

Challenges of the Effectiveness of Traumatic Brain Injuries Biomarkers in the Sports-Related Context

Abstract
:1. Introduction
2. Methods
3. Results
3.1. Current Guidelines
3.2. Markers
3.2.1. Markers of Neuronal Cell Body Injury
3.2.2. Markers of Glial Cell Injury
3.2.3. Markers of Axonal Injury
3.2.4. Markers of Inflammation
3.2.5. Other Markers

3.3. Methodological Assessment of mTBI Biomarkers
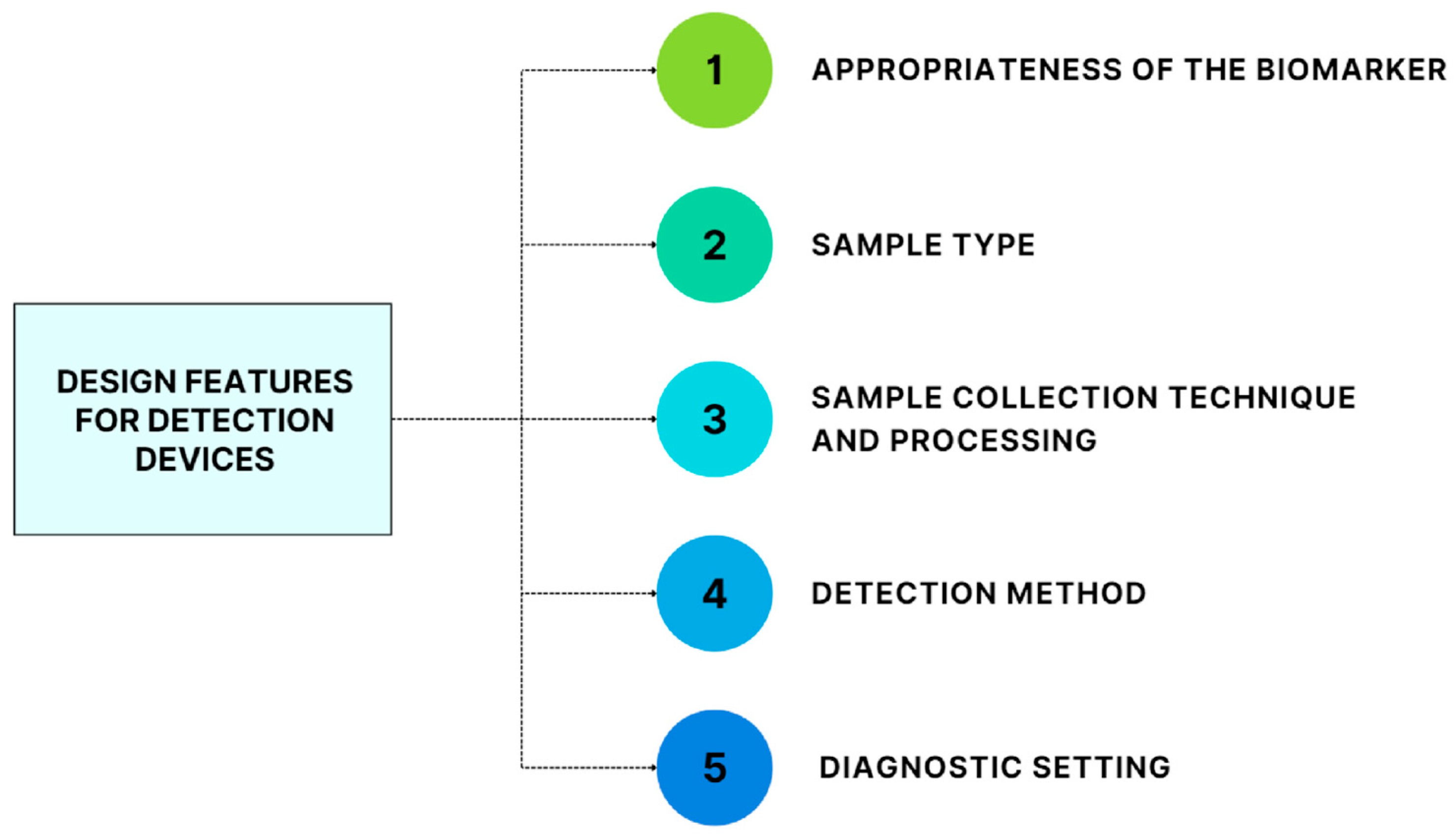
- (1)
- Appropriateness of the biomarker. The measured biomarkers should already provide proven clinically actionable information and be approved by regulatory agencies [34].
- (2)
- Sample type. Protein biomarkers can be found in CSF, serum, and plasma [34], as reported in depth for each biomarker in the previous paragraph.
- (3)
- Sample-collection technique and processing. They are conditioned by the choice of sample type, dictating kinetics, bioavailability, and assay detection limit [35].
- (4)
- Choice of the detection method. Conventional clinical immunoassays are antibody-based methods that exploit automated platforms based on turbidimetry or nephelometry. They are spectrophotometric-based methods, and rely on the formation of an immune complex that scatters light; they can suffer reduced signal-to-noise levels in samples with high protein or lipid concentrations (such as serum) that cause non-specific light scattering. Other antibody-based detection methods are based on antibodies conjugated to various labels such as enzymes, fluorophores, and chemiluminescent compounds (as in enzyme-linked immunosorbent assay (ELISA), sandwich ELISA, and competitive ELISA). Most immunoassay-based methods currently available in the clinical laboratory analyze each target of interest independently; therefore, analysis using a panel of biomarkers would require separate aliquots of the sample [34,36]. On the contrary, multiplexed assays allow the simultaneous measurement of multiple analytes, and are therefore more suitable for detecting a panel of protein biomarkers for mTBI. Multiplexed assays can be divided into planar and microsphere-suspension designs. The planar immunoassays are similar to traditional single-target immunoassays. They involve different microspots with specific capture antibodies arranged in a two-dimensional layout: The capture antibodies bind to the target, there is the addition of a detection antibody, and the specificity of the signal is then indicated by the x,y location. Microsphere-suspension immunoassays are most frequently used for multiplexed antibody-based assays: the capture antibodies are bound to microspheres that can be univocally identified by size or fluorescence, the microspheres bind to the target antigen, followed by the addition of a labelled detection antibody, and the beads are then determined by flow cytometry [36,37]. In the mTBI context, multiplexed immunoassays are preferred as they allow simultaneous measurement of multiple analytes with reduced sample volume. Their use is not without limitations: They require a comprehensive method of validation and complex quality control procedures. There can also be further complications if one or more quality control results fail for some but not for all the analytes, and it can be challenging to optimize the analytical conditions for several antigen–antibody interactions [34,36].
- (5)
- The diagnostic setting. In the context of mTBI, it would be ideal to have a device that could be used inside and outside the hospital. A point-of-care (POC) platform would enable rapid triage directly at the site of injury without requiring processing in a laboratory, thanks to its small and portable nature, the reduced requirement of sample volume, and fast turnaround time. It could also be used for monitoring and assessment in the ambulance and for monitoring the patient’s response at the hospital, with repeated measurements [32,36,38]. Many POC designs are available, but a critical difference that can enhance their quality is the presence of a built-in control that can indicate the correct execution of the assay. The most relevant POC designs in the mTBI context are lateral flow and cartridge/cassette devices. The detection they provide can be based on different principles (visual observation by the operator, charge-coupled device cameras, absorbance, surface plasmon resonance, fixed-polarized ellipsometry, diffraction, etc.) [36].

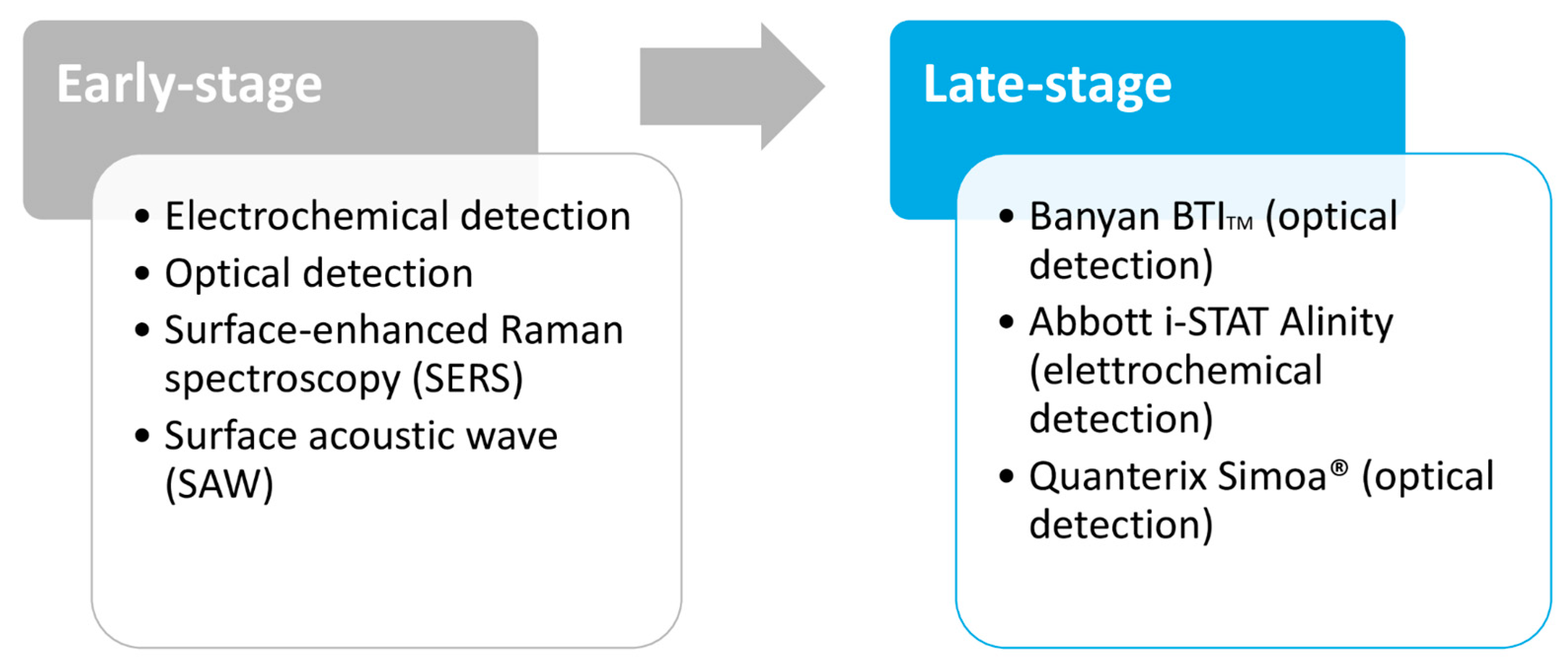
3.4. Technological Development Stage of Biomarker Detection Devices

{kind=link}
{kind=link}
{kind=link}
| Device | Detection Technique | Biomarkers | Sample | Analysis Time | Multiplex | References |
|---|---|---|---|---|---|---|
| Banyan BTI | Optical (chemiluminescence) | GFAP, UCH-L1 | Human serum | >2 h | No | [54] |
| Abbott i-STAT Alinity | Electrochemical (amperometric) | GFAP, UCH-L1 | Human plasma | 15 min | Yes | [55,56,57,58] |
| Quanterix Simoa® | Optical (fluorescence) | GFAP, UCH-L1, Tau, NF, NSE | Human serum, plasma, and CSF | 2 h 30 min per plate | Yes | [59,60,61] |
4. Discussion
4.1. Impact of mTBI Biomarkers on the Diagnostic-Therapeutic Pathway
4.2. Analytical Performances and Clinical Reliability
| Marker | Sample | Detection Time | Cut-Off | CNS Specificity | Sensitivity % | Specificity % | NPV % | PPV % | AUC | Method | Refs. |
|---|---|---|---|---|---|---|---|---|---|---|---|
| GFAP | Blood/Serum and CSF | 20–24 h post-injury | 30.0 pg/mL | Yes | 44.2 | 94.9 | 34.8 | 96.5 | 0.74–0.98 | ELISA platform (Banyan Biomarkers Inc.) | [25,64,66,68] |
| UCH-L1 | Blood/Serum and CSF | 6–24 h post-injury | 30.0 pg/mL | Also expressed in distal renal tubules and islets of Langerhans | 78.2 | 37.3 | 34.9 | 79.9 | 0.87 | ELISA platform (Banyan Biomarkers Inc.) | [68,70,71] |
| NFs | Blood and CSF | Rise through 12 d post-injury | 24.0 pg/mL | Also found in PNS | 97 | 96 | Not reported | Not reported | 0.99 | ELISA single-molecule array technology for quantification of NF-L | [77] |
| IL6 | Plasma or serum | 6–8 h post-injury | Not reported | No | Not reported | Not reported | Not reported | Not reported | 0.81 | Ultrasensitive single-molecule ELISA (SIMOA) | [30] |
| IL6 | Serum | 6–8 h post-injury | Not reported | No | 52 | 81 | Not reported | Not reported | Not reported | MSD V-PLEX assays | [29] |
| GFAP + UCH-L1 | EDTA anticoagulated plasma sample (20 µL) | Within 12 h of injury | 22 pg/mL GFAP and 327 pg/mL UCH-L1 | Yes | 97.6 | 36.4 | 99.6 | 9.5 | 0.94 | Abbott i-STAT Alinity | [70,73] |
4.3. Analytical Limitations and Conclusions
5. Future Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dewan, M.C.; Rattani, A.; Gupta, S.; Baticulon, R.E.; Hung, Y.-C.; Punchak, M.; Agrawal, A.; Adeleye, A.O.; Shrime, M.G.; Rubiano, A.M.; et al. Estimating the global incidence of traumatic brain injury. J. Neurosurg. 2019, 130, 1080–1097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holm, L.; Cassidy, J.D.; Carroll, L.; Borg, J. Summary of the WHO collaborating centre for neurotrauma task force on mild traumatic brain injury. J. Rehabil. Med. 2005, 37, 137–141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stein, S.C.; Spettell, C.; Young, G.; Ross, S.E. Limitations of neurological assessment in mild head injury. Brain Inj. 1993, 7, 425–430. [Google Scholar] [CrossRef]
- Easter, J.S.; Haukoos, J.S.; Meehan, W.P.; Novack, V.; Edlow, J.A. Will Neuroimaging Reveal a Severe Intracranial Injury in This Adult with Minor Head Trauma? JAMA 2015, 314, 2672. [Google Scholar] [CrossRef] [PubMed]
- Shackford, S.R.; Wald, S.L.; Ross, S.E.; Cogbill, T.H.; Hoyt, D.B.; Morris, J.A.; Mucha, P.A.; Pachter, H.L.; Sugerman, H.J. The clinical utility of computed tomographic scanning and neurologic examination in the management of patients with minor head injuries. J. Trauma Inj. Infect. Crit. Care 1992, 33, 385–394. [Google Scholar] [CrossRef]
- Langfitt, T.W.; Obrist, W.D.; Alavi, A.; Grossman, R.I.; Zimmerman, R.A.; Jaggi, J.; Uzzell, B.P.; Reivich, M.; Patton, D.R. Computerized tomography, magnetic resonance imaging, and positron emission tomography in the study of brain trauma. J. Neurosurg. 1986, 64, 760–767. [Google Scholar] [CrossRef]
- Lee, B.; Newberg, A. Neuroimaging in traumatic brain imaging. Neurorx 2005, 2, 372–383. [Google Scholar] [CrossRef]
- Eisele, A.; Hill-Strathy, M.; Michels, L.; Rauen, K. Magnetic Resonance Spectroscopy following Mild Traumatic Brain Injury: A Systematic Review and Meta-Analysis on the Potential to Detect Posttraumatic Neurodegeneration. Neurodegener. Dis. 2020, 20, 2–11. [Google Scholar] [CrossRef]
- Lefevre-Dognin, C.; Cogné, M.; Perdrieau, V.; Granger, A.; Heslot, C.; Azouvi, P. Definition and epidemiology of mild traumatic brain injury. Neurochirurgie 2020, 67, 218–221. [Google Scholar] [CrossRef]
- Danna-Dos-Santos, A.; Mohapatra, S.; Santos, M.; Degani, A.M. Long-term effects of mild traumatic brain injuries to oculomotor tracking performances and reaction times to simple environmental stimuli. Sci. Rep. 2018, 8, 4583. [Google Scholar] [CrossRef] [Green Version]
- Ghaith, H.S.; Nawar, A.A.; Gabra, M.D.; Abdelrahman, M.E.; Nafady, M.H.; Bahbah, E.I.; Ebada, M.A.; Ashraf, G.M.; Negida, A.; Barreto, G.E. A Literature Review of Traumatic Brain Injury Biomarkers. Mol. Neurobiol. 2022, 59, 4141–4158. [Google Scholar] [CrossRef]
- McDonald, S.J.; Shultz, S.R.; Agoston, D.V. The Known Unknowns: An Overview of the State of Blood-Based Protein Biomarkers of Mild Traumatic Brain Injury. J. Neurotrauma 2021, 38, 2652–2666. [Google Scholar] [CrossRef] [PubMed]
- Helmrich, M.I.R.A.R.; Lingsma, H.F.; Turgeon, A.F.; Yamal, J.-M.; Steyerberg, E.W. Prognostic Research in Traumatic Brain Injury: Markers, Modeling, and Methodological Principles. J. Neurotrauma 2021, 38, 2502–2513. [Google Scholar] [CrossRef] [PubMed]
- Foks, K.A.; Cnossen, M.C.; Dippel, D.W.; Maas, A.I.; Menon, D.; van der Naalt, J.; Steyerberg, E.W.; Lingsma, H.F.; Polinder, S.; on behalf of CENTER-TBI investigators and participants. Management of Mild Traumatic Brain Injury at the Emergency Department and Hospital Admission in Europe: A Survey of 71 Neurotrauma Centers Participating in the CENTER-TBI Study. J. Neurotrauma 2017, 34, 2529–2535. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stiell, I.G.; Wells, G.A.; Vandemheen, K.; Clement, C.; Lesiuk, H.; Laupacis, A.; McKnight, R.D.; Verbeek, R.; Brison, R.; Cass, D.; et al. The Canadian CT Head Rule for patients with minor head injury. Lancet 2001, 357, 1391–1396. [Google Scholar] [CrossRef]
- Ingebrigtsen, T.; Romner, B.; Kock-Jensen, C. Scandinavian Guidelines for Initial Management of Minimal, Mild, and Moderate Head Injuries. J. Trauma Inj. Infect. Crit. Care 2000, 48, 760–766. [Google Scholar] [CrossRef]
- Undén, J.; the Scandinavian Neurotrauma Committee (SNC); Ingebrigtsen, T.; Romner, B. Scandinavian guidelines for initial management of minimal, mild and moderate head injuries in adults: An evidence and consensus-based update. BMC Med. 2013, 11, 50. [Google Scholar] [CrossRef] [Green Version]
- Stiell, I.; Clement, C.M.; Rowe, B.H.; Schull, M.; Brison, R.; Cass, D.; Eisenhauer, M.A.; McKnight, R.D.; Bandiera, G.; Holroyd, B.; et al. Comparison of the Canadian CT Head Rule and the New Orleans Criteria in Patients with Minor Head Injury. JAMA 2005, 294, 1511–1518. [Google Scholar] [CrossRef] [Green Version]
- Goodacre, S. Hospital admissions with head injury following publication of NICE guidance. Emerg. Med. J. 2008, 25, 556–557. [Google Scholar] [CrossRef] [Green Version]
- Yates, D.; Aktar, R.; Hill, J. Assessment, investigation, and early management of head injury: Summary of NICE guidance. BMJ 2007, 335, 719–720. [Google Scholar] [CrossRef] [Green Version]
- National Institute for Health and Care Excellence (NICE). Head Injury: Assessment and Early Management. Guidance. Available online: https://www.nice.org.uk/guidance/cg176 (accessed on 17 December 2022).
- Fabbri, A.; Servadei, F.; Marchesini, G.; Dente, M.; Iervese, T.; Spada, M.; Vandelli, A. Clinical Performance of NICE Recommendations versus NCWFNS Proposal in Patients with Mild Head Injury. J. Neurotrauma 2005, 22, 1419–1427. [Google Scholar] [CrossRef] [PubMed]
- Servadei, F.; Teasdale, G.; Merry, G. Defining Acute Mild Head Injury in Adults: A Proposal Based on Prognostic Factors, Diagnosis, and Management. J. Neurotrauma 2001, 18, 657–664. [Google Scholar] [CrossRef] [PubMed]
- Huibregtse, M.E.; Bazarian, J.J.; Shultz, S.R.; Kawata, K. The biological significance and clinical utility of emerging blood biomarkers for traumatic brain injury. Neurosci. Biobehav. Rev. 2021, 130, 433–447. [Google Scholar] [CrossRef] [PubMed]
- Shahim, P.; Zetterberg, H. Neurochemical Markers of Traumatic Brain Injury: Relevance to Acute Diagnostics, Disease Monitoring, and Neuropsychiatric Outcome Prediction. Biol. Psychiatry 2021, 91, 405–412. [Google Scholar] [CrossRef]
- FDA Authorizes Marketing of First Blood Test to Aid in the Evaluation of Concussion in Adults. 2020. Available online: https://www.fda.gov/news-events/press-announcements/fda-authorizes-marketing-first-blood-test-aid-evaluation-concussion-adults (accessed on 16 December 2022).
- Khalil, M.; Teunissen, C.E.; Otto, M.; Piehl, F.; Sormani, M.P.; Gattringer, T.; Barro, C.; Kappos, L.; Comabella, M.; Fazekas, F.; et al. Neurofilaments as biomarkers in neurological disorders. Nat. Rev. Neurol. 2018, 14, 577–589. [Google Scholar] [CrossRef] [PubMed]
- Nitta, M.E.; Savitz, J.; Nelson, L.D.; Teague, T.K.; Hoelzle, J.B.; McCrea, M.A.; Meier, T.B. Acute elevation of serum inflammatory markers predicts symptom recovery after concussion. Neurology 2019, 93, e497–e507. [Google Scholar] [CrossRef]
- Meier, T.B.; Huber, D.L.; Bohorquez-Montoya, L.; Nitta, M.E.; Savitz, J.; Teague, T.K.; Bazarian, J.J.; Hayes, R.L.; Nelson, L.D.; McCrea, M.A. A Prospective Study of Acute Blood-Based Biomarkers for Sport-Related Concussion. Ann. Neurol. 2020, 87, 907–920. [Google Scholar] [CrossRef]
- Edwards, K.A.; Gill, J.M.; Pattinson, C.L.; Lai, C.; Brière, M.; Rogers, N.J.; Milhorn, D.; Elliot, J.; Carr, W. Interleukin-6 is associated with acute concussion in military combat personnel. BMC Neurol. 2020, 20, 209. [Google Scholar] [CrossRef]
- Shaw, A.C.; Goldstein, D.R.; Montgomery, R.R. Age-dependent dysregulation of innate immunity. Nat. Rev. Immunol. 2013, 13, 875–887. [Google Scholar] [CrossRef] [Green Version]
- Visser, K.; Koggel, M.; Blaauw, J.; van der Horn, H.J.; Jacobs, B.; van der Naalt, J. Blood-based biomarkers of inflammation in mild traumatic brain injury: A systematic review. Neurosci. Biobehav. Rev. 2021, 132, 154–168. [Google Scholar] [CrossRef]
- Wang, W.; Kwon, E.J.; Tsai, L.-H. MicroRNAs in learning, memory, and neurological diseases: Figure 1. Learn. Mem. 2012, 19, 359–368. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zetterberg, H.; Blennow, K. Fluid biomarkers for mild traumatic brain injury and related conditions. Nat. Rev. Neurol. 2016, 12, 563–574. [Google Scholar] [CrossRef] [PubMed]
- Kawata, K.; Liu, C.Y.; Merkel, S.F.; Ramirez, S.H.; Tierney, R.T.; Langford, D. Blood biomarkers for brain injury: What are we measuring? Neurosci. Biobehav. Rev. 2016, 68, 460–473. [Google Scholar] [CrossRef] [Green Version]
- Strathmann, F.G.; Schulte, S.; Goerl, K.; Petron, D.J. Blood-based biomarkers for traumatic brain injury: Evaluation of research approaches, available methods and potential utility from the clinician and clinical laboratory perspectives. Clin. Biochem. 2014, 47, 876–888. [Google Scholar] [CrossRef] [PubMed]
- Martins, T.B.; Anderson, J.L.; Muhlestein, J.B.; Horne, B.D.; Carlquist, J.F.; Roberts, W.L.; Hill, H.R. Risk Factor Analysis of Plasma Cytokines in Patients with Coronary Artery Disease by a Multiplexed Fluorescent Immunoassay. Am. J. Clin. Pathol. 2006, 125, 906–913. [Google Scholar] [CrossRef] [PubMed]
- Pankratova, N.; Jović, M.; Pfeifer, M.E. Electrochemical sensing of blood proteins for mild traumatic brain injury (mTBI) diagnostics and prognostics: Towards a point-of-care application. RSC Adv. 2021, 11, 17301–17319. [Google Scholar] [CrossRef] [PubMed]
- Krausz, A.D.; Korley, F.K.; Burns, M.A. The Current State of Traumatic Brain Injury Biomarker Measurement Methods. Biosensors 2021, 11, 319. [Google Scholar] [CrossRef]
- Haselwood, B.A.; La Belle, J.T. Development of electrochemical methods to enzymatically detect traumatic brain injury biomarkers. Biosens. Bioelectron. 2015, 67, 752–756. [Google Scholar] [CrossRef] [Green Version]
- Manesh, K.M.; Halámek, J.; Pita, M.; Zhou, J.; Tam, T.K.; Santhosh, P.; Chuang, M.-C.; Windmiller, J.R.; Abidin, D.; Katz, E.; et al. Enzyme logic gates for the digital analysis of physiological level upon injury. Biosens. Bioelectron. 2009, 24, 3569–3574. [Google Scholar] [CrossRef]
- Kim, C.; Searson, P.C. Magnetic bead-quantum dot assay for detection of a biomarker for traumatic brain injury. Nanoscale 2015, 7, 17820–17826. [Google Scholar] [CrossRef] [Green Version]
- Krausz, A.D.; Korley, F.K.; Burns, M.A. A Variable Height Microfluidic Device for Multiplexed Immunoassay Analysis of Traumatic Brain Injury Biomarkers. Biosensors 2021, 11, 320. [Google Scholar] [CrossRef] [PubMed]
- Langer, J.; Jimenez de Aberasturi, D.; Aizpurua, J.; Alvarez-Puebla, R.A.; Auguié, B.; Baumberg, J.J.; Bazan, G.C.; Bell, S.E.J.; Boisen, A.; Brolo, A.G.; et al. Present and Future of Surface-Enhanced Raman Scattering. ACS Nano 2020, 14, 28–117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pérez-Jiménez, A.I.; Lyu, D.; Lu, Z.; Liu, G.; Ren, B. Surface-enhanced Raman spectroscopy: Benefits, trade-offs and future developments. Chem. Sci. 2020, 11, 4563–4577. [Google Scholar] [CrossRef] [Green Version]
- Li, C.; Shah, K.A.; Narayan, R.K. Rapid detection of traumatic brain injury. Nat. Biomed. Eng. 2020, 4, 579–580. [Google Scholar] [CrossRef] [PubMed]
- Gao, X.; Zheng, P.; Kasani, S.; Wu, S.; Yang, F.; Lewis, S.; Nayeem, S.; Engler-Chiurazzi, E.B.; Wigginton, J.G.; Simpkins, J.W.; et al. Paper-Based Surface-Enhanced Raman Scattering Lateral Flow Strip for Detection of Neuron-Specific Enolase in Blood Plasma. Anal. Chem. 2017, 89, 10104–10110. [Google Scholar] [CrossRef] [PubMed]
- Gao, X.; Boryczka, J.; Zheng, P.; Kasani, S.; Yang, F.; Engler-Chiurazzi, E.B.; Simpkins, J.W.; Wigginton, J.G.; Wu, N. A “hot Spot”-Enhanced paper lateral flow assay for ultrasensitive detection of traumatic brain injury biomarker S-100β in blood plasma. Biosens. Bioelectron. 2021, 177, 112967. [Google Scholar] [CrossRef]
- Li, D.; Yang, M.; Li, H.; Mao, L.; Wang, Y.; Sun, B. SERS based protocol using flow glass-hemostix for detection of neuron-specific enolase in blood plasma. New J. Chem. 2018, 43, 5925–5931. [Google Scholar] [CrossRef]
- Chen, Z.; Zhou, J.; Tang, H.; Liu, Y.; Shen, Y.; Yin, X.; Zheng, J.; Zhang, H.; Wu, J.; Shi, X.; et al. Ultrahigh-Frequency Surface Acoustic Wave Sensors with Giant Mass-Loading Effects on Electrodes. ACS Sens. 2020, 5, 1657–1664. [Google Scholar] [CrossRef]
- Agostini, M.; Amato, F.; Vieri, M.; Greco, G.; Tonazzini, I.; Baroncelli, L.; Caleo, M.; Vannini, E.; Santi, M.; Signore, G.; et al. Glial-fibrillary-acidic-protein (GFAP) biomarker detection in serum-matrix: Functionalization strategies and detection by an ultra-high-frequency surface-acoustic-wave (UHF-SAW) lab-on-chip. Biosens. Bioelectron. 2020, 172, 112774. [Google Scholar] [CrossRef]
- Heller, A.; Feldman, B. Electrochemical Glucose Sensors and Their Applications in Diabetes Management. Chem. Rev. 2008, 108, 2482–2505. [Google Scholar] [CrossRef] [Green Version]
- Banyan Biomarkers. Discovery, Validation, Commercialization of Biochemical Markers. Available online: http://www.banyanbio.com/ (accessed on 17 December 2022).
- Banyan Provides Non-Exclusive License of Traumatic Brain Injury (TBI) Biomarkers to Abbott for Use on its Core Laboratory Instruments. 2019. Available online: https://www.businesswire.com/news/home/20190404005161/en/Banyan-Provides-Non-Exclusive-License-of-Traumatic-Brain-Injury-TBI-Biomarkers-to-Abbott-for-Use-on-its-Core-Laboratory-Instruments (accessed on 16 December 2022).
- 510(k) Substantial Equivalence Determination Decision Summary Assay Only. Available online: https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfpmn/pmn.cfm?ID=K201778 (accessed on 17 December 2022).
- Bazarian, J.J.; Welch, R.D.; Caudle, K.; Jeffrey, C.A.; Chen, J.Y.; Chandran, R.; McCaw, T.; Datwyler, S.A.; Zhang, H.; McQuiston, B. Accuracy of a rapid glial fibrillary acidic protein/ubiquitin carboxyl-terminal hydrolase L1 test for the prediction of intracranial injuries on head computed tomography after mild traumatic brain injury. Acad. Emerg. Med. 2021, 28, 1308–1317. [Google Scholar] [CrossRef] [PubMed]
- Abbott MediaRoom. Abbott Receives FDA 510(k) Clearance for the First Rapid Handheld Blood Test for Concussions. Available online: https://abbott.mediaroom.com/2021-01-11-Abbott-Receives-FDA-510-k-Clearance-for-the-First-Rapid-Handheld-Blood-Test-for-Concussions (accessed on 17 December 2022).
- Korley, F.K.; Jain, S.; Sun, X.; Puccio, A.M.; Yue, J.K.; Gardner, R.C.; Wang, K.K.W.; Okonkwo, D.O.; Yuh, E.L.; Mukherjee, P.; et al. Prognostic value of day-of-injury plasma GFAP and UCH-L1 concentrations for predicting functional recovery after traumatic brain injury in patients from the US TRACK-TBI cohort: An observational cohort study. Lancet Neurol. 2022, 21, 803–813. [Google Scholar] [CrossRef] [PubMed]
- Rissin, D.M.; Kan, C.W.; Campbell, T.G.; Howes, S.C.; Fournier, D.R.; Song, L.; Piech, T.; Patel, P.P.; Chang, L.; Rivnak, A.J.; et al. Single-molecule enzyme-linked immunosorbent assay detects serum proteins at subfemtomolar concentrations. Nat. Biotechnol. 2010, 28, 595–599. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rissin, D.M.; Kan, C.W.; Song, L.; Rivnak, A.J.; Fishburn, M.W.; Shao, Q.; Piech, T.; Ferrell, E.P.; Meyer, R.E.; Campbell, T.G.; et al. Multiplexed single molecule immunoassays. Lab Chip 2013, 13, 2902–2911. [Google Scholar] [CrossRef] [PubMed]
- Quanterix. Simoa Assay Kits. Available online: https://www.quanterix.com/simoa-assay-kits/ (accessed on 17 December 2022).
- CENTER-TBI. Available online: https://www.center-tbi.eu/ (accessed on 16 December 2022).
- TRACK-TBI. Transforming Research and Clinical Knowledge in TBI. Available online: https://tracktbi.ucsf.edu/ (accessed on 16 December 2022).
- Luoto, T.M.; Raj, R.; Posti, J.P.; Gardner, A.J.; Panenka, W.J.; Iverson, G.L. A Systematic Review of the Usefulness of Glial Fibrillary Acidic Protein for Predicting Acute Intracranial Lesions following Head Trauma. Front. Neurol. 2017, 8, 652. [Google Scholar] [CrossRef] [Green Version]
- CDC Injury Center. Updated Mild Traumatic Brain Injury Guideline for Adults. Concussion. Traumatic Brain Injury. 2021. Available online: https://www.cdc.gov/traumaticbraininjury/mtbi_guideline.html (accessed on 17 December 2022).
- Papa, L.; Brophy, G.M.; Welch, R.D.; Lewis, L.M.; Braga, C.F.; Tan, C.N.; Ameli, N.J.; Lopez, M.A.; Haeussler, C.A.; Giordano, D.I.M.; et al. Time Course and Diagnostic Accuracy of Glial and Neuronal Blood Biomarkers GFAP and UCH-L1 in a Large Cohort of Trauma Patients with and Without Mild Traumatic Brain Injury. JAMA Neurol. 2016, 73, 551–560. [Google Scholar] [CrossRef] [Green Version]
- Huebschmann, N.A.; Luoto, T.M.; Karr, J.E.; Berghem, K.; Blennow, K.; Zetterberg, H.; Ashton, N.J.; Simrén, J.; Posti, J.P.; Gill, J.M.; et al. Comparing Glial Fibrillary Acidic Protein (GFAP) in Serum and Plasma Following Mild Traumatic Brain Injury in Older Adults. Front. Neurol. 2020, 11, 1054. [Google Scholar] [CrossRef]
- Lewis, L.M.; Schloemann, D.T.; Papa, L.; Fucetola, R.P.; Bazarian, J.; Lindburg, M.; Welch, R.D. Utility of Serum Biomarkers in the Diagnosis and Stratification of Mild Traumatic Brain Injury. Acad. Emerg. Med. 2017, 24, 710–720. [Google Scholar] [CrossRef] [Green Version]
- Mondello, S.; Linnet, A.; Buki, A.; Robicsek, S.; Gabrielli, A.; Tepas, J.; Papa, L.; Brophy, G.M.; Tortella, F.; Hayes, R.L.; et al. Clinical utility of serum levels of ubiquitin C-terminal hydrolase as a biomarker for severe traumatic brain injury. Neurosurgery 2012, 70, 666–675. [Google Scholar] [CrossRef] [Green Version]
- Papa, L.M.; Lewis, L.M.; Silvestri, S.; Falk, J.L.; Giordano, P.; Brophy, G.M.; Demery, J.A.; Liu, M.C.M.; Mo, J.; Akinyi, L.M.; et al. Serum levels of ubiquitin C-terminal hydrolase distinguish mild traumatic brain injury from trauma controls and are elevated in mild and moderate traumatic brain injury patients with intracranial lesions and neurosurgical intervention. J. Trauma Inj. Infect. Crit. Care 2012, 72, 1335–1344. [Google Scholar] [CrossRef] [Green Version]
- Biberthaler, P.; Musaelyan, K.; Krieg, S.; Meyer, B.; Stimmer, H.; Zapf, J.; von Matthey, F.; Chandran, R.; Marino, J.A.; Beligere, G.; et al. Evaluation of Acute Glial Fibrillary Acidic Protein and Ubiquitin C-Terminal Hydrolase-L1 Plasma Levels in Traumatic Brain Injury Patients with and without Intracranial Lesions. Neurotrauma Rep. 2021, 2, 617–625. [Google Scholar] [CrossRef] [PubMed]
- Shahjouei, S.; Sadeghi-Naini, M.; Yang, Z.; Kobeissy, F.; Rathore, D.; Shokraneh, F.; Blackburn, S.; Manley, G.T.; Wang, K.K. The diagnostic values of UCH-L1 in traumatic brain injury: A meta-analysis. Brain Inj. 2017, 32, 1–17. [Google Scholar] [CrossRef]
- Bazarian, J.J.; Biberthaler, P.; Welch, R.D.; Lewis, L.M.; Barzo, P.; Bogner-Flatz, V.; Brolinson, P.G.; Büki, A.; Chen, J.Y.; Christenson, R.H.; et al. Serum GFAP and UCH-L1 for prediction of absence of intracranial injuries on head CT (ALERT-TBI): A multicentre observational study. Lancet Neurol. 2018, 17, 782–789. [Google Scholar] [CrossRef]
- Hiskens, M.I.; Schneiders, A.G.; Angoa-Pérez, M.; Vella, R.K.; Fenning, A.S. Blood biomarkers for assessment of mild traumatic brain injury and chronic traumatic encephalopathy. Biomarkers 2020, 25, 213–227. [Google Scholar] [CrossRef]
- Diaz-Arrastia, R.; Wang, K.; Papa, L.; Sorani, M.D.; Yue, J.; Puccio, A.M.; McMahon, P.J.; Inoue, T.; Yuh, E.L.; Lingsma, H.F.; et al. Acute Biomarkers of Traumatic Brain Injury: Relationship between Plasma Levels of Ubiquitin C-Terminal Hydrolase-L1 and Glial Fibrillary Acidic Protein. J. Neurotrauma 2014, 31, 19–25. [Google Scholar] [CrossRef]
- Shahim, P.; Politis, A.; van der Merwe, A.; Moore, B.; Ekanayake, V.; Lippa, S.M.; Chou, Y.-Y.; Pham, D.L.; Butman, J.A.; Diaz-Arrastia, R.; et al. Time course and diagnostic utility of NfL, tau, GFAP, and UCH-L1 in subacute and chronic TBI. Neurology 2020, 95, e623–e636. [Google Scholar] [CrossRef]
- Shahim, P.; Gren, M.; Liman, V.; Andreasson, U.; Norgren, N.; Tegner, Y.; Mattsson, N.; Andreasen, N.; Öst, M.; Zetterberg, H.; et al. Serum neurofilament light protein predicts clinical outcome in traumatic brain injury. Sci. Rep. 2016, 6, 36791. [Google Scholar] [CrossRef]
- Edwards, K.A.; Pattinson, C.L.; Guedes, V.A.; Peyer, J.; Moore, C.; Davis, T.; Devoto, C.; Turtzo, L.C.; Latour, L.; Gill, J.M. Inflammatory Cytokines Associate with Neuroimaging After Acute Mild Traumatic Brain Injury. Front. Neurol. 2020, 11, 348. [Google Scholar] [CrossRef]

| Risk Factor | New Orleans Criteria | Canadian CT Head Rule | NICE 2014 | NCWFS | Scandinavian |
|---|---|---|---|---|---|
| Headache | High risk | High risk | Medium risk | ||
| Vomiting | High risk | High risk | High risk | High risk | Medium risk |
| Post-traumatic seizure | High risk | High risk | High risk | ||
| Intoxication (drug or alcohol) | High risk | High risk | |||
| Persistent anterograde amnesia | High risk | High risk | |||
| Age | High risk > 60 years | High risk > 65 years | High risk > 65 years | ||
| Clinical signs of skull fracture | High risk | High risk | High risk | High risk | High risk |
| Contusion of the skull | High risk | High risk | High risk | High risk | High risk |
| Signs official fracture | High risk | ||||
| Contusion of the face | High risk | ||||
| GCS score deterioration | High risk | High risk | High risk | ||
| Pedestrian versus vehicle | Medium risk | High risk | |||
| Ejected from vehicle | Medium risk | High risk | |||
| Fall from height | Medium risk | High risk | |||
| Prolonged post-traumatic amnesia | Medium risk | High risk | High risk | Medium risk | |
| GCS < 15 at presentation | High risk | High risk | High risk | ||
| Loss of consciousness | High risk | Medium risk | |||
| Neurologic deficit | High risk | High risk | Medium risk | ||
| Anticoagulation therapy | High risk | High risk | High risk | ||
| High-energy trauma | |||||
| Multiple injuries | |||||
| Pre-traumatic seizure | High risk | ||||
| Unclear trauma mechanism | |||||
| Previous neurosurgery | High risk | ||||
| S100B ≥ 0.1 μg/L | Medium risk |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tomaiuolo, R.; Zibetti, M.; Di Resta, C.; Banfi, G. Challenges of the Effectiveness of Traumatic Brain Injuries Biomarkers in the Sports-Related Context. J. Clin. Med. 2023, 12, 2563. https://doi.org/10.3390/jcm12072563
Tomaiuolo R, Zibetti M, Di Resta C, Banfi G. Challenges of the Effectiveness of Traumatic Brain Injuries Biomarkers in the Sports-Related Context. Journal of Clinical Medicine. 2023; 12(7):2563. https://doi.org/10.3390/jcm12072563
Chicago/Turabian StyleTomaiuolo, Rossella, Martina Zibetti, Chiara Di Resta, and Giuseppe Banfi. 2023. "Challenges of the Effectiveness of Traumatic Brain Injuries Biomarkers in the Sports-Related Context" Journal of Clinical Medicine 12, no. 7: 2563. https://doi.org/10.3390/jcm12072563