
Seattle Protocol Is More Effective in Detection of Dysplasia Compared to Technology-Assisted Targeted Biopsies in Patients with Barrett’s Esophagus

Abstract
:1. Introduction
2. Methods
2.1. Patient’s Assessment and Endoscopic Evaluation
2.2. Statistical Analysis
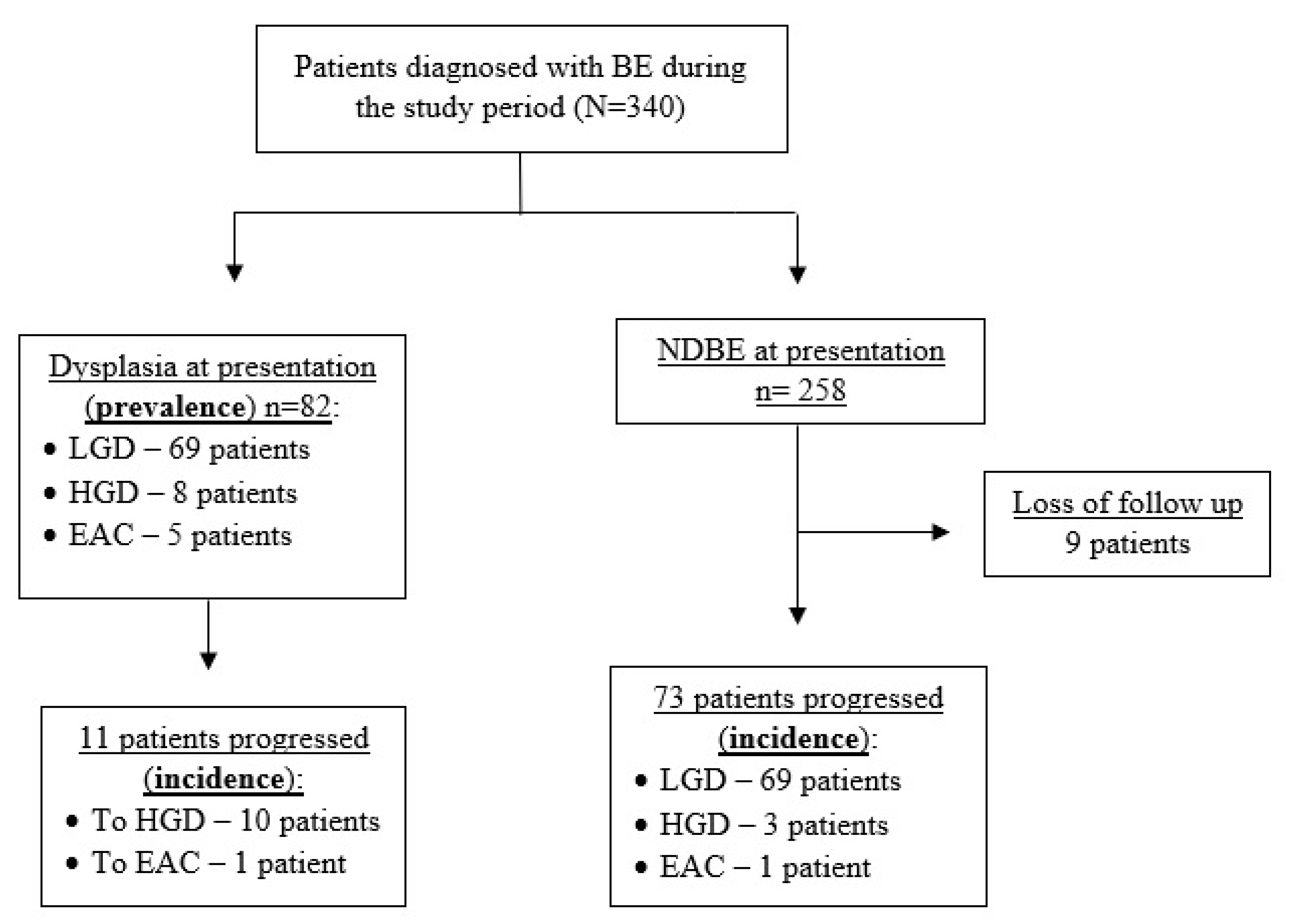
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chen, C.-L.; Liang, S.-W.; Wong, M.-W.; Yi, C.-H.; Liu, T.-T.; Lei, W.-Y.; Hung, J.-S.; Lin, L.; Rogers, B. Current advances in the diagnosis and management of gastroesophageal reflux disease. Tzu Chi Med. J. 2022, 34, 402. [Google Scholar] [CrossRef]
- El-Serag, H.B.; Sweet, S.; Winchester, C.C.; Dent, J. Update on the epidemiology of gastro-oesophageal reflux disease: A systematic review. Gut 2013, 63, 871–880. [Google Scholar] [CrossRef] [Green Version]
- Dirac, M.A.; Safiri, S.; Tsoi, D.; Adedoyin, R.A.; Afshin, A.; Akhlaghi, N.; Alahdab, F.; Almulhim, A.M.; Amini, S.; Ausloos, F.; et al. The global, regional, and national burden of gastro-oesophageal reflux disease in 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet Gastroenterol. Hepatol. 2020, 5, 561–581. [Google Scholar] [CrossRef] [Green Version]
- Falk, G.W. Reflux Disease and Barrett’s Esophagus. Endoscopy 1999, 31, 9–16. [Google Scholar] [CrossRef]
- Bennett, C.; Moayyedi, P.; Corley, D.A.; de Caestecker, J.; Falck-Ytter, Y.; Falk, G.; Vakil, N.; Sanders, S.; Vieth, M.; Inadomi, J.; et al. BOB CAT: A Large-Scale Review and Delphi Consensus for Management of Barrett’s Esophagus with No Dysplasia, Indefinite for, or Low-Grade Dysplasia. Am. J. Gastroenterol. 2015, 110, 662–682. [Google Scholar] [CrossRef] [Green Version]
- Ferlay, J.; Soerjomataram, I.; Dikshit, R.; Eser, S.; Mathers, C.; Rebelo, M.; Parkin, D.M.; Forman, D.; Bray, F. Cancer incidence and mortality worldwide: Sources, methods and major patterns in GLOBOCAN 2012. Int. J. Cancer 2015, 136, 29. [Google Scholar] [CrossRef]
- Desai, T.K.; Krishnan, K.; Samala, N.; Singh, J.; Cluley, J.; Perla, S.; Howden, C.W. The incidence of oesophageal adenocarcinoma in non-dysplastic Barrett’s oesophagus: A meta-analysis. Gut 2011, 61, 970–976. [Google Scholar] [CrossRef]
- Duits, L.C.; Phoa, K.N.; Curvers, W.L.; Kate, F.J.W.T.; Meijer, G.A.; Seldenrijk, C.A.; Offerhaus, G.J.; Visser, M.; Meijer, S.L.; Krishnadath, K.K.; et al. Barrett’s oesophagus patients with low-grade dysplasia can be accurately risk-stratified after histological review by an expert pathology panel. Gut 2014, 64, 700–706. [Google Scholar] [CrossRef] [Green Version]
- Hvid-Jensen, F.; Pedersen, L.; Drewes, A.M.; Sørensen, H.T.; Funch-Jensen, P. Incidence of Adenocarcinoma among Patients with Barrett’s Esophagus. Available online: https://www.nejm.org/doi/10.1056/NEJMoa1103042 (accessed on 10 February 2022).
- Sato, F.; Jin, Z.; Schulmann, K.; Wang, J.; Greenwald, B.D.; Ito, T.; Kan, T.; Hamilton, J.P.; Yang, J.; Paun, B.; et al. Three-Tiered Risk Stratification Model to Predict Progression in Barrett’s Esophagus Using Epigenetic and Clinical Features. PLoS ONE 2008, 3, e1890. [Google Scholar] [CrossRef] [Green Version]
- Codipilly, D.C.; Chandar, A.K.; Singh, S.; Wani, S.; Shaheen, N.J.; Inadomi, J.M.; Chak, A.; Iyer, P.G. The Effect of Endoscopic Surveillance in Patients with Barrett’s Esophagus: A Systematic Review and Meta-analysis. Gastroenterology 2018, 154, 2068–2086.e5. [Google Scholar] [CrossRef] [Green Version]
- Huang, J.; Koulaouzidis, A.; Marlicz, W.; Lok, V.; Chu, C.; Ngai, C.; Zhang, L.; Chen, P.; Wang, S.; Yuan, J.; et al. Global Burden, Risk Factors, and Trends of Esophageal Cancer: An Analysis of Cancer Registries from 48 Countries. Cancers 2021, 13, 141. [Google Scholar] [CrossRef] [PubMed]
- Shaheen, N.J.; Falk, G.W.; Iyer, P.G.; Souza, R.F.; Yadlapati, R.H.; Sauer, B.G.; Wani, S. Diagnosis and Management of Barrett’s Esophagus: An Updated ACG Guideline. Am. J. Gastroenterol. 2022, 117, 559–587. [Google Scholar] [CrossRef] [PubMed]
- McClave, S.A.; DiBaise, J.K.; Mullin, G.; Martindale, R.G. ACG Clinical Guideline: Nutrition Therapy in the Adult Hospitalized Patient. Am. J. Gastroenterol. 2016, 111, 315–334. [Google Scholar] [CrossRef]
- Abrams, J.A.; Kapel, R.C.; Lindberg, G.M.; Saboorian, M.H.; Genta, R.M.; Neugut, A.I.; Lightdale, C.J. Adherence to Biopsy Guidelines for Barrett’s Esophagus Surveillance in the Community Setting in the United States. Clin. Gastroenterol. Hepatol. 2009, 7, 736–742. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vithayathil, M.; Modolell, I.; Ortiz-Fernández-Sordo’, J.; Pappas, A.; Januszewicz, W.; O’Donovan, M.; Bianchi, M.; White, J.R.; Kaye, P.; Ragunath, K.; et al. The effect of procedural time on dysplasia detection rate during endoscopic surveillance of Barrett’s esophagus. Endoscopy 2023. [Google Scholar] [CrossRef] [PubMed]
- Westerveld, D.; Khullar, V.; Mramba, L.; Ayoub, F.; Brar, T.; Agarwal, M.; Forde, J.; Chakraborty, J.; Riverso, M.; Perbtani, Y.B.; et al. Adherence to quality indicators and surveillance guidelines in the management of Barrett’s esophagus: A retrospective analysis. Endosc. Int. Open 2018, 6, E300–E307. [Google Scholar] [CrossRef] [Green Version]
- Vázquez-Iglesias, J.L.; Alonso-Aguirre, P.; Diz-Lois, M.T.; Vázquez-Millán, M.A.; Alvarez, A.; Lorenzo, M.J. Acetic acid allows effective selection of areas for obtaining biopsy samples in Barrett??s esophagus. Eur. J. Gastroenterol. Hepatol. 2007, 19, 187–193. [Google Scholar] [CrossRef]
- Beg, S.; Mensa, M.; Fullard, M.; Finerty, E.; Richman, P.; Leahy, A. Impact of advanced endoscopic imaging on Barrett’s esophagus in daily clinical practice. Gastrointest. Endosc. 2018, 87, 1189–1194. [Google Scholar] [CrossRef]
- ASGE Technology Committee; Thosani, N.; Abu Dayyeh, B.K.; Sharma, P.; Aslanian, H.R.; Enestvedt, B.K.; Komanduri, S.; Manfredi, M.; Navaneethan, U.; Maple, J.T.; et al. ASGE Technology Committee systematic review and meta-analysis assessing the ASGE Preservation and Incorporation of Valuable Endoscopic Innovations thresholds for adopting real-time imaging–assisted endoscopic targeted biopsy during endoscopic surveillance of Barrett’s esophagus. Gastrointest. Endosc. 2016, 83, 684–698.e7. [Google Scholar] [CrossRef] [Green Version]
- Muthusamy, V.R.; Wani, S.; Gyawali, C.P.; Komanduri, S.; Bergman, J.; Canto, M.I.; Chak, A.; Corley, D.; Falk, G.W.; Fitzgerald, R.; et al. AGA Clinical Practice Update on New Technology and Innovation for Surveillance and Screening in Barrett’s Esophagus: Expert Review. Clin. Gastroenterol. Hepatol. 2022, 20, 2696–2706.e1. [Google Scholar] [CrossRef]
- Weusten, B.; Bisschops, R.; Coron, E.; Dinis-Ribeiro, M.; Dumonceau, J.-M.; Esteban, J.-M.; Hassan, C.; Pech, O.; Repici, A.; Bergman, J.; et al. Endoscopic management of Barrett’s esophagus: European Society of Gastrointestinal Endoscopy (ESGE) Position Statement. Endoscopy 2017, 49, 191–198. [Google Scholar] [CrossRef] [Green Version]
- Nachiappan, A.; Ragunath, K.; Card, T.; Kaye, P. Diagnosing dysplasia in Barrett’s oesophagus still requires Seattle protocol biopsy in the era of modern video endoscopy: Results from a tertiary centre Barrett’s dysplasia database. Scand. J. Gastroenterol. 2019, 55, 9–13. [Google Scholar] [CrossRef] [PubMed]
- Sharma, P.; Bergman, J.J.; Goda, K.; Kato, M.; Messmann, H.; Alsop, B.R.; Gupta, N.; Vennalaganti, P.; Hall, M.; Konda, V.; et al. Development and Validation of a Classification System to Identify High-Grade Dysplasia and Esophageal Adenocarcinoma in Barrett’s Esophagus Using Narrow-Band Imaging. Gastroenterology 2016, 150, 591–598. [Google Scholar] [CrossRef] [PubMed]
- Ikenoyama, Y.; Tanaka, K.; Umeda, Y.; Hamada, Y.; Yukimoto, H.; Yamada, R.; Tsuboi, J.; Nakamura, M.; Katsurahara, M.; Horiki, N.; et al. Effect of adding acetic acid when performing magnifying endoscopy with narrow band imaging for diagnosis of Barrett’s esophageal adenocarcinoma. Endosc. Int. Open 2022, 10, E1528–E1536. [Google Scholar] [CrossRef]
- Wolfsen, H.C.; Crook, J.E.; Krishna, M.; Achem, S.R.; Devault, K.R.; Bouras, E.P.; Loeb, D.S.; Stark, M.E.; Woodward, T.A.; Hemminger, L.L.; et al. Prospective, Controlled Tandem Endoscopy Study of Narrow Band Imaging for Dysplasia Detection in Barrett’s Esophagus. Gastroenterology 2008, 135, 24–31. [Google Scholar] [CrossRef]
- Pascarenco, O.D.; Coroş, M.F.; Pascarenco, G.; Boeriu, A.M.; Draşovean, S.C.; Onişor, D.M.; Brusnic, O.; Dobru, D. A preliminary feasibility study: Narrow-band imaging targeted versus standard white light endoscopy non-targeted biopsies in a surveillance Barrett’s population. Dig. Liver Dis. 2016, 48, 1048–1053. [Google Scholar] [CrossRef] [PubMed]
- Hajelssedig, O.E.; Pu, L.Z.C.T.; Thompson, J.Y.; Lord, A.; El Sayed, I.; Meyer, C.; Ali, F.S.; Abdulazeem, H.M.; O Kheir, A.; Siepmann, T.; et al. Diagnostic accuracy of narrow-band imaging endoscopy with targeted biopsies compared with standard endoscopy with random biopsies in patients with Barrett’s esophagus: A systematic review and meta-analysis. J. Gastroenterol. Hepatol. 2021, 36, 2659–2671. [Google Scholar] [CrossRef] [PubMed]
- Parasa, S.; Vennalaganti, S.; Gaddam, S.; Vennalaganti, P.; Young, P.; Gupta, N.; Thota, P.; Cash, B.; Mathur, S.; Sampliner, R.; et al. Development and Validation of a Model to Determine Risk of Progression of Barrett’s Esophagus to Neoplasia. Gastroenterology 2018, 154, 1282–1289.e2. [Google Scholar] [CrossRef]
- Bhat, S.; Coleman, H.G.; Yousef, F.; Johnston, B.T.; McManus, D.T.; Gavin, A.T.; Murray, L.J. Risk of Malignant Progression in Barrett’s Esophagus Patients: Results from a Large Population-Based Study. Gynecol. Oncol. 2011, 103, 1049–1057. [Google Scholar] [CrossRef] [Green Version]
- Elsheaita, A.; El-Bially, M.A.; Shamseya, M.M.; Ahmed, S.S.; Madkour, M.A.; Shamseya, A.M.; Nouh, H.H. Seattle protocol vs narrow band imaging guided biopsy in screening of Barrett’s esophagus in gastroesophageal reflux disease patients. Medicine 2020, 99, e19261. [Google Scholar] [CrossRef]
- Furneri, G.; Klausnitzer, R.; Haycock, L.; Ihara, Z. Economic value of narrow-band imaging versus white light endoscopy for the diagnosis and surveillance of Barrett’s esophagus: Cost-consequence model. PLoS ONE 2019, 14, e0212916. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nantes University Hospital High Resolution Virtual Chromoendoscopy Versus Seattle Protocol for the Surveillance of Barrett’s Esophagus: Impact on the Detection of High-Grade Dysplasia and Adenocarcinoma Lesions. 2022. Available online: clinicaltrials.gov (accessed on 16 March 2023).
- Xiong, Y.-Q.; Ma, S.-J.; Zhou, J.-H.; Zhong, X.-S.; Chen, Q. A meta-analysis of confocal laser endomicroscopy for the detection of neoplasia in patients with Barrett’s esophagus. J. Gastroenterol. Hepatol. 2016, 31, 1102–1110. [Google Scholar] [CrossRef]
- de Groof, A.J.; Swager, A.-F.; Pouw, R.; Weusten, B.L.; Schoon, E.J.; Bisschops, R.; Pech, O.; Meining, A.; Neuhaus, H.; Curvers, W.L.; et al. Blue-light imaging has an additional value to white-light endoscopy in visualization of early Barrett’s neoplasia: An international multicenter cohort study. Gastrointest. Endosc. 2018, 89, 749–758. [Google Scholar] [CrossRef] [PubMed]
- de Groof, A.J.; Struyvenberg, M.R.; van der Putten, J.; van der Sommen, F.; Fockens, K.N.; Curvers, W.L.; Zinger, S.; Pouw, R.; Coron, E.; Baldaque-Silva, F.; et al. Deep-Learning System Detects Neoplasia in Patients with Barrett’s Esophagus With Higher Accuracy Than Endoscopists in a Multistep Training and Validation Study With Benchmarking. Gastroenterology 2020, 158, 915–929.e4. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Clinical Parameters | |
|---|---|
| Age at diagnosis (years) | 64.0 (58.0–69.0) |
| Gender—male | 123 (79.30) |
| BMI | 28.9 (26.9–31.8) |
| GERD at baseline | 101 (65.16) |
| Family history of BE or EAC | 6 (3.87) |
| Ever smoke | 82 (52.90) |
| Alcohol use | 9 (5.81) |
| PPI type | |
| Omeprazole | 49 (31.61) |
| Lansoprazole | 31 (20.00) |
| Esomeprazole | 65 (41.93) |
| Lansoprazole | 10 (6.45) |
| Endoscopic and histologic parameters | |
| BE length | |
| C (cm) | 1.0 (0.0–2.0) |
| M (cm) | 2.0 (1.0–3.0) |
| Long segment BE | 55 (35.48) |
| Hiatal hernia | 77 (49.67) |
| Hiatal hernia size (cm) | 3.0 (3.0–4.0) |
| NDBE | 70 (45.16) |
| Indefinite for dysplasia | 3 (1.93) |
| LGD | 69 (44.51) |
| HGD | 8 (5.16) |
| EAC | 5 (3.22) |
| Number of surveillance endoscopies during follow-up | 3.0 (2.0–4.0) |
| Seattle Protocol | Targeted Biopsy | ||||
|---|---|---|---|---|---|
| HD-WL | NBI | Total | |||
| LGD, N (%) | 63 (91.3) | 1 (16.6) | 5 (83.3) | 6 (8.7) | |
| HGD, N (%) | 4 (50.0) | 3 (75.0) | 1 (25.0) | 4 (50.0) | |
| EAC, N (%) | 0 (0.0) | 3 (60.0) | 2 (40.0) | 5 (100.0) | |
| Total events, N (%) | 67 (81.7) | 7 (46.6) | 8 (53.3) | 15 (18.3) | |
| Seattle Protocol | Targeted Biopsy | ||||
|---|---|---|---|---|---|
| HD-WL | NBI | Total | |||
| LGD, N (%) | 57 (82.6) | 3 (25.0) | 9 (75.0) | 12 (17.4) | |
| HGD, N (%) | 8 (61.5) | 3 (60.0) | 2 (40.0) | 5 (38.5) | |
| EAC, N (%) | 0 (0.0) | 0 (0.0) | 2 (100.0) | 2 (100.0) | |
| Total events, N (%) | 65 (77.4) | 6 (31.6) | 13 (68.4) | 19 (22.6) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Peleg, N.; Ollech, J.E.; Shamah, S.; Sapoznikov, B. Seattle Protocol Is More Effective in Detection of Dysplasia Compared to Technology-Assisted Targeted Biopsies in Patients with Barrett’s Esophagus. J. Clin. Med. 2023, 12, 2544. https://doi.org/10.3390/jcm12072544
Peleg N, Ollech JE, Shamah S, Sapoznikov B. Seattle Protocol Is More Effective in Detection of Dysplasia Compared to Technology-Assisted Targeted Biopsies in Patients with Barrett’s Esophagus. Journal of Clinical Medicine. 2023; 12(7):2544. https://doi.org/10.3390/jcm12072544
Chicago/Turabian StylePeleg, Noam, Jacob E. Ollech, Steven Shamah, and Boris Sapoznikov. 2023. "Seattle Protocol Is More Effective in Detection of Dysplasia Compared to Technology-Assisted Targeted Biopsies in Patients with Barrett’s Esophagus" Journal of Clinical Medicine 12, no. 7: 2544. https://doi.org/10.3390/jcm12072544