
Post-Operative Anorectal Manometry in Children following Anorectal Malformation Repair: A Systematic Review
 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Study Selection
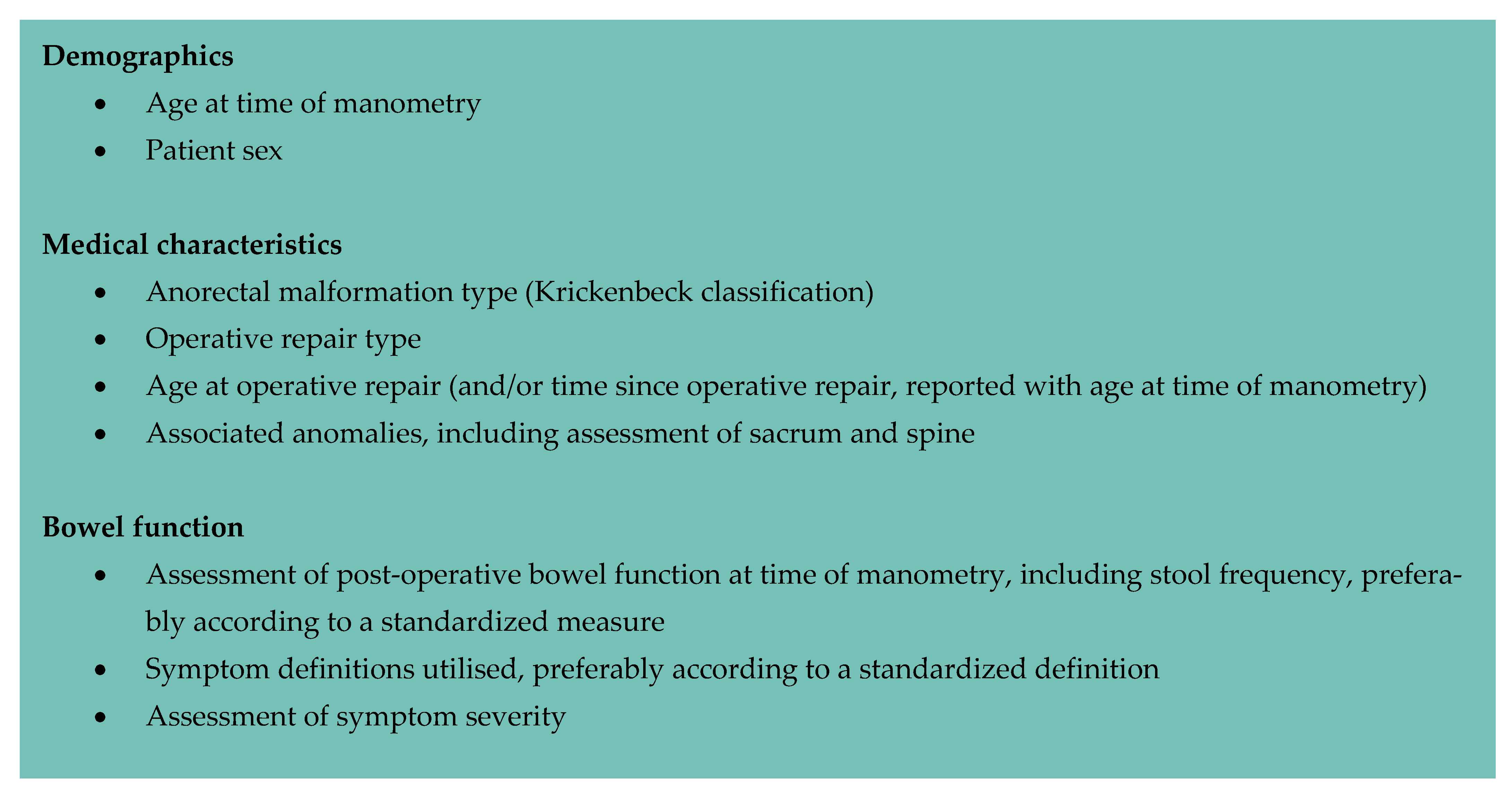
2.2. Data Extraction
2.3. Quality Assessment
3. Results
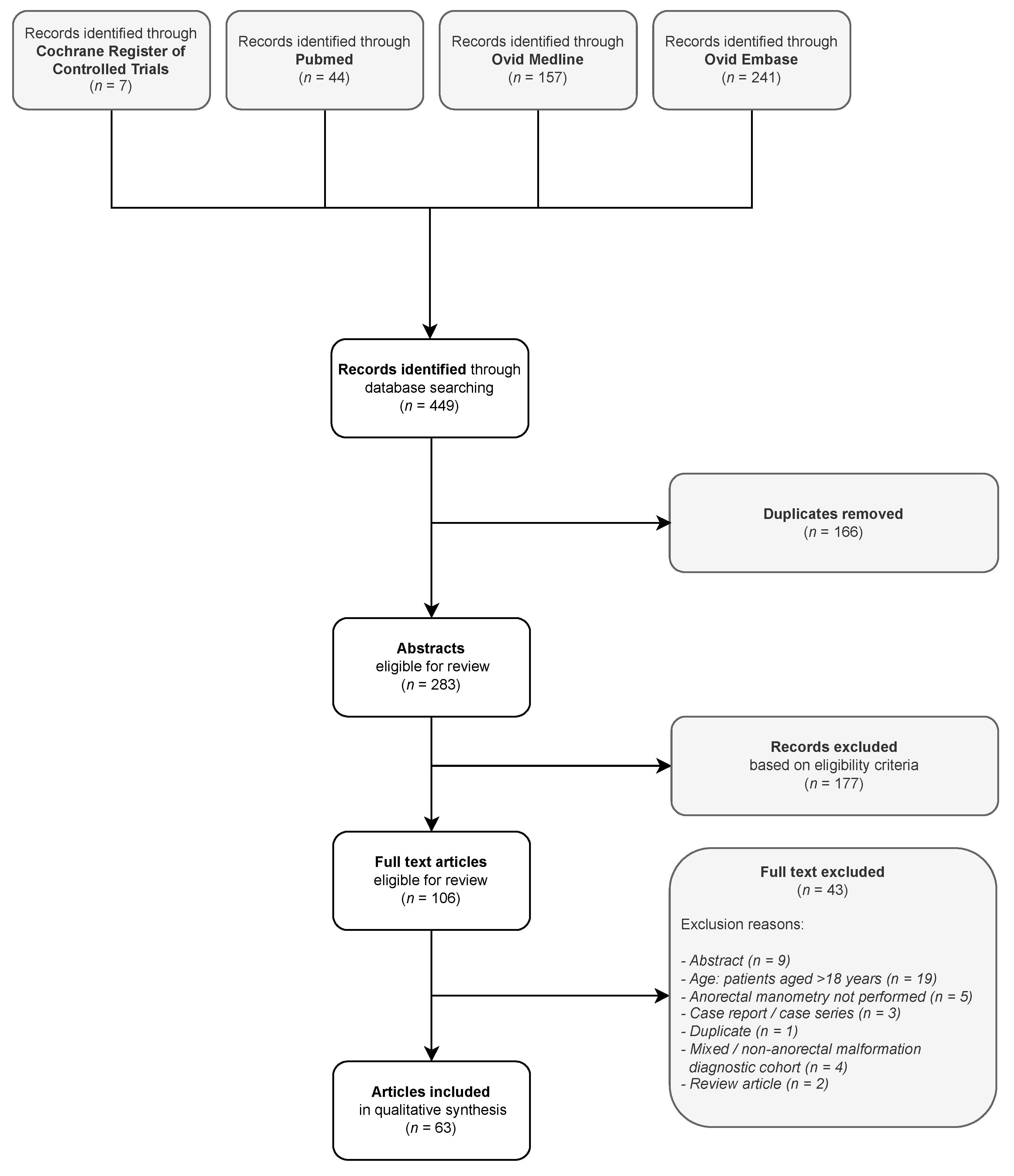
3.1. Search Results
3.2. Quality Assessment

{kind=link}
{kind=link}
| First Author | Year | Cohort (Total (Male)) | Study Population Summary | Age at Time of Manometry | Reported Anorectal Malformation Type 1 | Associated Anomalies | Surgical Repair Type | |
|---|---|---|---|---|---|---|---|---|
| Total 2 | Manometry 3 | |||||||
| Arnoldi [14] | 2014 | 30 (11) | 30 (11) | Toilet-trained children with anorectal malformation with a good, predicted prognosis 4 | Range: 2.5–10 years. Measure of central tendency not provided. Mean follow-up at assessment: 5 years. | Rectoperineal fistula: 19 Rectovestibular fistula: 10 Imperforate anus: 1 | Tethered cord: 6/30 (20%) Excluded: abnormal sacrum. Other anomalies not reported. | Three-stage repair (diverting colostomy, PSARP, colostomy closure): 9 (30%) Primary PSARP: 21/30 (70%) |
| Banasiuk [64] | 2021 | 12 (-) | 12 (-) | Children who had undergone surgery for anorectal disorders, including anal atresia | Median 70 (16–195) months | Perineal fistula (7) Rectourethral fistula (4) Persistent cloaca (1) | Not reported | Not reported |
| Becmeur [23] | 2001 | 14 (9) | 10 (-) | Children following three-flap anoplasty for primary or re-do repair | Not reported. Mean age at study conclusion: 6 years (range 3–14). | High/intermediate: rectobulbar fistula (8); rectovesical fistula (1); cloacal defect (1); long rectal atresia (1). Low: rectovulvar fistula (3). Not specified for manometry cohort | T21 (1); HD (1); psychomotor troubles (2); complex caudal malformation (3); GI duplication (1); ductus arteriosus (1); crossed renal ectopia (1); renal cystic dysplasia (1); hypospadias (1); supernumerary hemivertebra (1). | Three flap anoplasty: 14/14 Primary repair: 9/14 Re-do procedure: 5/14 |
| Bhat [56] | 2008 | 10 (9) | 10 (9) | High or intermediate anorectal malformation, following sigmoid colostomy formation but prior to PSARP | Post-PSARP age: mean 26.3 months (range 15–57). | Rectoprostatic fistula: 6 Rectobulbar fistula: 3 Rectovaginal fistula: 1 | Not reported | PSARP: 10/10 |
| Burjonrappa [61] | 2010 | 86 (53) | 6/14 (4) 5 | Patients with megarectum following surgery for anorectal malformation | Not reported. | High: 23 -developed megarectum: 6 (26%) Low: 63 -developed megarectum: 8 (13%) | Sacral vertebral anomalies: 13/86 | Children with megarectum: Mollard anterior approach: 1 Cutback: 1 Anal transposition: 2 Laparoscopic primary pullthrough: 3 Posterior-sagittal pullthrough: 2 Y-V plasty: 2 Dilatation only: 2 |
| Cahill [24] | 1985 | 6 (6) | 5 (5) | Patients with anorectal malformation following PSARP | Mean: 2.2 years (range 1.25–3.5 years) | Rectoprostatic fistula: 6 | Sacral anomaly: 1 | PSARP: 6/6 |
| Caldaro [43] | 2012 | 17 (13) | 17 (13) | Neurologically healthy children, >4 years, with constipation/FI, following anorectal malformation repair | Mean: 8.3 years (range 5–15 years). | High: rectobladderneck fistula (2); rectourethral fistula (4); cloaca (1). Intermediate: rectourethral fistula (4). Low: rectoperineal fistula (2); rectovestibular fistula (3); anal stenosis (1). | Myelomeningocele: 2 Tethered cord: 1 Renal: 2 VACTERL syndrome: 1 | PSARP: 17/17 |
| Caruso [67] | 2015 | 25 (15) | 25 (15) | Neurologically heathy children >4 years with “true” FI following anorectal malformation repair | Mean: 6.5 years (range 5–9 years). | Vestibular fistula: 3 Rectal atresia: 8 Bulbar fistula: 5 Prostatic fistula: 2 Cloaca: 2 Vaginal fistula: 1 Vesical fistula: 4 | Renal: 12 Genital: 10 Spinal: 5 | PSARP: 25 Laparoscopically assisted proportion not defined. |
| Caruso [72] | 2021 | 14 (-) | 14 (-) | Children with FI or bowel dysfunction not responsive to conventional laxative treatment, receiving transanal irrigation | Mean 10.29 ± 3.25 years | Rectobulbar fistula: 4 Rectovaginal fistula: 2 Rectovesical fistula: 4 Rectoprostatic fistula: 2 Perineal fistula: 2 | Spinal: 6 | Not reported |
| Chen [73] | 1998 | 58 (34) | 44 (-) | All children with anorectal malformation repaired by a single surgeon | Not reported. Manometry was performed within the 1st year of the repair and repeated at 1–2-year intervals. | High/intermediate. Blind pouch (10); fistula: rectobulbar (4); rectoprostatic (7); rectovesical (2); rectovaginal (1); rectovestibular (4); cloacal anomaly (2). Low. Fistula: anocutaneous and anterior perineal anus (16); rectoperineal (4); anovulvar or anovestibular (8). Not specified for manometry cohort | High/intermediate: EA (1); T21 (2); spinal (2); urogenital (5); cardiac (3). Low: EA (1); urogenital anomaly (2); duodenal obstruction (1); cardiac (2). | LSARP: 32 PSARP: 29 R-ASPA: 5 Total surgical cohort (n = 66). Operative details of study (n = 58) and manometry (n = 44) cohorts not provided. |
| Chung [22] | 2018 | 30 (-) | 30 (-) | Toilet-trained children following PSARP or LAARP without neurological comorbidities or cloacal malformation | PSARP: 15.5 years (range 8–32) LAARP: 9 years (range 5–14) | Krickenbeck classification: (PSARP, LAARP) Rectovesical: 2, 3 Rectoprostatic: 7, 8 Rectobulbar: 5, 5 | Not reported | PSARP: 14/30 (46.7%) LAARP: 16/30 (53.3%) |
| Doolin [44] | 1993 | 25 (15) | 25 (15) | Children following repair of anal atresia | Mean: 9.6 years (range 6–16) | Rectourethral fistula: 15 Rectovaginal fistula: 5 Vestibular fistula: 1 Cloaca: 3 Anorectal malformation without fistula: 1 | Not reported | Abdominoperineal pullthrough: 20 Presacral pullthrough: 4 Perineal anoplasty: 1 |
| El-Debeiky [25] | 2009 | 15 (15) | 9 (9) | Males with high anorectal malformation treated with laparoscopic-assisted pull-through | Not reported. Assessed at 3 years of age or older. | Rectobladderneck fistula: 15/15 | Not reported | Laparoscopically assisted pull-through: 15/15 |
| Emblem [40] | 1994 | 16 (8) | 16 (8) | Adolescents with low anorectal malformations following repair | Mean: 14.9 years (12–16) | Anocutaneous fistula: 16 (100%) | Not reported | Anal dilatation: 5 Anal cutback: 11 Secondary procedures: Anal transposition: 3 Posterior anoplasty: 2 |
| Emblem [45] | 1997 | 33 (16) | 33 (16) | Adolescents with anorectal malformations following repair | Intermediate/high: mean 15.8 years (14.6–17.1) Low: mean 14.9 years (13.7–16.2) | High/intermediate: 16 (48%) Low: 17 (52%) | Not reported | Sacroperineal, sacroabdominoperineal, abdominoperineal, perineal procedures according to the malformation type. Cohort distribution not reported. |
| Fukata [41] | 1997 | 15 (14) | 15 (14) | Patients with high or intermediate anorectal malformations | Median: 14 years (8–18) | High: 10 (67%) Intermediate: 5 (33%) | Not reported | Abdominoperineal rectoplasty: 15 (100%) |
| Hedlund [46] | 1992 | 30 (-) | 30 (-) | Patients with anorectal malformations following PSARP, without major sacral malformation | Range: 5–18 years. Measure of central tendency not provided | Bulbar fistula: 9 Prostatic fistula: 8 Vaginal fistula: 1 Vestibular fistula: 6 Rectal atresia: 3 No fistula: 3 | Not reported | PSARP: 30 |
| Heikenen [74] | 1999 | 13 (6) | Colonic manometry: 13 (6) Anorectal manometry: 10 (4) | Children with FI refractory to standard medical therapy following repair of anorectal malformation | Mean 8.6 years (range 5–13) | High: 7/10 Low: 3/10 | Not reported | Not reported |
| Hettiarachchi [47] | 2002 | 15 (5) | 15 (5) | Children with chronic constipation and/or FI following anorectal malformation repair | Median 2.5 years (range 1–15) | High: 6 Intermediate: 5 Low: 4 | Minor sacroneural anomalies: 3 Partial trisomy 22: 2 | “Variety of techniques used for reconstruction” [47]; not further specified. |
| Huang [20] | 2017 | 89 (0) | 43 (0) | Female patients with rectovestibular fistula | Not reported. Age at operation: -Modified semi-PSARP: 1.6 months (9 days–2.5 months) -Transperineal anal transposition: 6.4 (5–8) months Anorectal manometry performed 12 months post-operatively. | Imperforate anus with rectovestibular fistula: 43 | Cardiac: 27 Renal: 10 OA: 2 Polydactyly: 1 Absent coccyx: 1 Sacrococcygeal pilonidal sinus: 1 | One-stage modified semi-PSARP: 39 Transperineal anal transposition: 50 Manometry recipients: 43/89 (48% total cohort) -Modified semi-PSARP: 17 (39%) -Transperineal anal transposition: 26 (61%) |
| Husberg [26] | 1992 | 48 (24) | 43 (-) | Children with high or intermediate anorectal malformation | Range 7 months–16 years | Rectovesical fistula: 1 Rectoprostatic fistula: 15 Rectobulbar fistula: 4 Blind-ending rectum: 5 Cloacal malformation: 11 Rectovaginal fistula: 1 Rectovestibular fistula: 11 Not specified for manometry cohort | Concomitant malformations: 44 | Posterior sagittal approach: 48 |
| Ishihara [48] | 1987 | 49 (-) | 49 (-) | Patients with anorectal malformations following repair | Mean 9.5 years (range 5–20 years 6). | Translevator: 9 Intermediate: 6 Supralevator: 24 Operated at another hospital: 10 | Not reported | Not reported |
| Iwai [15] | 1988 | 28 (-) | 17 (-) | Patients with anorectal malformations following repair | Range: 5–14 years. Measure of central tendency not provided | High: 13 Intermediate: 6 Low: 9 Not specified for manometry cohort | Not reported | Not reported. Department practice -high/intermediate: abdominoperineal rectoplasty -low: perineoplasty |
| Iwai [68] | 1993 | 8 (-) | 8 (-) | Children undergoing biofeedback training for FI following anorectal malformation repair | Range: 6–12 years. Measure of central tendency not provided | High: 6 Intermediate: 2 | Not reported | Abdominoperineal rectoplasty: 7 Abdominosacroperineal rectoplasty: 1 |
| Iwai [65] | 1997 | 14 (-) | 14 (-) | Children undergoing biofeedback training for FI following anorectal malformation repair | Range: 5–14 years. Measure of central tendency not provided | High: 12 Intermediate: 2 | Sacral deformity: 0 | Not reported |
| Iwai [66] | 2007 | 5 (-) | 5 (-) | Children with severe constipation following anorectal malformation repair, treated with herbal medication | Mean: 11.5 years (range 7–17 years) | High: 4 Cloacal anomaly: 1 | Not reported | Not reported |
| Keshtgar [69] | 2007 | 16 (7) | 16 (7) | Children undergoing excision of megarectum for intractable FI | Median: 9 years (range 2–15 years) | High: 6 Intermediate: 4 Low: 6 | EA: 3 Duodenal atresia: 1 Caudal regression with sacral dysgenesis: 1 T21: 1 | Various approaches described for wider population; detail not provided for manometry cohort. |
| Keshtgar [49] | 2008 | 54 (27) | 54 (27) | Children with intractable FI/constipation following anorectal malformation repair | High (n = 34) 7 Median: 10.5 years (range 3.9–21.8) Low (n = 20) Median: 9.4 years (range 4.1–15.3). | Low: anal stenosis and anterior ectopic anus (12); perineal fistula (8). High: rectovestibular fistula (12); rectovesical (2); cloacal malformation (1); rectoprostatic urethral fistula (19). | Megarectum (16); megarectum + neuropathy (11); neuropathy (8); caudal regression (2); sacral dysgenesis (1); esophageal atresia (9); HD (1); T21 (1); T22 (1). | PSARP: 24 Abdominoperineal pullthrough: 8 Stephens: 2 Mollard: 1 Durham Smith: 3 Anal transposition: 7 Anoplasty: 9 |
| Kimura [27] | 2010 | 28 (25) | 28 (25) | Infants managed for high anorectal malformation | Not reported | Rectoprostatic fistula: 21 No fistula: 3 Rectovaginal fistula: 2 Rectovesical fistula: 1 Cloacal malformation: 1 | Not reported | Open ARP: 15 Laparoscopic ARP: 13 |
| Kudou [28] | 2005 | 20 (-) | 20 (-) | Children following LAARP or PSARP for management of high anorectal malformation | LAARP: mean 50.5 months (SD 10 months) PSARP: mean 73 months (SD 12 months). | LAARP: rectourethral fistula (7); rectovesical fistula (2); no fistula (1); rectovaginal fistula (2); cloaca (1). PSARP: rectourethral fistula (2); rectovesical fistula (2); no fistula (1); cloaca (2). | Spinal lipoma: 2 | LAARP: 13 PSARP: 7 |
| Kumar [57] | 2010 | 32 (18) | 32 (18) | Children with anorectal malformations following repair | Infant group: mean 8 months (range 6–12 months) Child group: mean 3.4 years (range 15 months–5.9 years) | Rectoprostatic fistula: 5 Rectobulbar fistula: 3 No fistula: 3 Rectovestibular fistula: 2 Rectovaginal fistula: 1 Anocutaneous fistula: 7 Rectoperineal fistula: 2 Anovestibular fistula: 9 | Renal: 13 Cardiac: 16 Sacral: 4 VACTERL: 1 Chromosomal: 1 | PSARP (high anomalies) or anoplasty (low anomalies). |
| Langemeijer [29] | 1991 | 50 (28) | 39 (-) | Patients with high malformation following PSARP | Not reported. Age at operation: -primary PSARP: 1 month–5 years -redo PSARP: 6–16 years | High: 39 | Not reported | Primary PSARP: 40 Redo PSARP: 10 Not specified for manometry cohort |
| Leung [70] | 2006 | 12 (10) | 9 (-) | Children >5 years old with FI following anorectal malformation repair | Age range: 5–17 years during program completion. | High: 7 Intermediate: 5 Not specified for manometry cohort | Not reported | Pullthrough: 7 PSARP: 5 |
| Lin [30] | 1996 | 27 (-) | 27 (-) | Children with high or intermediate malformation following PSARP or R-APSA | PSARP: <4 years: 10 >4 years: 13 R-APSA: <4 years: 4 | Rectoprostatic fistula: 8 Rectobulbar fistula: 3 Rectovaginal fistula: 3 Blind: 11 Cloacal anomaly: 2 | Spinal: 1 T21: 1 Renal: 2 Genital: 3 Esophageal: 1 | PSARP: 23 R-APSA: 4 |
| Lin [31] | 2003 | 22 (16) | 22 (16) | Patients with high or intermediate malformations following LAR or PSARP | LAR group: mean 16.2 months (range: -) PSARP: mean 17.1 months (range: -) | Rectoprostatic fistula: 12 Rectobulbar fistula: 3 Rectovaginal fistula: 6 Blind pouch: 1 | T21: 2 Genital: 3 Cardiac: 2 Renal: 1 Esophageal: 1 | LAR: 9 PSARP: 13 |
| Liu [32] | 2004 | 113 (90) | 113 (90) | Patients with intermediate or high malformations following PSARP | Not reported. Median age at last follow up: -Group 1: 7.8 years (range 4.9–13 years) -Group 2: 6.7 years (range 5.3–11.6 years) | Rectovesical fistula: 5 Rectoprostatic fistula: 10 Anorectal agenesis w/o fistula: 15 Rectovaginal fistula: 1 Rectobulbar fistula: 49 Anal agenesis w/o fistula: 12 Rectovestibular fistula: 21 | Sacral anomalies: 6 T21: 2 Genital: 4 | Traditional PSARP: 48 One-stage PSARP: 65 |
| Martins [50] | 1996 | 27 (17) | 27 (17) | Patients with intermediate or high malformations following PSARP | Range: 4–11 years. Measure of central tendency not provided. | Rectourethral fistula: 17 Rectovaginal fistula: 5 Rectovestibular fistula: 5 | Sacral malformation: 10 | PSARP: 27 |
| Mert [55] | 2021 | 23 (18) | 23 (18) | Children following anorectal malformation repair, able to cooperate during anorectal manometry without neurological or neurosurgical disorders | Median: 7 (range 5–14) years | Anorectal agenesis without fistula: 5 Rectovesical fistula: 5 Rectobulbar fistula: 4 Rectovestibular fistula: 2 8 Rectoperineal fistula: 7 | Not reported | Not reported |
| Mollard [75] | 1991 | 21 (-) | 13 (-) | Patients with intermediate or high malformations following repair | Not reported | High: 7 Intermediate: 6 | Not reported | Anterior perineal approach |
| Nagashima [62] | 1992 | 159 (108) | 32 (-) | Children following repair of anorectal malformations | Mean: 9 years (range 5–16 years). | High: 17 Intermediate: 6 Low: 9 | Not reported | Abdominoperineal rectoplasty: high/intermediate (23) Perineoplasty: low (9) |
| Niedzielski [33] | 2008 | 94 (44) | 91 (42) | Children following PSARP | Not reported. Assessed 6 months–16 years following PSARP (mean 11.4 years). | Not specified for manometry cohort Perineal fistula (26); vestibular fistula (17); vaginal fistula (5: 2 low, 3 high); anal stenosis (3); cutaneous fistula (1); cloaca (4); no fistula (10); midline raphe fistula (6); bulbar fistula (5); prostatic fistula (9); rectoanal stenosis (5); bladder neck fistula (2); rectal atresia (1). Specified for manometry cohort: high (68); low (23). | Not reported | PSARP: 91 |
| Ninan [71] | 1994 | 13 (9) | 13 (9) | Children undergoing levatorplasty for management of FI following anorectal malformation repair | Not reported. Age at levatorplasty: mean 10.7 years (4–17) | High malformation: 11 Rectovestibular fistula: 1 Cloaca: 1 | Renal: 6 Cardiac: 1 Esophageal: 2 T21: 1 Spinal: 1 | Sacroperineal pullthrough: 5 Sacroabdominoperineal pullthrough: 7 Anoplasty: 1 |
| Okada [21] | 1993 | 10 (4) | 6 (-) | Patients following ASARP for re-operation due to FI following anorectal malformation repair | Not reported. Median age at redo operation: 4.5 years (range 2–7). Median follow-up at assessment: 3.29 years (range 1.1–5.3). | High: 3 Intermediate: 5 Low: 2 Not specified for manometry cohort | Not reported | ASARP (re-operation): 10/10 |
| Penninckx [16] | 1986 | 54 (20) | 19 (-) | Infants with anorectal malformation treated at a single center | Vaginal anal canal: mean 31 ± 15 months Urethral anal canal: mean 7 ± 3 months Vesical anal canal: mean 43 ± 6 months No orifice: mean 14 ± 15 months | Vaginal anal canal: 6 Urethral anal canal: 5 Vesical anal canal: 2 No orifice: 6 | Not reported | Variety of repair strategies reported, without specification of cohort size. |
| Ray [76] | 2004 | 115 (69) | 115 (69) | Children with intermediate or high malformation, following PSARP | Not reported. | High: 12 Intermediate: 103 | Spinal: 2 Renal: 3 | PSARP: - ASARP: - |
| Ren [34] | 2019 | 48 (48) | 22 (22) | Children with intermediate malformations following SILAARP or PSARP | SILAARP: 29.20 months ± 10.21 PSARP: 32.07 months ± 10.54 | Rectobulbar fistula: 48 | Spinal: 18 Renal: 16 Cardiac: 11 | PSARP: 14 SILAARP: 34 |
| Rintala [35] | 1990 | 30 (25) | 30 (25) | Patients with intermediate or high malformations following repair | Group 1: mean 3.1 years (range 1–6 years) Group 2: mean 8.8 years (range 5–13 years) | High: 25 Intermediate: 5 | Not reported | Group 1: 14 PSARP (12) or sacroperineal pull-through (2). Group 2: 16 primary sacro-abdominoperineal pull-through (16); with nine undergoing secondary reconstruction by PSARP (9). |
| Rintala [36] | 1995 | 65 (36) | 53 (-) | Patients with intermediate or high malformations | Not reported | Rectoprostatic fistula: 26 Rectobulbar fistula: 5 Anal agenesis: 4 Rectovesical fistula: 2 Cloaca: 9 Rectovestibular fistula: 16 Rectovaginal fistula: 3 Not specified for manometry cohort | Not reported | PSARP: 53 |
| Rintala [58] | 1993 | 40 (22) | 40 (22) | Patients with intermediate or high anorectal malformations | Not reported | Rectoprostatic fistula: 17 Rectobulbar fistula: 4 Anal agenesis: 2 Cloaca: 8 Rectovestibular fistula: 8 Rectovaginal fistula: 1 | Not reported | PSARP: 40 |
| Rintala [17] | 1990 | 10 (-) | 9 (-) | Patients with intermediate or high malformations | Not reported | High: - Intermediate: - | Not reported | PSARP: 9 |
| Rintala [59] | 1995 | 46 (25) | 46 (25) | Patients following PSARP for intermediate and high malformations | Mean 6.2 years (range 3.8–10). | Rectoprostatic fistula: 19 Rectobulbar fistula: 4 Anal agenesis: 3 Cloaca: 9 Rectovestibular fistula: 9 Rectovaginal fistula: 2 | Significant sacral/spinal defects: 11 T21: 2 | PSARP: 46 |
| Rintala [60] | 1995 | 16 (14) | 16 (14) | Patients undergoing secondary PSARP for intractable FI following primary anorectal malformation repair | Not reported. Manometry performed prior to secondary repair. Age at secondary repair: mean 12.4 years (range 8–16). | Rectourethral fistula: 11 Rectovesical fistula: 2 High anomaly, no fistula: 1 Cloaca: 2 | Significant sacral anomalies: 4 | Secondary repair PSARP: 16 Primary repair Sacroabdominoperineal pullthrough: 10 Abdominoperineal pullthrough: 6 |
| Ruttenstock [18] | 2013 | 12 (0) | 12 (0) | Patients with an externally accessible fistula | Median 585 days (range 197–1287 days) | Perineal fistula: 7 Rectovestibular fistula: 5 | Cardiac: 3 Renal: 4 Sacral: 2 Chromosomal: 1 | ASARP: 6 Mini-PSARP: 6 |
| Sangkhathat [63] | 2004 | 24 (18) | 24 (18) | Infants less than three years of age, post-anoplasty for treatment of anorectal malformation | Mean 9.6 months (range 2–36 months) | Perineal fistula: 6 Vestibular fistula: 3 Rectobulbar urethral fistula: 6 Rectovaginal fistula: 1 Blind rectal pouch: 8 | T21: 4 Opitz syndrome: 1 Caudal regression: 1 | PSARP: - Posterior myectomy and Y-V plasty: - Limited PSARP: - |
| Schuster [19] | 2000 | 10 (1) | 10 (1) | Patients managed for perineal fistula using anal transposition technique | Mean 20.75 months (range 6–72 months) | Perineal fistula: 10 | Not reported | Anal transposition technique: 10 |
| Schuster [42] | 2001 | 17 (10) | 17 (10) | Children with anorectal malformations following PSARP | Mean: 5.4 years (32–120 months) | Fistula location: rectovaginal (3); vestibular (2); rectovesical (2); prostatic (1); bulbar urethral (4) perineal (2). Cloacal malformation: 2 Rectal atresia: 1 | Normal sacrum: 7/17 (42%) | PSARP: 17/17 (100%) Secondary PSARP: 4/17 (24%) |
| Senel [51] | 2007 | 18 (12) | 18 (12) | Children with anorectal malformations following repair | Mean 6.2 years (range 63–104 months) | Rectovesical fistula: 1 Rectoprostatic fistula: 4 Rectal atresia: 1 Rectovestibular fistula: 5 Rectovaginal: 1 9 Rectobulbar: 6 | Not reported | PSARP: 9 Sacroperineal pullthrough: 3 Perineal pullthrough: 6 |
| Sonnino [37] | 1991 | 5 (3) | 5 (3) | Children with FI treated with gracilis muscle transposition | Mean: 13 years (range 10–17 years) | High anorectal malformation: 5 | VACTERL: 3 | Gracilis muscle transposition: 5 Primary repair not reported. |
| Tang [52] | 2017 | 6 (2) | 6 (2) | Children with defecation disorders | Mean 5 years (range 4–9) | Not reported | Not reported | PSARP: 6 |
| Tong [38] | 2011 | 61 (50) | 61 (50) | Infants with high anorectal malformation treated with LAARP vs. PSARP | 3.1–4.4 years Age at operation: LAARP: mean 5.3 months (range 3–10) PSARP: mean 4.9 months (range 3–11) | Rectoprostatic fistula: 39 Rectobulbar fistula: 13 Rectovesical fistula: 2 Rectovaginal fistula: 7 | Not reported | LAARPT: 33 PSARP: 28 |
| Vital Junior [53] | 2007 | 82 (46) | 82 (46) | Children with anorectal malformation following PSARP | Mean: 85.5 months (range 12–204) | High: 45 Intermediate: 37 | Not reported | PSARP: 82 |
| Wang [54] | 2016 | 47 (31) | 47 (31) | Children treated at a single center without congenital megarectum, sacral or spinal deformities | Mean: 4 years (range 1.4–8.9) | Rectourethral fistula: 15 Rectovaginal fistula: 2 Rectovesical fistula: 1 Perineal fistula: 11 Anovestibular fistula: 6 Anal stenosis: 2 Anal hole 10: 1 No fistula: 9 | Not reported | PSARP: 23 Transperineal anorectoplasty: 24 |
| Yang [39] | 2009 | 23 (19) | 23 (19) | Children with high anorectal malformations following PSARP or LAARP | LAARP: mean 17.4 months (SD 4.9) PSARP: mean 19.3 months (SD 6.2) | Rectourethral fistula: 6 Rectoprostatic fistula: 5 Rectovesical fistula: 4 Rectovaginal fistula: 3 Anorectal agenesis: 5 | Not reported | LAARPT: 11 (11 male) PSARP: 12 (8 male) |
3.3. Anorectal Manometry Characteristics
3.3.1. Equipment
3.3.2. Preparation and Sedation
| First Author | Year | Catheter Type | No. Sensors | Sensor Spacing | Preparation | Sedation/Anesthetic |
|---|---|---|---|---|---|---|
| Arnoldi [14] | 2014 | WP | 4 | - | Enema: performed evening prior | No sedation |
| Banasiuk [64] | 2021 | 3D HRAM | 256 | - | No routine preparation. Saline enema, if required | - |
| Becmeur [23] | 2001 | - | - | - | - | - |
| Bhat [56] | 2008 | FP | Open tip | - | - | - |
| Burjonrappa [61] | 2010 | WP | - | - | - | - |
| Cahill [24] | 1985 | WP | 8 | - | - | - |
| Caldaro [43] | 2012 | WP | 4 | - | Enema: performed day prior | No sedation |
| Caruso [67] | 2015 | WP | 4 | - | - | No sedation |
| Caruso [72] | 2021 | 3D HRAM | 256 | - | - | - |
| Chen [73] | 1998 | WP | 4 | 0.5 cm | - | Rectal secobarbital: 6 mg/kg (<2 years) |
| Chung [22] | 2018 | WP HRAM | 8 | - | - | No sedation |
| Doolin [44] | 1993 | SaP | Open tip | - | - | - |
| El-Debeiky [25] | 2009 | S + WP | - | 2.5 cm | - | - |
| Emblem [40] | 1994 | Micro-transducer | - | - | - | - |
| Emblem [45] | 1997 | Micro-transducer | - | - | - | - |
| Fukata [41] | 1997 | WP Foley catheter | 1 | - | - | - |
| Hedlund [46] | 1992 | WP | 1 | - | - | - |
| Heikenen [74] | 1999 | WP | 8 | - | - | - |
| Hettiarachchi [47] | 2002 | WP | 4 | - | No preparation | Ketamine |
| Huang [20] | 2017 | - | - | - | - | - |
| Husberg [26] | 1992 | WP 11 | 1 | - | - | Ketamine or pentothal-N20 (if required). |
| Ishihara [48] | 1987 | WP | 1 | - | Enema | Monosodium trichlorethyl phosphate (<4 years) |
| Iwai [15] | 1988 | FP Foley catheter | - | - | - | - |
| Iwai [68] | 1993 | FP | - | - | - | - |
| Iwai [65] | 1997 | FP | - | - | - | - |
| Iwai [66] | 2007 | FP | - | - | - | - |
| Keshtgar [69] | 2007 | Microballoon | 4 | 1 cm | - | Ketamine |
| Keshtgar [49] | 2008 | Microballoon | 4 | 1 cm | - | Ketamine |
| Kimura [27] | 2010 | WP Foley catheter | - | - | - | - |
| Kudou [28] | 2005 | - | - | - | - | Triclofos sodium |
| Kumar [57] | 2010 | SaP | 4 | 1 cm | Glycerin enema | No sedation |
| Langemeijer [29] | 1991 | WP | Open tip | - | - | Nitrous oxide (<2 years) |
| Leung [70] | 2006 | - | - | - | - | - |
| Lin [30] | 1996 | WP | 4 | 0.5 cm | - | Secobarbiturates (<2 years) |
| Lin [31] | 2003 | WP | 3 | - | - | Secobarbiturates; general anesthetic (<1 year). |
| Liu [32] | 2004 | WP | Open tip | - | - | No sedation |
| Martins [50] | 1996 | Balloon | 2 | - | - | No sedation |
| Mert [55] | 2021 | FP | 8 | 0.5 mm | Enema: performed 2 h prior (70% sorbitol, glycerin, and tri-Sodium citrate hydrate) | No sedation |
| Mollard [75] | 1991 | FP | 2 | 3 cm | - | - |
| Nagashima [62] | 1992 | WP | Open tip | - | Glycerin enema | - |
| Niedzielski [33] | 2008 | - | - | - | - | - |
| Ninan [71] | 1994 | - | - | - | - | - |
| Okada [21] | 1993 | WP | Open tip | - | - | - |
| Penninckx [16] | 1986 | Microballoon | 1–3 | - | - | - |
| Ray [76] | 2004 | FP | - | - | - | - |
| Ren [34] | 2019 | HRAM 12 | - | - | - | Chloral hydrate |
| Rintala [35] | 1990 | SaP | 1 | - | - | Ketamine (if required) |
| Rintala [36] | 1995 | SaP 13 | 1 | - | - | - |
| Rintala [58] | 1993 | SaP 13 | 1 | - | - | - |
| Rintala [17] | 1990 | SaP 14 | 1 | - | - | - |
| Rintala [59] | 1995 | SaP 13 | 1 | - | - | - |
| Rintala [60] | 1995 | SaP 13 | 1 | - | - | - |
| Ruttenstock [18] | 2013 | SaP | 4 | 5 mm | Bowel washout day prior | - |
| Sangkhathat [63] | 2004 | WP | 2 | 2 cm | - | Chloral hydrate |
| Schuster [19] | 2000 | WP | 8 | - | - | - |
| Schuster [42] | 2001 | WP | 8 | - | - | - |
| Senel [51] | 2007 | WP | 4 | 0.5 cm | - | - |
| Sonnino [37] | 1991 | Double balloon | - | - | No preparation | - |
| Tang [52] | 2017 | WP HRAM | 24 | 1 cm | Sodium phosphate rectal fleet enema | No sedation |
| Tong [38] | 2011 | WP | 8 | - | - | Chloral hydrate 1 mL/kg |
| Vital Junior [53] | 2007 | WP | 4 | - | - | - |
| Wang [54] | 2016 | HRAM | 12 | - | Enema | Chloral hydrate 0.3–0.5 mL/kg (if required) |
| Yang [39] | 2009 | - | - | - | - | Chloral hydrate 1 mL/kg |
3.3.3. Parameters
3.4. Anorectal Manometry Outcomes
3.4.1. Resting Pressure
3.4.2. Rectoanal Inhibitory Reflex
3.4.3. Squeeze Pressure
3.4.4. Normal Findings
3.4.5. Post-Operative Outcome Assessment
4. Discussion
4.1. Manometry Outcomes
4.2. Manometry Outcomes and Clinical Correlates
4.3. Practice Variability
5. Limitations and Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
Abbreviations
Appendix A
| 1. anorectal malformations/or anus, imperforate/ |
| 2. ((anorectal or anal or rectal) adj3 (anomal* or atresia* or malformation* or stenos#s)).tw,kf. |
| 3. ((anus adj3 (imperforate* or agenesi* or atresia)) or atresia-ani or atretic-anus).tw,kf. |
| 4. manometry/ |
| 5. manometr*.tw,kf. |
| 6. (1 or 2 or 3) and (4 or 5) |
| 7. exp animals/not human*.sh. |
| 8. 6 not 7 |
| 1. anorectal malformation/or anus atresia/ |
| 2. ((anorectal or anal or rectal) adj3 (anomal* or atresia* or malformation* or stenos#s)).tw,kw,dq. |
| 3. ((anus adj3 (imperforate* or agenesi* or atresia)) or atresia-ani or atretic-anus).tw,kw,dq. |
| 4. manometry/ |
| 5. manometr*.tw,kw,dq. |
| 6. (1 or 2 or 3) and (4 or 5) |
| 7. exp animal/not human*.sh. |
| 8. 6 not 7 |
References
- Levitt, M.A.; Peña, A. Anorectal malformations. Orphanet J. Rare Dis. 2007, 2, 33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peña, A.; Bischoff, A. History of the Treatment of Anorectal Malformations; Springer International Publishing: Berlin/Heidelberg, Germany, 2015; pp. 1–16. [Google Scholar] [CrossRef]
- Peña, A.; Devries, P.A. Posterior sagittal anorectoplasty: Important technical considerations and new applications. J. Pediatr. Surg. 1982, 17, 796–811. [Google Scholar] [CrossRef] [PubMed]
- Kyrklund, K.; Pakarinen, M.P.; Rintala, R.J. Long-term bowel function, quality of life and sexual function in patients with anorectal malformations treated during the PSARP era. Semin. Pediatr. Surg. 2017, 26, 336–342. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rigueros Springford, L.; Connor, M.J.; Jones, K.; Kapetanakis, V.V.; Giuliani, S. Prevalence of Active Long-term Problems in Patients With Anorectal Malformations: A Systematic Review. Dis. Colon. Rectum. 2016, 59, 570–580. [Google Scholar] [CrossRef] [PubMed]
- Carrington, E.V.; Scott, S.M.; Bharucha, A.; Mion, F.; Remes-Troche, J.M.; Malcolm, A.; Heinrich, H.; Fox, M.; Rao, S.S. Expert consensus document: Advances in the evaluation of anorectal function. Nat. Rev. Gastroenterol. Hepatol. 2018, 15, 309–323. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carrington, E.V.; Heinrich, H.; Knowles, C.H.; Rao, S.S.; Fox, M.; Scott, S.M. Methods of anorectal manometry vary widely in clinical practice: Results from an international survey. Neurogastroenterol. Motil. 2017, 29, e13016. [Google Scholar] [CrossRef] [PubMed]
- Carrington, E.V.; Heinrich, H.; Knowles, C.H.; Fox, M.; Rao, S.; Altomare, D.F.; Bharucha, A.E.; Burgell, R.; Chey, W.D.; Chiarioni, G.; et al. The international anorectal physiology working group (IAPWG) recommendations: Standardized testing protocol and the London classification for disorders of anorectal function. Neurogastroenterol. Motil. 2020, 32, e13679. [Google Scholar] [CrossRef] [Green Version]
- Athanasakos, E.; Cleeve, S.; Thapar, N.; Lindley, K.; Perring, S.; Cronin, H.; Borrelli, O.; Mutalib, M. Anorectal manometry in children with defecation disorders BSPGHAN Motility Working Group consensus statement. Neurogastroenterol. Motil. 2020, 32, e13797. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Int. J. Surg. 2010, 8, 336–341. [Google Scholar] [CrossRef] [Green Version]
- Wells, G.A.; Tugwell, P.; O’Connell, D.; Welch, V.; Peterson, J.; Shea, B.; Losos, M. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomized Studies in Meta-Analyses. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.htm (accessed on 19 November 2020).
- Holschneider, A.; Hutson, J.; Peña, A.; Beket, E.; Chatterjee, S.; Coran, A.; Davies, M.; Georgeson, K.; Grosfeld, J.; Gupta, D.; et al. Preliminary report on the International Conference for the Development of Standards for the Treatment of Anorectal Malformations. J. Pediatr. Surg. 2005, 40, 1521–1526. [Google Scholar] [CrossRef]
- Stephens, F.D.; Smith, D.E.; Paul, N.W. Anorectal malformations in children: Update 1988. March Dimes Birth Defects Found. Birth Defects Orig. Artic. Ser. 1988, 24, 1–604. [Google Scholar]
- Arnoldi, R.; Macchini, F.; Gentilino, V.; Farris, G.; Morandi, A.; Brisighelli, G.; Leva, E. Anorectal malformations with good prognosis: Variables affecting the functional outcome. J. Pediatr. Surg. 2014, 49, 1232–1236. [Google Scholar] [CrossRef] [PubMed]
- Iwai, N.; Yanagihara, J.; Tokiwa, K.; Deguchi, E.; Takahashi, T. Voluntary anal continence after surgery for anorectal malformations. J. Pediatr. Surg. 1988, 23, 393–397. [Google Scholar] [CrossRef]
- Penninckx, F.; Kerremans, R. Internal sphincter-saving in imperforate anus with or without fistula. A manometric study. Int. J. Color. Dis. 1986, 1, 28–32. [Google Scholar] [CrossRef]
- Rintala, R.; Lindahl, H.; Sariola, H.; Rapola, J.; Louhimo, I. The rectourogenital connection in anorectal malformations is an ectopic anal canal. J. Pediatr. Surg. 1990, 25, 665–668. [Google Scholar] [CrossRef] [PubMed]
- Ruttenstock, E.M.; Zani, A.; Huber-Zeyringer, A.; Hollwarth, M.E. Pre- and postoperative rectal manometric assessment of patients with anorectal malformations: Should we preserve the fistula? Dis. Colon. Rectum. 2013, 56, 499–504. [Google Scholar] [CrossRef] [PubMed]
- Schuster, T.; Joppich, I.; Schneider, K.; Jobst, G. A computerised vector manometry study of the so-called ectopic anus. Pediatr. Surg. Int. 2000, 16, 8–14. [Google Scholar] [CrossRef]
- Huang, Y.; Shen, C.; Zheng, S.; Xiao, X. A follow-up study on postoperative function after a modified semi-posterior sagittal one-stage anorectoplasty for female imperforate anus with a rectovesibula fistula. Int. J. Clin. Exp. Med. 2017, 10, 913–920. [Google Scholar]
- Okada, A.; Tamada, H.; Tsuji, H.; Azuma, T.; Yagi, M.; Kubota, A.; Kamata, S. Anterior sagittal anorectoplasty as a redo operation for imperforate anus. J. Pediatr. Surg. 1993, 28, 933–938. [Google Scholar] [CrossRef]
- Chung, P.H.Y.; Wong, C.W.Y.; Wong, K.K.Y.; Tam, P.K.H. Assessing the long term manometric outcomes in patients with previous laparoscopic anorectoplasty (LARP) and posterior sagittal anorectoplasty (PSARP). J. Pediatr. Surg. 2018, 53, 1933–1936. [Google Scholar] [CrossRef]
- Becmeur, F.; Hofmann-Zango, I.; Jouin, H.; Moog, R.; Kauffmann, I.; Sauvage, P. Three-flap anoplasty for imperforate anus: Results for primary procedure or for redoes. Eur. J. Pediatr. Surg. 2001, 11, 311–314. [Google Scholar] [CrossRef] [PubMed]
- Cahill, J.L.; Christie, D.L. Results after posterior sagittal anorectoplasty: A new approach to high imperforate anus. Am. J. Surg. 1985, 149, 629–631. [Google Scholar] [CrossRef] [PubMed]
- El-Debeiky, M.S.; Safan, H.A.; Shafei, I.A.; Kader, H.A.; Hay, S.A. Long-term functional evaluation of fecal continence after laparoscopic-assisted pull-through for high anorectal malformations. J. Laparoendosc. Adv. Surg. Tech. A 2009, 19 (Suppl. 1), S51–S54. [Google Scholar] [CrossRef] [PubMed]
- Husberg, B.; Lindahl, H.; Rintala, R.; Frenckner, B. High and intermediate imperforate anus: Results after surgical correction with special respect to internal sphincter function. J. Pediatr. Surg. 1992, 27, 185–188; discussion 188–189. [Google Scholar] [CrossRef] [PubMed]
- Kimura, O.; Iwai, N.; Sasaki, Y.; Tsuda, T.; Deguchi, E.; Ono, S.; Furukawa, T. Laparoscopic versus open abdominoperineal rectoplasty for infants with high-type anorectal malformation. J. Pediatr. Surg. 2010, 45, 2390–2393. [Google Scholar] [CrossRef] [PubMed]
- Kudou, S.; Iwanaka, T.; Kawashima, H.; Uchida, H.; Nishi, A.; Yotsumoto, K.; Kaneko, M. Midterm follow-up study of high-type imperforate anus after laparoscopically assisted anorectoplasty. J. Pediatr. Surg. 2005, 40, 1923–1926. [Google Scholar] [CrossRef]
- Langemeijer, R.A.T.M.; Molenaar, J.C. Continence after posterior sagittal anorectoplasty. J. Pediatr. Surg. 1991, 26, 587–590. [Google Scholar] [CrossRef]
- Lin, C.-L.; Chen, C.-C. The rectoanal relaxation reflex and continence in repaired anorectal malformations with and without an internal sphincter-saving procedure. J. Pediatr. Surg. 1996, 31, 630–633. [Google Scholar] [CrossRef]
- Lin, C.L.; Wong, K.K.; Lan, L.C.; Chen, C.C.; Tam, P.K. Earlier appearance and higher incidence of the rectoanal relaxation reflex in patients with imperforate anus repaired with laparoscopically assisted anorectoplasty. Surg. Endosc. 2003, 17, 1646–1649. [Google Scholar] [CrossRef]
- Liu, G.; Yuan, J.; Geng, J.; Wang, C.; Li, T. The treatment of high and intermediate anorectal malformations: One stage or three procedures? J. Pediatr. Surg. 2004, 39, 1466–1471. [Google Scholar] [CrossRef]
- Niedzielski, J. Results of surgical correction of anorectal malformations in children—16-years experience. [Polish, English]. Chir. Pol. 2008, 10, 16–29. [Google Scholar]
- Ren, X.; Xu, H.; Jiang, Q.; Diao, M.; Li, X.; Li, L. Single-incision laparoscopic-assisted anorectoplasty for treating children with intermediate-type anorectal malformations and rectobulbar fistula: A comparative study. Pediatr. Surg. Int. 2019, 35, 1255–1263. [Google Scholar] [CrossRef] [PubMed]
- Rintala, R. Postoperative internal sphincter function in anorectal malformations—A manometric study. Pediatr. Surg. Int. 1990, 5, 127–130. [Google Scholar] [CrossRef]
- Rintala, R.; Lindahl, H. Internal sphincter-saving posterior sagittal anorectoplasty for high and intermediate anorectal malformations: Technical considerations. Pediatr. Surg. Int. 1995, 10, 345–349. [Google Scholar] [CrossRef]
- Sonnino, R.E.; Reinberg, O.; Bensoussan, A.L.; Laberge, J.M.; Blanchard, H. Gracilis muscle transposition for anal incontinence in children: Long-term follow-up. J. Pediatr. Surg. 1991, 26, 1219–1223. [Google Scholar] [CrossRef] [PubMed]
- Tong, Q.S.; Tang, S.T.; Pu, J.R.; Mao, Y.Z.; Wang, Y.; Li, S.W.; Cao, Q.Q.; Ruan, Q.L. Laparoscopically assisted anorectal pull-through for high imperforate anus in infants: Intermediate results. J. Pediatr. Surg. 2011, 46, 1578–1586. [Google Scholar] [CrossRef]
- Yang, J.; Zhang, W.; Feng, J.; Guo, X.; Wang, G.; Weng, Y.; Sun, X.; Yu, D. Comparison of clinical outcomes and anorectal manometry in patients with congenital anorectal malformations treated with posterior sagittal anorectoplasty and laparoscopically assisted anorectal pull through. J. Pediatr. Surg. 2009, 44, 2380–2383. [Google Scholar] [CrossRef]
- Emblem, R.; Diseth, T.; Morkrid, L.; Stien, R.; Bjordal, R. Anal endosonography and physiology in adolescents with corrected low anorectal anomalies. J. Pediatr. Surg. 1994, 29, 447–451. [Google Scholar] [CrossRef]
- Fukata, R.; Iwai, N.; Yanagihara, J.; Iwata, G.; Kubota, Y. A comparison of anal endosonography with electromyography and manometry in high and intermediate anorectal anomalies. J. Pediatr. Surg. 1997, 32, 839–842. [Google Scholar] [CrossRef]
- Schuster, T.; Lagler, F.; Pfluger, T.; Dietz, H.G.; Joppich, I. A computerized vector manometry and MRI study in children following posterior sagittal anorectoplasty. Pediatr. Surg. Int. 2001, 17, 48–53. [Google Scholar] [CrossRef]
- Caldaro, T.; Romeo, E.; De Angelis, P.; Gambitta, R.A.; Rea, F.; Torroni, F.; Foschia, F.; Federici Di Abriola, G.; Dall’Oglio, L. Three-dimensional endoanal ultrasound and anorectal manometry in children with anorectal malformations: New discoveries. J. Pediatr. Surg. 2012, 47, 956–963. [Google Scholar] [CrossRef] [PubMed]
- Doolin, E.J.; Black, C.T.; Donaldson, J.S.; Schwartz, D.; Raffensperger, J.G. Rectal manometry, computed tomography, and functional results of anal atresia surgery. J. Pediatr. Surg. 1993, 28, 195–198. [Google Scholar] [CrossRef] [PubMed]
- Emblem, R.; Diseth, T.; Morkrid, L. Anorectal anomalies: Anorectal manometric function and anal endosonography in relation to functional outcome. Pediatr. Surg. Int. 1997, 12, 516–519. [Google Scholar] [CrossRef] [PubMed]
- Hedlund, H.; Pena, A.; Rodriguez, G.; Maza, J. Long-term anorectal function in imperforate anus treated by a posterior sagittal anorectoplasty: Manometric investigation. J. Pediatr. Surg. 1992, 27, 906–909. [Google Scholar] [CrossRef] [PubMed]
- Hettiarachchi, M.; Garcea, G.; de Souza, N.M.; Williams, A.D.; Clayden, G.S.; Ward, H.C. Evaluation of dysfunction following reconstruction of an anorectal anomaly. Pediatr. Surg. Int. 2002, 18, 405–409. [Google Scholar]
- Ishihara, M.; Okabe, I.; Morita, K. Assessment of the percentages of maximum static pressure in the anal canal for postoperative continence in patients with imperforate anus. Jpn. J. Surg. 1987, 17, 230–235. [Google Scholar] [CrossRef]
- Keshtgar, A.S.; Athanasakos, E.; Clayden, G.S.; Ward, H.C. Evaluation of outcome of anorectal anomaly in childhood: The role of anorectal manometry and endosonography. Pediatr. Surg. Int. 2008, 24, 885–892. [Google Scholar] [CrossRef]
- Martins, J.L.; Pinus, J. Clinical and manometric postoperative evaluation of posterior sagital anorectoplasty (PSARP) in patients with upper and intermediate anorectal malformations. Sao Paulo Med. J. 1996, 114, 1303–1308. [Google Scholar] [CrossRef] [Green Version]
- Senel, E.; Demirbag, S.; Tiryaki, T.; Erdogan, D.; Cetinkursun, S.; Cakmak, O. Postoperative anorectal manometric evaluation of patients with anorectal malformation. Pediatr. Int. 2007, 49, 210–214. [Google Scholar] [CrossRef]
- Tang, P.M.Y.; Leung, M.W.Y.; Hung, J.W.S.; Chung, K.L.Y.; Liu, C.S.W.; Chao, N.S.Y.; Liu, K.K.W. Application of three dimensional high resolution anorectal manometry to demonstrate anal sphincter pressure asymmetry in children after anorectal surgery: A pilot study. Hong Kong J. Paediatr. 2017, 22, 204–208. [Google Scholar]
- Vital Junior, P.F.; Martins, J.L.; Peterlini, F.L. Posterior sagittal anorectoplasty in anorectal anomalies: Clinical, manometric and profilometric evaluation. Sao Paulo Med. J. 2007, 125, 163–169. [Google Scholar] [CrossRef] [Green Version]
- Wang, Z.; Hu, L.; Jin, X.; Li, X.; Xu, L. Evaluation of postoperative anal functions using endoanal ultrasonography and anorectal manometry in children with congenital anorectal malformations. J. Pediatr. Surg. 2016, 51, 416–420. [Google Scholar] [CrossRef] [PubMed]
- Mert, M.; Sayan, A.; Köylüoğlu, G. Comparing the fecal continence scores of patients with anorectal malformation with anorectal manometric findings. Pediatr. Surg. Int. 2021, 37, 1013–1019. [Google Scholar] [CrossRef] [PubMed]
- Bhat, N.A.; Grover, V.P.; Bhatnagar, V. Pre-operative manometry of the blind rectal pouch to predict post-operative potential for continence in anorectal malformation. Trop. Gastroenterol. 2008, 29, 51–54. [Google Scholar] [PubMed]
- Kumar, S.; Al Ramadan, S.; Gupta, V.; Helmy, S.; Debnath, P.; Alkholy, A. Use of anorectal manometry for evaluation of postoperative results of patients with anorectal malformation: A study from Kuwait. J. Pediatr. Surg. 2010, 45, 1843–1848. [Google Scholar] [CrossRef] [PubMed]
- Rintala, R.; Lindahl, H.; Marttinen, E.; Sariola, H. Constipation is a major functional complication after internal sphincter-saving posterior sagittal anorectoplasty for high and intermediate anorectal malformations. J. Pediatr. Surg. 1993, 28, 1054–1058. [Google Scholar] [CrossRef]
- Rintala, R.J.; Lindahl, H. Is normal bowel function possible after repair of intermediate and high anorectal malformations? J. Pediatr. Surg. 1995, 30, 491–494. [Google Scholar] [CrossRef]
- Rintala, R.J.; Lindahl, H. Secondary posterior sagittal anorectoplasty for anorectal malformations. Long-term follow-up extending beyond childhood. Pediatr. Surg. Int. 1995, 10, 414–417. [Google Scholar] [CrossRef]
- Burjonrappa, S.; Youssef, S.; Lapierre, S.; Bensoussan, A.; Bouchard, S. Megarectum after surgery for anorectal malformations. J. Pediatr. Surg. 2010, 45, 762–768. [Google Scholar] [CrossRef]
- Nagashima, M.; Iwai, N.; Yanagihara, J.; Shimotake, T. Motility and sensation of the rectosigmoid and the rectum in patients with anorectal malformations. J. Pediatr. Surg. 1992, 27, 1273–1277. [Google Scholar] [CrossRef]
- Sangkhathat, S.; Patrapinyokul, S.; Osatakul, N. Crucial role of rectoanal inhibitory reflex in emptying function after anoplasty in infants with anorectal malformations. Asian J. 2004, 27, 125–129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Banasiuk, M.; Dziekiewicz, M.; Dembiński, Ł.; Piotrowski, D.; Kamiński, A.; Banaszkiewicz, A. Three-dimensional high-resolution anorectal manometry in children after surgery for anorectal disorders. In European Review for Medical and Pharmacological Sciences; Verduci: Rome, Italy, 2021; Volume 25, pp. 2981–2993. [Google Scholar]
- Iwai, N.; Iwata, G.; Kimura, O.; Yanagihara, J. Is a new biofeedback therapy effective for fecal incontinence in patients who have anorectal malformations? J. Pediatr. Surg. 1997, 32, 1626–1629. [Google Scholar] [CrossRef] [PubMed]
- Iwai, N.; Kume, Y.; Kimura, O.; Ono, S.; Aoi, S.; Tsuda, T. Effects of herbal medicine Dai-Kenchu-to on anorectal function in children with severe constipation. Eur. J. Pediatr. Surg. 2007, 17, 115–118. [Google Scholar] [CrossRef] [PubMed]
- Caruso, A.M.; Catalano, P.; Li Voti, G.; Salerno, S.; Casuccio, A.; Di Pace, M.R.; Cimador, M. Prognostic evaluation of biofeedback response in patients treated for anorectal malformation. J. Pediatr. Surg. 2015, 50, 1648–1652. [Google Scholar] [CrossRef] [PubMed]
- Iwai, N.; Nagashima, M.; Shimotake, T.; Iwata, G. Biofeedback therapy for fecal incontinence after surgery for anorectal malformations: Preliminary results. J. Pediatr. Surg. 1993, 28, 863–866. [Google Scholar] [CrossRef]
- Keshtgar, A.S.; Ward, H.C.; Richards, C.; Clayden, G.S. Outcome of excision of megarectum in children with anorectal malformation. J. Pediatr. Surg. 2007, 42, 227–233. [Google Scholar] [CrossRef]
- Leung, M.W.; Wong, B.P.; Leung, A.K.; Cho, J.S.; Leung, E.T.; Chao, N.S.; Chung, K.W.; Kwok, W.K.; Liu, K.K. Electrical stimulation and biofeedback exercise of pelvic floor muscle for children with faecal incontinence after surgery for anorectal malformation. Pediatr. Surg. Int. 2006, 22, 975–978. [Google Scholar] [CrossRef]
- Ninan, G.K.; Puri, P. Levatorplasty using a posterior sagittal approach in secondary faecal incontinence. Pediatr. Surg. Int. 1994, 9, 17–20. [Google Scholar] [CrossRef] [Green Version]
- Caruso, A.M.; Milazzo, M.P.M.; Bommarito, D.; Girgenti, V.; Amato, G.; Paviglianiti, G.; Casuccio, A.; Catalano, P.; Cimador, M.; Di Pace, M.R. Advanced Management Protocol of Transanal Irrigation in Order to Improve the Outcome of Pediatric Patients with Fecal Incontinence. Children 2021, 8, 1174. [Google Scholar] [CrossRef]
- Chen, C.C.; Lin, C.L.; Lu, W.T.; Hsu, W.M.; Chen, J.C. Anorectal function and endopelvic dissection in patients with repaired imperforate anus. Pediatr. Surg. Int. 1998, 13, 133–137. [Google Scholar] [CrossRef]
- Heikenen, J.B.; Werlin, S.L.; Di Lorenzo, C.; Hyman, P.E.; Cocjin, J.; Flores, A.F.; Reddy, S.N. Colonic motility in children with repaired imperforate anus. Dig. Dis. Sci. 1999, 44, 1288–1292. [Google Scholar] [CrossRef] [PubMed]
- Mollard, P.; Meunier, P.; Mouriquand, P.; Bonnet, J.P. High and intermediate imperforate anus: Functional results and postoperative manometric assessment. Eur. J. Pediatr. Surg. 1991, 1, 282–286. [Google Scholar] [CrossRef] [PubMed]
- Ray, A.K.; Singhania, A.K.; Mukherjee, S. Post PSARP anorectal manometry—Experience of 115 cases of imperforate anus. J. Indian Med. Assoc. 2004, 102, 253–255. [Google Scholar] [PubMed]
- Heitmann, P.T.; Rabbitt, P.; Schloithe, A.C.; Wattchow, D.A.; Scott, S.M.; Dinning, P.G. The relationships between the results of contemporary tests of anorectal structure and sensorimotor function and the severity of fecal incontinence. Neurogastroenterol. Motil. 2020, 32, e13946. [Google Scholar] [CrossRef] [PubMed]
- Heitmann, P.T.; Rabbitt, P.; Schloithe, A.; Patton, V.; Skuza, P.P.; Wattchow, D.A.; Dinning, P.G. Relationships between the results of anorectal investigations and symptom severity in patients with faecal incontinence. Int. J. Color. Dis. 2019, 34, 1445–1454. [Google Scholar] [CrossRef] [PubMed]
- Heitmann, P.T.; Vollebregt, P.F.; Knowles, C.H.; Lunniss, P.J.; Dinning, P.G.; Scott, S.M. Understanding the physiology of human defaecation and disorders of continence and evacuation. Nat. Rev. Gastroenterol. Hepatol. 2021, 18, 751–769. [Google Scholar] [CrossRef] [PubMed]
- Levitt, M.A.; Kant, A.; Peña, A. The morbidity of constipation in patients with anorectal malformations. J. Pediatr. Surg. 2010, 45, 1228–1233. [Google Scholar] [CrossRef]
- Lane, V.A.; Calisto, J.; Deblaauw, I.; Calkins, C.M.; Samuk, I.; Avansino, J.R. Assessing the previously repaired patient with an anorectal malformation who is not doing well. Semin. Pediatr. Surg. 2020, 29, 150995. [Google Scholar] [CrossRef]
- Bischoff, A.; Bealer, J.; Duncan Peña, A. Error traps and culture of safety in anorectal malformations. Semin. Pediatr. Surg. 2019, 28, 131–134. [Google Scholar] [CrossRef]
- King, S.K.; Krois, W.; Lacher, M.; Saadai, P.; Armon, Y.; Midrio, P. Optimal management of the newborn with an anorectal malformation and evaluation of their continence potential. Semin. Pediatr. Surg. 2020, 29, 150996. [Google Scholar] [CrossRef]
- Bajwa, A.; Fellow, R.; Emmanuel, A. The physiology of continence and evacuation. Best Pract. Res. Clin. Gastroenterol. 2009, 23, 477–485. [Google Scholar] [CrossRef]
- Scott, S.M.; Gladman, M.A. Manometric, sensorimotor, and neurophysiologic evaluation of anorectal function. Gastroenterol. Clin. North Am. 2008, 37, 511–538. [Google Scholar] [CrossRef]
- Dinning, P.G.; Wiklendt, L.; Maslen, L.; Gibbins, I.; Patton, V.; Arkwright, J.W.; Lubowski, D.Z.; O’Grady, G.; Bampton, P.A.; Brookes, S.J.; et al. Quantification of in vivo colonic motor patterns in healthy humans before and after a meal revealed by high-resolution fiber-optic manometry. Neurogastroenterol. Motil. 2014, 26, 1443–1457. [Google Scholar] [CrossRef] [Green Version]
- Rao, S.S.; Welcher, K. Periodic rectal motor activity: The intrinsic colonic gatekeeper? Am. J. Gastroenterol. 1996, 91, 890–897. [Google Scholar]
- Patton, V.; Wiklendt, L.; Arkwright, J.W.; Lubowski, D.Z.; Dinning, P.G. The effect of sacral nerve stimulation on distal colonic motility in patients with faecal incontinence. Br. J. Surg. 2013, 100, 959–968. [Google Scholar] [CrossRef] [PubMed]
- Lin, A.Y.; Du, P.; Dinning, P.G.; Arkwright, J.W.; Kamp, J.P.; Cheng, L.K.; Bissett, I.P.; O’Grady, G. High-resolution anatomic correlation of cyclic motor patterns in the human colon: Evidence of a rectosigmoid brake. Am. J. Physiol. Gastrointest. Liver Physiol. 2017, 312, G508–G515. [Google Scholar] [CrossRef] [PubMed]


First Author | Resting Pressure | Squeeze Pressure | Endurance Squeeze | Anal Canal Length | High Pressure Zone (HPZ) | Sensation | Maximum Volume tolerated | RAIR | Cough | Rectal Compliance | Other |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Arnoldi [14] | ● | ● | ● | ||||||||
| Banasiuk [64] | ● | ● | ● | ● | ● | Resting and squeeze pressures of the puborectalis muscle 16 | |||||
| Becmeur [23] | ● | ● | |||||||||
| Bhat [56] | ● | ||||||||||
| Burjonrappa [61] | ● | ● | |||||||||
| Cahill [24] | ● | ● | |||||||||
| Caldaro [43] | ● | ● | ● | ● | ● | ||||||
| Caruso [67] | ● | ● | Sphincter symmetry | ||||||||
| Caruso [72] | ● | ● | Sphincterial asymmetry 17, rectal sensitivity 18 | ||||||||
| Chen [73] | ● 19 | ● | Anorectal pressure gradient | ||||||||
| Chung [22] | ● | ● | ● | ● | |||||||
| Doolin [44] | ● | ● 20 | ● | Spontaneous contraction pressure; rectal contraction frequency (number/minute) | |||||||
| El-Debeiky [25] | ● | ● | ● | ● | ● | ● | |||||
| Emblem [40] | ● | ● | ● | ||||||||
| Emblem [45] | ● | ● | |||||||||
| Fukata [41] | ● | ● | |||||||||
| Hedlund [46] | ● | ● | ● | Average rectal volume | |||||||
| Heikenen [74] | ● | ● | ● | ||||||||
| Hettiarachchi [47] | ● | Manometric rectal score, IAS length and activity scores | |||||||||
| Huang [20] | ● 21 | ● | Active systolic blood pressure; rectal compliance 22 | ||||||||
| Husberg [26] | ● | ● | |||||||||
| Ishihara [48] | ● 23 | ||||||||||
| Iwai [15] | ● | ||||||||||
| Iwai [68] | ● | ● | ● | ● | ● | ● | Anorectal pressure difference | ||||
| Iwai [65] | ● | ● | ● | ● | ● | ● | ● | ||||
| Iwai [66] | ● | ● | ● | ● | ● | ● | ● | ||||
| Keshtgar [69] | ● | ● | |||||||||
| Keshtgar [49] | ● | ● | |||||||||
| Kimura [27] | ● | ● | |||||||||
| Kudou [28] | ● | ● 24 | ● | ||||||||
| Kumar [57] | ● | ● | ● | ||||||||
| Langemeijer [29] | ● | ● | ● | ||||||||
| Leung [70] | ● | ||||||||||
| Lin [30] | ● | ● | Anorectal pressure profile, slow wave activity of the anal canal. | ||||||||
| Lin [31] | ● | ● | |||||||||
| Liu [32] | ● | ● | ● | ||||||||
| Martins [50] | ● | ● | ● | ● | Duration of sustained voluntary contraction, perianal stimulation, crying, pressure curve during balloon withdrawal. | ||||||
| Mert [55] | ● | ● | ● | ● | ● | ● | First urge to defecate volume; area under curve during maximum voluntary squeeze. | ||||
| Mollard [75] | ● | ● | ● | Maximal anal resting closure pressure: maximal anal pressure minus rectal pressure. | |||||||
| Nagashima [62] | ● | ● | ● | ● | Anorectal pressure difference. 25 | ||||||
| Niedzielski [33] | ● | ● | ● | Rectoanal pressure gradient, reflex pressure amplitude. | |||||||
| Ninan [71] | ● | ||||||||||
| Okada [21] | ● 26 | ● 27 | |||||||||
| Penninckx [16] | ● | ● | Anal slow pressure waves at rest | ||||||||
| Ray [76] | ● | ● | ● | ● | |||||||
| Ren [34] | ● | ● | ● | ||||||||
| Rintala [35] | ● | ● | Slow pressure-wave activity of the anal canal | ||||||||
| Rintala [36] | ● | ● | |||||||||
| Rintala [58] | ● | ● | |||||||||
| Rintala [17] | ● | ● | Slow pressure-wave activity of the anal canal | ||||||||
| Rintala [59] | ● | ● | |||||||||
| Rintala [60] | ● | ● | ● | ||||||||
| Ruttenstock [18] | ● | ● | ● | ||||||||
| Sangkhathat [63] | ● | ● | ● | Resting rectoanal pressure gradient 28 | |||||||
| Schuster [19] | ● 29 | ● | ● | ● | Segmental and total asymmetry indexes; vector volume 30 | ||||||
| Schuster [42] | ● 31 | ● 32 | ● 33 | ● | Sphincter length; vector volume 34 | ||||||
| Senel [51] | ● | ● | |||||||||
| Sonnino [37] | ● | ● | ● | ||||||||
| Tang [52] | ● | ● | Inter-quadrant pressure asymmetry index 35 | ||||||||
| Tong [38] | ● | ● | ● | ● | Asymmetry index, vector volume 36 | ||||||
| Vital Junior [53] | ● | ● 37 | ● | ● | ● | Maximum pressure, pressure during perianal stimulation, pressure asymmetry | |||||
| Wang [54] | ● | ● | |||||||||
| Yang [39] | ● | ● | ● | ||||||||
| Prevalence | 55 | 29 | 1 | 7 | 10 | 14 | 7 | 52 | 2 | 5 |
| First Author | Manometry Population Summary | Summary of Key Anorectal Manometry Findings | Key Limitations |
|---|---|---|---|
| Arnoldi [14] | Toilet-trained children with anorectal malformations with a good predicted prognosis 38 |
| Exclusion based on toilet training status introduces potential selection bias (excluding children who may never attain continence); although the homogenous population is a strength, findings not generalizable to the wider anorectal malformation cohort. |
| Banasiuk [64] | Children who had undergone surgery for anorectal disorders, including anal atresia |
| Clinical characteristics, such as gender of diagnostic subgroups and operative repair type unknown; small, heterogenous anorectal malformation cohort: wide age range with diverse malformation types. |
| Becmeur [23] | Children following three-flap anoplasty for primary or re-do repair |
| Small, heterogeneous cohort; significant proportion of cohort with comorbidities likely to impact continence; very limited description of manometry methods/results. |
| Bhat [56] | High or intermediate anorectal malformation, following sigmoid colostomy formation but prior to PSARP |
| Small cohort; associated anomalies not reported; limited description of statistical methods to support findings (e.g., correlation between anal canal pressures and Kelly score); short follow up period to support conclusion that post-operative continence may be predicted pre-operatively (median age 29 months (range 19–60) at assessment). |
| Burjonrappa [61] | Patients with megarectum following surgery for anorectal malformation |
| Small, heterogeneous manometry cohort (six children); select population (children with megarectum); limited manometric assessment with variable reporting of findings. |
| Cahill [24] | Patients with anorectal malformation following PSARP |
| Small cohort; limited description of manometry techniques, findings, and interpretation; too young at follow up to adequately assess bowel function to support the interpretation of findings. |
| Caldaro [43] | Neurologically healthy children, >4 years, with constipation/FI, following anorectal malformation repair |
| Small malformation subgroups limit strength of findings with respect to malformation types. |
| Caruso [67] | Neurologically heathy children >4 years with “true” FI following anorectal malformation repair |
| Manometry/MRI assessment would benefit from clarification of scoring; relatively small subgroups (determined by pre-operative assessment). |
| Caruso [72] | Children with FI or bowel dysfunction not responsive to conventional laxative treatment, receiving transanal irrigation |
| Small anorectal malformation cohort; surgical repair type not reported. |
| Chen [73] | All children with anorectal malformation repaired by a single surgeon |
| Limited cohort data provided for manometry cohort; limited by technology available; idiosyncratic symptom assessments may limit comparability. |
| Chung [22] | Toilet-trained children following PSARP or LAARP without neurological comorbidities or cloacal malformation |
| Small operative/malformation subgroups; difference in time period between operative subgroups—results may be confounded by evolution of pre- and post-operative care; PSARP subgroup older than LAARP cohort and includes subjects >18 years, limiting comparability. |
| Doolin [44] | Children following repair of anal atresia |
| Malformation classification not known for all patients; limited by technology available. |
| El-Debeiky [25] | Males with high anorectal malformation treated with laparoscopic-assisted pull-through |
| Small cohort; unclear age at assessment limited, qualitative reporting of manometry findings, without clarification of interpretation (e.g., “high” versus “low” resting pressure); assessment of correlation between manometry findings and function not reported. |
| Emblem [40] | Adolescents with low anorectal malformations following repair |
| Small cohort; limited by technology available; limited information provided regarding technique. |
| Emblem [45] | Adolescents with anorectal malformations following repair |
| Small malformation subgroups limit strength of findings with respect to malformation types; cohort details limited (type of malformation and surgical repair); limited by technology available; potentially subject to non-responder bias. |
| Fukata [41] | Patients with high or intermediate anorectal malformations |
| Small cohort; limited by manometry techniques available; functional outcome reported as Kelly score without description of symptom profile; methods/outcomes to assess statistical correlations not reported. |
| Hedlund [46] | Patients with anorectal malformations following PSARP, without major sacral malformation |
| Statistical assessment of correlation between manometry findings and clinical outcomes not reported; limited reporting of patient cohort data; limited reporting of manometry outcomes. |
| Heikenen [74] | Children with FI refractory to standard medical therapy following repair of anorectal malformation |
| Limited reporting of anorectal manometry technique and outcomes; small cohort; anorectal manometry not performed in all children. |
| Hettiarachchi [47] | Children with chronic constipation and/or FI following anorectal malformation repair |
| Small, heterogenous cohort, particularly with respect to age, repair, malformation type, associated anomalies, and functional outcomes; idiosyncratic scoring system limits comparability; limited objective reporting of manometry findings. |
| Huang [20] | Female patients with rectovestibular fistula |
| Manometric assessment of “active systolic blood pressure” and measurement of rectal compliance unclear; assessment of correlation between symptom groups and manometry findings not performed. |
| Husberg [26] | Children with high or intermediate anorectal malformation |
| Limited by technology and surgical repair techniques available; limited reporting of manometry findings; bi-national cohort, assessed utilizing different anorectal manometry techniques; small sub-cohort > 4 years contributing to functional evaluation. |
| Ishihara [48] | Patients with anorectal malformations following repair |
| Limited by technology available; limited reporting of cohort demographic and medical details; few comparable manometry findings (results expressed as percent maximum static pressure of control group). |
| Iwai [65] | Children undergoing biofeedback training for FI following anorectal malformation repair |
| Small cohort; limited cohort characteristics provided, including median cohort age at assessment, operative repair type, or characterization of FI; limited description of manometry technique. |
| Iwai [66] | Children with severe constipation following anorectal malformation repair, treated with herbal medication |
| Very small anorectal malformation sub-cohort; limited description of manometry technique; statistical comparison of manometry findings in anorectal malformation cohort not performed, due to small cohort size. |
| Iwai [68] | Children undergoing biofeedback training for FI following anorectal malformation repair |
| Small cohort; responders had three or more sessions (non-responders only one or two sessions), potentially confounding this result; limited description of manometry techniques. |
| Iwai [15] | Patients with anorectal malformations following repair |
| Manometry not performed in all patients; limited description of cohort characteristic; limited manometric assessment performed; statistical assessment of correlation between manometry findings and bowel function scores not assessed/reported. |
| Keshtgar [69] | Children undergoing excision of megarectum for intractable FI |
| Heterogenous cohort with respect to malformation and primary repair types; quantitative manometry results not provided. |
| Keshtgar [49] | Children with intractable FI/constipation following anorectal malformation repair |
| Children with high malformations excluded due to inclusion of patients >18 years of age; heterogenous cohort with respect to malformation and primary repair types; idiosyncratic classification of malformations (high or low) |
| Kimura [27] | Infants managed for high anorectal malformation |
| Limited by technology used; minimal description of manometry techniques and interpretation; 17-year study period introduces potential confounding factors related to other treatment advances; shorter mean follow up following laparoscopic procedure (11.8 versus 4.3 years). |
| Kudou [28] | Children following LAARP or PSARP for management of high anorectal malformation |
| Small cohort; LAARP group significantly younger at evaluation. |
| Kumar [57] | Children with anorectal malformations following repair |
| Functional outcomes not reported/assessed in comparison to manometric findings; relatively small malformation/age subgroups. |
| Langemeijer [29] | Patients with high malformation following PSARP |
| Limited by technology available; limited description of manometry technique and interpretation; limited manometric assessment performed; statistical assessment of correlation between manometry findings/function not performed/reported. |
| Leung [70] | Children >5 years old with FI following anorectal malformation repair |
| Small cohort; manometry not performed in all patients; limited manometric assessment performed, with limited description of equipment, technique, and interpretation. |
| Lin [30] | Children with high or intermediate malformation following PSARP or R-APSA |
| Small cohort in the context of multiple operative subgroups; study-specific assessment of bowel function may limit comparability of findings. |
| Lin [31] | Patients with high or intermediate malformations following LAR or PSARP |
| Small operative sub-groups; assessment of bowel function based on stool frequency, without report of associated symptoms (e.g., constipation, FI). |
| Liu [32] | Patients with intermediate or high malformations following PSARP |
| Limited description of manometry technique/interpretation; manometry results compared with Modified Wingspread Scoring categories (e.g., “excellent”, “poor”), without definition of relationship to symptoms (e.g., constipation, FI). |
| Martins [50] | Patients with intermediate or high malformations following PSARP |
| Limited by technology available; study-specific continence assessment may limit comparability of findings; limited reporting of manometry findings. |
| Mert [55] | Children following anorectal malformation repair, able to cooperate during anorectal manometry without neurological or neurosurgical disorders |
| Small cohort in the context of the wide age range and heterogenous malformation types; limited description of cohort characteristics. |
| Mollard [75] | Patients with intermediate or high malformations following repair |
| Small cohort; manometry performed in sub-cohort, with group characteristics not detailed; statistical assessment of correlation between manometry findings and bowel function not reported; limited by technology available. |
| Nagashima [62] | Children following repair of anorectal malformations |
| Small cohort given heterogenous nature of malformation types and patient ages; limited by technology available; study-specific scoring system lacks specificity, may limit comparability. |
| Niedzielski [33] | Children following PSARP |
| Wide age range/time elapsed post-operatively at manometric assessment; limited description of manometric technique; statistical assessment of correlation of manometric outcomes with bowel function not reported/performed. |
| Ninan [71] | Children undergoing levatorplasty for management of FI following anorectal malformation repair |
| Small study; limited by technology available; no description of manometry technique or equipment; limited reporting of manometry findings/interpretation. |
| Okada [21] | Patients following ASARP for re-operation due to FI following anorectal malformation repair |
| Small manometry cohort (n = 6); limited by available technology; assessment of correlation between manometry findings and symptoms not performed; cohort characteristics and bowel function scores provided for total cohort only. |
| Penninckx [16] | Infants with anorectal malformation treated at a single center |
| Limited description of manometry technique and interpretation; select group underwent post-operative assessment; infants with perineal anus (surrounded by EAS) of almost normal caliber used as controls; limited by technology available. |
| Ray [76] | Children with intermediate or high malformation, following PSARP |
| Limited description of manometry technique, assessment, interpretation, and outcome; limited by technology available; statistical assessment of correlation between manometry findings and functional outcomes not performed/reported; limited cohort characteristics provided. |
| Ren [34] | Children with intermediate malformations following SILAARP or PSARP |
| Manometry not performed in all patients; limited description of manometry technique and interpretation |
| Rintala [35] | Patients with intermediate or high malformations following repair |
| Sedation differed between groups (Group 1 were sedated, Group 2 were not); Group 2 were older (mean 3.1 versus 8.8 years); statistical assessment of correlation between manometry findings and function not performed/reported; limited by technology available. |
| Rintala [36] | Patients with intermediate or high malformations |
| Limited by technology available; limited description of cohort characteristics, including age at assessment and outcome with respect to function. |
| Rintala [58] | Patients with intermediate or high malformations |
| Limited by technology available; limited description of cohort characteristics, including age at assessment; study-specific rating of bowel function may limit comparability. |
| Rintala [17] | Patients with intermediate or high anorectal malformations |
| Small cohort; limited by technology available; limited description of cohort characteristics, including function; limited manometry data reported. |
| Rintala [59] | Patients following PSARP for intermediate and high malformations |
| Limited by technology available; heterogenous cohort; manometry and assessment of function appear to have been performed at different time points. |
| Rintala [60] | Patients undergoing secondary PSARP for intractable FI following primary anorectal malformation repair |
| Small cohort; limited by technology available; limited description of manometry technique/interpretation; statistical assessment of correlation with clinical function scores not performed/reported. |
| Ruttenstock [18] | Patients with an externally accessible fistula |
| Small cohort; limited by technology available. |
| Sangkhathat [63] | Infants less than three years of age, post-anoplasty for treatment of anorectal malformation |
| Limited characterization of bowel function; limited description of associated anomalies, including spinal anomalies. |
| Schuster [19] | Patients managed for perineal fistula using anal transposition technique |
| Small cohort; unclear whether post-operative manometry results were provided (assessed pre- and post-operatively). |
| Schuster [42] | Children with anorectal malformations following PSARP |
| Small cohort; range of anorectal malformation types further restricts subgroup size. |
| Senel [51] | Children with anorectal malformations following repair |
| Small, heterogenous cohort; limited description of associated anomalies (including spinal); function reported as summative scores of assessment instruments, which may limit comparability. |
| Sonnino [37] | Children with FI treated with gracilis muscle transposition |
| Small, heterogenous cohort; limited description of manometry outcomes; limited statistical analysis reported to aid interpretation of the significance of findings. |
| Tang [52] | Children with defecation disorders |
| Small anorectal malformation sub-cohort (n = 6); lack of normative 3D HRAM data in children. |
| Tong [38] | Infants with high anorectal malformation treated with LAARP vs. PSARP |
| Choice of intervention based on surgeon and/or parent preference (non-randomized); statistical assessment of correlation between clinical score and manometry findings not reported. |
| Vital Junior [53] | Children with anorectal malformation following PSARP |
| Limited description of malformation type; idiosyncratic aspects of continence assessment may impact upon the comparability of findings. |
| Wang [54] | Children treated at a single center without congenital megarectum, sacral or spinal deformities |
| Limited reporting of manometry findings; limited description of manometry parameters/interpretation utilized; heterogenous cohort. |
| Yang [39] | Children with high anorectal malformation following PSARP or LAARP |
| Small sub-cohorts; association between functional outcomes and manometry findings reported without assessment of statistical correlation; relatively short follow up period and young cohort age given reported associations between anorectal manometry findings and functional outcomes. |
| First Author | Year | Assessment | Post-Operative Bowel Function |
|---|---|---|---|
| Arnoldi [14] | 2014 | Rintala score: normal (≥18), good (12–17), fair (7–11), poor (≤6). Evaluated: frequency of defecation, FI, constipation, awareness, social problems. Scores ≤ 18 classified as pathological. | Normal (≥18): 17/30 (57%). Pathological (12–17): 43%. No patient scored ≤ 11. Normal scores correlated with absence of neurospinal dysraphism and neonatal colostomy. No correlation between normal scores and malformation type or operative timing. |
| Banasiuk [64] | 2021 | Classified according to Rome III criteria into asymptomatic (A), non-retentive fecal incontinence (NRFI), constipated (C), and retentive fecal incontinence (RFI). | A: 0 (0%); NRFI: 5 (41.7%); RFI: 4 (33.3%); C: 3 (25%) |
| Becmeur [23] | 2001 | Clinical continence score. Components: ability to hold back defecation, feels the need to defecate, frequency of defecation, staining, accidents, constipation, social problems, appearance. | Group A (primary three-flap anoplasty): 16.1 (1998), 15.7 (1999) Group B (re-do three-flap anoplasty): 11.5 (1998), 15 (1999) Higher scores in children without associated anomalies: 19.6 versus 10 (p = 0.02). Healthy controls: 22.5 |
| Bhat [56] | 2008 | Kelly score: poor (0–2); fair (3–4); good (5–6). Components: continence, staining of underwear, sphincter squeeze. | Median: 4 (range 1–6). |
| Burjonrappa [61] | 2010 | Modified Wingfield score (MWS) for fecal continence: normal function = 0, constipation/fecal incontinence = 1, intermittent fecal incontinence = 2, continuous fecal incontinence = 3. | Prior to excision of megarectum: MWS 3 Post-op: low malformations: normal (0) 6/8; (1) 1/8; 2 1/8; high malformations: normal (0) 4/6; (1) 2/6 |
| Cahill [24] | 1985 | Not reported. | “Normal continence” achieved in 3/6 patients. |
| Caldaro [43] | 2012 | Modified Wingfield score: fecal continence graded as normal function (0); constipation (1); intermittent soiling >3 episodes per week (2); daily soiling (3). | Constipation: 6/17; fecal incontinence: 11/17. |
| Caruso [67] | 2015 | Abbreviated Baylor Continence Scale: score 0 (good continence)–24 (severe incontinence). | Group 1: pre-treatment 11.2 ± 0.8; post-treatment 4.7 ± 2.5 (p = 0.008) Group 2: pre-treatment 14.8 ± 1.1; post-treatment 7.5 ± 3.1 (p = 0.027) Group 3: pre-treatment 18.6 ± 1.2; post-treatment 13.3 ± 3.6 (p = 0.027) Group 4: pre-treatment 22.0 ± 1.8; post-treatment 17.5 ± 3.1 (p = 0.066) |
| Caruso [72] | 2021 | Rintala continence score: 0 (very bad) to 20 (excellent). | 0 month: severe FI; 1 month: 6.14 ± 1.34; 3 months: 9.8 ± 1.57; 6 months: 16.8 ± 2.2 |
| Chen [73] | 1998 | Normal: >4 years post-repair with 1–3 bowel actions daily, no FI. Mild constipation: bowel action 2–3 daily, cisapride or laxatives but without enemas, resolving with 1–2 years of conservative treatment. Severe constipation: bowel movements dependent on medication and/or enemas > 2 years post-repair. Soiling: bowel action >4 times per day, with constant or intermittent staining of underwear > 2 years post-repair. | LSARP (low anomalies). Constipation: 10/28 (35.7%); >2 years 3/25; fecal incontinence: 1/23 (4.3%); normal function: 20/23 (86.9%) PSARP (intermediate–high anomalies). Constipation: 18/25 (72.0%); >2 years 10/25; fecal incontinence: 6/22 (27.3%); normal function: 11/22 (50%) R-ASPA (intermediate—high anomalies): normal function: 5/5 (100%) |
| Chung [22] | 2018 | Bowel function score (maximum total score: 20): normal ≥18. Constipation defined according to Rome III criteria. | PSARP: median 12.5 (8–18); normal BFS 42.9%. LAARP: median 16 (10–20); normal BFS 62.5%. |
| Doolin [44] | 1993 | Clinical assessment of the following variables: (1) continence (A, incontinent; B, spotting; C, continent); (2) enema (A, none; B, occasional; C, daily); (3) rectal tone (A, none; B, fair; C, normal); and (4) sensation (A, yes; B, no). | (1) Continence: A, incontinent (7, 29%); B, spotting (9, 37%); C, continent (8, 33%) (2) Enemas: A, none (7, 29%); B, occasional (5, 20%); C, daily (12, 50%) (3) Rectal tone: A, none (1, 4%); B, fair (23, 92%); C, normal (1, 4%) (4) Sensation: A, yes (25, 100%); B, no (0, 0%) |
| El-Debeiky [25] | 2009 | Questionnaire (parent report), including Kelly Score. | Kelly score: 3–5. Fecal incontinence: 3/9. |
| Emblem [40] | 1994 | Wingspread classification: continence assessed using a rating scale (1 clean–4 constant fecal incontinence). | (1) Clean: 11; (2) staining: 3; (3) intermittent fecal soiling: 2; (4) constant soiling: 0. |
| Emblem [45] | 1997 | Continence scale (1–4): (1) continent for liquids, solids, and gas; (2) occasionally incontinent for loose stools; (3) incontinent for loose and sometimes solid stools; (4) incontinent for loose and solid stools. | Significantly better continence demonstrated following repair of low malformations (males: 1.3; 95% CI 0.7–1.8 versus females: 1.9; 95% CI 1.4–2.4) than intermediate/high malformations (3.0; 95% CI 2.5–3.5). |
| Fukata [41] | 1997 | Kelly score (max. score 6): (1) control of feces and bowel habits; (2) absence of fecal staining; (3) sling action of puborectalis. 39 | Cohort: 4 (2–6); high malformation: 4 (3–5); intermediate malformation: 4 (2–6). Summarized as median Kelly score. |
| Hedlund [46] | 1992 | Soiling, constipation, diarrhea (grade 0–3); voluntary bowel actions. | Soiling: grade 1 (11/30); grade 1 (13/30); grade 2 (2/30); grade 3 (4/30). Constipation: grade 1 (13/30); grade 1 (8/30); grade 2 (9/30); grade 3 (0/30). Diarrhea: grade 1 (29/30); grade 1 (0/30); grade 2 (1/30); grade 3 (0/30). |
| Heikenen [74] | 1999 | - | All had FI refractory to medical therapy; however, bowel function not further defined. |
| Hettiarachchi [47] | 2002 | Modified Wingfield score | Median 3 (range 1–3). |
| Huang [20] | 2017 | Krickenbeck classification | Significantly lower incidence of FI (p = 0.049) and grade 2 or 3 constipation (p = 0.049, in the modified-PSARP group. |
| Husberg [26] | 1992 | (1) Continent; (2) minor soiling; (3) frequent soiling; (4) FI. | Positive RAIR: normal 11/15; minor soiling 3/15; frequent soiling 1/15; constipation management 10/15. Negative RAIR: minor soiling 3/6; frequent soiling 2/6; FI 1/6. |
| Ishihara [48] | 1987 | - | Translevator type: normal defecation 9/9. Intermediate type: normal defecation 2/6; constipation 2/6; incontinence 2/6. Supralevator type: normal defecation 7/23; constipation 10/23; incontinence 6/23. |
| Iwai [65] | 1997 | Kelly score | Improvement in Kelly score post biofeedback: 5/14. |
| Iwai [66] | 2007 | Japanese Study Group for Anorectal Malformation Scoring System: (1) rectal sensation; (2) constipation; (3) FI; (4) soiling. Score: good (7–8); fair (4–6); poor (0–3). | Pre-intervention: 4.5 ± 1.3 Post-intervention: 6.0 ± 1.2 |
| Iwai [68] | 1993 | Kelly score | Pre-biofeedback: median 1.5 (range 0–4); post-biofeedback: median 3 (range 1–4). |
| Iwai [15] | 1988 | Kelly score | Low anomaly: median 6 (range 4–6); intermediate: 4.5 (3–6); high: 4 (1–6). |
| Keshtgar [69] | 2008 | Modified Wingfield score | Isolated anorectal anomaly: median 1 (range 1–3). Associated megarectum and/or neuropathy: median 3 (range 1–3). |
| Keshtgar [49] | 2007 | Modified Wingfield score | Pre-operative: mean 3 (range 3–3). Post-operative: mean 0 (range 0–3). |
| Kimura [27] | 2010 | Japanese Study Group for Anorectal Malformation Scoring System: (1) fecal sensation; (2) constipation; (3) FI; (4) soiling. Score: good (7–8); fair (4–6); poor (0–3). | Open anorectoplasty: poor 1/14 (7.1%); fair 10/14 (71.4%); good 3/14 (21.4%). Lap-anorectoplasty: poor 0/5 (0%); fair 4/5 (80%); good 1/5 (20%). |
| Kudou [28] | 2005 | Kelly clinical score | LAARP: 3.8 ± 1.3. PSARP: 3.4 ± 0.8. |
| Kumar [57] | 2010 | - | - |
| Langemeijer [29] | 1991 | Presence and frequency of soiling; incontinence: soiling >1/day. | Continent: 3/50; intermittent incontinence: 7/50; incontinent: 24/50; constipation: 2/50; pseudo-continence (with enemas): 20/50. |
| Leung [70] | 2006 | Soiling frequency rank; Rintala continence score. | Pre-intervention: soiling frequency rank: 1.62; mean Rintala score: 11.6 Post-intervention: soiling frequency rank: 2.59 (six month), 2.85 (twelfth month); mean Rintala score: 12.9 (six month), 13.5 (twelfth month) |
| Lin [30] | 1996 | (1) Continent with constipation; (2) continent without constipation; (3) occasional soiling (<3/week); (4) incontinent (>4/week). | |
| Lin [31] | 2003 | Frequency of bowel actions: <1/day; 1–4/day; >5/day. | PSARP: <1/day 3/13 (23%); 1–4/day 7/13 (54%); >5/day 3/13 (23%). LAR: <1/day: 1/9 (11%); 1–4/day 7/9 (78%); >5/day 1/9 (11%). |
| Liu [32] | 2004 | Modified Wingspread score: excellent–poor outcome. Constipation: <3 bowel actions/week, rectal impaction, or fecal mass. Continence: ability to stay clean without staining or soiling. FI: regular loss of solid feces. Soiling: loss of small amounts of feces. | Group 1 (PSARP): constipation 23/48; soiling/FI: 23/48. Good–excellent score: 28/48 (58.3%). Group 2 (1-stage PSARP): constipation 29/65; soiling/FI: 33/65. Good–excellent score: 35/65 (53.8%) |
| Martins [50] | 1996 | Clinical + manometric assessment: (1) continent: 1–2 bowel actions/day without FI, good upper and lower rectal contractions; (2) partially continent: 3–5 bowel actions/day with frequent soiling or rectal prolapse, with moderate upper or lower rectal contractions; (3) incontinent: >5 bowel actions/day, constant FI, large anal opening, and light or no upper or lower rectal contractions. | Continent: 13/27 (1 with sacral malformation, 12 without sacral malformations). Partially continent: 7/27 (3 with sacral malformations, 4 without sacral malformations). Incontinent: 7/27 (6 with sacral malformations, 1 without sacral malformation). |
| Mert [55] | Holschneider’s questionnaire (HQ); Rintala’s questionnaire (RQ); Krickenbeck’s questionnaire (KQ), and Peña’s questionnaire (PQ). | Summary statistics not provided (see paper, Table 2). | |
| Mollard [75] | Clinical assessment: subjective parent report. | Fecal incontinence: 1/13 (cloacal malformation); constipation resolving within 1 post-operative year: 12/13. | |
| Nagashima [62] | Clinical classification: (1) normal bowel function; (2) FI: incontinence >2/week; (3) constipation: enema required daily to achieve bowel action. | Normal: 18/32 (5 high malformation, 4 intermediate malformation, 9 low malformation) FI: 12/32 (10 high malformation, 2 intermediate malformation) Constipation: 2/32 (high malformation). | |
| Niedzielski [33] | Modified Kelly score. Assessed: frequency of stools (0–2 pts); stool consistency (0–2 pts); staining (0–2 pts); need for treatment (drugs, enemas, diapers) (0–2 pts); rectoanal inhibitory reflex on manometry (0 or 2 pts). Score: good (10–8); satisfactory (7–4); poor (0–3). | Good: 83/91 (91.2%); fair 5/91 (5.5%); unsatisfactory 3/91 (3.3%). | |
| Ninan [71] | 1994 | Clinical assessment (excellent, improved, poor). Criteria not reported. | Pre-levatorplasty: persistent FI in all patients. Post-levatorplasty: excellent 6/13 (46%); improved 5/13 (39%); poor 2/13 (15%). |
| Okada [21] | 1993 | Kelly score: poor (0–2); fair (3–4); good (5–6). | Poor: 7/10; fair: 3/10; good: 0/10. |
| Penninckx [16] | 1986 | - | - |
| Ray [76] | 2004 | Kiesewetter criteria | Intermediate anomalies: continent. High anomalies: poor continence in 50%. |
| Ren [34] | 2019 | Krickenbeck classification | Comparable rates of voluntary bowel movements, constipation, and FI between SILAARP and PSARP groups. |
| Rintala [35] | 1990 | Clinical assessment: degree of soiling; medication requirement. (1) Good: voluntary bowel movements without medication or FI; (2) fair: minor FI or clean with oral medication; (3) poor: daily FI or enema dependent. | Group 1 (PSARP, Stephens): good (6/14); fair (4/14); poor (4/14). Group 2 (sacroabdominoperineal ± PSARP redo): good (0/16); fair (10/16); poor (6/16). |
| Rintala [36] | 1995 | - | - |
| Rintala [58] | 1993 | Clinical assessment of constipation, soiling, voluntary bowel movements. Constipation graded 0 (no constipation)–3 (severe, unmanageable). | Constipation requiring management: 26/40 (65%). FI: 4/33 (12%) with functioning IAS (determined by RAIR); 5/7 (71%) without. |
| Rintala [17] | 1990 | - | - |
| Rintala [59] | 1995 | Clinical scoring of anorectal function, determined from hospital records. Maximum score = 20. | Excellent: 16/46 (35%; mean 18.4 ± 0.6). Good: 16/46 (35%; mean 13.2 ± 2.0). Fair: 10/46 (22%; mean 8.8 ± 1.4). Poor: 4/46 (9%; mean 7.5 ± 1.7). Intermediate vs. high malformation: mean 16.1 ± 4.2 vs. mean 12.9 ± 3.9. |
| Rintala [60] | 1995 | Modified Holschneider score. Components: frequency of defecation, stool consistency, soiling, sensation, urgency, discrimination of bowel contents, need for care. Poor (0–4); fair (5–9); good (10–14). | Pre-operative: 7.8 ± 1.3. Post-operative: 10.1 ± 1.6. |
| Ruttenstock [18] | 2013 | Krickenbeck outcome assessment. | All patients demonstrated voluntary bowel movements with no FI. Constipation (Krickenbeck grade 2): 3/12. |
| Sangkhathat [63] | 2004 | Patients classified as constipated (<1 bowel action/day, laxative/enema requirement and/or grey discoloration or hard feces) or not constipated. | Constipation: 8/24 (33%). |
| Schuster [19] | 2000 | - | - |
| Schuster [42] | 2001 | Modified Kelly score (maximum total score 14): frequency of bowel movements, stool consistency, soiling, sensation, feeling of fullness, warning period, need for bowel care | Good (10–14): 4/17; fair (5–9): 6/17; poor (0–5): 7/17. |
| Senel [51] | 2007 | Kelly clinical score and Kiesewetter-Chang score (good: continent; fair: socially continent; poor: incontinent). | Kelly score: median 5 (range 0–6). Kiesewetter-Chang: good 14/18 (78%); fair 3/18 (17%); poor 1/18 (5%). |
| Sonnino [37] | 1991 | Clinical evaluation: (1) soiling, (2) necessity for diapers, (3) dietary requirements. | Continent: 4/7; occasional soiling (<2 episodes/week): 3/7. |
| Tang [52] | 2017 | Rintala score | Mean 18.3 (range 17–20). |
| Tong [38] | 2011 | Kelly score. Components: FI, fecal staining, sphincter squeeze. | LAARPT: 3.52 ± 1.42. PSARP: 3.49 ± 0.82 |
| Vital Junior [53] | 2007 | Continent (1–2 bowel actions/day, no FI, good sphincter contractility); partially continent (3–5 bowel actions/day, frequent FI, upper and lower sphincter contractility only); or fecally incontinent (>5 bowel actions/day, constant FI, abnormal anal appearance absent or weak contractions of the sphincter complex). | Continent: 31 (37.8%); partially continent: 21 (25.6%); incontinent: 30 (36.6%). |
| Wang [54] | 2016 | Scoring system, including (1) desire to defecate, (2) constipation, and (3) FI. Anal function rated as: good (5–6 points), intermediate (3–4 points), or poor (0–2 points). | Good (5–6 points): 29 children (61.7%); intermediate (3–4 points): 13 children (27.7%); and poor (1–2 points): 5 patients (10.6%). |
| Yang [39] | 2009 | Kelly score. Components: continence, staining, squeezing force. | LAARPT: 3.91 ± 1.14 (good: 4; fair: 5; poor: 2). PSARP: 3.83 ± 1.40 (good: 4; fair: 6; poor: 2). |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Evans-Barns, H.M.E.; Tien, M.Y.; Trajanovska, M.; Safe, M.; Hutson, J.M.; Dinning, P.G.; King, S.K. Post-Operative Anorectal Manometry in Children following Anorectal Malformation Repair: A Systematic Review. J. Clin. Med. 2023, 12, 2543. https://doi.org/10.3390/jcm12072543
Evans-Barns HME, Tien MY, Trajanovska M, Safe M, Hutson JM, Dinning PG, King SK. Post-Operative Anorectal Manometry in Children following Anorectal Malformation Repair: A Systematic Review. Journal of Clinical Medicine. 2023; 12(7):2543. https://doi.org/10.3390/jcm12072543
Chicago/Turabian StyleEvans-Barns, Hannah M. E., Melissa Y. Tien, Misel Trajanovska, Mark Safe, John M. Hutson, Phil G. Dinning, and Sebastian K. King. 2023. "Post-Operative Anorectal Manometry in Children following Anorectal Malformation Repair: A Systematic Review" Journal of Clinical Medicine 12, no. 7: 2543. https://doi.org/10.3390/jcm12072543