
Comparison between Fasting and Non-Fasting Cut-Off Values of Triglyceride in Diagnosing High Triglyceride in Chinese Hypertensive Outpatients
Abstract
:1. Introduction
2. Patients and Methods
2.1. Study Subjects
2.2. Specimen Collection
2.3. Laboratory Assays
2.4. Cut-Off Values to Determine HTG and HRC
2.5. Evaluation of Awareness and Acceptance of Non-Fasting Blood Lipid Tests in Chinese Outpatients
2.6. Statistical Analysis
3. Results
3.1. General Clinical Characteristics of Two Groups
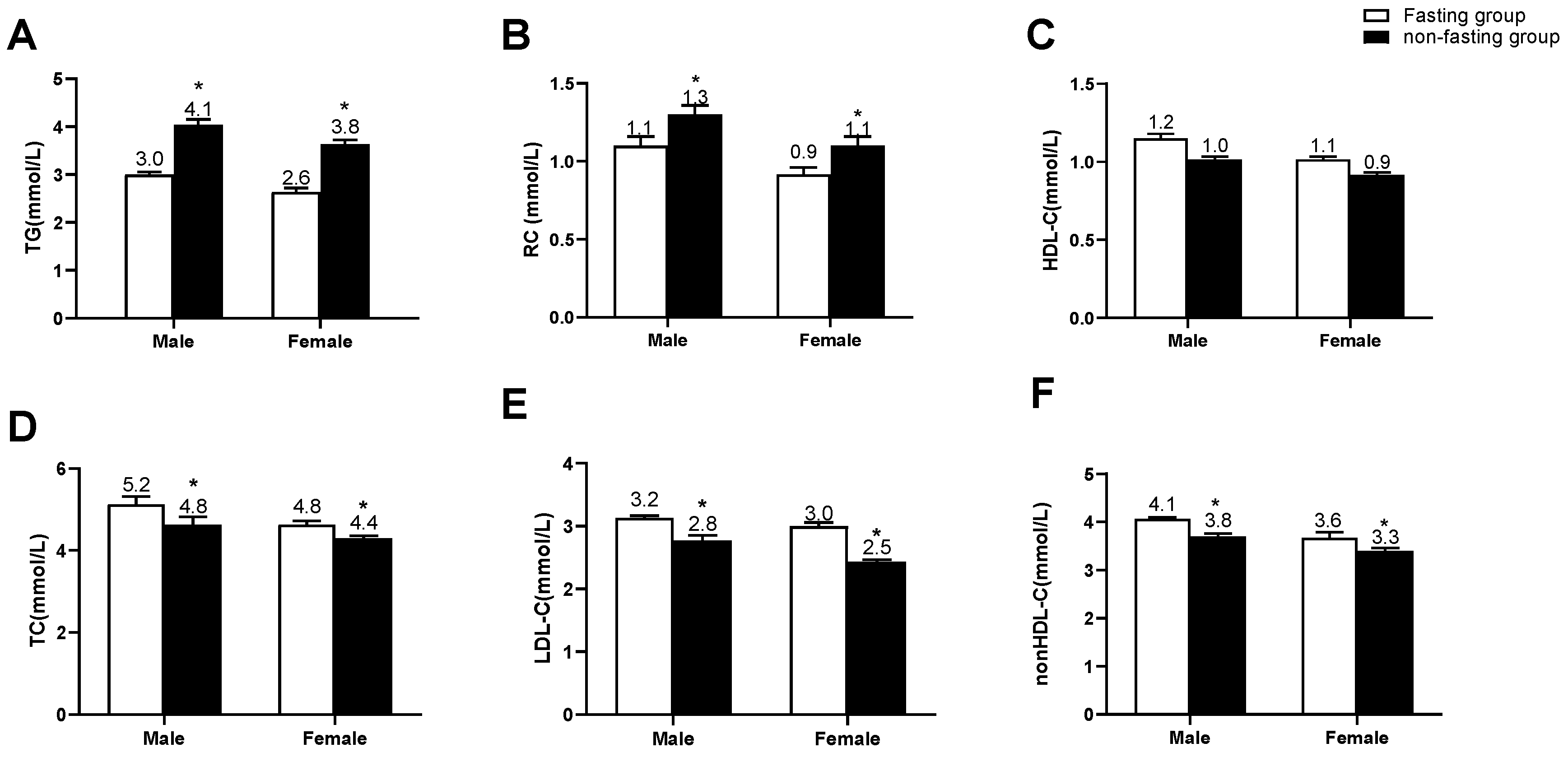
3.2. Comparison of Blood Lipid Levels between Two Groups
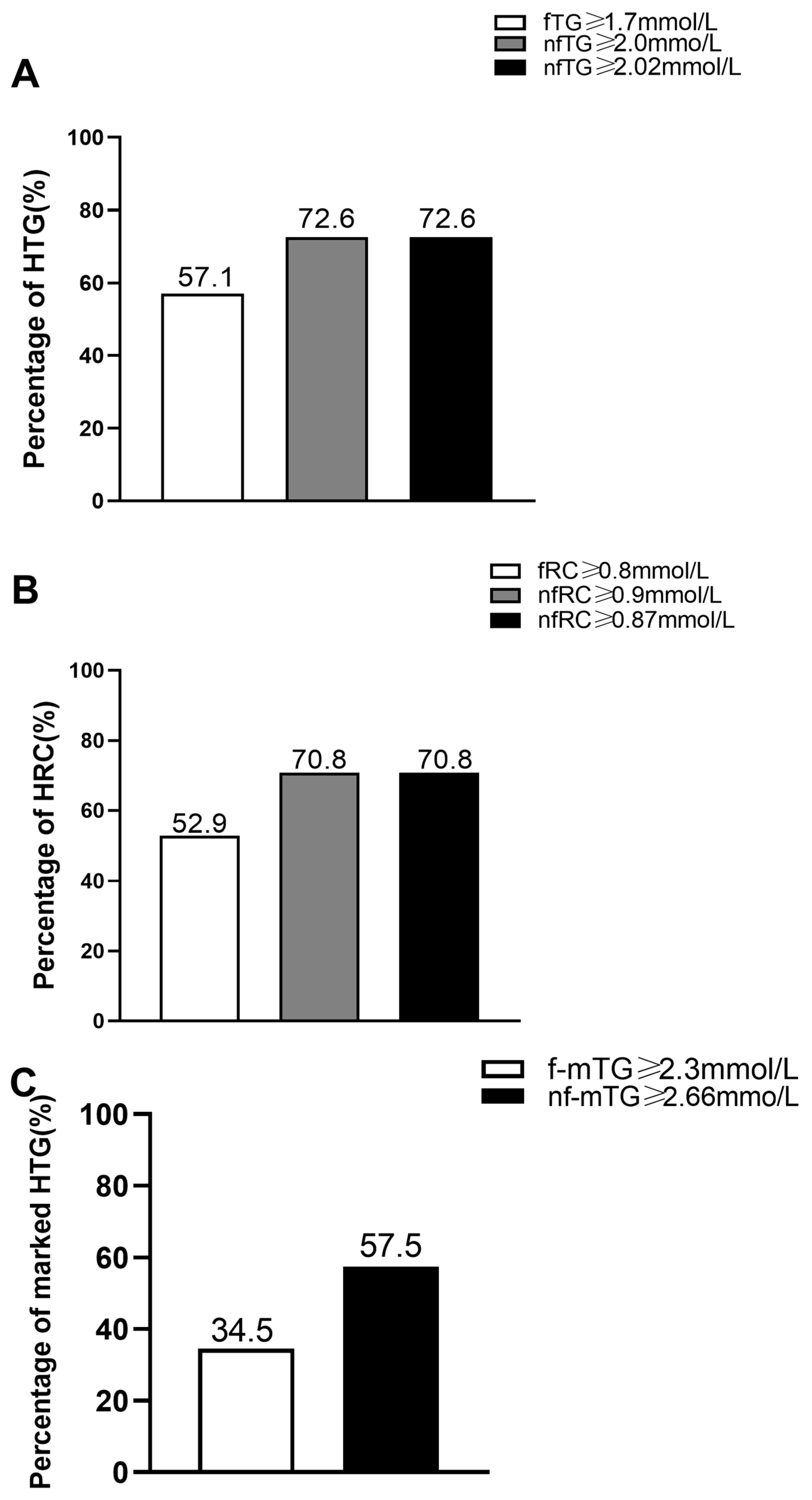
3.3. Comparisons of Percentages of HTG, HRC, and Marked HTG between Two Groups
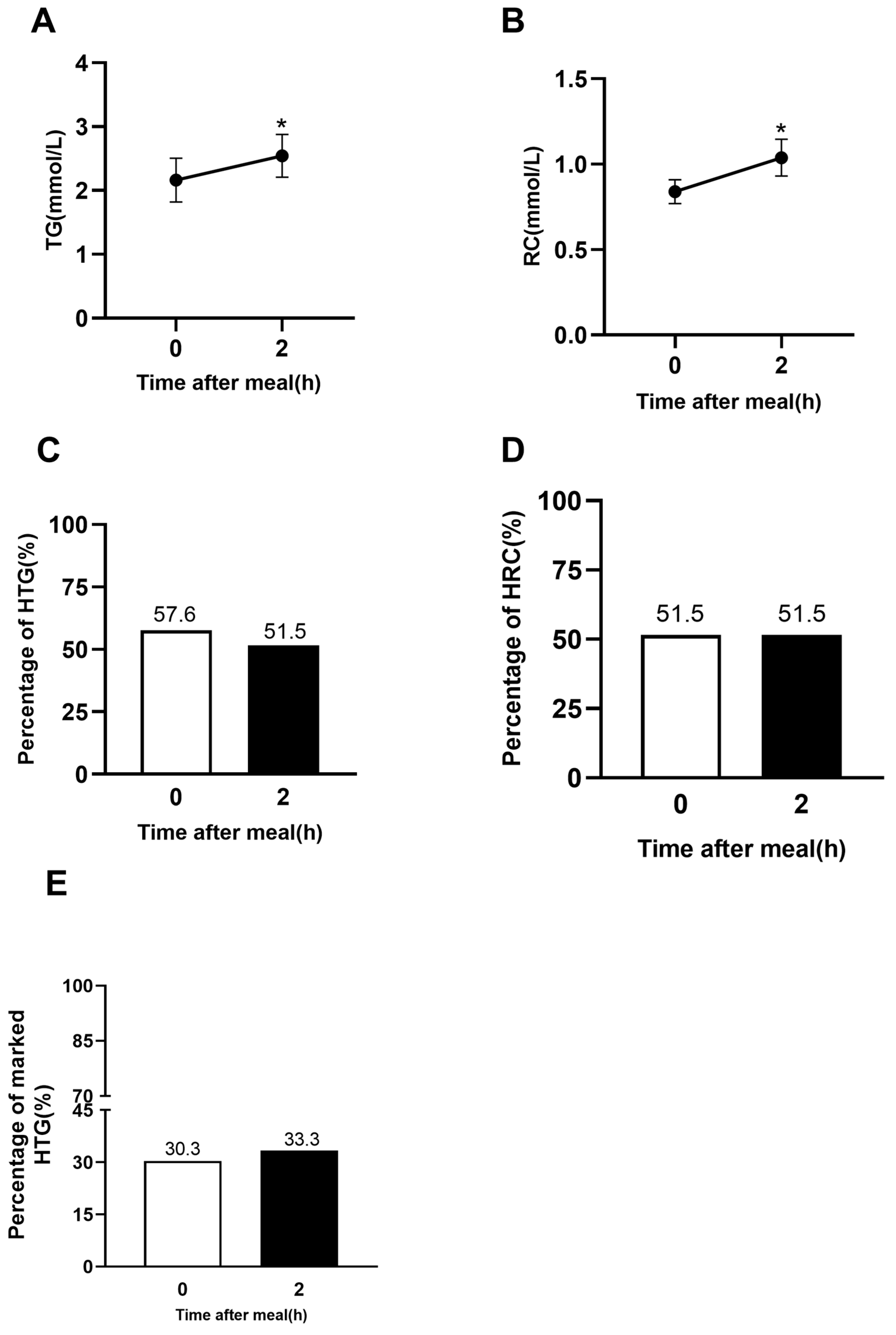
3.4. Comparisons of Blood Lipid Levels and Percentages of HTG, HRC, and Marked HTG before and after a Daily Meal in 33 Outpatients
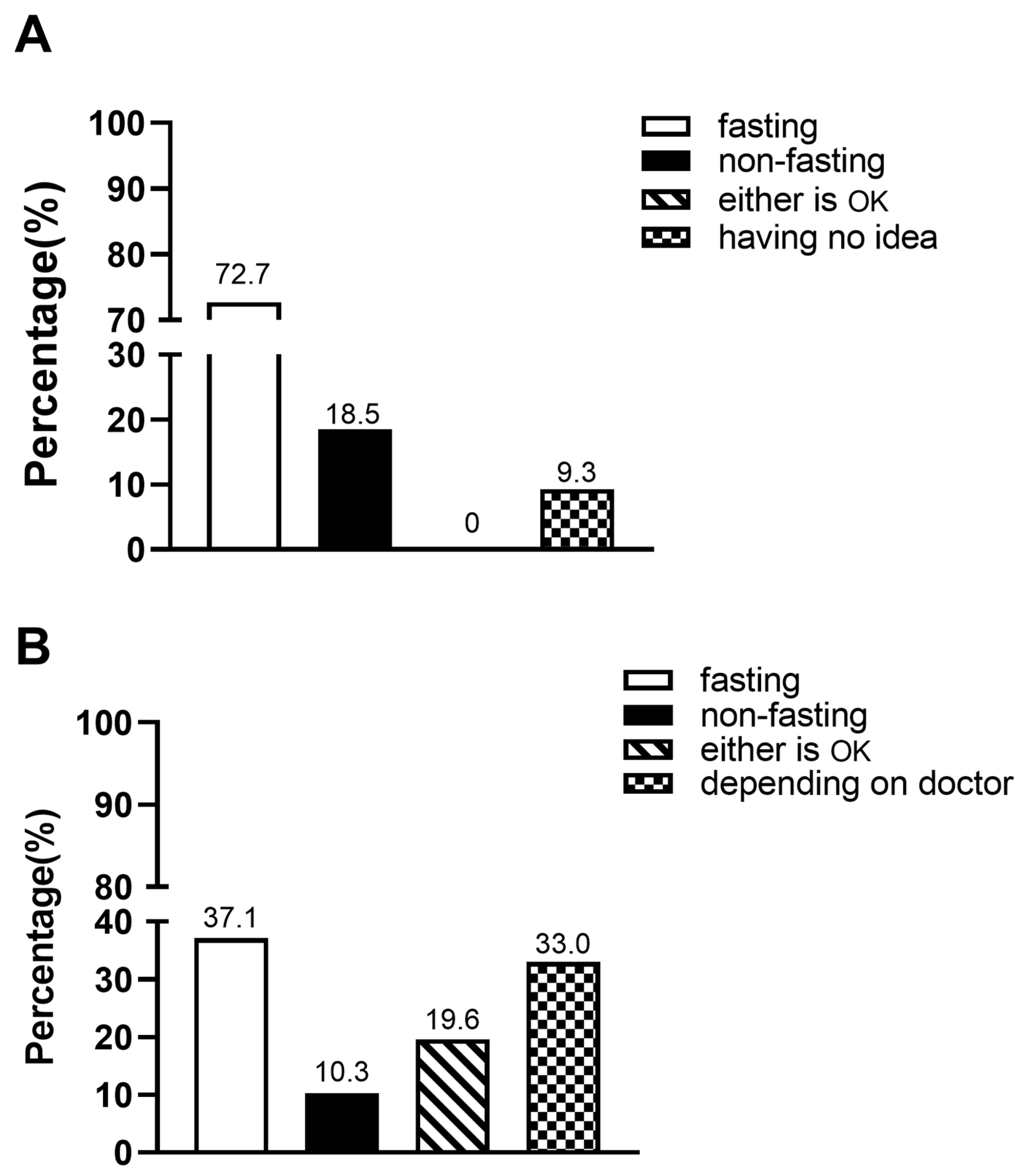
3.5. Awareness and Acceptance of Non-Fasting Lipid Test
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sander, G.E.; Giles, T.D. Hypertension and lipids: Lipid factors in the hypertension syndrome. Curr. Hypertens. Rep. 2002, 4, 458–463. [Google Scholar] [CrossRef] [PubMed]
- Dolgalev, I.V.; Brazovskaya, N.G.; Ivanova, A.Y.; Shipkhineeva, A.Y.; Bogajchuk, P.M. Impact of hypertension, overweight, hypertriglyceridemia and their combination for mortality rate according to the results of a 27-year cohort prospective study. Kardiologiia 2019, 59, 44–52. [Google Scholar] [CrossRef] [PubMed]
- Ling, Y.; Jiang, J.; Wu, B.; Gao, X. Serum triglyceride, high-density lipoprotein cholesterol, apolipoprotein B, and coronary heart disease in a Chinese population undergoing coronary angiography. J. Clin. Lipidol. 2017, 11, 646–656. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.; Zhang, H.; Lu, J.; Ding, Q.; Li, X.; Wang, X.; Sun, D.; Tan, L.; Mu, L.; Liu, J.; et al. Prevalence of Dyslipidemia and Availability of Lipid-Lowering Medications Among Primary Health Care Settings in China. JAMA Netw. Open 2021, 4, e2127573. [Google Scholar] [CrossRef] [PubMed]
- Tushuizen, M.E.; Pouwels, P.J.; Bontemps, S.; Rustemeijer, C.; Matikainen, N.; Heine, R.J.; Taskinen, M.R.; Diamant, M. Postprandial lipid and apolipoprotein responses following three consecutive meals associate with liver fat content in type 2 diabetes and the metabolic syndrome. Atherosclerosis 2010, 211, 308–314. [Google Scholar] [CrossRef]
- Hu, D.Y. New guidelines and evidence for the prevention and treatment of dyslipidemia and atherosclerotic cardiovascular disease in China. Zhonghua Xin Xue Guan Bing Za Zhi 2016, 44, 826–827. [Google Scholar] [CrossRef] [Green Version]
- Liu, L.; Zhao, S.P. Expert consensus on the non-fasting blood lipid detection and clinical application. Zhonghua Nei Ke Za Zhi 2021, 60, 400–405. [Google Scholar]
- Lee, J.S.; Chang, P.Y.; Zhang, Y.; Kizer, J.R.; Best, L.G.; Howard, B.V. Triglyceride and HDL-C Dyslipidemia and Risks of Coronary Heart Disease and Ischemic Stroke by Glycemic Dysregulation Status: The Strong Heart Study. Diabetes Care 2017, 40, 529–537. [Google Scholar] [CrossRef] [Green Version]
- Lamarche, B.; Tchernof, A.; Mauriege, P.; Cantin, B.; Dagenais, G.R.; Lupien, P.J.; Després, J.P. Fasting insulin and apolipoprotein B levels and low-density lipoprotein particle size as risk factors for ischemic heart disease. JAMA 1998, 279, 1955–1961. [Google Scholar] [CrossRef]
- Bansal, S.; Buring, J.E.; Rifai, N.; Mora, S.; Sacks, F.M.; Ridker, P.M. Fasting compared with nonfasting triglycerides and risk of cardiovascular events in women. JAMA 2007, 298, 309–316. [Google Scholar] [CrossRef] [Green Version]
- Nordestgaard, B.G.; Benn, M.; Schnohr, P.; Tybjærg-Hansen, A. Nonfasting triglycerides and risk of myocardial infarction, ischemic heart disease, and death in men and women. JAMA 2007, 298, 299–308. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bureau of Disease Prevention and Control, National Health Commission of People’s Republic of China; National Center for Cardiovascular Diseases; Chinese Academy of Medical Science & Peking Union Medical College, Fuwai Hospital; Chinese Center for Control and Prevention; Chinese Society of Cardiology; Chinese Medical Doctor Association Hypertension Committee; China Sport Science Society; Chinese Nutrition Society; Chinese Stroke Association; Editorial Board of Chinese Journal of Cardiology. National guideline for hypertension management in China (2019). Zhonghua Xin Xue Guan Bing Za Zhi 2020, 48, 10–46. [Google Scholar]
- Whelton, P.K.; Carey, R.M.; Aronow, W.S.; Casey, D.E.; Collins, K.J.; Dennison Himmelfarb, C.; DePalma, S.M.; Gidding, S.; Jamerson, K.A.; Jones, D.W.; et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2018, 71, e127–e248. [Google Scholar] [PubMed]
- Nordestgaard, B.G.; Langsted, A.; Mora, S.; Kolovou, G.; Baum, H.; Bruckert, E.; Watts, G.F.; Sypniewska, G.; Wiklund, O.; Borén, J.; et al. Fasting Is Not Routinely Required for Determination of a Lipid Profile: Clinical and Laboratory Implications Including Flagging at Desirable Concentration Cutpoints-A Joint Consensus Statement from the European Atherosclerosis Society and European Federation of Clinical Chemistry and Laboratory Medicine. Eur. Heart J. 2016, 37, 1944–1958. [Google Scholar] [PubMed] [Green Version]
- Xu, J.; Chen, Y.Q.; Zhao, S.P.; Liu, L. Determination of optimal cut-off points after a high-fat meal corresponding to fasting elevations of triglyceride and remnant cholesterol in Chinese subjects. Lipids Health Dis. 2019, 18, 206. [Google Scholar] [CrossRef] [Green Version]
- Xu, J.; Qu, P.; Du, X.; Xiang, Q.; Guo, L.; Zhu, L.; Tan, Y.; Fu, Y.; Wen, T.; Liu, L. Change in Postprandial Level of Remnant Cholesterol After a Daily Breakfast in Chinese Patients With Hypertension. Front. Cardiovasc. Med. 2021, 8, 685385. [Google Scholar] [CrossRef]
- Guo, L.L.; Zhu, L.Y.; Xu, J.; Xie, Y.Y.; Xiang, Q.Y.; Jiang, Z.Y.; Tan, Y.R.; Liu, L. Determination of the Optimal Cutoff Value of Triglyceride That Corresponds to Fasting Levels in Chinese Subjects With Marked Hypertriglyceridemia. Front. Cardiovasc. Med. 2021, 8, 736059. [Google Scholar] [CrossRef]
- Perez-Martinez, P.; Delgado-Lista, J.; Perez-Jimenez, F.; Lopez-Miranda, J. Update on genetics of postprandial lipemia. Atheroscler. Suppl. 2010, 11, 39–43. [Google Scholar] [CrossRef]
- Tian, F.; Xiang, Q.Y.; Zhang, M.Y.; Chen, Y.Q.; Lin, Q.Z.; Wen, T.; Liu, L. Changes in non-fasting concentrations of blood lipids after a daily Chinese breakfast in overweight subjects without fasting hypertriglyceridemia. Clin. Chim. Acta 2019, 490, 147–153. [Google Scholar] [CrossRef]
- Guo, L.L.; Chen, Y.Q.; Lin, Q.Z.; Tian, F.; Xiang, Q.Y.; Zhu, L.Y.; Xu, J.; Wen, T.; Liu, L. Non-HDL-C Is More Stable Than LDL-C in Assessing the Percent Attainment of Non-fasting Lipid for Coronary Heart Disease Patients. Front. Cardiovasc. Med. 2021, 8, 649181. [Google Scholar] [CrossRef]
- Lin, Q.; Fu, Y.; Zang, X.; Liu, Q.; Liu, L. The Role of Fasting LDL-C Levels in Their Non-fasting Reduction in Patients With Coronary Heart Disease. Front. Cardiovasc. Med. 2021, 8, 686234. [Google Scholar] [CrossRef] [PubMed]
- Langsted, A.; Freiberg, J.J.; Nordestgaard, B.G. Fasting and nonfasting lipid levels: Influence of normal food intake on lipids, lipoproteins, apolipoproteins, and cardiovascular risk prediction. Circulation 2008, 118, 2047–2056. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Langsted, A.; Nordestgaard, B.G. Nonfasting lipids, lipoproteins, and apolipoproteins in individuals with and without diabetes: 58,434 individuals from the Copenhagen General Population Study. Clin. Chem. 2011, 57, 482–489. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Du, X.; Zhang, S.L.; Liu, L. Association between remnant lipoprotein-cholesterol and coronary heart disease. Zhonghua Xin Xue Guan Bing Za Zhi 2016, 44, 657–660. [Google Scholar] [PubMed]
- Mooradian, A.D. Dyslipidemia in type 2 diabetes mellitus. Nat. Rev. Endocrinol. 2009, 5, 150–159. [Google Scholar] [CrossRef] [PubMed]
- Zhao, S.P.; Liu, L.; Cheng, Y.C.; Shishehbor, M.H.; Liu, M.H.; Peng, D.Q.; Li, Y.L. Xuezhikang, an extract of cholestin, protects endothelial function through antiinflammatory and lipid-lowering mechanisms in patients with coronary heart disease. Circulation 2004, 110, 915–920. [Google Scholar] [CrossRef] [Green Version]
- Ling, L.; Shuiping, Z.; Yanchun, C.; Yuling, L. Optimal time point to measure postprandial hypertriglyceridemia after a high-fat meal. Chin. J. Endocrinol. Metab. 2004, 20, 23–25. [Google Scholar]
- Yang, D.; Cai, Q.; Qi, X.; Zhou, Y. Postprandial Lipid Concentrations and Daytime Biological Variation of Lipids in a Healthy Chinese Population. Ann. Lab. Med. 2018, 38, 431–439. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Fasting Group (n = 119) | Postprandial Group (n = 106) | |
|---|---|---|
| Age (y) | 45.5 ± 10.6 | 46.0 ± 9.6 |
| Men, n (%) | 80 (67.2) | 71 (67.0) |
| BMI (kg/m2) | 27.1 ± 3.7 | 26.4 ± 3.8 |
| Waist (cm) | 94.1 ± 10.4 | 94.9 ± 11.8 |
| Current smoking, n (%) | 32 (26.9) | 15 (14.2) * |
| Central obesity, n (%) | 88 (74.0) | 75 (71) |
| CHD, n (%) | 5 (4.2) | 3 (2.8) |
| DM, n (%) | 6 (5.0) | 4 (3.8) |
| SBP (mm Hg) | 157.2 ± 22.5 | 154.6 ± 19.5 |
| DBP (mm Hg) | 98.1 ± 15.8 | 102.5 ± 88.7 |
| HR (bpm) | 85.3 ± 14.7 | 88.7 ± 14.4 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xie, Y.; Qu, P.; Guo, L.; Xu, J.; Zhu, L.; Tan, Y.; Wen, T.; Liu, L. Comparison between Fasting and Non-Fasting Cut-Off Values of Triglyceride in Diagnosing High Triglyceride in Chinese Hypertensive Outpatients. J. Clin. Med. 2023, 12, 2539. https://doi.org/10.3390/jcm12072539
Xie Y, Qu P, Guo L, Xu J, Zhu L, Tan Y, Wen T, Liu L. Comparison between Fasting and Non-Fasting Cut-Off Values of Triglyceride in Diagnosing High Triglyceride in Chinese Hypertensive Outpatients. Journal of Clinical Medicine. 2023; 12(7):2539. https://doi.org/10.3390/jcm12072539
Chicago/Turabian StyleXie, Yingying, Peiliu Qu, Liling Guo, Jin Xu, Liyuan Zhu, Yangrong Tan, Tie Wen, and Ling Liu. 2023. "Comparison between Fasting and Non-Fasting Cut-Off Values of Triglyceride in Diagnosing High Triglyceride in Chinese Hypertensive Outpatients" Journal of Clinical Medicine 12, no. 7: 2539. https://doi.org/10.3390/jcm12072539