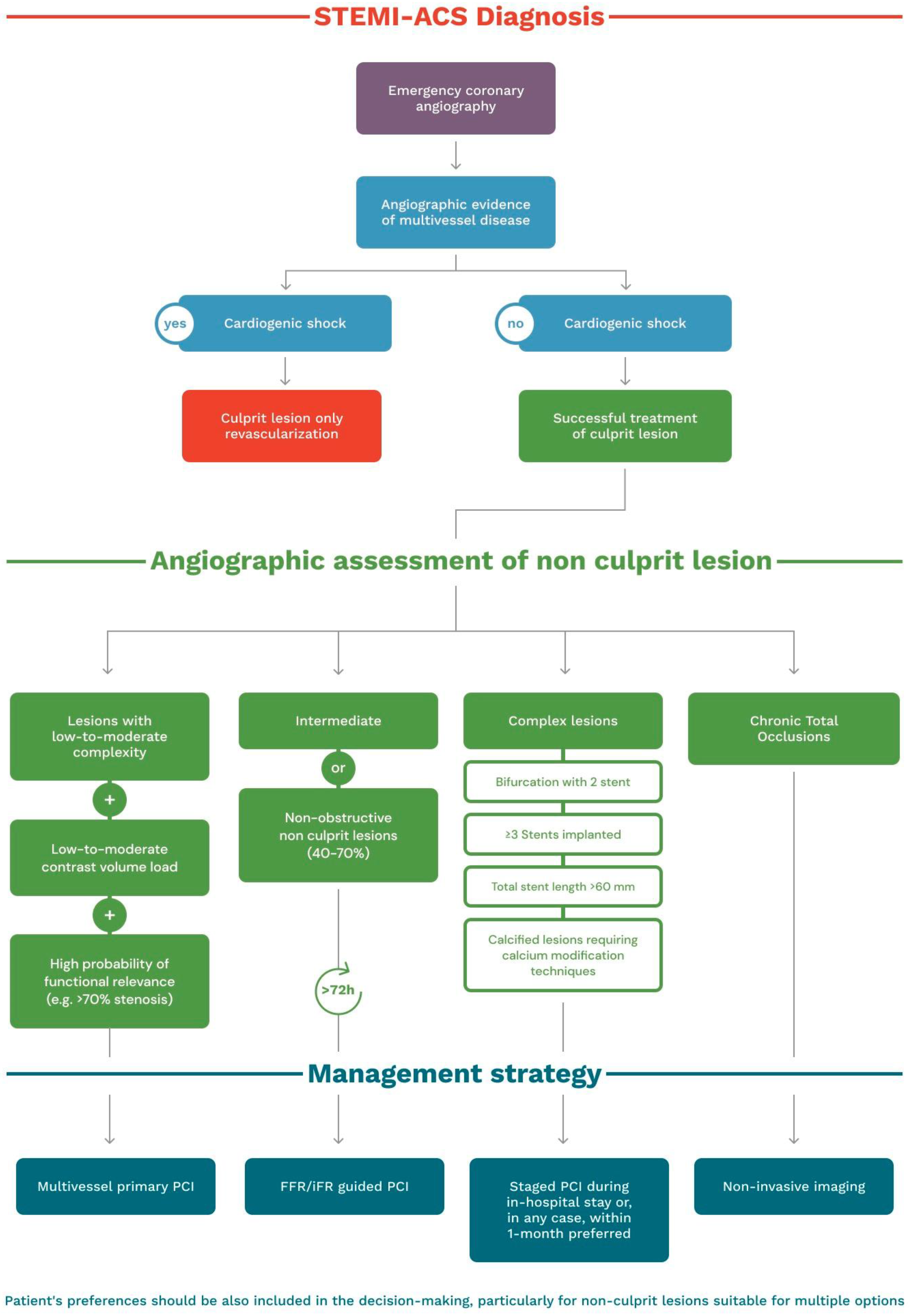
6. Treatment Algorithm
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ACC | American College of Cardiology |
| ACS | acute coronary syndrome |
| AHA | American Heart Association |
| AKI | acute kidney injury |
| CABG | coronary bypass artery grafting |
| CI | confidence interval |
| CR | complete revascularization |
| CS | cardiogenic shock |
| CV | cardiovascular |
| ESC | European Society of Cardiology |
| FFR | fractional flow reserve |
| FU | follow-up |
| HR | hazard ratio |
| IDR | ischemia-driven revascularization |
| IRA | non-infarct related artery |
| IVUS | intravascular ultrasound |
| MACE | major adverse cardiac events |
| MI | myocardial infarction |
| MLA | minimal lumen Area |
| NIRS | near-infrared spectroscopy |
| OCT | optical coherence tomography |
| PCI | percutaneous coronary intervention |
| QCA | quantitative coronary angiography |
| RR | repeat revascularizations |
| SCAI | Society for Cardiovascular Angiography & Interventions |
| SR | stent restenosis |
| STEMI | ST-segment elevation myocardial infarction |
| TCFA | thin cap fibroatheroma |
| VH | virtual histology |
References
- O’Gara, P.T.; Kushner, F.G.; Ascheim, D.D.; Casey, D.E., Jr.; Chung, M.K.; de Lemos, J.A.; Ettinger, S.M.; Fang, J.C.; Fesmire, F.M.; Franklin, B.A.; et al. 2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction: Executive Summary A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation 2013, 127, 529–555. [Google Scholar] [CrossRef] [Green Version]
- Levine, G.N.; Bates, E.R.; Blankenship, J.C.; Bailey, S.R.; Bittl, J.A.; Cercek, B.; Chambers, C.E.; Ellis, S.G.; Guyton, R.A.; Hollenberg, S.M.; et al. 2015 ACC/AHA/SCAI Focused Update on Primary Percutaneous Coronary Intervention for Patients with ST-Elevation Myocardial Infarction An Update of the 2011 ACCF/AHA/SCAI Guideline for Percutaneous Coronary Intervention and the 2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction a Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Society for Cardiovascular Angiography and Interventions. Circulation 2016, 133, 1135–1147. [Google Scholar] [PubMed] [Green Version]
- Ibanez, B.; James, S.; Agewall, S.; Antunes, M.J.; Bucciarelli-Ducci, C.; Bueno, H.; Caforio, A.L.P.; Crea, F.; Goudevenos, J.A.; Halvorsen, S.; et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur. Heart J. 2018, 39, 119–177. [Google Scholar] [PubMed] [Green Version]
- Keeley, E.C.; Boura, J.A.; Grines, C.L. Comparison of Primary and Facilitated Percutaneous Coronary Interventions for ST-Elevation Myocardial Infarction: Quantitative Review of Randomised Trials. Lancet 2006, 367, 579–588. [Google Scholar] [CrossRef] [PubMed]
- Park, D.W.; Clare, R.M.; Schulte, P.J.; Pieper, K.S.; Shaw, L.K.; Califf, R.M.; Ohman, E.M.; van de Werf, F.; Hirji, S.; Harrington, R.A.; et al. Extent, Location, and Clinical Significance of Non-Infarct-Related Coronary Artery Disease among Patients with ST-Elevation Myocardial Infarction. JAMA 2014, 312, 2019–2027. [Google Scholar] [CrossRef] [PubMed]
- Tripathi, B.; Yeh, R.W.; Bavishi, C.P.; Sardar, P.; Atti, V.; Mukherjee, D.; Bashir, R.; Abbott, J.D.; Giri, J.; Chatterjee, S. Etiologies, Trends, and Predictors of Readmission in ST-Elevation Myocardial Infarction Patients Undergoing Multivessel Percutaneous Coronary Intervention. Catheter. Cardiovasc. Interv. 2019, 94, 905–914. [Google Scholar] [CrossRef]
- Sorajja, P.; Gersh, B.J.; Cox, D.A.; McLaughlin, M.G.; Zimetbaum, P.; Costantini, C.; Stuckey, T.; Tcheng, J.E.; Mehran, R.; Lansky, A.J.; et al. Impact of Multivessel Disease on Reperfusion Success and Clinical Outcomes in Patients Undergoing Primary Percutaneous Coronary Intervention for Acute Myocardial Infarction. Eur. Heart J. 2007, 28, 1709–1716. [Google Scholar] [CrossRef] [Green Version]
- Parodi, G.; Memisha, G.; Valenti, R.; Trapani, M.; Migliorini, A.; Santoro, G.M.; Antoniucci, D. Five Year Outcome after Primary Coronary Intervention for Acute ST Elevation Myocardial Infarction: Results from a Single Centre Experience. Heart 2005, 91, 1541–1544. [Google Scholar] [CrossRef] [Green Version]
- Toutouzas, K.; Drakopoulou, M.; Mitropoulos, J.; Tsiamis, E.; Vaina, S.; Vavuranakis, M.; Markou, V.; Bosinakou, E.; Stefanadis, C. Elevated Plaque Temperature in Non-Culprit de Novo Atheromatous Lesions of Patients with Acute Coronary Syndromes. J. Am. Coll. Cardiol. 2006, 47, 301–306. [Google Scholar] [CrossRef] [Green Version]
- Rioufol, G.; Finet, G.; Ginon, I.; André-Fouët, X.; Rossi, R.; Vialle, E.; Desjoyaux, E.; Convert, G.; Huret, J.F.; Tabib, A. Multiple Atherosclerotic Plaque Rupture in Acute Coronary Syndrome: A Three-Vessel Intravascular Ultrasound Study. Circulation 2002, 106, 804–808. [Google Scholar] [CrossRef] [Green Version]
- Pilgrim, T.; Piccolo, R.; Heg, D.; Roffi, M.; Tüller, D.; Vuilliomenet, A.; Muller, O.; Cook, S.; Weilenmann, D.; Kaiser, C.; et al. Biodegradable polymer sirolimus-eluting stents versus durable polymer everolimus-eluting stents for primary percutaneous coronary revascularisation of acute myocardial infarction. EuroIntervention 2016, 12, e1343–e1354. [Google Scholar] [CrossRef] [Green Version]
- Piccolo, R.; Pilgrim, T.; Heg, D.; Franzone, A.; Rat-Wirtzler, J.; Räber, L.; Silber, S.; Serruys, P.W.; Jüni, P.; Windecker, S. Comparative Effectiveness and Safety of New-Generation Versus Early-Generation Drug-Eluting Stents According to Complexity of Coronary Artery Disease: A Patient-Level Pooled Analysis of 6,081 Patients. JACC Cardiovasc. Interv. 2015, 8, 1657–1666. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Piscione, F.; Piccolo, R.; Cassese, S.; Galasso, G.; De Rosa, R.; D’Andrea, C.; Chiariello, M. Effect of drug-eluting stents in patients with acute ST-segment elevation myocardial infarction undergoing percutaneous coronary intervention: A meta-analysis of randomised trials and an adjusted indirect comparison. EuroIntervention 2010, 5, 853–860. [Google Scholar] [CrossRef] [PubMed]
- Piccolo, R.; Galasso, G.; Capuano, E.; De Luca, S.; Esposito, G.; Trimarco, B.; Piscione, F. Trans radial versus transfemoral approach in patients undergoing percutaneous coronary intervention for acute coronary syndrome. A meta-analysis and trial sequential analysis of randomized controlled trials. PLoS ONE 2014, 9, e96127. [Google Scholar] [CrossRef] [Green Version]
- Lawton, J.S.; Tamis-Holland, J.E.; Bangalore, S.; Bates, E.R.; Beckie, T.M.; Bischoff, J.M.; Bittl, J.A.; Cohen, M.G.; DiMaio, J.M.; Don, C.W.; et al. 2021 ACC/AHA/SCAI Guideline for Coronary Artery Revascularization: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2022, 79, e21–e129. [Google Scholar] [CrossRef]
- Hanratty, C.G.; Koyama, Y.; Rasmussen, H.H.; Nelson, G.I.C.; Hansen, P.S.; Ward, M.R. Exaggeration of Nonculprit Stenosis Severity During Acute Myocardial Infarction: Implications for Immediate Multivessel Revascularization. J. Am. Coll. Cardiol. 2002, 40, 911–916. [Google Scholar] [CrossRef] [Green Version]
- van der Hoeven, N.W.; Janssens, G.N.; de Waard, G.A.; Everaars, H.; Broyd, C.J.; Beijnink, C.W.H.; van de Ven, P.M.; Nijveldt, R.; Cook, C.M.; Petraco, R.; et al. Temporal Changes in Coronary Hyperemic and Resting Hemodynamic Indices in Non culprit Vessels of Patients with ST-Segment Elevation Myocardial Infarction. JAMA Cardiol. 2019, 4, 736–744. [Google Scholar] [CrossRef]
- de Waard, G.A.; Hollander, M.R.; Teunissen, P.F.A.; Jansen, M.F.; Eerenberg, E.S.; Beek, A.M.; Marques, K.M.; van de Ven, P.M.; Garrelds, I.M.; Danser, A.H.J.; et al. Changes in Coronary Blood Flow After Acute Myocardial Infarction Insights From a Patient Study and an Experimental Porcine Model. JACC Cardiovasc. Interv. 2016, 9, 602–613. [Google Scholar] [CrossRef] [PubMed]
- di Mario, C.; Sansa, M.; Airoldi, F.; Sheiban, I.; Manari, A.; Petronio, A.; Piccaluga, E.; de Servi, S.; Ramondo, A.; Colusso, S.; et al. Single vs Multivessel Treatment during Primary Angioplasty: Results of the Multicentre Randomised HEpacoatTM for CuLPrit or Multivessel Stenting for Acute Myocardial Infarction (HELP AMI) Study. Int. J. Cardiovasc. Intervent. 2004, 6, 128–133. [Google Scholar]
- Politi, L.; Sgura, F.; Rossi, R.; Monopoli, D.; Guerri, E.; Leuzzi, C.; Bursi, F.; Sangiorgi, G.M.; Modena, M.G. A Randomised Trial of Target-Vessel versus Multi-Vessel Revascularisation in ST-Elevation Myocardial Infarction: Major Adverse Cardiac Events during Long-Term Follow-Up. Heart 2010, 96, 662–667. [Google Scholar] [CrossRef]
- Wald, D.S.; Morris, J.K.; Wald, N.J.; Chase, A.J.; Edwards, R.J.; Hughes, L.O.; Berry, C.; Oldroyd, K.G. Randomized Trial of Preventive Angioplasty in Myocardial Infarction. N. Engl. J. Med. 2013, 369, 1115–1123. [Google Scholar] [CrossRef] [Green Version]
- Gershlick, A.H.; Khan, J.N.; Chb, M.B.; Kelly, D.J.; Greenwood, J.P.; Sasikaran, T.; Curzen, N.; Blackman, D.J.; Dalby, M.; Fairbrother, K.L.; et al. Randomized Trial of Complete Versus Lesion-Only Revascularization in Patients Undergoing Primary Percutaneous Coronary Intervention for STEMI and Multivessel Disease The CvLPRIT Trial. J. Am. Coll. Cardiol. 2015, 65, 963–972. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mehta, S.R.; Wood, D.A.; Storey, R.F.; Mehran, R.; Bainey, K.R.; Nguyen, H.; Meeks, B.; di Pasquale, G.; López-Sendón, J.; Faxon, D.P.; et al. Complete Revascularization with Multivessel PCI for Myocardial Infarction. N. Engl. J. Med. 2019, 381, 1411–1421. [Google Scholar] [CrossRef] [Green Version]
- Wood, D.A.; Cairns, J.A.; Wang, J.; Mehran, R.; Storey, R.F.; Nguyen, H.; Meeks, B.; Kunadian, V.; Tanguay, J.F.; Kim, H.H.; et al. Timing of Staged Non culprit Artery Revascularization in Patients with ST-Segment Elevation Myocardial Infarction: COMPLETE Trial. J. Am. Coll. Cardiol. 2019, 74, 2713–2723. [Google Scholar] [CrossRef]
- Sheth, T.; Pinilla-Echeverri, N.; Moreno, R.; Wang, J.; Wood, D.A.; Storey, R.F.; Mehran, R.; Bainey, K.R.; Bossard, M.; Bangalore, S.; et al. Non culprit Lesion Severity and Outcome of Revascularization in Patients With STEMI and Multivessel Coronary Disease. J. Am. Coll. Cardiol. 2020, 76, 1277–1286. [Google Scholar] [CrossRef] [PubMed]
- Ntalianis, A.; Sels, J.-W.; Davidavicius, G.; Tanaka, N.; Muller, O.; Trana, C.; Barbato, E.; Hamilos, M.; Mangiacapra, F.; Heyndrickx, G.R.; et al. Fractional Flow Reserve for the Assessment of Nonculprit Coronary Artery Stenoses in Patients with Acute Myocardial Infarction. JACC Cardiovasc. Interv. 2010, 3, 1274–1281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Engstrøm, T.; Kelbæk, H.; Helqvist, S.; Høfsten, D.E.; Kløvgaard, L.; Holmvang, L.; Jørgensen, E.; Pedersen, F.; Saunamäki, K.; Clemmensen, P.; et al. Complete Revascularisation versus Treatment of the Culprit Lesion Only in Patients with ST-Segment Elevation Myocardial Infarction and Multivessel Disease (DANAMI-3-PRIMULTI): An Open-Label, Randomised Controlled Trial. Lancet 2015, 386, 665–671. [Google Scholar] [CrossRef]
- Lønborg, J.; Engstrøm, T.; Kelbæk, H.; Helqvist, S.; Kløvgaard, L.; Holmvang, L.; Pedersen, F.; Jørgensen, E.; Saunamäki, K.; Clemmensen, P.; et al. Fractional Flow Reserve-Guided Complete Revascularization Improves the Prognosis in Patients with ST-Segment-Elevation Myocardial Infarction and Severe Non culprit Disease. Circ. Cardiovasc. Interv. 2017, 10, e004460. [Google Scholar] [CrossRef]
- Smits, P.C.; Abdel-Wahab, M.; Neumann, F.-J.; Boxma-de Klerk, B.M.; Lunde, K.; Schotborgh, C.E.; Piroth, Z.; Horak, D.; Wlodarczak, A.; Ong, P.J.; et al. Fractional Flow Reserve–Guided Multivessel Angioplasty in Myocardial Infarction. N. Engl. J. Med. 2017, 376, 1234–1244. [Google Scholar] [CrossRef]
- Gupta, A.; Bajaj, N.S.; Arora, P.; Arora, G.; Qamar, A.; Bhatt, D.L. FFR-Guided Multivessel Stenting Reduces Urgent Revascularization Compared with Infarct-Related Artery Only Stenting in ST-Elevation Myocardial Infarction: A Meta-Analysis of Randomized Controlled Trials. Int. J. Cardiol. 2018, 252, 63–67. [Google Scholar] [CrossRef]
- Bainey, K.R.; Engstrøm, T.; Smits, P.C.; Gershlick, A.H.; James, S.K.; Storey, R.F.; Wood, D.A.; Mehran, R.; Cairns, J.A.; Mehta, S.R. Complete vs Culprit-Lesion-Only Revascularization for ST-Segment Elevation Myocardial Infarction: A Systematic Review and Meta-Analysis. JAMA Cardiol. 2020, 5, 881–888. [Google Scholar] [CrossRef]
- Puymirat, E.; Cayla, G.; Simon, T.; Steg, P.G.; Montalescot, G.; Durand-Zaleski, I.; le Bras, A.; Gallet, R.; Khalife, K.; Morelle, J.-F.; et al. Multivessel PCI Guided by FFR or Angiography for Myocardial Infarction. N. Engl. J. Med. 2021, 385, 297–308. [Google Scholar] [CrossRef]
- Lee, J.M.; Kim, H.K.; Park, K.H.; Choo, E.H.; Kim, C.J.; Lee, S.H.; Kim, M.C.; Hong, Y.J.; Ahn, S.G.; Doh, J.-H.; et al. Fractional Flow Reserve versus Angiography-Guided Strategy in Acute Myocardial Infarction with Multivessel Disease: A Randomized Trial. Eur. Heart J. 2023, 44, 473–484. [Google Scholar] [CrossRef]
- Ames, J.; Oldstein, A.G.; Emetriou, E.D.; Rines, I.L.G.; Azen, M.; Houkfeh, S.; O’n Eill, W. Multiple Complex Coronary Plaques in Patients with Acute Myocardial Infarction. N. Engl. J Med. 2000, 343, 915–922. [Google Scholar]
- Stone, G.W.; Maehara, A.; Lansky, A.J.; de Bruyne, B.; Cristea, E.; Mintz, G.S.; Mehran, R.; McPherson, J.; Farhat, N.; Marso, S.P.; et al. A Prospective Natural-History Study of Coronary Atherosclerosis. N. Engl. J. Med. 2011, 364, 226–235. [Google Scholar] [CrossRef]
- Waksman, R.; di Mario, C.; Torguson, R.; Ali, Z.A.; Singh, V.; Skinner, W.H.; Artis, A.K.; ten Cate, T.; Powers, E.; Kim, C.; et al. Identification of Patients and Plaques Vulnerable to Future Coronary Events with Near-Infrared Spectroscopy Intravascular Ultrasound Imaging: A Prospective, Cohort Study. Lancet 2019, 394, 1629–1637. [Google Scholar] [CrossRef] [PubMed]
- Oemrawsingh, R.M.; Cheng, J.M.; García-García, H.M.; van Geuns, R.-J.; de Boer, S.P.M.; Simsek, C.; Kardys, I.; Lenzen, M.J.; van Domburg, R.T.; Regar, E.; et al. Near-Infrared Spectroscopy Predicts Cardiovascular Outcome in Patients with Coronary Artery Disease. J. Am. Coll. Cardiol. 2014, 64, 2510–2518. [Google Scholar] [CrossRef]
- Xing, L.; Higuma, T.; Wang, Z.; Aguirre, A.D.; Mizuno, K.; Takano, M.; Dauerman, H.L.; Park, S.-J.; Jang, Y.; Kim, C.-J.; et al. Clinical Significance of Lipid-Rich Plaque Detected by Optical Coherence Tomography A 4-Year Follow-Up Study. J. Am. Coll. Cardiol. 2017, 69, 2502–2513. [Google Scholar] [CrossRef] [PubMed]
- Prati, F.; Romagnoli, E.; Gatto, L.; la Manna, A.; Burzotta, F.; Ozaki, Y.; Marco, V.; Boi, A.; Fineschi, M.; Fabbiocchi, F.; et al. Relationship Between coronary Plaque morphology of the Left Anterior Descending artery and 12months Clinical Outcome: The CLIMA Study. Eur. Heart J. 2020, 41, 383–391. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pinilla-Echeverri, N.; Mehta, S.R.; Wang, J.; Lavi, S.; Schampaert, E.; Cantor, W.J.; Bainey, K.R.; Welsh, R.C.; Kassam, S.; Mehran, R.; et al. Nonculprit Lesion Plaque Morphology in Patients with ST-Segment-Elevation Myocardial Infarction: Results from the COMPLETE Trial Optical Coherence Tomography Substudys. Circ. Cardiovasc. Interv. 2020, 13, e008768. [Google Scholar] [CrossRef]
- Stone, G.W.; Maehara, A.; Ali, Z.A.; Held, C.; Matsumura, M.; Kjøller-Hansen, L.; Bøtker, H.E.; Maeng, M.; Engstrøm, T.; Wiseth, R.; et al. Percutaneous Coronary Intervention for Vulnerable Coronary Atherosclerotic Plaque. J. Am. Coll. Cardiol. 2020, 76, 2289–2301. [Google Scholar] [CrossRef]
- Tian, J.; Dauerman, H.; Toma, C.; Samady, H.; Itoh, T.; Kuramitsu, S.; Domei, T.; Jia, H.; Vergallo, R.; Soeda, T.; et al. Prevalence and Characteristics of TCFA and Degree of Coronary Artery Stenosis An OCT, IVUS, and Angiographic Study. J. Am. Coll. Cardiol. 2014, 64, 672–680. [Google Scholar] [CrossRef] [Green Version]
- Burzotta, F.; Leone, A.M.; Aurigemma, C.; Zambrano, A.; Zimbardo, G.; Arioti, M.; Vergallo, R.; de Maria, G.L.; Cerracchio, E.; Romagnoli, E.; et al. Fractional Flow Reserve or Optical Coherence Tomography to Guide Management of Angiographically Intermediate Coronary Stenosis: A Single-Center Trial. JACC Cardiovasc. Interv. 2020, 13, 49–58. [Google Scholar] [CrossRef]
- Shlofmitz, E.; Jeremias, A.; Parviz, Y.; Galougahi, K.K.; Redfors, B.; Petrossian, G.; Edens, M.; Matsumura, M.; Maehara, A.; Mintz, G.S.; et al. External Elastic Lamina vs. Luminal Diameter Measurement for Determining Stent Diameter by Optical Coherence Tomography: An ILUMIEN III Substudy. Eur. Heart J. Cardiovasc. Imaging 2021, 22, 753–759. [Google Scholar] [CrossRef]
- Räber, L.; Mintz, G.S.; Koskinas, K.C.; Johnson, T.W.; Holm, N.R.; Onuma, Y.; Radu, M.D.; Joner, M.; Yu, B.; Jia, H.; et al. Clinical Use of Intracoronary Imaging. Part 1: Guidance and Optimization of Coronary Interventions. An Expert Consensus Document of the European Association of Percutaneous Cardiovascular Interventions. Eur. Heart J. 2018, 39, 3281–3300. [Google Scholar] [CrossRef] [Green Version]
- Tanaka, A.; Imanishi, T.; Kitabata, H.; Kubo, T.; Takarada, S.; Tanimoto, T.; Kuroi, A.; Tsujioka, H.; Ikejima, H.; Komukai, K.; et al. Lipid-Rich Plaque and Myocardial Perfusion after Successful Stenting in Patients with Non-ST-Segment Elevation Acute Coronary Syndrome: An Optical Coherence Tomography Study. Eur. Heart J. 2009, 30, 1348–1355. [Google Scholar] [CrossRef] [Green Version]
- Osman, M.; Syed, M.; Patibandla, S.; Sulaiman, S.; Kheiri, B.; Shah, M.K.; Bianco, C.; Balla, S.; Patel, B. Fifteen-Year Trends in Incidence of Cardiogenic Shock Hospitalization and in-Hospital Mortality in the United States. J. Am. Heart Assoc. 2021, 10, e021061. [Google Scholar] [CrossRef] [PubMed]
- Webb, J.G.; Lowe, A.M.; Sanborn, T.A.; White, H.D.; Sleeper, L.A.; Carere, R.G.; Buller, C.E.; Wong, S.C.; Boland, J.; Dzavik, V.; et al. Percutaneous Coronary Intervention for Cardiogenic Shock in the SHOCK Trial. J. Am. Coll. Cardiol. 2003, 42, 1380–1386. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sousa-Uva, M.; Neumann, F.J.; Ahlsson, A.; Alfonso, F.; Banning, A.P.; Benedetto, U.; Byrne, R.A.; Collet, J.P.; Falk, V.; Head, S.J.; et al. 2018 ESC/EACTS Guidelines on Myocardial Revascularization. Eur. Heart J. 2019, 55, 4–90. [Google Scholar] [CrossRef] [Green Version]
- Udith, J.; Ochman, S.H.; Leeper, Y.A.S.; Ohn, J.; Ebb, G.W.; Anborn, I.A.S.; Hite, A.D.W.; Avid, J.D.; Alley, T.; Hristopher, C.; et al. Early Revascularization in Acute Myocardial Infarction Complicated by Cardiogenic Shock. N. Engl. J. Med. 1999, 341, 625–634. [Google Scholar]
- White, H.D.; Assmann, S.F.; Sanborn, T.A.; Jacobs, A.K.; Webb, J.G.; Sleeper, L.A.; Wong, C.K.; Stewart, J.T.; Aylward, P.E.G.; Wong, S.C.; et al. Comparison of Percutaneous Coronary Intervention and Coronary Artery Bypass Grafting after Acute Myocardial Infarction Complicated by Cardiogenic Shock: Results from the Should We Emergently Revascularize Occluded Coronaries for Cardiogenic Shock (SHOCK) Trial. Circulation 2005, 112, 1992–2001. [Google Scholar]
- Thiele, H.; Akin, I.; Sandri, M.; Fuernau, G.; de Waha, S.; Meyer-Saraei, R.; Nordbeck, P.; Geisler, T.; Landmesser, U.; Skurk, C.; et al. PCI Strategies in Patients with Acute Myocardial Infarction and Cardiogenic Shock. N. Engl. J. Med. 2017, 377, 2419–2432. [Google Scholar] [CrossRef] [Green Version]
- Khan, M.S.; Siddiqi, T.J.; Usman, M.S.; Riaz, H.; Khan, A.R.; Murad, M.H.; Kalra, A.; Figueredo, V.M.; Bhatt, D.L. Meta-Analysis Comparing Culprit Vessel Only Versus Multivessel Percutaneous Coronary Intervention in Patients With Acute Myocardial Infarction and Cardiogenic Shock. Am. J. Cardiol. 2019, 123, 218–226. [Google Scholar] [CrossRef] [PubMed]
- Farhan, S.; Vogel, B.; Montalescot, G.; Barthelemy, O.; Zeymer, U.; Desch, S.; de Waha-Thiele, S.; Maier, L.S.; Sandri, M.; Akin, I.; et al. Association of Culprit Lesion Location with Outcomes of Culprit-Lesion-Only vs. Immediate Multivessel Percutaneous Coronary Intervention in Cardiogenic Shock: A Post Hoc Analysis of a Randomized Clinical Trial. JAMA Cardiol. 2020, 5, 1329–1337. [Google Scholar] [CrossRef] [PubMed]
- Rasoul, S.; Ottervanger, J.P.; de Boer, M.J.; Dambrink, J.H.E.; Hoorntje, J.C.A.; Marcel Gosselink, A.T.; Zijlstra, F.; Suryapranata, H.; van ’t Hof, A.W.J. Predictors of 30-Day and 1-Year Mortality after Primary Percutaneous Coronary Intervention for ST-Elevation Myocardial Infarction. Coron. Artery Dis. 2009, 20, 415–421. [Google Scholar] [CrossRef] [PubMed]
- Karthikeyan, G.; Peix, A.; Devasenapathy, N.; Jimenez-Heffernan, A.; Haque, S.U.; Rodella, C.; Giubbini, R.; Rosas, E.A.; Ozkan, E.; Keng, Y.J.F.; et al. Ischemia-Guided vs Routine Non-Culprit Vessel Angioplasty for Patients with ST Segment Elevation Myocardial Infarction and Multi-Vessel Disease: The IAEA SPECT STEMI Trial. J. Nucl. Cardiol. 2022, 1–12. [Google Scholar] [CrossRef]
- Ong, P.; Martínez Pereyra, V.; Sechtem, U.; Bekeredjian, R. Management of Patients with ST-Segment Myocardial Infarction and Multivessel Disease: What Are the Options in 2022? Coron. Artery Dis. 2022, 33, 485–489. [Google Scholar] [CrossRef]


{kind=link}
| Study | Population (n), Randomization Ratio | Intervention Group | Control Group | Assessment of NCL | Primary Endpoint | Results |
|---|---|---|---|---|---|---|
| PRAMI | n = 465, 1:1 | 234 patients with CR during index procedure | 231 patients with culprit-only revascularization | Angiography > 50% | MACE: Cardiovascular death, non-fatal MI, refractory angina at 23 months FU. | 9% vs. 23% (p < 0.001) |
| CvLPRIT | n = 296, 1:1 | 150 patients with CR during index procedure or index admission | 146 patients with culprit-only revascularization | Angiography > 70% (1 view) or >50% (2 views) | MACE: Death, MI, any repeat revascularization, HF at 1-year FU. | 10% vs. 21.2% (p = 0.009) |
| COMPLETE | n = 4041, 1:1 | 2016 patients with CR during staged procedure in index admission or post-discharge | 2025 patients with culprit-only revascularization | Angiography > 70% or angiography between 50%–69% and FFR < 0.80 | (1) Composite of cardiovascular death and MI. (2) Composite of cardiovascular death, MI, and ischemia driven revascularization (IDR) at 3-year FU. | (1) 7.8% vs. 10.5% (p = 0.004) (2) 8.9% vs. 16.7% (p < 0.001) |
| DANAMI-3-PRIMULTI | n = 627. 1:1 | 314 patients with CR during staged procedure in index admission | 313 patients with culprit-only revascularization | Angiography > 90% or angiography > 50% and FFR < 0.80 | MACE: Death, re-infarction, ischemia driven revascularization at 27-month FU. | 13% vs. 22% (p = 0.004) |
| COMPARE-ACUTE | n = 885, 2:1 | 295 patients with CR during index procedure or index admission | 590 patients with culprit-only revascularization | Angiography > 50% and FFR < 0.80 | MACE: Death, non-fatal MI, revascularization, cerebrovascular events at 1-year FU. | 8% vs. 21% (p < 0.001) |
| FLOWER-MI | n = 1163, 1:1 | 586 patients with CR FFR-guided during index procedure or index admission | 577 patients with CR angio-guided during index procedure or index admission | Angiography > 50% in the control group and angiography > 50% and FFR < 0.80 in the intervention group | Composite of death for any cause, non-fatal MI, and unplanned hospitalization leading to urgent revascularization at 1-year FU. | 5.5% vs. 4.2% (p = 0.31) |
| FRAME AMI | n = 562, 1:1 | 284 patients with CR FFR-guided PCI | 278 patients with CR angio-guided PCI | Angiography > 50% in the control group Angiography > 50% and FFR < 0.80 in the intervention group | Composite of time to death, MI or RR at 3.5-year FU. | 7.4% vs. 19.7% (p = 0.003) |
| CULPRIT-SHOCK | n = 706, 1:1 | 344 patients with CS in culprit lesion-only PCI | 342 patients with CS in immediate multivessel PCI | Angiography > 70% | Composite of death or severe renal failure leading to renal replacement therapy at 30-day FU. | 45.9% vs. 55.4 (p = 0.01) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Piccolo, R.; Manzi, L.; Simonetti, F.; Leone, A.; Angellotti, D.; Immobile Molaro, M.; Verde, N.; Cirillo, P.; Di Serafino, L.; Franzone, A.; et al. Management of Non-Culprit Lesions in STEMI Patients with Multivessel Disease. J. Clin. Med. 2023, 12, 2572. https://doi.org/10.3390/jcm12072572
Piccolo R, Manzi L, Simonetti F, Leone A, Angellotti D, Immobile Molaro M, Verde N, Cirillo P, Di Serafino L, Franzone A, et al. Management of Non-Culprit Lesions in STEMI Patients with Multivessel Disease. Journal of Clinical Medicine. 2023; 12(7):2572. https://doi.org/10.3390/jcm12072572
Chicago/Turabian StylePiccolo, Raffaele, Lina Manzi, Fiorenzo Simonetti, Attilio Leone, Domenico Angellotti, Maddalena Immobile Molaro, Nicola Verde, Plinio Cirillo, Luigi Di Serafino, Anna Franzone, and et al. 2023. "Management of Non-Culprit Lesions in STEMI Patients with Multivessel Disease" Journal of Clinical Medicine 12, no. 7: 2572. https://doi.org/10.3390/jcm12072572