
Outcomes in Patients with Pulmonary Arterial Hypertension Underwent Transcatheter Closure of an Atrial Septal Defect
 , , , and
, , , and
Abstract
:1. Introduction
2. Methods
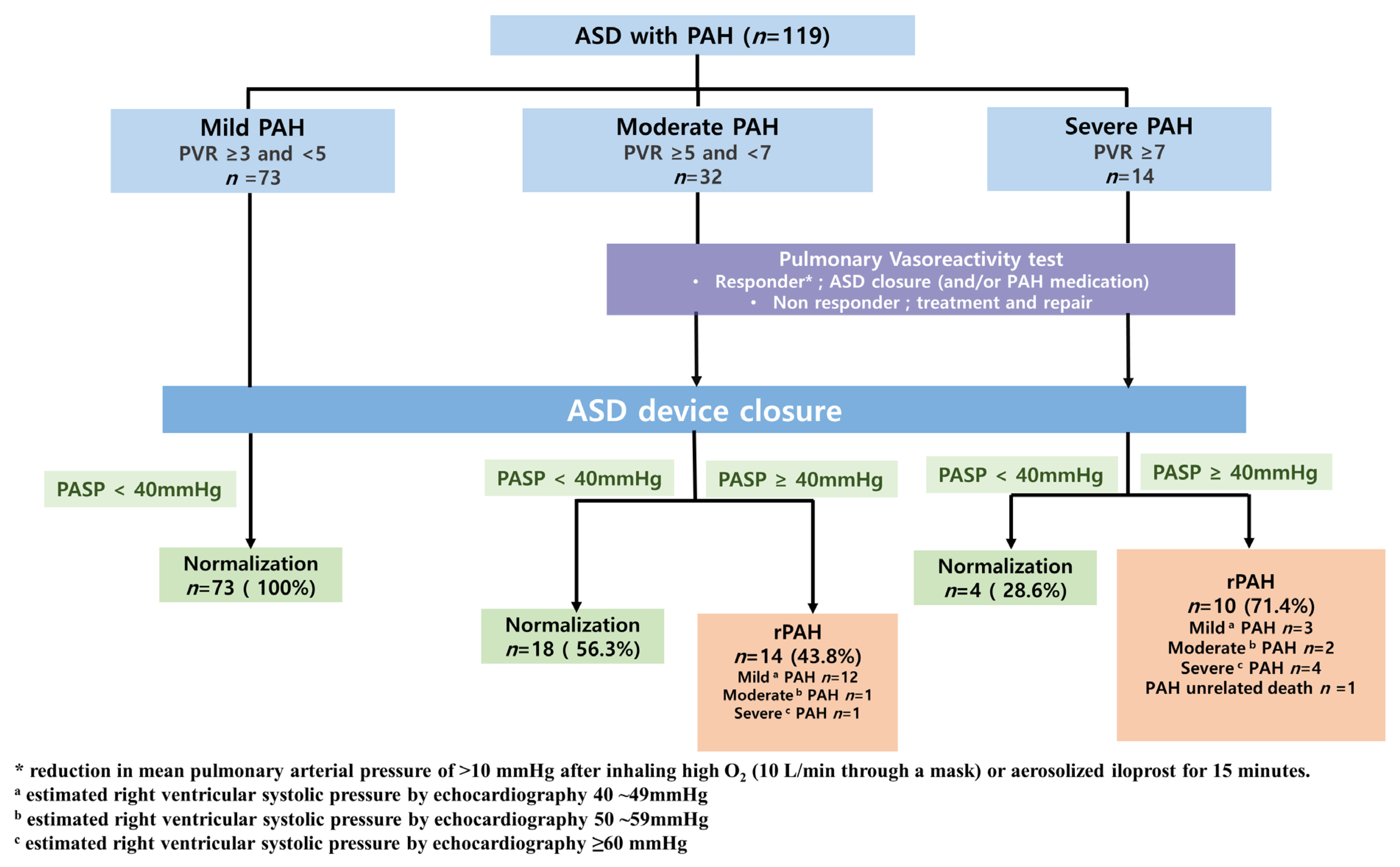
2.1. Patient Selection
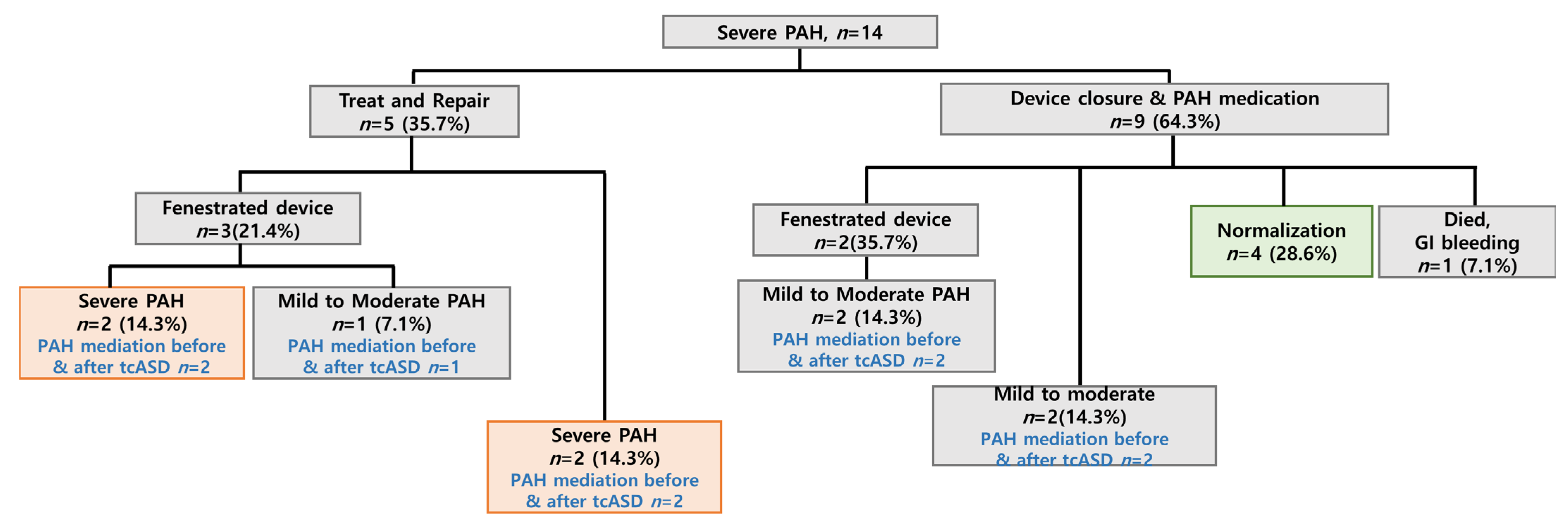
2.2. Personalized Treatment Strategies
2.3. Follow-Up
2.4. Statistical Analysis
2.5. Ethics Statement
3. Results
3.1. Ethics Statement
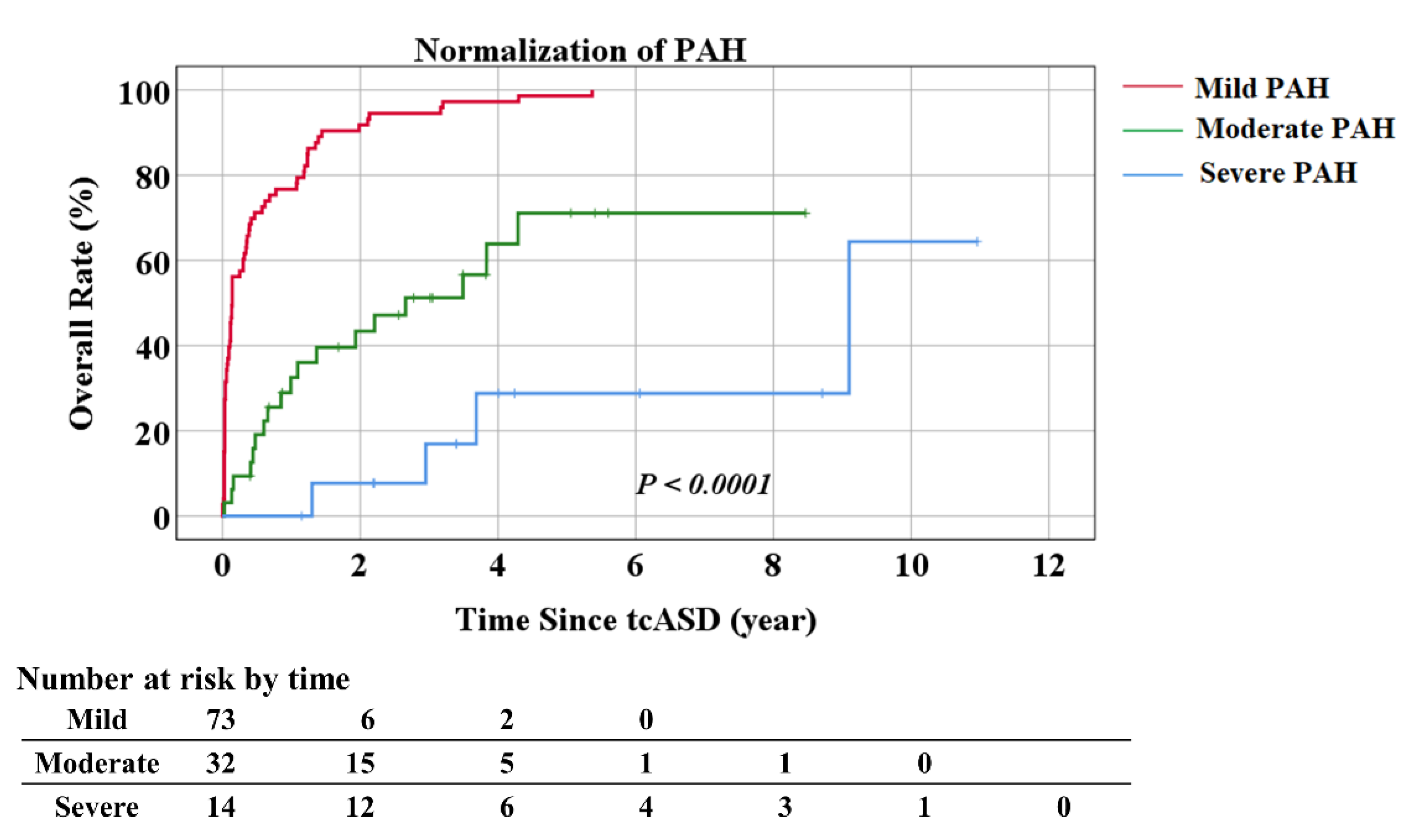
3.2. Treatment Outcomes Post-tcASD
3.3. Factors Associated with PAP Normalization
4. Discussion
5. Study Limitations
6. Conclusions
7. Patients
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Van Der Linde, D.; Konings, E.E.; Slager, M.A.; Witsenburg, M.; Helbing, W.A.; Takkenberg, J.J.; Roos-Hesselink, J.W. Birth prevalence of congenital heart disease worldwide: A systematic review and meta-analysis. J. Am. Coll. Cardiol. 2011, 58, 2241–2247. [Google Scholar] [CrossRef] [Green Version]
- Vogel, M.; Berger, F.; Kramer, A.; Alexi-Meshkishvili, V.; Lange, P.E. Incidence of secondary pulmonary hypertension in adults with atrial septal or sinus venosus defects. Heart 1999, 82, 30–33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Craig, R.J.; Selzer, A. Natural History and Prognosis of Atrial Septal Defect. Circulation 1968, 37, 805–815. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zwijnenburg, R.D.; Baggen, V.J.; Geenen, L.W.; Voigt, K.R.; Roos-Hesselink, J.W.; Bosch, A.E.V.D. The prevalence of pulmonary arterial hypertension before and after atrial septal defect closure at adult age: A systematic review. Am. Heart J. 2018, 201, 63–71. [Google Scholar] [CrossRef] [PubMed]
- Varma, C.; Benson, L.N.; Silversides, C.; Yip, J.; Warr, M.R.; Webb, G.; Siu, S.; McLaughlin, P.R. Outcomes and alternative techniques for device closure of the large secundum atrial septal defect. Catheter. Cardiovasc. Interv. 2004, 61, 131–139. [Google Scholar] [CrossRef]
- Gabriels, C.; De Meester, P.; Pasquet, A.; De Backer, J.; Paelinck, B.P.; Morissens, M.; Van De Bruaene, A.; Delcroix, M.; Budts, W. A different view on predictors of pulmonary hypertension in secundum atrial septal defect. Int. J. Cardiol. 2014, 176, 833–840. [Google Scholar] [CrossRef]
- D’Alto, M.; Mahadevan, V.S. Pulmonary arterial hypertension associated with congenital heart disease. Eur. Respir. Rev. 2012, 21, 328–337. [Google Scholar] [CrossRef] [Green Version]
- Baumgartner, H.; De Backer, J. The ESC Clinical Practice Guidelines for the Management of Adult Congenital Heart Disease 2020. Eur. Heart J. 2020, 41, 4153–4154. [Google Scholar] [CrossRef]
- Stout, K.K.; Daniels, C.J.; Aboulhosn, J.A.; Bozkurt, B.; Broberg, C.S.; Colman, J.M.; .Crumb, S.R.; Dearani, J.A.; Fuller, S.; Gurvitz, M.; et al. 2018 AHA/ACC Guideline for the Management of Adults With Congenital Heart Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2019, 73, e81–e192. [Google Scholar] [CrossRef]
- Takaya, Y.; Akagi, T.; Sakamoto, I.; Kanazawa, H.; Nakazawa, G.; Murakami, T.; Yao, A.; Nanasato, M.; Saji, M.; Hirokami, M.; et al. Efficacy of treat-and-repair strategy for atrial septal defect with pulmonary arterial hypertension. Heart 2022, 108, 382–387. [Google Scholar] [CrossRef]
- Constantine, A.; Dimopoulos, K. Evaluating a strategy of PAH therapy pre-treatment in patients with atrial septal defects and pulmonary arterial hypertension to permit safe repair (“treat-and-repair”). Int. J. Cardiol. 2019, 291, 142–144. [Google Scholar] [CrossRef] [PubMed]
- Kijima, Y.; Akagi, T.; Takaya, Y.; Akagi, S.; Nakagawa, K.; Kusano, K.; Sano, S.; Ito, H. Treat and Repair Strategy in Patients With Atrial Septal Defect and Significant Pulmonary Arterial Hypertension. Circ. J. 2016, 80, 227–234. [Google Scholar] [CrossRef] [Green Version]
- Yong, G.; Khairy, P.; De Guise, P.; Dore, A.; Marcotte, F.; Mercier, L.A.; Noble, S.; Ibrahim, R. Pulmonary arterial hypertension in patients with transcatheter closure of secundum atrial septal defects: A longitudinal study. Circ. Cardiovasc. Interv. 2009, 2, 455–462. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Veldtman, G.R.; Razack, V.; Siu, S.; El-Hajj, H.; Walker, F.; Webb, G.D.; Benson, L.N.; McLaughlin, P.R. Right ventricular form and function after percutaneous atrial septal defect device closure. J. Am. Coll. Cardiol. 2001, 37, 2108–2113. [Google Scholar] [CrossRef] [Green Version]
- Monte, I.P.; Tropea, L.R.; Tamburino, C.; Deste, W.; Lavanco, V.; Mangiafico, S. Long-term results after percutaneous closure of atrial septal defect: Cardiac remodeling and quality of life. J. Cardiovasc. Echogr. 2013, 23, 53–59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kefer, J.; Sluysmans, T.; Hermans, C.; El Khoury, R.; Lambert, C.; Van De Wyngaert, F.; Ovaert, C.; Pasquet, A. Percutaneous transcatheter closure of interatrial septal defect in adults: Procedural outcome and long-term results. Catheter. Cardiovasc. Interv. 2012, 79, 322–330. [Google Scholar] [CrossRef]
- Altindag, T.; Roos-Hesselink, J.; Cuypers, J.; Van Domburg, R.; De Jaegere, P.; Meijboom, F.; Witsenburg, M. Transcatheter device closure of atrial septal defects in patients aged 40 years and older. Neth. Heart J. 2010, 18, 537–542. [Google Scholar] [CrossRef]
- Akseer, S.; Horlick, E.; Vishwanath, V.; Hobbes, B.; Huszti, E.; Mak, S.; Lee, D.S.; Abrahamyan, L. Prevalence and outcomes of pulmonary hypertension after percutaneous closure of atrial septal defect: A systematic review and meta-analysis. Eur. Respir. Rev. 2020, 29, 200099. [Google Scholar] [CrossRef]
- McQuillan, B.M.; Picard, M.H.; Leavitt, M.; Weyman, A.E. Clinical Correlates and Reference Intervals for Pulmonary Artery Systolic Pressure Among Echocardiographically Normal Subjects. Circulation 2001, 104, 2797–2802. [Google Scholar] [CrossRef] [Green Version]
- Balint, O.H.; Samman, A.; Haberer, K.; Tobe, L.; McLaughlin, P.; Siu, S.C.; Horlick, E.; Granton, J.; Silversides, C.K. Outcomes in patients with pulmonary hypertension undergoing percutaneous atrial septal defect closure. Heart 2008, 94, 1189–1193. [Google Scholar] [CrossRef]
- Schubert, S.; Peters, B.; Abdul-Khaliq, H.; Nagdyman, N.; Lange, P.; Ewert, P. Left ventricular conditioning in the elderly patient to prevent congestive heart failure after transcatheter closure of atrial septal defect. Catheter. Cardiovasc. Interv. 2005, 64, 333–337. [Google Scholar] [CrossRef] [PubMed]
- Al-Hindi, A.; Cao, Q.L.; Hijazi, Z.M. Transcatheter closure of secundum atrial septal defect in the elderly. J. Invasive Cardiol. 2009, 21, 70–75. [Google Scholar] [PubMed]
- Berner, M.; Beghetti, M.; Spahr-Schopfer, I.; Oberhansli, I.; Friedli, B. Inhaled nitric oxide to test the vasodilator capacity of the pulmonary vascular bed in children with long-standing pulmonary hypertension and congenital heart disease. Am. J. Cardiol. 1996, 77, 532–535. [Google Scholar] [CrossRef]
- Joung, B.; Lee, J.M.; Lee, K.H.; Kim, T.-H.; Choi, E.-K.; Lim, W.-H.; Kang, K.-W.; Shim, J.; Lim, H.E.; Park, J.; et al. 2018 Korean Guideline of Atrial Fibrillation Management. Korean Circ. J. 2018, 48, 1033–1080. [Google Scholar] [CrossRef] [Green Version]
- Rudski, L.G.; Lai, W.W.; Afilalo, J.; Hua, L.; Handschumacher, M.D.; Chandrasekaran, K.; Solomon, S.D.; Louie, E.K.; Schiller, N.B. Guidelines for the echocardiographic assessment of the right heart in adults: A report from the American Society of Echocardiography endorsed by the European Association of Echocardiography, a registered branch of the European Society of Cardiology, and the Canadian Society of Echocardiography. J. Am. Soc. Echocardiogr. 2010, 23, 685–713. [Google Scholar] [PubMed]
- Nyboe, C.; Karunanithi, Z.; Nielsen-Kudsk, J.E.; Hjortdal, V.E. Long-term mortality in patients with atrial septal defect: A nationwide cohort-study. Eur. Heart J. 2018, 39, 993–998. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.K.; Chiu, S.N.; Lin, M.T.; Chen, C.A.; Lu, C.W.; Wu, M.H. Transcatheter Closure of Atrial Septal Defect Associated With Pulmonary Artery Hypertension using Fenestrated Devices. Am. J. Cardiol. 2021, 147, 122–128. [Google Scholar] [CrossRef] [PubMed]
- Satoh, A.; Katayama, K.; Hiro, T.; Yano, M.; Miura, T.; Kohno, M.; Fujii, T.; Matsuzaki, M. Effect of Right Ventricular Volume Overload on Left Ventricular Diastolic Function in Patients With Atrial Septal Defect. Jpn. Circ. J. 1996, 60, 758–766. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Variables | Group | p-Value | ||
|---|---|---|---|---|
| Mild (N = 73) | Moderate (N = 32) | Severe (N = 14) | Overall | |
| Age (years) at cath | 48.85 ± 13.03 | 50.48 ± 17.78 | 35.74 ± 13.47 | 0.0049 * |
| Wt (kg) | 61 (53, 70) | 54.5 (49.6, 63.0) | 51.5 (48.0, 57.0) | 0.0139 * |
| Ht (cm) | 161.68 ± 9.98 | 159.14 ± 7.74 | 160.50 ± 6.26 | 0.4159 |
| BSA (m2) | 1.68 ± 0.20 | 1.59 ± 0.17 | 1.58 ± 0.14 | 0.0369 * |
| Sex | 0.0479 * | |||
| Male | 23 (31.5) | 8 (25.0) | 0 (0.0) | |
| Female | 50 (68.5) | 24 (75.0) | 14 (100.0) | |
| Pre-procedural AFib | 13 (17.8) | 10 (31.3) | 5 (35.7) | 0.2360 |
| ASD_size (mm) | 26.34 ± 6.39 | 26.16 ± 6.77 | 24.29 ± 7.03 | 0.5604 |
| TR > GII | 10 (13.7) | 6 (19.4) | 2 (14.3) | 0.7596 |
| MR > GI | 13 (17.8) | 7 (22.6) | 1 (7.1) | 0.4559 |
| Pre-procedural echo RVSP | 43 (40, 52) | 59.5 (55.0, 67.0) | 89.5 (69.0, 110.0) | <0.0001 * |
| PASP (mmHg) | 45 (40, 50) | 60.0 (51.0, 64.5) | 85.5 (74.0, 100.0) | <0.0001 * |
| mPAP (mmHg) | 25 (25, 30) | 34 (30, 40) | 50 (42, 60) | <0.0001 * |
| Qp/Qs | 2.54 (2.13, 3.29) | 2.40 (1.93, 2.83) | 1.67 (1.40, 2.28) | 0.0009 * |
| PVR (WU) | 3.32 (3.15, 3.48) | 5.56 (5.30, 6.21) | 8.45 (8.17, 9.12) | <0.0001 * |
| NYHA | <0.0001 * | |||
| 1 | 43 (58.9) | 6 (19.4) | 1 (7.1) | |
| 2 | 25 (34.2) | 21 (67.7) | 7 (50.0) | |
| 3 | 5 (6.8) | 4 (12.9) | 5 (35.7) | |
| 4 | 0 (0.0) | 0 (0.0) | 1 (7.1) | |
| Group | p-Value | |||
|---|---|---|---|---|
| Variables | Mild (N = 73) | Moderate (N = 32) | Severe (N = 14) | Overall |
| Last follow-up RVSP | 32 (30, 33) | 36.0 (31.0, 40.5) | 50.5 (38.0, 69.0) | <0.0001 * |
| Normalization | 73 (100) | 18 (56.2) | 4 (28.6) | <0.0001 * |
| Time to normalization (months) | 1.68 (0.43, 8.21) | 11.04 (5.29, 26.51) | 39.79 (25.49, 76.70) | <0.0001 * |
| Persistent severe PAH | 2 (2.7) | 1 (3.2) | 3 (21.4) | 0.0274 * |
| Follow up months | 53.62 (23.77, 82.68) | 42.05 (29.84, 66.05) | 51.44 (40.70, 76.47) | 0.5870 |
| MACEs † | 6 (8.2) | 12 (37.5) | 8 (57.1) | <0.0001 * |
| Post-procedural AFib | 6 (8.2) | 5 (15.6) | 3 (21.4) | 0.2720 |
| Last NYHA | <0.0001 * | |||
| 1 | 57 (78.1) | 17 (54.8) | 6 (42.9) | |
| 2 | 15 (20.5) | 13 (41.9) | 4 (28.6) | |
| 3 | 1 (1.4) | 1 (3.2) | 4 (28.6) | |
| Pul.vasodilator at last follow-up | 0 (0.0) | 17 (53.1) | 10 (71.4) | <0.0001 * |
| Variables | Normalization | p-Value | |
|---|---|---|---|
| No (n = 24) | Yes (n = 95) | ||
| Age (years) | 58.66 (33.49, 69.41) | 47.64 (35.93, 57.82) | 0.1285 |
| Weight (kg) | 52.05 (48.85, 61.70) | 59.00 (52.00, 69.00) | 0.0484 * |
| Height (cm) | 159.33 ± 8.06 | 161.24 ± 9.29 | 0.3566 |
| BSA (m2) | 1.55 (1.46, 1.64) | 1.62 (1.53, 1.80) | 0.0471 * |
| ASD-size (mm) | 24.95 ± 7.70 | 26.33 ± 6.22 | 0.3623 |
| Sex | 0.5146 | ||
| Male | 5 (20.8) | 26 (27.4) | |
| Female | 19 (79.2) | 69 (72.6) | |
| TR > GII | 7 (29.2) | 11 (11.7) | 0.0525 |
| MR > G1 | 4 (16.7) | 17 (18.1) | >0.999 |
| PASP (mmHg) | 64.0 (54.5, 77.5) | 45.0 (40.0, 59.0) | <0.0001 * |
| mPAP (mmHg) | 39 (29, 50) | 27 (25, 30) | <0.0001 * |
| Qp/Qs | 2.19 (1.58, 2.74) | 2.46 (2.07, 3.13) | 0.0272 * |
| PVR (WU) | 6.45 (5.40, 8.45) | 3.40 (3.20, 4.85) | <0.0001 * |
| Device_size | 28.0 (22.0, 32.5) | 30.0 (26.0, 34.0) | 0.2433 |
| Pre-procedural AFib | 9 (37.5) | 19 (20.2) | 0.0980 |
| AFib at last follow-up | 5 (20.0) | 9 (9.6) | 0.1500 |
| MACEs | 10 (40.0) | 16 (17.0) | 0.0130 * |
| NYHA | <0.0001 * | ||
| 1 | 2 (8.3) | 48 (51.1) | |
| 2 | 13 (54.2) | 40 (42.6) | |
| 3 | 8 (33.3) | 6 (6.4) | |
| 4 | 1 (4.2) | 0 (0.0) | |
| Last NYHA | <0.0001 * | ||
| 1 | 7 (29.2) | 73 (77.7) | |
| 2 | 12 (50.0) | 20 (21.3) | |
| 3 | 5 (20.8) | 1 (1.1) | |
| Variables | OR | 95% CI Lower | 95% CI Upper | p-Value |
|---|---|---|---|---|
| Age (years) | 1.025 | 0.994 | 1.058 | 0.1149 |
| Weight (kg) | 0.984 | 0.955 | 1.013 | 0.2778 |
| Height (cm) | 0.976 | 0.928 | 1.027 | 0.3542 |
| BSA (m2) | 0.080 | 0.006 | 1.117 | 0.0604 |
| Sex | ||||
| 1: Male | 1 (ref) | |||
| 2: Female | 1.432 | 0.485 | 4.230 | 0.5162 |
| ASD_size | 0.968 | 0.904 | 1.037 | 0.3599 |
| Device_size | 0.952 | 0.890 | 1.018 | 0.1485 |
| PASP | 1.074 | 1.039 | 1.110 | <0.0001 * |
| Qp/Qs | 0.475 | 0.242 | 0.933 | 0.0306 * |
| PVR (WU) | 2.610 | 1.811 | 3.760 | <0.0001 * |
| TR > GII | 3.107 | 1.053 | 9.165 | 0.0400 * |
| MR > G1 | 0.906 | 0.274 | 2.993 | 0.8712 |
| pre-procedural AFib | 1.768 | 0.820 | 6.233 | 0.1790 |
| Post-procedural AFib | 1.365 | 0.750 | 4.27 | 0.2130 |
| Variables | OR | 95% CI Lower | 95% CI Upper | p-Value |
|---|---|---|---|---|
| Age | 1.114 | 1.051 | 1.180 | 0.0003 * |
| PVR | 4.605 | 2.548 | 8.323 | <0.0001 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Seol, J.-H.; Jung, S.-Y.; Lee, H.-B.; Kim, A.-Y.; Kim, E.-H.; Min, I.-K.; Kim, N.-K.; Choi, J.-Y. Outcomes in Patients with Pulmonary Arterial Hypertension Underwent Transcatheter Closure of an Atrial Septal Defect. J. Clin. Med. 2023, 12, 2540. https://doi.org/10.3390/jcm12072540
Seol J-H, Jung S-Y, Lee H-B, Kim A-Y, Kim E-H, Min I-K, Kim N-K, Choi J-Y. Outcomes in Patients with Pulmonary Arterial Hypertension Underwent Transcatheter Closure of an Atrial Septal Defect. Journal of Clinical Medicine. 2023; 12(7):2540. https://doi.org/10.3390/jcm12072540
Chicago/Turabian StyleSeol, Jae-Hee, Se-Yong Jung, Han-Byul Lee, Ah-Young Kim, Eun-Hwa Kim, In-Kyung Min, Nam-Kyun Kim, and Jae-Young Choi. 2023. "Outcomes in Patients with Pulmonary Arterial Hypertension Underwent Transcatheter Closure of an Atrial Septal Defect" Journal of Clinical Medicine 12, no. 7: 2540. https://doi.org/10.3390/jcm12072540