
The Midwest Sarcoma Trials Partnership: Bridging Academic and Community Networks in a Collaborative Approach to Sarcoma
 , ,
, ,  , and
, and 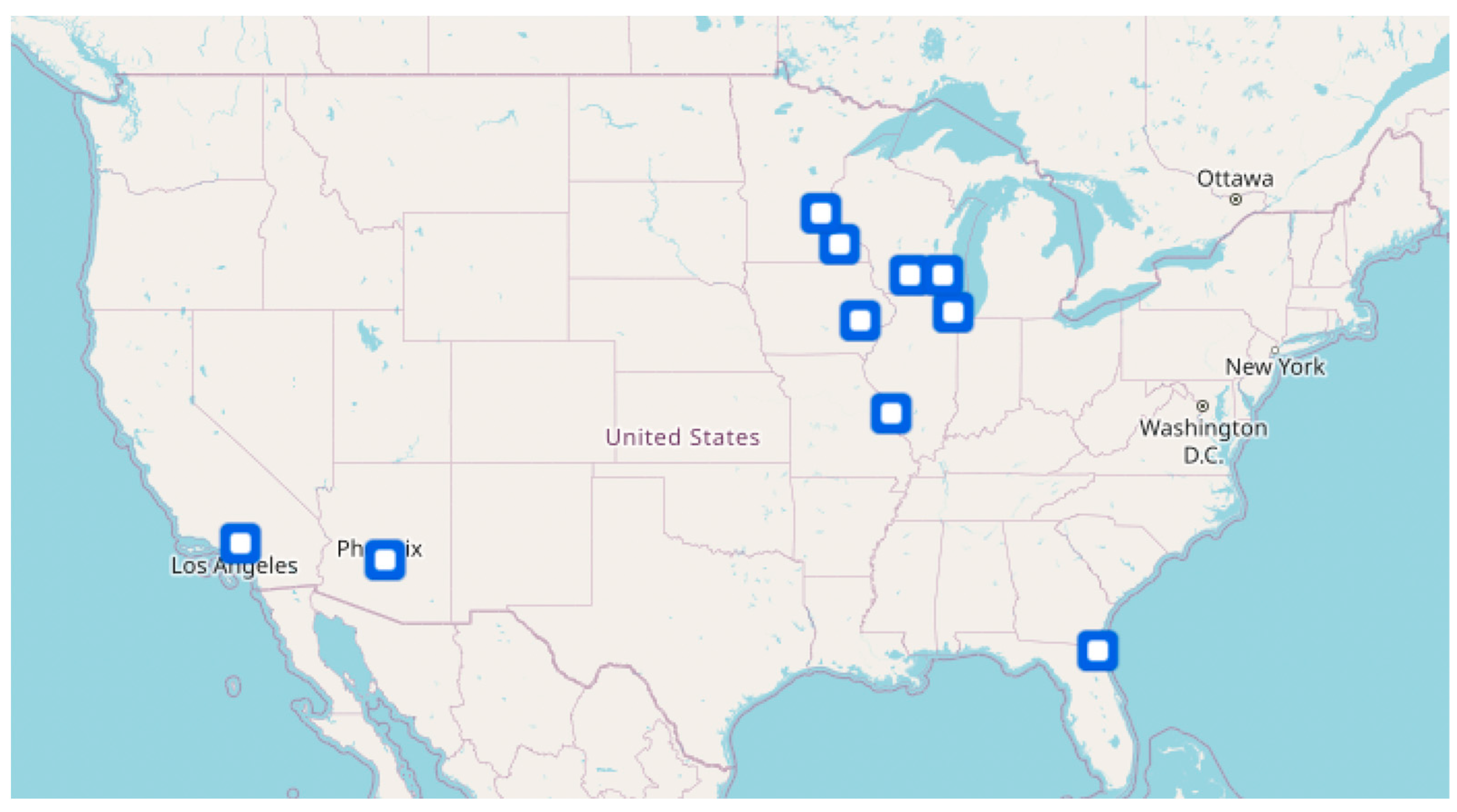{kind=link}
{kind=link}
Abstract
:1. Sarcoma and the Complexities of Treatment
2. Collaboration between Academic and Community Programs in Sarcoma
3. The City of Hope and the Midwest Sarcoma Trials Partnership
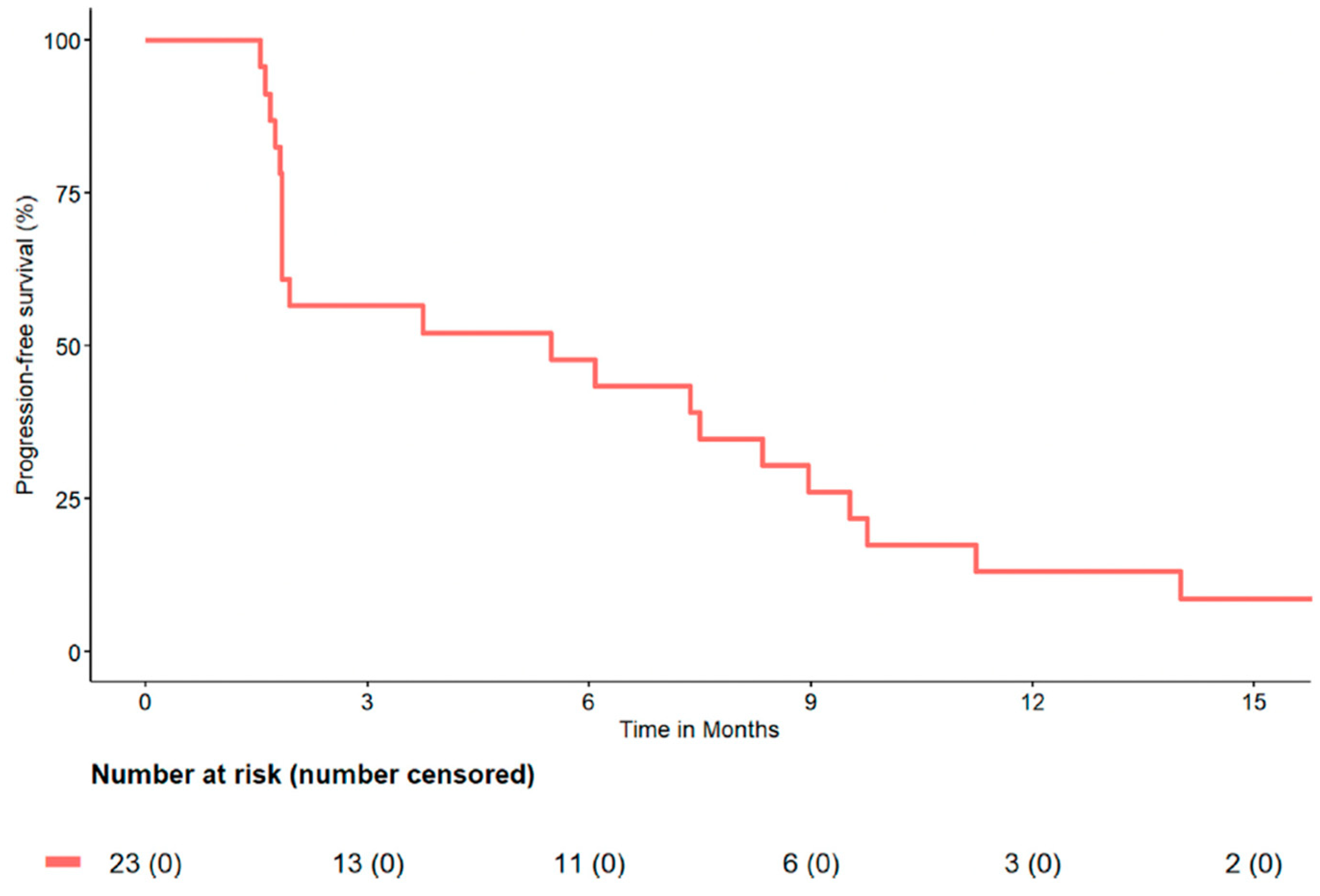
4. MWSTP’s Impact on Soft Tissue Sarcoma Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer statistics, 2022. CA Cancer J. Clin. 2022, 72, 7–33. [Google Scholar] [CrossRef] [PubMed]
- Grünewald, T.G.; Alonso, M.; Avnet, S.; Banito, A.; Burdach, S.; Cidre-Aranaz, F.; Di Pompo, G.; Distel, M.; Dorado-Garcia, H.; Garcia-Castro, J.; et al. Sarcoma treatment in the era of molecular medicine. EMBO Mol. Med. 2020, 12, e11131. [Google Scholar] [CrossRef]
- Yoon, S.S.; Segal, N.H.; Olshen, A.B.; Brennan, M.F.; Singer, S. Circulating angiogenic factor levels correlate with extent of disease and risk of recurrence in patients with soft tissue sarcoma. Ann. Oncol. 2004, 15, 1261–1266. [Google Scholar] [CrossRef]
- Farid, M.; Ngeow, J. Sarcomas Associated with Genetic Cancer Predisposition Syndromes: A Review. Oncol. 2016, 21, 1002–1013. [Google Scholar] [CrossRef] [Green Version]
- Liu, L.; Dehner, C.; Grandhi, N.; Lyu, Y.; Borcherding, D.C.; Chrisinger, J.S.A.; Zhang, X.; Luo, J.; Tao, Y.; Parkes, A.; et al. The Impact of TSC-1 and -2 Mutations on Response to Therapy in Malignant PEComa: A Multicenter Retrospective Analysis. Genes 2022, 13, 1932. [Google Scholar] [CrossRef]
- Hoven-Gondrie, M.L.; Bastiaannet, E.; Ho, V.K.; van Leeuwen, B.L.; Liefers, G.-J.; Hoekstra, H.J.; Suurmeijer, A.J.H. Worse Survival in Elderly Patients with Extremity Soft-Tissue Sarcoma. Ann. Surg. Oncol. 2016, 23, 2577–2585. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lyu, H.G.; Haider, A.H.; Landman, A.B.; Raut, C.P. The opportunities and shortcomings of using big data and national databases for sarcoma research. Cancer 2019, 125, 2926–2934. [Google Scholar] [CrossRef]
- Judson, I.; Verweij, J.; Gelderblom, H.; Hartmann, J.T.; Schöffski, P.; Blay, J.-Y.; Kerst, J.M.; Sufliarsky, J.; Whelan, J.; Hohenberger, P.; et al. Doxorubicin alone versus intensified doxorubicin plus ifosfamide for first-line treatment of advanced or metastatic soft-tissue sarcoma: A randomised controlled phase 3 trial. Lancet Oncol. 2014, 15, 415–423. [Google Scholar] [CrossRef] [PubMed]
- von Mehren, M.; Kane, J.M.; Agulnik, M.; Bui, M.M.; Carr-Ascher, J.; Choy, E.; Connelly, M.; Dry, S.; Ganjoo, K.N.; Gonzalez, R.J.; et al. Soft Tissue Sarcoma, Version 2.2022, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2022, 20, 815–833. [Google Scholar] [CrossRef]
- Savina, M.; Le Cesne, A.; Blay, J.-Y.; Ray-Coquard, I.; Mir, O.; Toulmonde, M.; Cousin, S.; Terrier, P.; Ranchere-Vince, D.; Meeus, P.; et al. Patterns of care and outcomes of patients with METAstatic soft tissue SARComa in a real-life setting: The METASARC observational study. BMC Med. 2017, 15, 78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saerens, M.; Brusselaers, N.; Rottey, S.; Decruyenaere, A.; Creytens, D.; Lapeire, L. Immune checkpoint inhibitors in treatment of soft-tissue sarcoma: A systematic review and meta-analysis. Eur. J. Cancer 2021, 152, 165–182. [Google Scholar] [CrossRef] [PubMed]
- Grünwald, V.; Karch, A.; Schuler, M.; Schöffski, P.; Kopp, H.-G.; Bauer, S.; Kasper, B.; Lindner, L.H.; Chemnitz, J.-M.; Crysandt, M.; et al. Randomized Comparison of Pazopanib and Doxorubicin as First-Line Treatment in Patients with Metastatic Soft Tissue Sarcoma Age 60 Years or Older: Results of a German Intergroup Study. J. Clin. Oncol. 2020, 38, 3555–3564. [Google Scholar] [CrossRef] [PubMed]
- Rytlewski, J.; Milhem, M.M.; Monga, V. Turning ‘Cold’ tumors ‘Hot’: Immunotherapies in sarcoma. Ann. Transl. Med. 2021, 9, 1039. [Google Scholar] [CrossRef]
- Carpenter, W.R.; Fortune-Greeley, A.K.; Zullig, L.L.; Lee, S.-Y.; Weiner, B.J. Sustainability and performance of the National Cancer Institute’s Community Clinical Oncology Program. Contemp. Clin. Trials 2012, 33, 46–54. [Google Scholar] [CrossRef] [Green Version]
- Kim, D.J.; Otap, D.; Ruel, N.; Gupta, N.; Khan, N.; Dorff, T. NCI–Clinical Trial Accrual in a Community Network Affiliated with a Designated Cancer Center. J. Clin. Med. 2020, 9, 1970. [Google Scholar] [CrossRef]
- Mehta, C.R.; Liu, L.; Theuer, C. An adaptive population enrichment phase III trial of TRC105 and pazopanib versus pazopanib alone in patients with advanced angiosarcoma (TAPPAS trial). Ann. Oncol. 2019, 30, 103–108. [Google Scholar] [CrossRef]
- Sturm, E.C.; Marasco, I.S.; Katz, S.C. Multidisciplinary Management of Angiosarcoma—A Review. J. Surg. Res. 2021, 257, 213–220. [Google Scholar] [CrossRef] [PubMed]
- Penel, N.; Bui, B.N.; Bay, J.-O.; Cupissol, D.; Ray-Coquard, I.; Piperno-Neumann, S.; Kerbrat, P.; Fournier, C.; Taieb, S.; Jimenez, M.; et al. Phase II Trial of Weekly Paclitaxel for Unresectable Angiosarcoma: The ANGIOTAX Study. J. Clin. Oncol. 2008, 26, 5269–5274. [Google Scholar] [CrossRef]
- Wilhelm, S.M.; Dumas, J.; Adnane, L.; Lynch, M.; Carter, C.A.; Schütz, G.; Thierauch, K.-H.; Zopf, D. Regorafenib (BAY 73-4506): A new oral multikinase inhibitor of angiogenic, stromal and oncogenic receptor tyrosine kinases with potent preclinical antitumor activity. Int. J. Cancer 2011, 129, 245–255. [Google Scholar] [CrossRef]
- Agulnik, M.; Schulte, B.; Robinson, S.; Hirbe, A.C.; Kozak, K.; Chawla, S.P.; Attia, S.; Rademaker, A.; Zhang, H.; Abbinanti, S.; et al. An open-label single-arm phase II study of regorafenib for the treatment of angiosarcoma. Eur. J. Cancer 2021, 154, 201–208. [Google Scholar] [CrossRef]
- van der Graaf, W.T.; Blay, J.-Y.; Chawla, S.P.; Kim, D.-W.; Bui-Nguyen, B.; Casali, P.G.; Schöffski, P.; Aglietta, M.; Staddon, A.P.; Beppu, Y.; et al. Pazopanib for metastatic soft-tissue sarcoma (PALETTE): A randomised, double-blind, placebo-controlled phase 3 trial. Lancet 2012, 379, 1879–1886. [Google Scholar] [CrossRef] [PubMed]
- Hirbe, A.C.; Eulo, V.; Moon, C.I.; Luo, J.; Myles, S.; Seetharam, M.; Toeniskoetter, J.; Kershner, T.; Haarberg, S.; Agulnik, M.; et al. A phase II study of pazopanib as front-line therapy in patients with non-resectable or metastatic soft-tissue sarcomas who are not candidates for chemotherapy. Eur. J. Cancer 2020, 137, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Agulnik, M.; Costa, R.; Milhem, M.; Rademaker, A.; Prunder, B.; Daniels, D.; Rhodes, B.; Humphreys, C.; Abbinanti, S.; Nye, L.; et al. A phase II study of tivozanib in patients with metastatic and nonresectable soft-tissue sarcomas. Ann. Oncol. 2017, 28, 121–127. [Google Scholar] [CrossRef]
- Chang, E.; Weinstock, C.; Zhang, L.; Fiero, M.H.; Zhao, M.; Zahalka, E.; Ricks, T.K.; Zirkelbach, J.F.; Qiu, J.; Yu, J.; et al. FDA Approval Summary: Tivozanib for Relapsed or Refractory Renal Cell Carcinoma. Clin. Cancer Res. 2022, 28, 441–445. [Google Scholar] [CrossRef] [PubMed]
- Schulte, B.; Mohindra, N.; Milhem, M.; Attia, S.; Robinson, S.; Monga, V.; Hirbe, A.C.; Oppelt, P.; Charlson, J.; Helenowski, I.; et al. Phase II study of pazopanib with oral topotecan in patients with metastatic and non-resectable soft tissue and bone sarcomas. Br. J. Cancer 2021, 125, 528–533. [Google Scholar] [CrossRef] [PubMed]
- (U.S.). NLoM. Abemaciclib for Bone and Soft Tissue Sarcoma with Cyclin-Dependent Kinase (CDK) Pathway Alteration. Identifier NCT04040205 2019. Available online: https://clinicaltrials.gov/ct2/show/NCT04040205 (accessed on 20 November 2022).
- Medicine NLo. Cabozantinib and Temozolomide for the Treatment of Unresectable or Metastatic Leiomyosarcoma or Other Soft Tissue Sarcoma. Identifier NCT04200443. Available online: https://clinicaltrials.gov/ct2/show/NCT04040205 (accessed on 20 November 2022).
- (U.S.). NLoM. A Dose Escalation and Dose Expansion Study of NOX66 Plus Doxorubicin in Anthracycline-naïve, Adult Pa-tients with Soft Tissue Sarcoma. Identifier NCT05100628. Available online: https://clinicaltrials.gov/ct2/show/NCT05100628 (accessed on 20 November 2022).
- Miller, D.; Livingston, J.A.; Park, Y.; Posey, K.; Godbole, S.; Skubitz, K.; Robinson, S.I.; Agulnik, M.; Davis, L.E.; Van Tine, B.A.; et al. Pregnancy outcomes related to the treatment of sarcomas with anthracyclines and/or ifosfamide during pregnancy. Cancer Med. 2022, 11, 3471–3478. [Google Scholar] [CrossRef]
- Monga, V.; Skubitz, K.M.; Maliske, S.; Mott, S.L.; Dietz, H.; Hirbe, A.C.; Van Tine, B.A.; Oppelt, P.; Okuno, S.; Robinson, S.; et al. A Retrospective Analysis of the Efficacy of Immunotherapy in Metastatic Soft-Tissue Sarcomas. Cancers 2020, 12, 1873. [Google Scholar] [CrossRef]
- Rajasekaran, R.B.; Whitwell, D.; Cosker, T.D.A.; Gibbons, C.L.M.H.; Carr, A. Will virtual multidisciplinary team meetings become the norm for musculoskeletal oncology care following the COVID-19 pandemic?—Experience from a tertiary sarcoma centre. BMC Musculoskelet. Disord. 2021, 22, 18. [Google Scholar] [CrossRef]
- Pan, M.; Yu, J.; Sidhu, M.; Seto, T.; Fang, A. Impact of a Virtual Multidisciplinary Sarcoma Case Conference on Treatment Plan and Survival in a Large Integrated Healthcare System. JCO Oncol. Pract. 2021, 17, e1711–e1718. [Google Scholar] [CrossRef]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Heater, N.K.; Okuno, S.; Robinson, S.; Attia, S.; Seetharam, M.; Siontis, B.L.; Yoon, J.; Chawla, S.; Milhem, M.M.; Monga, V.; et al. The Midwest Sarcoma Trials Partnership: Bridging Academic and Community Networks in a Collaborative Approach to Sarcoma. J. Clin. Med. 2023, 12, 2561. https://doi.org/10.3390/jcm12072561
Heater NK, Okuno S, Robinson S, Attia S, Seetharam M, Siontis BL, Yoon J, Chawla S, Milhem MM, Monga V, et al. The Midwest Sarcoma Trials Partnership: Bridging Academic and Community Networks in a Collaborative Approach to Sarcoma. Journal of Clinical Medicine. 2023; 12(7):2561. https://doi.org/10.3390/jcm12072561
Chicago/Turabian StyleHeater, Natalie K., Scott Okuno, Steven Robinson, Steven Attia, Mahesh Seetharam, Brittany L. Siontis, Janet Yoon, Sant Chawla, Mohammed M. Milhem, Varun Monga, and et al. 2023. "The Midwest Sarcoma Trials Partnership: Bridging Academic and Community Networks in a Collaborative Approach to Sarcoma" Journal of Clinical Medicine 12, no. 7: 2561. https://doi.org/10.3390/jcm12072561