

Alcohol Consumption within 48 hours before Onset Is Associated with Adverse Clinical Outcomes in Hypertriglyceridemic Pancreatitis

Abstract
:1. Introduction
2. Materials and Methods
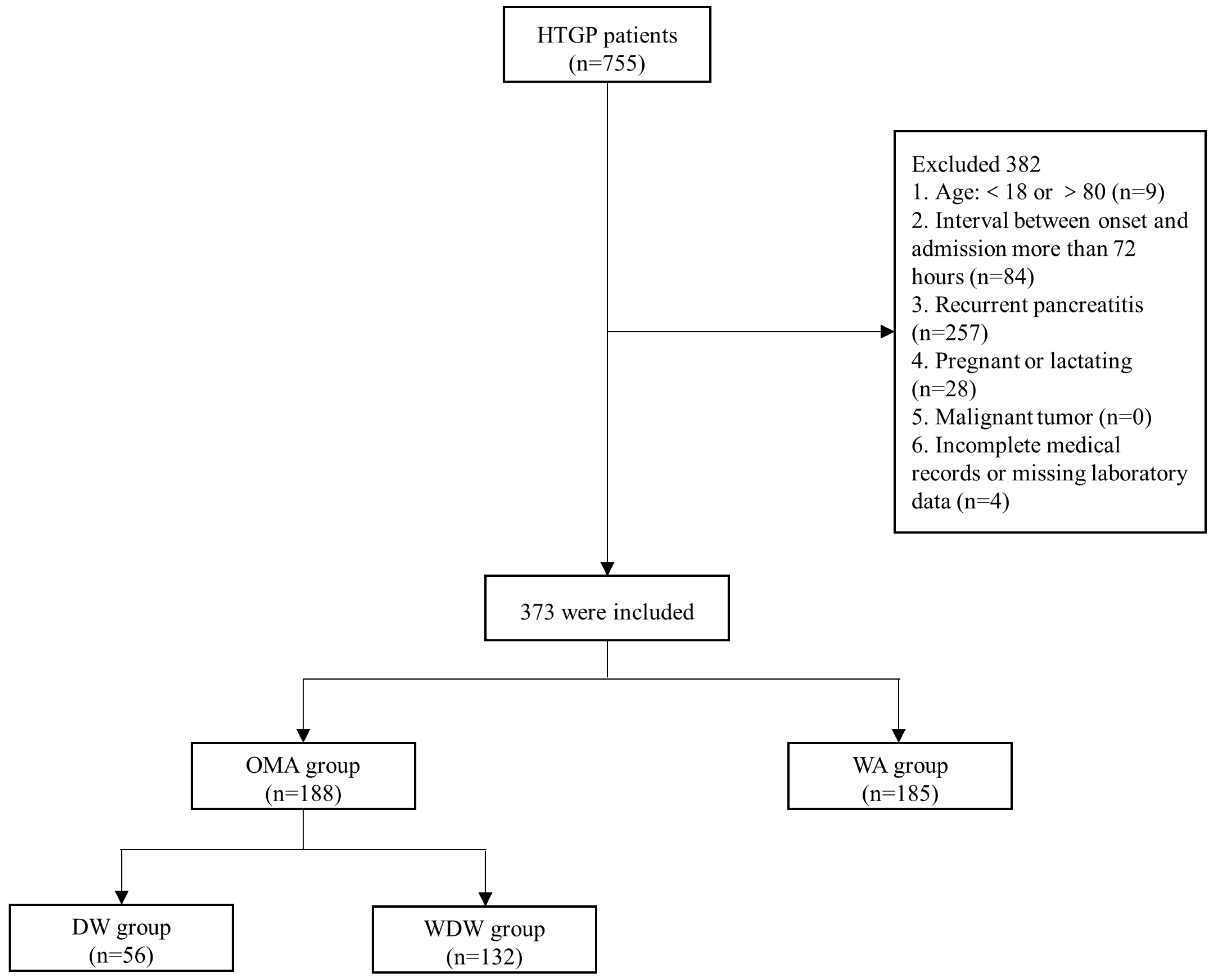
2.1. Study Design and Participants
2.2. Definition
2.3. Study Outcomes
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics, Clinical Scoring Systems and Laboratory Findings of Patients in the OMA Group and WA Group
3.2. Clinical Outcomes of Patients in the OMA Group and WA Group
3.3. Multivariate Logistic Regression Analysis for Primary Outcomes in OMA Group and WA Group
3.4. Subgroup Analysis
Baseline Characteristics, Clinical Scoring Systems, Laboratory Findings and Clinical Outcomes of the Patients in the DW Group and the WDW Group Were Analyzed
3.5. Multivariate Logistic Regression Analysis for Primary Outcomes among DW Group, WDW Group and WA Group
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Crockett, S.D.; Wani, S.; Gardner, T.B.; Falck-Ytter, Y.; Barkun, A.N.; American Gastroenterological Association Institute Clinical Guidelines Committee. American Gastroenterological Association Institute Guideline on Initial Management of Acute Pancreatitis. Gastroenterology 2018, 154, 1096–1101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xiao, A.Y.; Tan, M.L.Y.; Wu, L.M.; Asrani, V.M.; Windsor, J.A.; Yadav, D.; Petrov, M.S. Global incidence and mortality of pancreatic diseases: A systematic review, meta-analysis, and meta-regression of population-based cohort studies. Lancet Gastroenterol. Hepatol. 2016, 1, 45–55. [Google Scholar] [CrossRef] [PubMed]
- Iannuzzi, J.P.; King, J.A.; Leong, J.H.; Quan, J.; Windsor, J.W.; Tanyingoh, D.; Coward, S.; Forbes, N.; Heitman, S.J.; Shaheen, A.A.; et al. Global Incidence of Acute Pancreatitis Is Increasing Over Time: A Systematic Review and Meta-Analysis. Gastroenterology 2022, 162, 122–134. [Google Scholar] [CrossRef]
- Huang, Y.X.; Jia, L.; Jiang, S.M.; Wang, S.B.; Li, M.X.; Yang, B.H. Incidence and clinical features of hyperlipidemic acute pancreatitis from Guangdong, China: A retrospective multicenter study. Pancreas 2014, 43, 548–552. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jo, S.I.; Chang, J.H.; Kim, T.H.; Kim, C.W.; Kim, J.K.; Han, S.W. Subsets associated with developing acute pancreatitis in patients with severe hypertriglyceridemia and the severity of pancreatitis. Pancreatology 2019, 19, 795–800. [Google Scholar] [CrossRef]
- Jin, M.; Bai, X.; Chen, X.; Zhang, H.; Lu, B.; Li, Y.; Lai, Y.; Qian, J.; Yang, H. A 16-year trend of etiology in acute pancreatitis: The increasing proportion of hypertriglyceridemia-associated acute pancreatitis and its adverse effect on prognosis. J. Clin. Lipidol. 2019, 13, 947–953. [Google Scholar] [CrossRef]
- Zheng, Y.; Zhou, Z.; Li, H.; Li, J.; Li, A.; Ma, B.; Zhang, T.; Liao, Q.; Ye, Y.; Zhang, Z.; et al. A multicenter study on etiology of acute pancreatitis in Beijing during 5 years. Pancreas 2015, 44, 409–414. [Google Scholar] [CrossRef]
- Zhu, Y.; Pan, X.; Zeng, H.; He, W.; Xia, L.; Liu, P.; Zhu, Y.; Chen, Y.; Lv, N. A Study on the Etiology, Severity, and Mortality of 3260 Patients With Acute Pancreatitis According to the Revised Atlanta Classification in Jiangxi, China Over an 8-Year Period. Pancreas 2017, 46, 504–509. [Google Scholar] [CrossRef]
- Pu, W.; Luo, G.; Chen, T.; Jing, L.; Hu, Q.; Li, X.; Xia, H.; Deng, M.; Lü, M.; Chen, X.J.P. A 5-Year Retrospective Cohort Study: Epidemiology, Etiology, Severity, and Outcomes of Acute Pancreatitis. Pancreas 2020, 49, 1161–1167. [Google Scholar] [CrossRef]
- Tenner, S.; Baillie, J.; DeWitt, J.; Vege, S.S.; American College of Gastroenterology. American College of Gastroenterology guideline: Management of acute pancreatitis. Am. J. Gastroenterol. 2013, 108, 1400–1415. [Google Scholar] [CrossRef]
- Deng, L.; Xue, P.; Huang, L.; Yang, X.; Wan, M.; Xia, Q. Binge drinking aggravates the outcomes of first-attack severe acute pancreatitis. Pancreas 2010, 39, 149–152. [Google Scholar] [CrossRef]
- Papachristou, G.I.; Muddana, V.; Yadav, D.; O’Connell, M.; Sanders, M.K.; Slivka, A.; Whitcomb, D.C. Comparison of BISAP, Ranson’s, APACHE-II, and CTSI scores in predicting organ failure, complications, and mortality in acute pancreatitis. Am. J. Gastroenterol. 2010, 105, 435–441, quiz 442. [Google Scholar] [CrossRef]
- Hagjer, S.; Kumar, N. Evaluation of the BISAP scoring system in prognostication of acute pancreatitis—A prospective observational study. Int. J. Surg. 2018, 54, 76–81. [Google Scholar] [CrossRef]
- Banks, P.A.; Bollen, T.L.; Dervenis, C.; Gooszen, H.G.; Johnson, C.D.; Sarr, M.G.; Tsiotos, G.G.; Vege, S.S.; Acute Pancreatitis Classification Working, G. Classification of acute pancreatitis—2012: Revision of the Atlanta classification and definitions by international consensus. Gut 2013, 62, 102–111. [Google Scholar] [CrossRef] [PubMed]
- Yeligar, S.M.; Chen, M.M.; Kovacs, E.J.; Sisson, J.H.; Burnham, E.L.; Brown, L.A. Alcohol and lung injury and immunity. Alcohol 2016, 55, 51–59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Criddle, D.N. The role of fat and alcohol in acute pancreatitis: A dangerous liaison. Pancreatology 2015, 15, S6–S12. [Google Scholar] [CrossRef] [PubMed]
- Klop, B.; do Rego, A.T.; Cabezas, M.C. Alcohol and plasma triglycerides. Curr. Opin. Lipidol. 2013, 24, 321–326. [Google Scholar] [CrossRef]
- Schneider, J.; Liesenfeld, A.; Mordasini, R.; Schubotz, R.; Zöfel, P.; Kubel, F.; Vandré-Plozzitzka, C.; Kaffarnik, H. Lipoprotein fractions, lipoprotein lipase and hepatic triglyceride lipase during short-term and long-term uptake of ethanol in healthy subjects. Atherosclerosis 1985, 57, 281–291. [Google Scholar] [CrossRef]
- Mudráková, E.; Poledne, R.; Kovář, J. Postprandial triglyceridemia after single dose of alcohol in healthy young men. Nutr. Metab. Cardiovasc. Dis. NMCD 2013, 23, 183–188. [Google Scholar] [CrossRef]
- Nawaz, H.; Koutroumpakis, E.; Easler, J.; Slivka, A.; Whitcomb, D.C.; Singh, V.P.; Yadav, D.; Papachristou, G.I. Elevated serum triglycerides are independently associated with persistent organ failure in acute pancreatitis. Am. J. Gastroenterol. 2015, 110, 1497–1503. [Google Scholar] [CrossRef]
- Zhang, Y.; He, W.; He, C.; Wan, J.; Lin, X.; Zheng, X.; Li, L.; Li, X.; Yang, X.; Yu, B.; et al. Large triglyceride-rich lipoproteins in hypertriglyceridemia are associated with the severity of acute pancreatitis in experimental mice. Cell Death Dis. 2019, 10, 728. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Havel, R.J. Pathogenesis, differentiation and management of hypertriglyceridemia. Adv. Intern. Med. 1969, 15, 117–154. [Google Scholar] [PubMed]
- Lee, P.J.; Papachristou, G.I. New insights into acute pancreatitis. Nat. Rev. Gastroenterol. Hepatol. 2019, 16, 479–496. [Google Scholar] [CrossRef]
- Kirkpatrick, A.W.; Roberts, D.J.; De Waele, J.; Jaeschke, R.; Malbrain, M.L.; De Keulenaer, B.; Duchesne, J.; Bjorck, M.; Leppaniemi, A.; Ejike, J.C.; et al. Intra-abdominal hypertension and the abdominal compartment syndrome: Updated consensus definitions and clinical practice guidelines from the World Society of the Abdominal Compartment Syndrome. Intensive Care Med. 2013, 39, 1190–1206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dellinger, R.P.; Levy, M.M.; Rhodes, A.; Annane, D.; Gerlach, H.; Opal, S.M.; Sevransky, J.E.; Sprung, C.L.; Douglas, I.S.; Jaeschke, R.; et al. Surviving Sepsis Campaign: International guidelines for management of severe sepsis and septic shock, 2012. Intensive Care Med. 2013, 39, 165–228. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variables | Total | OMA Group (n = 188) | WA Group (n = 185) | p |
|---|---|---|---|---|
| Sex(male), n (%) | 305 (81.8) | 180 (95.7) | 125 (67.6) | <0.001 |
| Age, years, IQR | 41.0 (33.0–47.0) | 42.0 (35.0–47.0) | 40.0 (31.0–46.0) | 0.204 |
| BMI, kg/m2, IQR | 25.9 (24.0–27.6) | 26.1 (24.2–27.8) | 25.5 (23.9–27.4) | 0.272 |
| Transfer status, n (%) | 218 (58.4) | 110 (58.5) | 108 (58.4) | 0.979 |
| History of smoking, n (%) | 144 (38.6) | 116 (61.7) | 28 (15.1) | <0.001 |
| Comorbidities, n (%) | ||||
| Hypertension | 65 (17.4) | 31 (16.5) | 34 (18.4) | 0.631 |
| Diabetes mellitus | 76 (20.4) | 40 (21.3) | 36 (19.5) | 0.663 |
| Hyperlipidemia | 81 (21.7) | 44 (23.4) | 37 (20.0) | 0.425 |
| COPD | 2 (0.5) | 1 (0.5) | 1 (0.5) | 1 |
| Coronary artery disease | 1 (0.3) | 1 (0.5) | 0 (0) | 1 |
| Variables | Total | OMA Group (n = 188) | WA Group (n = 185) | p |
|---|---|---|---|---|
| Clinical score systems, n (%) | ||||
| CTSI score ≥ 4 | 157 (42.1) | 82 (43.6) | 75 (40.5) | 0.547 |
| Ranson score ≥ 3 | 203 (54.4) | 102 (54.3) | 101 (54.6) | 0.948 |
| APACHE II score ≥ 8 | 154 (41.3) | 91 (48.4) | 63 (34.1) | 0.005 |
| Laboratory findings, median (IQR) | ||||
| WBC, × 109/L | 13.1 (10.4–16.1) | 12.6 (10.0–16.0) | 14.0 (11.1–17.2) | 0.013 |
| Hb, g/L, | 158 (144–174) | 158 147–178) | 157 (141–173) | 0.073 |
| HCT, % | 44.6 (41.0–49.0) | 44.9 (41.8–49.9) | 44.0 (40.1–47.7) | 0.027 |
| Serum ALT, U/L | 24.0 (16.0–36.0) | 25.0 (16.0–36.0) | 23.0 (15.0–36.0) | 0.400 |
| Serum AST, U/L | 29.4 (22.0–47.0) | 33.0 (23.0–52.0) | 27.0 (20.0–42.0) | 0.007 |
| Serum TB, umol/L | 14.2 (9.9–20.9) | 15.2 (10.7–22.9) | 13.0 (9.7–19.6) | 0.015 |
| Serum DB, umol/L | 3.4 (2.0–5.2) | 3.8 (2.5–5.9) | 3.0 (1.9–4.7) | 0.002 |
| Serum TG, mmol/L | 18.1 (13.9–27.0) | 18.1 (14.0–27.0) | 18.0 (13.9–27.0) | 0.621 |
| Serum GLU, mmol/L | 12.6 (8.5–17.4) | 12.2 (8.5–16.8) | 13.9 (8.5–17.6) | 0.318 |
| Serum BUN, mmol/L | 4.8 (3.5–6.8) | 4.9 (3.5–7.1) | 4.8 (3.5–6.4) | 0.521 |
| Serum Cr, umol/L | 66.0 (53.5–91.5) | 68.0 (56.1–102.0) | 62.7 (50.8–86.2) | 0.033 |
| Serum Ca, mmol/L | 2.0 (1.7–2.2) | 2.0 (1.7–2.2) | 2.0 (1.7–2.2) | 0.549 |
| Serum CRP, mg/L | 214 (134–372) | 250.0 (145.0–384.0) | 197.0 (121.0–334.0) | 0.060 |
| Variables | Total | OMA Group (n = 188) | WA Group (n = 185) | p |
|---|---|---|---|---|
| Primary outcomes, n (%) | ||||
| SAP | 134 (35.9) | 77 (41.0) | 57 (30.8) | 0.041 |
| Necrotizing pancreatitis | 131 (35.1) | 76 (40.4) | 55 (29.7) | 0.030 |
| Secondary outcomes | ||||
| Persistent organ failure, n (%) | 134 (35.9) | 77 (41.0) | 57 (30.8) | 0.041 |
| Persistent respiratory failure | 130 (34.9) | 76 (40.4) | 54 (29.2) | 0.023 |
| Persistent renal failure | 48 (12.9) | 30 (16.0) | 18 (9.7) | 0.073 |
| Persistent circulatory failure | 25 (6.7) | 16 (8.5) | 9 (4.9) | 0.159 |
| Persistent MOF, n (%) | 51 (13.7) | 34 (18.1) | 17 (9.2) | 0.012 |
| ACS, n (%) | 23 (6.2) | 13 (6.9) | 10 (5.4) | 0.545 |
| Sepsis, n (%) | 31 (8.3) | 20 (10.6) | 11 (6.0) | 0.101 |
| IPN, n (%) | 42 (11.3) | 25 (13.3) | 17 (9.2) | 0.209 |
| Organ function support, n (%) | ||||
| CRRT | 57 (15.3) | 31 (16.5) | 26 (14.1) | 0.513 |
| Mechanical ventilation | 75 (20.1) | 48 (25.5) | 27 (14.6) | 0.008 |
| Local complications, n (%) | ||||
| APFC | 133 (35.7) | 61 (32.4) | 72 (38.9) | 0.192 |
| ANC | 131 (35.1) | 76 (40.4) | 55 (29.7) | 0.030 |
| PPC | 3 (0.8) | 2 (1.1) | 1 (0.5) | 1 |
| WON | 35 (9.4) | 21 (11.2) | 14 (7.6) | 0.233 |
| Interventions of local complications, n (%) | 42 (11.3) | 27 (14.4) | 15 (8.1%) | 0.056 |
| PCD | 38 (10.2) | 24 (12.8) | 14 (7.6) | 0.097 |
| ETD | 7 (1.9) | 5 (2.7) | 2 (1.1) | 0.449 |
| ETN | 14 (3.8) | 8 (4.3) | 6 (3.2) | 0.607 |
| ON | 4 (1.1) | 4 (2.1) | 0 (0) | 0.123 |
| Length of hospital stay, days, IQR | 11.0 (7.0–18.0) | 12.0 (7.0–19.0) | 10.0 (7.0–16.0) | 0.157 |
| Hospital total costs, yuan, IQR | 26,993 (14,538–57,137) | 31,118 (16,287–66,847) | 23,999 (12,466–46,117) | 0.016 |
| ICU admission, n (%) | 139 (37.3) | 78 (41.5) | 61 (33.0) | 0.089 |
| Dead, n (%) | 26 (7.0) | 16 (8.5) | 10 (5.4) | 0.239 |
| OR (95% CI) | p | |
|---|---|---|
| SAP | ||
| Transfer status (ref: no) | ||
| Yes | 1.40 (0.90, 2.18) | 0.132 |
| Hypertension (ref: no) | ||
| Yes | 1.52 (0.86, 2.67) | 0.15 |
| Hyperlipidemia (ref: no) | ||
| Yes | 1.32 (0.78, 2.22) | 0.303 |
| Drinking status (ref: without alcohol) | ||
| occasional or moderate alcohol | 1.57 (1.02, 2.41) | 0.041 |
| Necrotizing pancreatitis | ||
| Age, year | 1.02 (1.00, 1.04) | 0.083 |
| Transfer status (ref: no) | ||
| Yes | 1.89 (1.20, 2.97) | 0.006 |
| Drinking status (ref: without alcohol) | ||
| occasional or moderate alcohol | 1.60 (1.04, 2.48) | 0.034 |
| Variables | Total | DW (n = 56) | WDW (n = 132) | p |
|---|---|---|---|---|
| Primary outcomes, n (%) | ||||
| SAP | 77 (41.0) | 32 (57.1) | 45 (34.1) | 0.003 |
| Necrotizing pancreatitis | 76 (40.4) | 30 (53.6) | 46 (34.8) | <0.017 |
| Secondary outcomes | ||||
| Persistent organ failure, n (%) | 77 (41.0) | 32 (57.1) | 45 (34.1) | 0.003 |
| Persistent respiratory failure | 76 (40.4) | 31 (55.4) | 45 (34.1) | 0.007 |
| Persistent renal failure | 30 (16.0) | 13 (23.2) | 17 (12.9) | 0.077 |
| Persistent circulatory failure | 16 (8.5) | 5 (8.9) | 11 (8.3) | 1 |
| Persistent MOF, n (%) | 34 (18.1) | 13 (23.2) | 21 (15.9) | 0.234 |
| ACS, n (%) | 13 (6.9) | 6 (10.7) | 7 (5.3) | 0.306 |
| Sepsis, n (%) | 20 (10.6) | 9 (16.1) | 11 (8.3) | 0.116 |
| IPN, n (%) | 25 (13.3) | 11 (19.6) | 14 (10.6) | 0.095 |
| Organ function support, n (%) | ||||
| CRRT | 31 (16.5) | 12 (21.4) | 19 (14.4) | 0.235 |
| Mechanical ventilation | 48 (25.5) | 19 (33.9) | 29 (22.0) | 0.085 |
| Local complications, n (%) | ||||
| APFC | 61 (32.4) | 13 (23.2) | 48 (36.4) | 0.078 |
| ANC | 76 (40.4) | 30 (53.6) | 46 (34.8) | <0.017 |
| PPC | 2 (1.1) | 1 (1.8) | 1 (0.8) | 0.508 |
| WON | 21 (11.2) | 10 (17.9) | 11 (8.3) | 0.058 |
| Interventions of local complications, n (%) | 27 (14.4) | 11 (19.6) | 16 (12.1) | 0.179 |
| PCD | 24 (12.8) | 10 (17.9) | 14 (10.6) | 0.173 |
| ETD | 5 (2.7) | 0 (0) | 5 (3.8) | 0.327 |
| ETN | 8 (4.3) | 2 (3.6) | 6 (4.5) | 1 |
| ON | 4 (2.1) | 2 (3.6) | 2 (1.5) | 0.733 |
| Length of hospital stay, days, IQR | 12.0 (7.0–19.0) | 16.5 (8.0–24.0) | 11.0 (7.0–16.0) | 0.019 |
| Hospital total costs, yuan, IQR | 31,118 (16,287–66,847) | 51,366 (22,230–11,2063) | 26,603 (15,486–54,197) | 0.008 |
| ICU admission, n (%) | 78 (41.5) | 32 (57.1) | 46 (34.8) | 0.005 |
| Dead, n (%) | 16 (8.5) | 6 (10.7) | 10 (7.6) | 0.675 |
| OR (95% CI) | p | |
|---|---|---|
| SAP | ||
| Transfer status (ref: no) | ||
| Yes | 1.35 (0.86, 2.11) | 0.187 |
| Hypertension (ref: no) | ||
| Yes | 1.67 (0.94, 2.96) | 0.081 |
| Hyperlipidemia (ref: no) | ||
| Yes | 1.29 (0.76, 2.18) | 0.353 |
| Drinking status (ref: without alcohol) | ||
| without drinking within 48 h before onset (WDW) | 1.16 (0.72, 1.88) | 0.544 |
| drinking within 48 h before onset (DW) | 3.09 (1.66, 5.77) | <0.001 |
| Necrotizing pancreatitis | ||
| Age, year | 1.02 (1.00, 1.05) | 0.06 |
| Transfer status (ref: no) | ||
| Yes | 1.84 (1.17, 2.89) | 0.009 |
| Drinking status (ref: without alcohol) | ||
| without drinking within 48 h before onset (WDW) | 1.26 (0.78, 2.05) | 0.345 |
| drinking within 48 h before onset (DW) | 2.71 (1.46, 5.05) | 0.002 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lai, T.; Zhu, Y.; Lu, N.; He, W. Alcohol Consumption within 48 hours before Onset Is Associated with Adverse Clinical Outcomes in Hypertriglyceridemic Pancreatitis. J. Clin. Med. 2023, 12, 2566. https://doi.org/10.3390/jcm12072566
Lai T, Zhu Y, Lu N, He W. Alcohol Consumption within 48 hours before Onset Is Associated with Adverse Clinical Outcomes in Hypertriglyceridemic Pancreatitis. Journal of Clinical Medicine. 2023; 12(7):2566. https://doi.org/10.3390/jcm12072566
Chicago/Turabian StyleLai, Tianming, Yin Zhu, Nonghua Lu, and Wenhua He. 2023. "Alcohol Consumption within 48 hours before Onset Is Associated with Adverse Clinical Outcomes in Hypertriglyceridemic Pancreatitis" Journal of Clinical Medicine 12, no. 7: 2566. https://doi.org/10.3390/jcm12072566