1. Introduction
Spine infection is an infectious disease which can be developed by pyogenic, tuberculous, or brucellar causes, with pyogenic origin being the most common cause. The incidence of pyogenic spine infection (PSI) is increasing due to an aging population with degenerative spine diseases, chronic immune-compromising diseases, frequent spine procedures, and diagnostic advancement [
1,
2]. The annual incidence of hospitalization with PSI in the United States between 1998 and 2013 rose from 2.9 to 5.4 per 100,000 individuals [
3]. Among the causes of PSI, spine procedures such as spine surgery, epidural injection, nerve root block, or discography are arising as the primary routes of PSI through hematogenous spread or direct inoculation of virulent organisms with an increasing prevalence of degenerative spine diseases [
4].
There is still no clear guidance regarding the duration and administration route for antibiotics in the treatment of PSI. Generally, an extended course of parenteral antibiotics followed by a maintenance course of oral antibiotics is recommended [
5,
6,
7]. However, guidelines for treating PSI remain ambiguous due to variability in treatment duration and regional antibiotic resistance [
8,
9]. Furthermore, the destruction of spinal joints, such as the intervertebral disc and endplates, progressed by infection causes sustained back pain and disability even after the discontinuation of antibiotic treatment. Quality of life and the ability to return to work were significantly decreased in the patients with PSI regardless of treatment modality [
10,
11,
12].
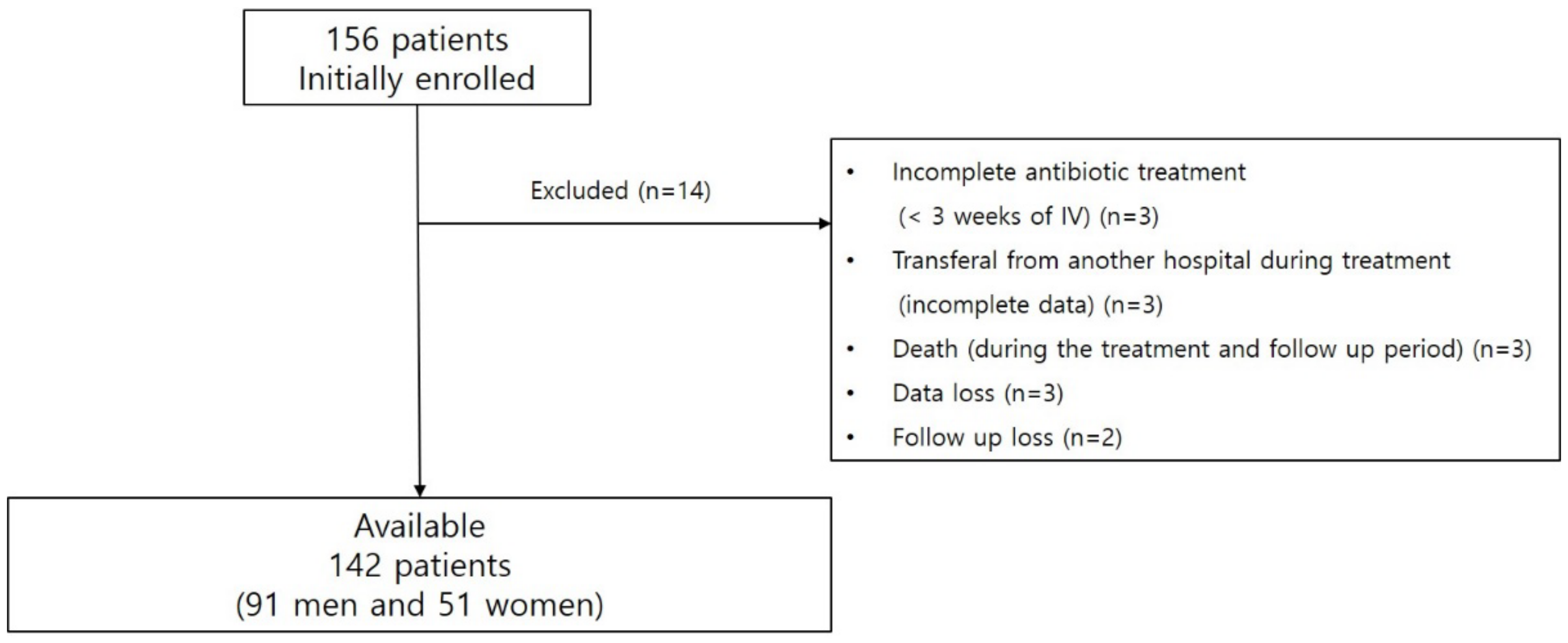
To the best of our knowledge, there are no sufficient data analyzing medical burden and functional status related with PSI. Treatment guidelines are also lacking, as mentioned above. In this study, we investigated the clinical factors associated with the length/cost of hospitalization for the medical burden and initial/6-month short form 36 (SF-36) for the functional status in the treatment of PSI, respectively.
4. Discussion
In this study, we analyzed the clinical factors associated with the medical burden and functional ability of PSI. Elevation of initial blood inflammatory markers (WBC and CRP), presence of weakness, wide extent of the PSI lesion, combined epidural or back muscle abscess, identification of the causative bacteria, and the presence of bacteremia were statistically significant factors associated with increasing both the medical burden and functional disability. In the literature, old age and more comorbidities are associated with higher mortality rates, more adverse events, and prolonged hospitalization in the treatment of PSI [
10,
21]. Contrary to the common expectation, age and comorbidity showed no statistical significance in the medical burden presented as the length and cost of hospitalization; however, they were one of the major factors related to the initial and 6-month functional disability in this study. Our data suggest that functional disability is related to functional ability before PSI, which is correlative with age, comorbidity, and degenerative spinal problems presented as radiculopathy. Based on these results, we expect that the medical burden and functional disability mainly depend on the severity of infectious status and involvement of PSI lesion. ESR and CRP levels correlate with the presence of an inflammatory response; higher ESR and CRP may be more likely to occur in more infectious conditions [
22]. In this study, ESR was a significant factor that increased medical burden such as WBC and CRP, but was not related to function disability. In particular, identification of the causative bacteria and bacteremia were associated with increased medical burden and functional disability than otherwise, which may be associated with increased blood inflammatory markers, extent of the lesion, and presence of abscess. A previous study in Korea showed that a spinal epidural abscess with bacteremia required a longer duration (>8 weeks) of antibiotic treatment [
23].
Previous studies have presented guidelines for the treatment of PSI. However, there are still no definite guidelines for the use of antibiotics due to the differences in the causative pathogen, antibiotic resistance rate, and variations in regional medical systems. The guideline of Infectious Diseases Society of America suggests the use of parenteral antibiotics or oral antibiotics with a high bioavailability for more than six weeks. Although some authors in regions with a low incidence of antibiotic resistance recommend changing to oral antibiotics after relatively short-term parenteral antibiotics less than two weeks, this recommendation should be cautiously applied in regions with a high rate of antibiotic resistance. In Korea, the commonly isolated bacteria of PSI are
Staphylococcus aureus (58.8%),
Streptococcus species (11.3%),
Escherichia coli (11.0%), and the incidence of methicillin-resistant
Staphylococcus aureus is noted as 43.3% [
24]. Additionally, there is a high incidence of antibiotic resistance of
Staphylococcus to methicillin (80%), K. pneumoniae to ceftazidime (25~35%) and quinolone (30%), and
Pseudomonas aeruginosa to ceftazidime (21%) and imipenem (17%) in nosocomial infection [
25,
26,
27]. Consequently, the final effective antibiotics are usually focused on methicillin-resistant
Staphylococcus aureus and multi-drug resistant gram-negative pathogens in patients with a high risk or a poor response for the initial empirical antibiotics regardless of the identification of the causative pathogen, which can result in the long-term use of parenteral antibiotics and hospitalization for PSI in Korea.
The medical burden depends on the length and cost of hospitalization. The cost of hospitalization consists of expenses involved in the room charge, prescription, examination, and nursing mainly incurred during the peri-antibiotic therapy period. Generally, after four weeks of hospitalization with antibiotic therapy, overall conditions such as back pain and fever improve [
28]. Considering that the main cause of hospitalization is for the administration of parenteral antibiotics due to a higher rate of antibiotic resistance, it is required to consider using oral antibiotics with high bioavailability in order to decrease medical burden and use medical resources efficiently. Several studies suggest that switching antibiotic therapy from parenteral to oral administration for patients with PSI has several advantages, including reduced length of hospitalization. Li et al. [
29] reported in their open-labeled randomized trial reported that oral antibiotics might be non-inferior to parenteral therapy for complex orthopedic infection. Flury et al. [
30] reported that switching oral antibiotics after two weeks of parenteral antibiotics may be safe for primary bacterial vertebral osteomyelitis. However, these studies are limited by the fact that their analyses did not perform any sub-group analysis depending on the pathogens and their antimicrobial susceptibility. The risk of newly increased antibiotic resistance rate means that the wide use of high bioavailable oral antibiotics should be considered.
In our results, recurrence (7.7%, 11/142) was identified as a significant factor for increasing medical burden, unlike functional disability. The recurrence rates in the previous studies vary widely. One study in the US showed a recurrence rate of approximately 14% (35/253) in which 90% of them received more than four weeks of antibiotic therapy [
31]. In another study in Korea, there was 9.9% (31/319) of recurrence after 49 days of parenteral antibiotics therapy for hematogenous vertebral osteomyelitis [
24]. According to a recent study in Denmark, the recurrence rate was 13% (12/93) after 87 days of treatment with a mean of 34 days of parenteral and 52 days of oral antibiotic therapy [
32]. However, there was no significant difference in recurrence rate between the patients who received less than six weeks of antibiotic therapy (with 20 ± 16 days of parenteral antibiotic therapy) and other patients who underwent more than six weeks (with 35 ± 16 days of parenteral antibiotic therapy) [
33]. Unfortunately, there is still no definite method to evaluate and achieve an accurate therapeutic response to avoid recurrence. Although the CRP is still considered as the most useful and widely used method for evaluating therapeutic response, it has low specificity and vulnerability to other general conditions [
34,
35]. Accurate determination of therapeutic response with low recurrence is an important issue for the improvement of the overall prognosis of PSI, which is associated with medical burden. Recently, positron emission tomography was introduced as a new modality to evaluate therapeutic response in PSI, and further studies are needed to apply this as real-world evidence in terms of value of evaluating therapeutic response and cost-effectiveness [
14,
36].
There are several limitations in our study. First, PSI is being treated in various settings such as a department of infectious medicine, orthopedics, and spinal neurosurgery. The participants in this study were patients with PSI treated in a spinal neurosurgery department. The relatively low recurrence (7.7%, 11/142) and death rates (1.9%, 3/156) could be attributed to our participants having relatively better general conditions compared to those who are treated in infectious medicine departments. However, the mean CCI of the participants of this study was 3.07 ± 1.77, which is higher than the mean CCI (2.42 ± 2.12 for a group without recurrence, 2.28 ± 2.22 for a group with recurrence) in a nationwide cohort study of 2148 patients [
37]. We presume that long-term parenteral antibiotic therapy for PSI is appropriate for low rates of recurrence and death in regions with a higher antibiotic resistance. Moreover, our cohort only included non-postoperatively developed PSI, which may also result in the low recurrence and death rate. Second, this is a single center study including a relatively small population under a retrospective study design. However, a nationwide cohort study including 7305 pyogenic vertebral osteomyelitis patients in Korea reported individual medical costs of
$10,049 ± 94 in 2007, and
$16,672 ± 17,729 in 2016 [
38]. Our study data show
$14,070.17 ± 9289.39, which is a similar figure considering the gap in which the participants were enrolled. Furthermore, our study also presented the clinical factors associated with the medical burden and functional disability of PSI, which can be clinically useful data in the real world. Third, the study population does not include post-operative PSI; therefore, the results do not represent all types of PSIs. Interestingly, there was no significant difference in the medical burden and functional disability between spontaneous and procedure-related (non-surgical) PSI groups in the
t-test. However, the procedure-related factor showed statistical significance for the length of hospitalization in the multivariable analysis (OR 2.702). Some studies reported that lumbar epidural injection is considered to be a safe procedure and only 0.001–0.1% of spine infections caused by it require hospitalization [
39,
40,
41]. However, little is known about the epidemiology of the difference in severity, recurrence rate, and functional outcome between spontaneous and procedure-related PSIs.





{kind=link}