
Robotic versus Open Pyeloplasty: Perioperative and Functional Outcomes

 ,
,  ,
,  ,
,  ,
,  , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
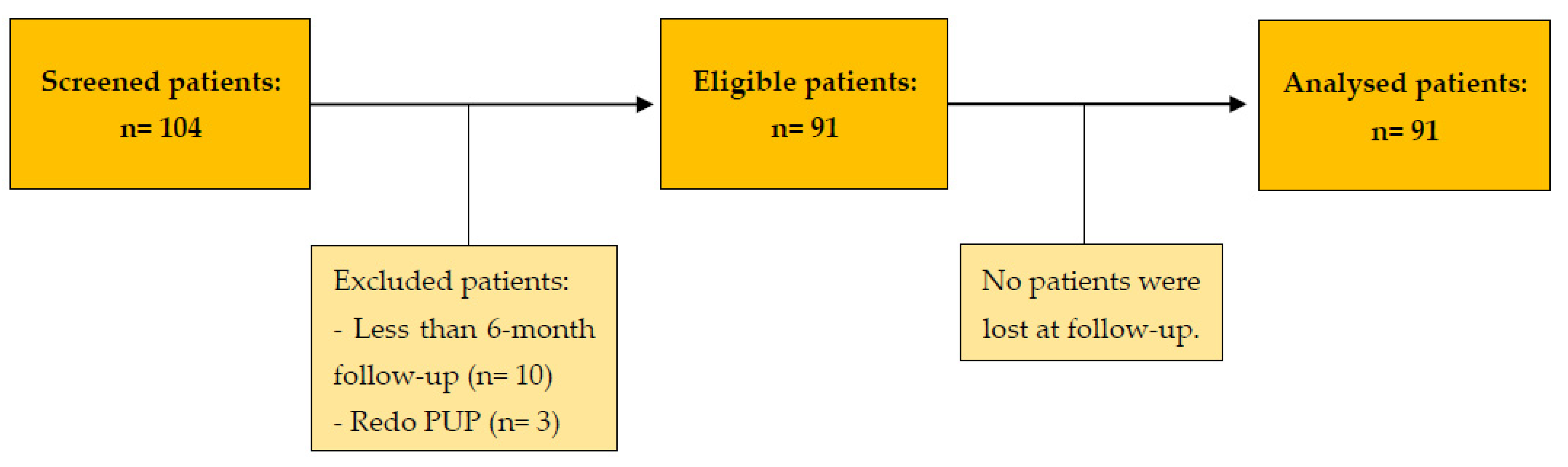
2.1. Study Design and Patient Recruitment
2.2. Data Collection
- Preoperative data: age, Charlson comorbidity index (CCI), body mass index (BMI), surgical history, and UPJO characteristics (side, signs and symptoms, preoperative and postoperative imaging, and prior nephrostomy or double-J stent).
- Intraoperative data: operating time, estimated bleeding, presence of crossing vessel or stones, complications, and conversion to open surgery.
- Postoperative data: length of hospital stay, analgesics and antibiotics requirement, early complications, late complications, and functional outcomes. All complications were classified with the Clavien–Dindo scale [13].
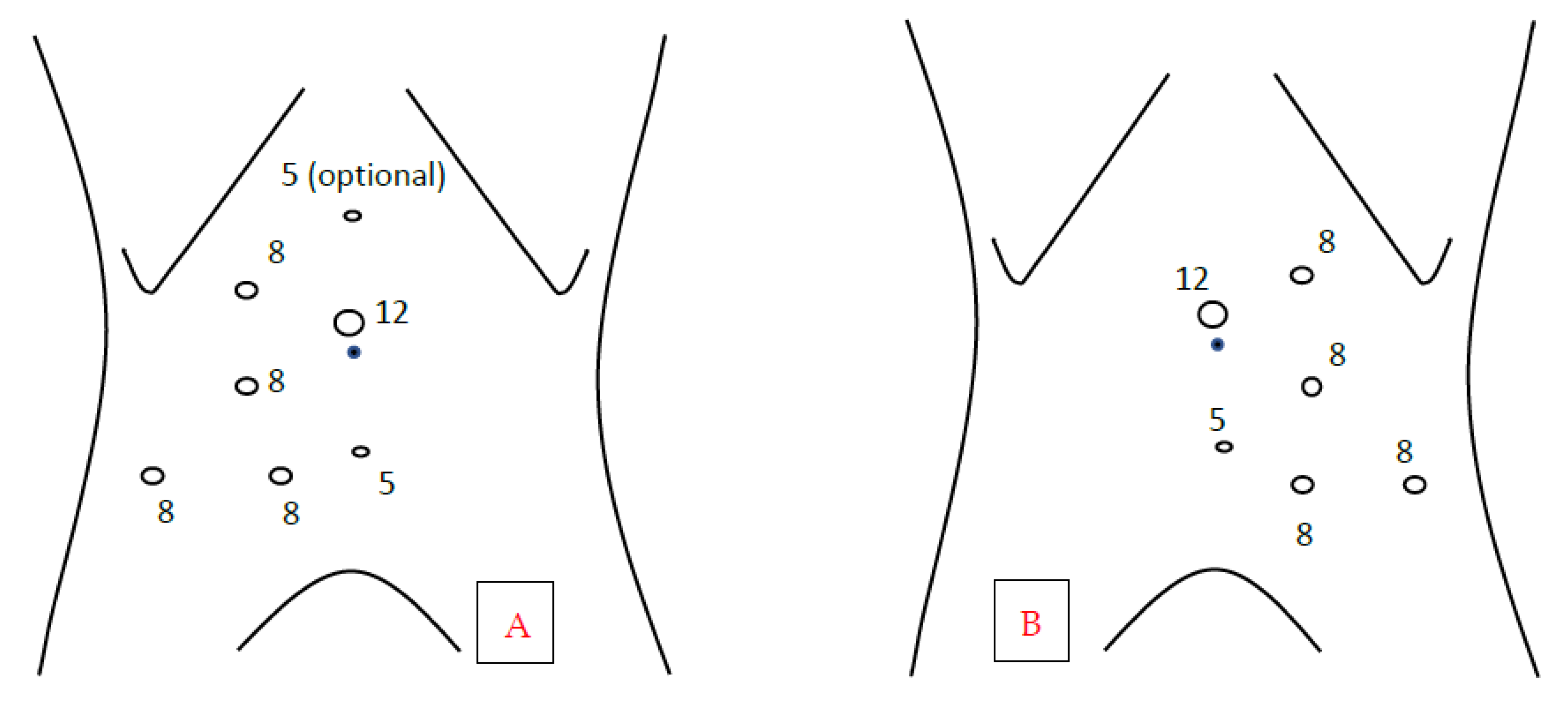
2.3. Patient Preparation and Positioning
2.4. Surgical Procedures
2.4.1. Open Pyeloplasty
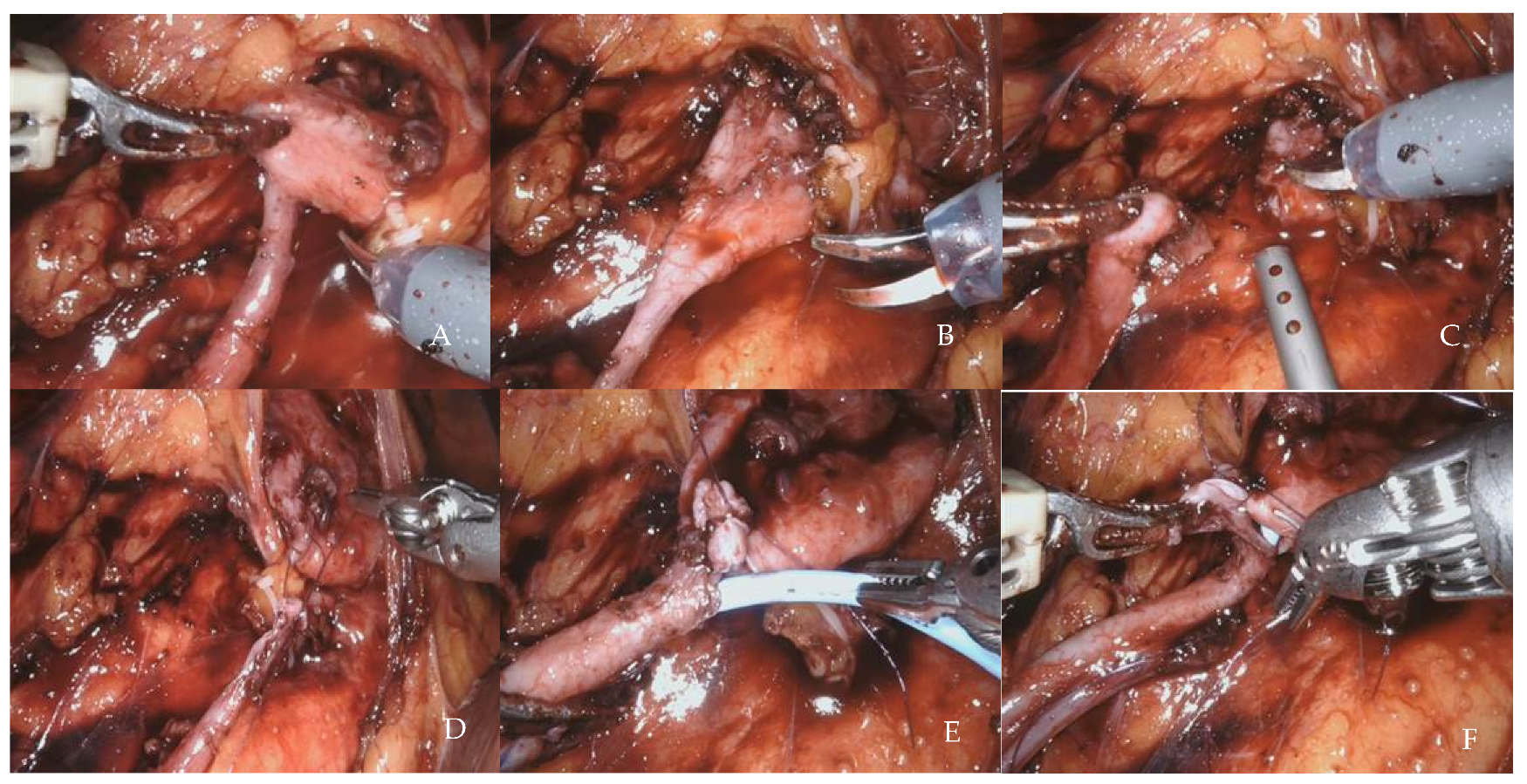
2.4.2. Robot-Assisted Laparoscopic Pyeloplasty
2.5. Postoperative Management and Follow Up
2.6. Primary Outcome
2.7. Secondary Outcomes
- -
- the cost of diagnostic procedures performed during hospitalization.
- -
- the cost of the hospital stay.
- -
- the cost of the operating room.
- -
- the cost of devices used for surgery (including robotic equipment).
2.8. Statistical Analysis
3. Results
3.1. Patient Demographics
3.2. Primary Outcome
3.3. Secondary Outcomes
3.4. Predictors of Failures
4. Discussion
- Early preoperative removal (at least four weeks before) of a previously positioned stent, eventually replaced with a nephrostomy tube, to avoid inflamed tissues at the level of the UPJ.
- Limited isolation of the ureter and in situ anastomosis to avoid devascularization.
- Wide pelvis isolation to improve its mobilization.
- No coagulation on the ureteral and pelvis section margins.
- Landmark stitch on the ureter to avoid ureteral twisting.
- About 15 mm length of ureteral spatulation and pelvis opening, not including the scarred tissue that can be used for ureteral manipulation.
- Do not incorporate too much ureteral mucosa into the suture to avoid narrowing the anastomosis.
- Tension-free, watertight, and intubated anastomosis, usually performing a running suture, but an interrupted anastomosis, is a good alternative if there is too much tension.
- Kidney–psoas hitching if necessary to ensure a tension-free anastomosis, especially in the case of inflamed tissues (previous pyelonephritis, stone disease, or stenting).
- Avoid pelvis resection to shorten the suture length (pelvis tailoring is usually unnecessary).
- Selection bias: we adopted extensive inclusion and exclusion criteria to include all patients undergoing pyeloplasty in our center.
- Observer bias: an independent researcher performed the assessment.
- Attrition bias: electronic medical record review of consecutive RALP and OP cases was performed based on a prospectively maintained database. We made numerous attempts to contact the patients if they could not be reached at the last follow-up, keeping the attrition bias to zero.
- Learning curve bias: we performed a supplementary analysis by removing the first five cases of each surgeon involved in RALP surgery, obtaining similar results.
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Uberoi, J.; Disick, G.I.S.; Munver, R. Minimally Invasive Surgical Management of Pelvic-Ureteric Junction Obstruction: Update on the Current Status of Robotic-Assisted Pyeloplasty. BJU Int. 2009, 104, 1722–1729. [Google Scholar] [CrossRef]
- Chow, A.K.; Rosenberg, B.J.; Capoccia, E.M.; Cherullo, E.E. Risk Factors and Management Options for the Adult Failed Ureteropelvic Junction Obstruction Repair in the Era of Minimally Invasive and Robotic Approaches: A Comprehensive Literature Review. J. Endourol. 2020, 34, 1112–1119. [Google Scholar] [CrossRef]
- Khan, F.; Ahmed, K.; Lee, N.; Challacombe, B.; Khan, M.S.; Dasgupta, P. Management of Ureteropelvic Junction Obstruction in Adults. Nat. Rev. Urol. 2014, 11, 629–638. [Google Scholar] [CrossRef] [PubMed]
- Ozayar, A.; Friedlander, J.I.; Shakir, N.A.; Gahan, J.C.; Cadeddu, J.A.; Morgan, M.S.C. Equivocal Ureteropelvic Junction Obstruction on Diuretic Renogram--Should Minimally Invasive Pyeloplasty Be Offered to Symptomatic Patients? J. Urol. 2015, 193, 1278–1282. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, B.L.; Lai, J.C.; Seelam, R.; Hanley, J.M.; Wolf, J.S.; Hollenbeck, B.K.; Hollingsworth, J.M.; Dick, A.W.; Setodji, C.M.; Saigal, C.S. Variation in the Use of Open Pyeloplasty, Minimally Invasive Pyeloplasty, and Endopyelotomy for the Treatment of Ureteropelvic Junction Obstruction in Adults. J. Endourol. 2017, 31, 210–215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lai, W.R.; Stewart, C.A.; Thomas, R. Technology Based Treatment for UreteroPelvic Junction Obstruction. J. Endourol. 2017, 31, S59–S63. [Google Scholar] [CrossRef] [Green Version]
- Pogorelić, Z.; Brković, T.; Budimir, D.; Todorić, J.; Košuljandić, Đ.; Jerončić, A.; Biočić, M.; Saraga, M. Endoscopic Placement of Double-J Ureteric Stents in Children as a Treatment for Primary Hydronephrosis. Can. J. Urol. 2017, 2, 8853–8858. [Google Scholar]
- Schuessler, W.W.; Grune, M.T.; Tecuanhuey, L.V.; Preminger, G.M. Laparoscopic Dismembered Pyeloplasty. J. Urol. 1993, 150, 1795–1799. [Google Scholar] [CrossRef]
- Yanke, B.V.; Lallas, C.D.; Pagnani, C.; Bagley, D.H. Robot-Assisted Laparoscopic Pyeloplasty: Technical Considerations and Outcomes. J. Endourol. 2008, 22, 1291–1296. [Google Scholar] [CrossRef]
- Gettman, M.T.; Neururer, R.; Bartsch, G.; Peschel, R. Anderson-Hynes Dismembered Pyeloplasty Performed Using the Da Vinci Robotic System. Urology 2002, 60, 509–513. [Google Scholar] [CrossRef]
- Mantica, G.; Ambrosini, F.; Parodi, S.; Tappero, S.; Terrone, C. Comparison of Safety, Efficacy and Outcomes of Robot Assisted Laparoscopic Pyeloplasty vs Conventional Laparoscopy. Res. Rep. Urol. 2020, 12, 555–562. [Google Scholar] [CrossRef] [PubMed]
- Patel, V. Robotic-Assisted Laparoscopic Dismembered Pyeloplasty. Urology 2005, 66, 45–49. [Google Scholar] [CrossRef] [PubMed]
- Clavien, P.A.; Barkun, J.; De Oliveira, M.L.; Vauthey, J.N.; Dindo, D.; Schulick, R.D.; de Santibañes, E.; Pekolj, J.; Slankamenac, K.; Bassi, C.; et al. The Clavien-Dindo Classification of Surgical Complications: Five-Year Experience. Ann. Surg. 2009, 250, 187–196. [Google Scholar] [CrossRef] [Green Version]
- Sivaraman, A.; Leveillee, R.J.; Patel, M.B.; Chauhan, S.; Bracho, J.E.; Moore, C.R.; Coelho, R.F.; Palmer, K.J.; Schatloff, O.; Bird, V.G.; et al. Robot-Assisted Laparoscopic Dismembered Pyeloplasty for Ureteropelvic Junction Obstruction: A Multi-Institutional Experience. Urology 2012, 79, 351–355. [Google Scholar] [CrossRef] [PubMed]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P.; STROBE Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for Reporting Observational Studies. J. Clin. Epidemiol. 2008, 61, 344–349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marien, T.; Bjurlin, M.A.; Wynia, B.; Bilbily, M.; Rao, G.; Zhao, L.C.; Shah, O.; Stifelman, M.D. Outcomes of Robotic-Assisted Laparoscopic Upper Urinary Tract Reconstruction: 250 Consecutive Patients. BJU Int. 2015, 116, 604–611. [Google Scholar] [CrossRef] [PubMed]
- Mufarrij, P.W.; Woods, M.; Shah, O.D.; Palese, M.A.; Berger, A.D.; Thomas, R.; Stifelman, M.D. Robotic Dismembered Pyeloplasty: A 6-Year, Multi-Institutional Experience. J. Urol. 2008, 180, 1391–1396. [Google Scholar] [CrossRef]
- Masieri, L.; Sforza, S.; Mari, A.; Morselli, S.; Tellini, R.; Di Maida, F.; Vignolini, G.; Serni, S.; Carini, M.; Minervini, A. Robot-Assisted Pyeloplasty for Ureteropelvic Junction Obstruction: Experience from a Tertiary Referral Center. Minerva Urol. E Nefrol. Ital. J. Urol. Nephrol. 2019, 71, 168–173. [Google Scholar] [CrossRef] [PubMed]
- Popelin, M.-B.; Pinar, U.; Benamran, D.; Ingels, A.; Parra, J.; Vaessen, C.; Seisen, T.; de La Taille, A.; Roupret, M. Functional Outcomes after Robot-Assisted Pyeloplasty for Ureteropelvic Junction Obstruction: A Bi-Centre Experience. Int. J. Med. Robot. Comput. Assist. Surg. MRCAS 2021, 17, e2201. [Google Scholar] [CrossRef]
- Autorino, R.; Eden, C.; El-Ghoneimi, A.; Guazzoni, G.; Buffi, N.; Peters, C.A.; Stein, R.J.; Gettman, M. Robot-Assisted and Laparoscopic Repair of Ureteropelvic Junction Obstruction: A Systematic Review and Meta-Analysis. Eur. Urol. 2014, 65, 430–452. [Google Scholar] [CrossRef]
- Rasool, S.; Singh, M.; Jain, S.; Chaddha, S.; Tyagi, V.; Pahwa, M.; Pandey, H. Comparison of Open, Laparoscopic and Robot-Assisted Pyeloplasty for Pelviureteric Junction Obstruction in Adult Patients. J. Robot. Surg. 2020, 14, 325–329. [Google Scholar] [CrossRef] [PubMed]
- Hopf, H.L.; Bahler, C.D.; Sundaram, C.P. Long-Term Outcomes of Robot-Assisted Laparoscopic Pyeloplasty for Ureteropelvic Junction Obstruction. Urology 2016, 90, 106–111. [Google Scholar] [CrossRef] [PubMed]
- Minnillo, B.J.; Cruz, J.A.S.; Sayao, R.H.; Passerotti, C.C.; Houck, C.S.; Meier, P.M.; Borer, J.G.; Diamond, D.A.; Retik, A.B.; Nguyen, H.T. Long-Term Experience and Outcomes of Robotic Assisted Laparoscopic Pyeloplasty in Children and Young Adults. J. Urol. 2011, 185, 1455–1460. [Google Scholar] [CrossRef] [PubMed]
- Tobis, S.; Venigalla, S.; Balakumaran, K.; Scosyrev, E.; Lloyd, G.L.; Golijanin, D.J.; Joseph, J.V.; Rashid, H.; Wu, G. Analysis of a Large Single-Center Experience with Robot-Assisted Pyeloplasty. Int. J. Urol. Off. J. Jpn. Urol. Assoc. 2013, 20, 230–234. [Google Scholar] [CrossRef]
- Başataç, C.; Boylu, U.; Önol, F.F.; Gümüş, E. Comparison of Surgical and Functional Outcomes of Open, Laparoscopic and Robotic Pyeloplasty for the Treatment of Ureteropelvic Junction Obstruction. Turk. J. Urol. 2014, 40, 24–30. [Google Scholar] [CrossRef]
- Sorensen, M.D.; Delostrinos, C.; Johnson, M.H.; Grady, R.W.; Lendvay, T.S. Comparison of the Learning Curve and Outcomes of Robotic Assisted Pediatric Pyeloplasty. J. Urol. 2011, 185 (Suppl. 6), 2517–2522. [Google Scholar] [CrossRef]
- Yu, H.; Hevelone, N.D.; Lipsitz, S.R.; Kowalczyk, K.J.; Hu, J.C. Use, Costs and Comparative Effectiveness of Robotic Assisted, Laparoscopic and Open Urological Surgery. J. Urol. 2012, 187, 1392–1398. [Google Scholar] [CrossRef]
- Link, R.E.; Bhayani, S.B.; Kavoussi, L.R. A Prospective Comparison of Robotic and Laparoscopic Pyeloplasty. Ann. Surg. 2006, 243, 486–491. [Google Scholar] [CrossRef]
- Totaro, A.; Campetella, M.; Bientinesi, R.; Gandi, C.; Palermo, G.; Russo, A.; Aceto, P.; Bassi, P.; Sacco, E. The New Surgical Robotic Platform HUGOTM RAS: System Description and Docking Settings for Robot-Assisted Radical Prostatectomy. Urologia 2022, 89, 603–609. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| RALP Group (N= 43) | OP Group (N = 48) | p Value | |
|---|---|---|---|
| Gender | |||
| Male | 16 (37.2) | 25 (52.1) | |
| Female | 27 (62.8) | 23 (47.9) | 0.225 |
| Age, years | 44 ± 19.3 | 49.7± 17,5 | 0.197 |
| BMI, kg/m2 | 25.7 ± 2.9 | 25.5 ± 4.6 | 0.596 |
| CCI | 2.0 ± 2.1 | 1.6 ± 1.7 | 0.015 |
| Side | |||
| Right | 25 (58.1) | 30 (62.5) | |
| Left | 18 (41.9) | 18 (37.5) | 0.883 |
| Presence of symptoms at diagnosis | 30 (69.8) | 34 (70.8) | 0.905 |
| Renal colic | 19 (44.1) | 19 (39.5) | |
| Chronic Flank pain | 10 (23.2) | 13 (27.0) | |
| Recurrent UTIs | 3 (7.0) | 5 (10.4) | |
| Acute pyelonephritis | 0 (0) | 3 (8.8) | |
| Asymptomatic | 13 (30.2) | 14 (29. 1) | |
| Preoperative double-j stent | 1 (2.3) | 3 (6.3) | 0.689 |
| Preoperative nephrostomy | 8 (18.6) | 16 (33.3) | 0.176 |
| Previous abdominal surgery | 10 (23.5) | 19 (39.5) | 0.148 |
| Concomitant stone disease | 7 (16.3) | 16 (33.3) | 0.103 |
| RALP Group | OP Group | p Value | |
|---|---|---|---|
| (n = 43) | (n = 48) | ||
| INTRAOPERATIVE OUTCOMES | |||
| Operative time, min | 170.0 ± 49.5 | 171.9 ± 54.8 | 0.868 |
| Crossing vessels | 28 (65) | 19 (39.6) | 0.026 |
| Estimated blood loss, mL | 26.7 ± 11.4 | 80.2 ± 85.5 | <0.001 |
| Blood transfusion | 0 (0) | 0 (0) | |
| Intraoperative complications | |||
| Renal vein lesion | 0 (0) | 1 (2.1) | 0.341 |
| Conversion to open surgery | 0 (0) | n.a. | |
| EARLY POSTOPERATIVE OUTCOMES | |||
| Clavien–Dindo Classification I II III IV | 7 (16.2) 2 (4.6) 2 (4.6) 3 (7.0) 0 (0) | 23 (47.9) 5 (10.4) 13 (27.1) 4 (8.3) 1 (2.1) | 0.002 |
| Clavien–Dindo ≥ 2 complications | 5 (11.6) | 18 (37.5) | 0.009 |
| Wound infections | 0 (0) | 4 (8.3) | |
| Surgical site infections | 0 (0) | 6 (12.5) | |
| Pneumonia | 0 (0) | 2 (4.2) | |
| Abdominal hematoma | 1 (2.3) | 0 (0) | |
| Hematuria | 1 (2.3) | 1 (2.1) | |
| Stent displacement | 2 (4.6) | 1 (2.1) | |
| Urinary leakage | 1 (2.3) | 2 (4.2) | |
| Urosepsis | 0 (0) | 2 (4.2) | |
| Analgesic (paracetamol) requirement, mg | 2218.75 ± 2587.0 | 3531.9 ± 2842.6 | 0.019 |
| Patients requiring postoperative antibiotic course | 4 (9.3) | 18 (37.5) | 0.004 |
| Length of hospital stay, days | 7.7 ± 2.4 | 8.9 ± 4.5 | 0.131 |
| LATE POSTOPERATIVE OUTCOMES | |||
| Complications, n. (%) | 3 (7.0) | 9 (18.7) | 0.178 |
| Laparocele requiring surgical correction | 0 (0) | 1 (2.1) | 0.922 |
| Nephrostomy Placement, n. (%) | 3 (7.0) | 8 (16.7) | 0.274 |
| RALP Group | OP Group | p Value | |
|---|---|---|---|
| Cost of diagnostic procedures performed during the hospitalization, € | 240.5 ± 146.5 | 445.5 ± 382.0 | 0.0009 |
| Cost of hospital stay, € | 2320.0 ± 630.4 | 3022.2 ± 1852.9 | 0.0153 |
| Cost of the operating room, € | 1854.3 ± 503.4 | 2460.4 ± 635.0 | <0.0001 |
| Cost of devices used for surgery (including robotic equipment), € | 4286.0 ± 1083.7 | 398.9 ± 112.0 | <0.0001 |
| Total cost, € | 8700.9 ± 1274.7 | 6327.1 ± 2404.4 | <0.0001 |
| OR | 95% CI | p Value | |
|---|---|---|---|
| Sex (male vs. female) | 0.66 | 0.18–2.44 | 0.539 |
| Age (one-year increase) | 1.02 | 0.98–1.05 | 0.247 |
| BMI (unit increase) | 1.13 | 0.99–1.30 | 0.060 |
| CCI (unit increase) | 1.19 | 0.87–1.61 | 0.260 |
| Side (left versus right) | 2.91 | 0.81–11.92 | 0.109 |
| Presence of symptoms at diagnosis (yes vs. no) | 2.04 | 0.41–10.16 | 0.381 |
| Previous abdominal surgery (yes vs. no) | 1.26 | 0.35–4.47 | 0.718 |
| Preoperative double-j stent or nephrostomy (yes vs. no) | 1.14 | 0.22–5.92 | 0.871 |
| Crossing vessel (yes vs. no) | 0.75 | 0.21–2.67 | 0.661 |
| Concomitant stone disease (yes vs. no) | 2,87 | 0.78–10.50 | 0.111 |
| Postoperative infections (yes vs. no) | 1.71 | 0.45–6.47 | 0.426 |
| Surgical approach (robotic vs. open) | 0.39 | 0.09–1.59 | 0.192 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moretto, S.; Gandi, C.; Bientinesi, R.; Totaro, A.; Marino, F.; Gavi, F.; Russo, A.; Aceto, P.; Pierconti, F.; Bassi, P.; et al. Robotic versus Open Pyeloplasty: Perioperative and Functional Outcomes. J. Clin. Med. 2023, 12, 2538. https://doi.org/10.3390/jcm12072538
Moretto S, Gandi C, Bientinesi R, Totaro A, Marino F, Gavi F, Russo A, Aceto P, Pierconti F, Bassi P, et al. Robotic versus Open Pyeloplasty: Perioperative and Functional Outcomes. Journal of Clinical Medicine. 2023; 12(7):2538. https://doi.org/10.3390/jcm12072538
Chicago/Turabian StyleMoretto, Stefano, Carlo Gandi, Riccardo Bientinesi, Angelo Totaro, Filippo Marino, Filippo Gavi, Andrea Russo, Paola Aceto, Francesco Pierconti, Pierfrancesco Bassi, and et al. 2023. "Robotic versus Open Pyeloplasty: Perioperative and Functional Outcomes" Journal of Clinical Medicine 12, no. 7: 2538. https://doi.org/10.3390/jcm12072538