
Physiotherapy as an Effective Method to Support the Treatment of Male Urinary Incontinence: A Systematic Review

 , , , , and
, , , , and
Abstract
:1. Introduction
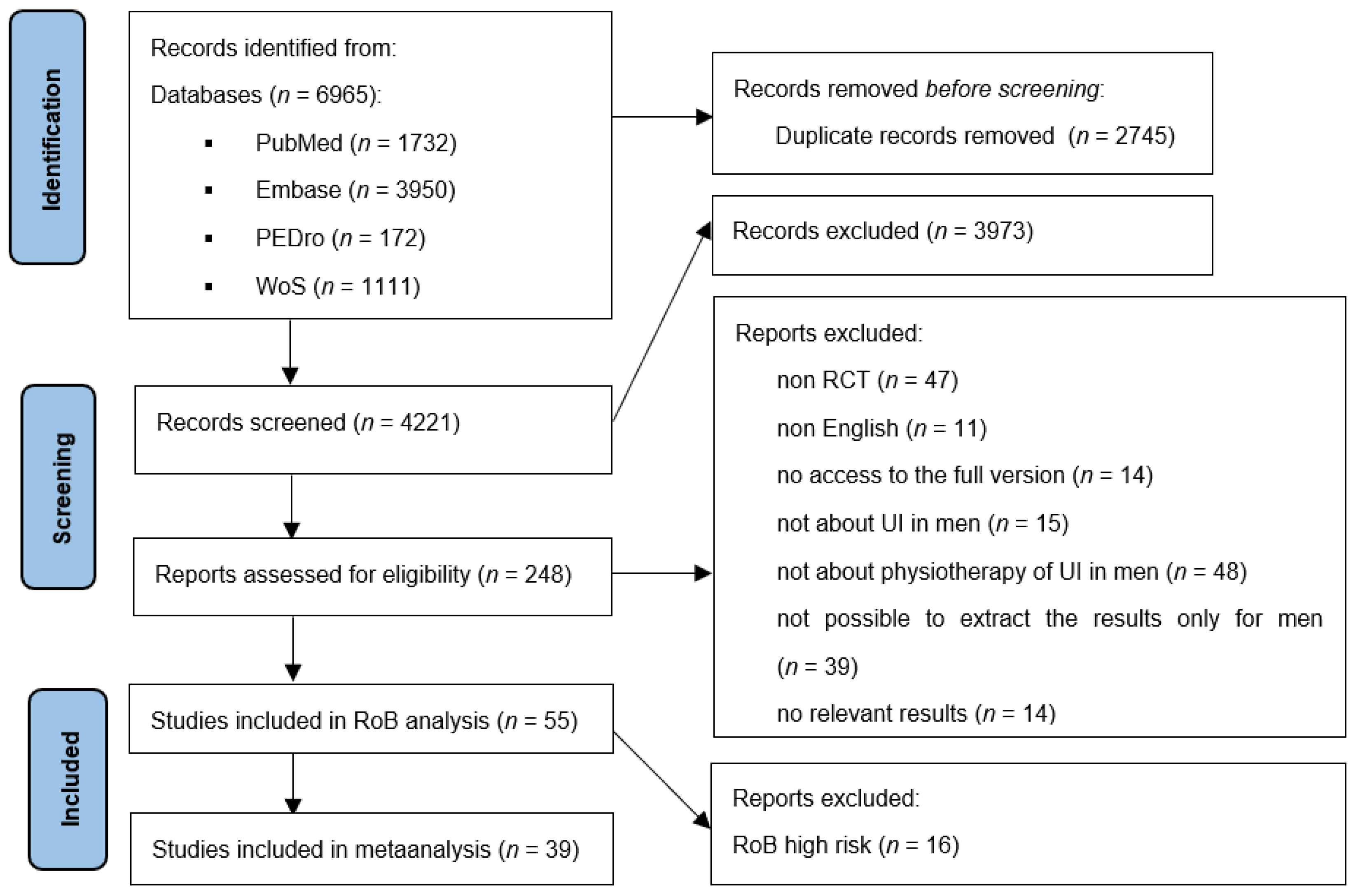
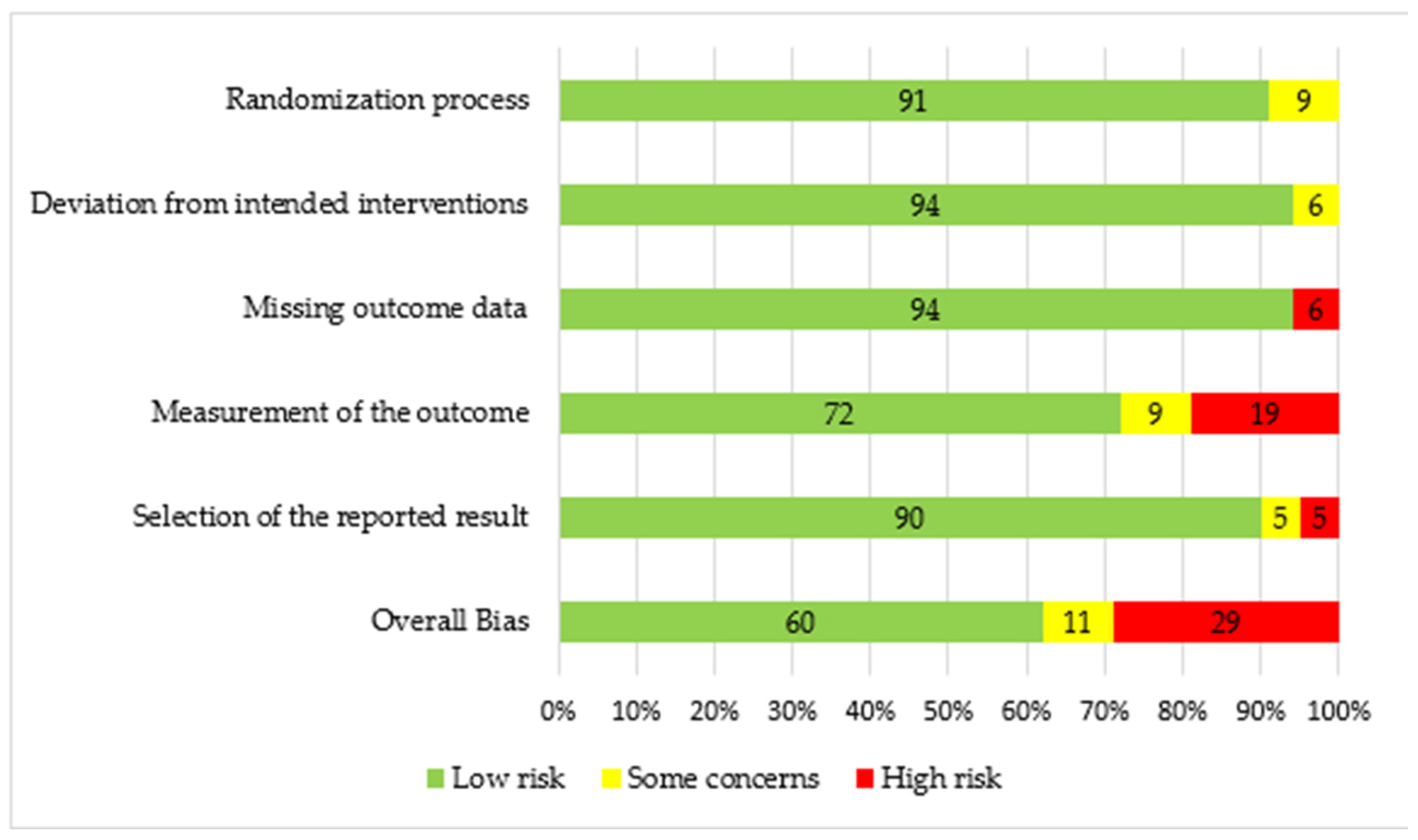
2. Materials and Methods
3. Results
3.1. Pelvic Floor Muscle Training in Men with UI
3.2. Pelvic Floor Muscle Training and Biofeedback
3.3. Electrical Stimulation in Men with UI
4. Discussion
5. Limitations of the Study
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A


References
- Helfand, B.T.; Smith, A.R.; Lai, H.H.; Yang, C.C.; Gore, J.L.; Erickson, B.A.; Kreder, K.J.; Cameron, A.P.; Weinfurt, K.P.; Griffith, J.W.; et al. Prevalence and Characteristics of Urinary Incontinence in a Treatment Seeking Male Prospective Cohort: Results from the LURN Study. J. Urol. 2018, 200, 397–404. [Google Scholar] [CrossRef]
- Park, H.K.; Chang, S.; Palmer, M.H.; Kim, I.; Choi, H. Assessment of the Impact of Male Urinary Incontinence on Health-Related Quality of Life: A Population Based Study. Low. Urin. Tract Symptoms 2015, 7, 22–26. [Google Scholar] [CrossRef] [PubMed]
- Das, A.K.; Kucherov, V.; Glick, L.; Chung, P. Male urinary incontinence after prostate disease treatment. Can. J. Urol. 2020, 27 (Suppl. S3), 36–43. [Google Scholar] [PubMed]
- Holze, S.; Mende, M.; Healy, K.V.; Koehler, N.; Gansera, L.; Truss, M.C.; Rebmann, U.; Degener, S.; Stolzenburg, J.-U. Comparison of various continence definitions in a large group of patients undergoing radical prostatectomy: A multicentre, prospective study. BMC Urol. 2019, 19, 70. [Google Scholar] [CrossRef]
- Pernar, C.H.; Ebot, E.M.; Wilson, K.M.; Mucci, L.A. The Epidemiology of Prostate Cancer. Cold Spring Harb. Perspect. Med. 2018, 8, a030361. [Google Scholar] [CrossRef] [Green Version]
- Strączyńska, A.; Weber-Rajek, M.A.-O.; Strojek, K.A.-O.; Piekorz, Z.A.-O.; Styczyńska, H.A.-O.; Goch, A.; Radzimińska, A.A.-O. The Impact of Pelvic Floor Muscle Training on Urinary Incontinence in Men After Radical Prostatectomy (RP)—A Systematic Review. Clin. Interv. Aging 2019, 14, 1997–2005. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rehder, P.; Staudacher, N.M.; Schachtner, J.; Berger, M.E.; Schillfahrt, F.; Hauser, V.; Mueller, R.; Skradski, V.; Horninger, W.; Glodny, B. Hypothesis That Urethral Bulb (Corpus Spongiosum) Plays an Active Role in Male Urinary Continence. Adv. Urol. 2016, 2016, 6054730. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pan, L.-H.; Lin, M.-H.; Pang, S.-T.; Wang, J.; Shih, W.-M.; Shih, W.-M. Improvement of Urinary Incontinence, Life Impact, and Depression and Anxiety with Modified Pelvic Floor Muscle Training After Radical Prostatectomy. Am. J. Men’s Heath 2019, 13, 1557988319851618. [Google Scholar] [CrossRef]
- Canning, A.; Raison, N.; Aydin, A.; Cheikh Youssef, S.; Khan, S.; Dasgupta, P.; Ahmed, K. A systematic review of treatment options for post-prostatectomy incontinence. World J. Urol. 2022, 40, 2617–2626. [Google Scholar] [CrossRef]
- Mazur-Bialy, A.I.; Kołomańska-Bogucka, D.; Nowakowski, C.; Tim, S. Urinary Incontinence in Women: Modern Methods of Physiotherapy as a Support for Surgical Treatment or Independent Therapy. J. Clin. Med. 2020, 9, 1211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hodges, P.W.; Stafford, R.E.; Hall, L.; Neumann, P.; Morrison, S.; Frawley, H.; Doorbar-Baptist, S.; Nahon, I.; Crow, J.; Thompson, J.; et al. Reconsideration of pelvic floor muscle training to prevent and treat incontinence after radical prostatectomy. Urol. Oncol. Semin. Orig. Investig. 2019, 38, 354–371. [Google Scholar] [CrossRef] [PubMed]
- Chung, E.; Katz, D.J.; Love, C. Adult male stress and urge urinary incontinence—A review of pathophysiology and treatment strategies for voiding dysfunction in men. Aust. Fam. Physician 2017, 46, 661–666. [Google Scholar] [PubMed]
- Hall, L.M.; Aljuraifani, R.A.; Hodges, P.W. Design of programs to train pelvic floor muscles in men with urinary dysfunction: Systematic review. Neurourol. Urodyn. 2018, 37, 2053–2087. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; the PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [Green Version]
- Ahmed, M.T.; Mohammed, A.H.; Amansour, A. Effect of pelvic floor electrical stimulation and biofeedback on the recovery of urinary continence after radical prostatectomy/Radikal prostatektomi sonrasi uriner inkontinansin duzelmesinde pelvik tabanda biofeedback ve elektrik stimulasyonunun etkisi. Turk. J. Phys. Med. Rehabil. 2012, 58, 170. [Google Scholar] [CrossRef]
- Allameh, F.; Rayegani, S.M.; Razzaghi, M.; Abedi, A.R.; Rahavian, A.; Javadi, A.; Montazeri, S. Comparison of the effect of the pelvic floor muscle biofeedback prior or postradical prostatectomy on urinary incontinence: A randomized controlled trial. Turk. J. Urol. 2021, 47, 436–441. [Google Scholar] [CrossRef]
- Anan, G.; Kaiho, Y.; Iwamura, H.; Ito, J.; Kohada, Y.; Mikami, J.; Sato, M. Preoperative pelvic floor muscle exercise for early continence after holmium laser enucleation of the prostate: A randomized controlled study. BMC Urol. 2020, 20, 3. [Google Scholar] [CrossRef] [Green Version]
- Aydın Sayılan, A.; Özbaş, A. The Effect of Pelvic Floor Muscle Training on Incontinence Problems After Radical Prostatectomy. Am. J. Men’s Health 2018, 12, 1007–1015. [Google Scholar] [CrossRef]
- Bernardes, M.; Mata, L.; Azevedo, C.; Izidoro, L.C.R.; Oliveira, C.M.C.; Chianca, T.C.M. Effectiveness of systemic acupuncture in the control of urinary incontinence following radical prostatectomy: A randomized clinical trial. Rev. Esc. Enferm. USP 2022, 56, e20220135. [Google Scholar] [CrossRef]
- Centemero, A.; Rigatti, L.; Giraudo, D.; Lazzeri, M.; Lughezzani, G.; Zugna, D.; Montorsi, F.; Rigatti, P.; Guazzoni, G. Preoperative Pelvic Floor Muscle Exercise for Early Continence After Radical Prostatectomy: A Randomised Controlled Study. Eur. Urol. 2010, 57, 1039–1043. [Google Scholar] [CrossRef] [PubMed]
- De Lira, G.H.S.; Fornari, A.; Cardoso, L.F.; Aranchipe, M.; Kretiska, C.; Rhoden, E.L. Effects of perioperative pelvic floor muscle training on early recovery of urinary continence and erectile function in men undergoing radical prostatectomy: A randomized clinical trial. Int. Braz. J. Urol. 2019, 45, 1196–1203. [Google Scholar] [CrossRef] [PubMed]
- Faithfull, S.; Cockle-Hearne, J.; Lemanska, A.; Otter, S.; Skene, S.S. Randomised controlled trial to investigate the effectiveness of the symptom management after radiotherapy (SMaRT) group intervention to ameliorate lower urinary tract symptoms in men treated for prostate cancer. Support. Care Cancer 2022, 30, 3165–3176. [Google Scholar] [CrossRef]
- Floratos, D.L.; Sonke, G.S.; Rapidou, C.A.; Alivizatos, G.J.; Deliveliotis, C.; Constantinides, C.A.; Theodorou, C. Biofeedback vs verbal feedback as learning tools for pelvic muscle exercises in the early management of urinary incontinence after radical prostatectomy. BJU Int. 2002, 89, 714–719. [Google Scholar] [CrossRef] [Green Version]
- Geraerts, I.; Van Poppel, H.; Devoogdt, N.; Joniau, S.; Van Cleynenbreugel, B.; De Groef, A.; Van Kampen, M. Influence of Preoperative and Postoperative Pelvic Floor Muscle Training (PFMT) Compared with Postoperative PFMT on Urinary Incontinence After Radical Prostatectomy: A Randomized Controlled Trial. Eur. Urol. 2013, 64, 766–772. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gezginci, E.; Goktas, S.; Ata, A. Effect of perioperative pelvic floor muscle training program on incontinence and quality of life after radical prostatectomy: A randomized controlled trial. Clin. Rehabil. 2022, 37, 2692155221134477. [Google Scholar] [CrossRef]
- Gomes, C.S.; Pedriali, F.R.; Urbano, M.R.; Moreira, E.H.; Averbeck, M.A.; Almeida, S.H.M. The effects of Pilates method on pelvic floor muscle strength in patients with post-prostatectomy urinary incontinence: A randomized clinical trial. Neurourol. Urodyn. 2018, 37, 346–353. [Google Scholar] [CrossRef]
- Heydenreich, M.; Puta, C.; Gabriel, H.H.; Dietze, A.; Wright, P.; Zermann, D.-H. Does trunk muscle training with an oscillating rod improve urinary incontinence after radical prostatectomy? A prospective randomized controlled trial. Clin. Rehabil. 2020, 34, 320–333. [Google Scholar] [CrossRef]
- Van Kampen, M.; de Weerdt, W.; Van Poppel, H.; De Ridder, D.; Feys, H.; Baert, L. Effect of pelvic-floor re-education on duration and degree of incontinence after radical prostatectomy: A randomised controlled trial. Lancet 2000, 355, 98–102. [Google Scholar] [CrossRef]
- Laurienzo, C.E.; Magnabosco, W.J.; Jabur, F.; Faria, E.F.; Gameiro, M.O.; Sarri, A.J.; Kawano, P.R.; Yamamoto, H.A.; Reis, L.O.; Amaro, J.L. Pelvic floor muscle training and electrical stimulation as rehabilitation after radical prostatectomy: A randomized controlled trial. J. Phys. Ther. Sci. 2018, 30, 825–831. [Google Scholar] [CrossRef] [Green Version]
- Laurienzo, C.E.; Sacomani, C.A.R.; Rodrigues, T.R.; Zequi, S.C.; Guimarães, G.C.; Lopes, A. Results of preoperative electrical stimulation of pelvic floor muscles in the continence status following radical retropubic prostatectomy. Int. Braz. J. Urol. 2013, 39, 182–188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manassero, F.; Traversi, C.; Ales, V.; Pistolesi, D.; Panicucci, E.; Valent, F.; Selli, C. Contribution of early intensive prolonged pelvic floor exercises on urinary continence recovery after bladder neck-sparing radical prostatectomy: Results of a prospective controlled randomized trial. Neurourol. Urodyn. 2007, 26, 985–989. [Google Scholar] [CrossRef] [PubMed]
- Mariotti, G.; Sciarra, A.; Gentilucci, A.; Salciccia, S.; Alfarone, A.; DI Pierro, G.B.; Gentile, V. Early Recovery of Urinary Continence After Radical Prostatectomy Using Early Pelvic Floor Electrical Stimulation and Biofeedback Associated Treatment. J. Urol. 2009, 181, 1788–1793. [Google Scholar] [CrossRef] [PubMed]
- Mariotti, G.; Salciccia, S.; Innocenzi, M.; Gentilucci, A.; Fasulo, A.; Gentile, V.; Sciarra, A. Recovery of Urinary Continence After Radical Prostatectomy Using Early vs Late Pelvic Floor Electrical Stimulation and Biofeedback-associated Treatment. Urology 2015, 86, 115–120. [Google Scholar] [CrossRef]
- Milios, J.E.; Ackland, T.R.; Green, D.J. Pelvic floor muscle training in radical prostatectomy: A randomized controlled trial of the impacts on pelvic floor muscle function and urinary incontinence. BMC Urol. 2019, 19, 16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moore, K.N.; Valiquette, L.; Fau -Chetner, M.P.; Chetner Mp Fau -Byrniak, S.; Byrniak, S.; Fau -Herbison, G.P.; Herbison, G.P. Return to continence after radical retropubic prostatectomy: A randomized trial of verbal and written instructions versus therapist-directed pelvic floor muscle therapy. Urology 2008, 72, 1280–1286. [Google Scholar] [CrossRef] [PubMed]
- Nilssen, S.R.; Mørkved, S.; Overgård, M.; Lydersen, S.; Angelsen, A. Does physiotherapist-guided pelvic floor muscle training increase the quality of life in patients after radical prostatectomy? A randomized clinical study. Scand. J. Urol. Nephrol. 2012, 46, 397–404. [Google Scholar] [CrossRef] [PubMed]
- Oh, J.J.; Kim, J.A.-O.; Lee, H.; Lee, S.; Jin Jeong, S.; Kyu Hong, S.; Eun Lee, S.; Byun, S.S. Effect of personalized extracorporeal biofeedback device for pelvic floor muscle training on urinary incontinence after robot-assisted radical prostatectomy: A randomized controlled trial. Neurourol. Urodyn. 2020, 39, 674–681. [Google Scholar] [CrossRef]
- Overgård, M.; Angelsen, A.; Lydersen, S.; Mørkved, S. Does Physiotherapist-Guided Pelvic Floor Muscle Training Reduce Urinary Incontinence After Radical Prostatectomy? A Randomised Controlled Trial. Eur. Urol. 2008, 54, 438–448. [Google Scholar] [CrossRef]
- Pané-Alemany, R.; Ramírez-García, I.; Kauffmann, S.; Blanco-Ratto, L.; Carralero-Martínez, A.; Sánchez Ruiz, E. Efficacy of transcutaneous perineal electrostimulation versus intracavitary anal electrostimulation in the treatment of urinary incontinence after a radical prostatectomy: Randomized controlled trial. Neurourol. Urodyn. 2021, 40, 1761–1769. [Google Scholar] [CrossRef]
- Perez, F.S.B.; Rosa, N.C.; Da Rocha, A.F.; Peixoto, L.R.T.; Miosso, C.J. Effects of Biofeedback in Preventing Urinary Incontinence and Erectile Dysfunction after Radical Prostatectomy. Front. Oncol. 2018, 8, 20. [Google Scholar] [CrossRef] [Green Version]
- Pedriali, F.R.; Gomes, C.S.; Soares, L.; Urbano, M.R.; Moreira, E.C.; Averbeck, M.A.; de Almeida, S.H. Is pilates as effective as conventional pelvic floor muscle exercises in the conservative treatment of post-prostatectomy urinary incontinence? A randomised controlled trial. Neurourol. Urodyn. 2016, 35, 615–621. [Google Scholar] [CrossRef] [PubMed]
- Porru, D.; Campus, G.; Caria, A.; Madeddu, G.; Cucchi, A.; Rovereto, B.; Scarpa, R.M.; Pili, P.; Usai, E. Impact of early pelvic floor rehabilitation after transurethral resection of the prostate. Neurourol. Urodyn. 2001, 20, 53–59. [Google Scholar] [CrossRef]
- Rajkowska-Labon, E.; Bakuła, S.; Kucharzewski, M.; Śliwiński, Z. Efficacy of Physiotherapy for Urinary Incontinence following Prostate Cancer Surgery. BioMed. Res. Int. 2014, 2014, 785263. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, L.H.; Prota, C.; Gomes, C.M.; de Bessa, J., Jr.; Boldarine, M.P.; Dall’Oglio, M.F.; Bruschini, H.; Srougi, M. Long-Term Effect of Early Postoperative Pelvic Floor Biofeedback on Continence in Men Undergoing Radical Prostatectomy: A Prospective, Randomized, Controlled Trial. J. Urol. 2010, 184, 1034–1039. [Google Scholar] [CrossRef] [PubMed]
- Santos, N.A.; Saintrain, M.V.; Regadas, R.P.; da Silveira, R.A.; De Menezes, F.J. Assessment of Physical Therapy Strategies for Recovery of Urinary Continence after Prostatectomy. Asian Pac. J. Cancer Prev. 2017, 18, 81–86. [Google Scholar] [CrossRef] [PubMed]
- Serdà, B.-C.; Marcos-Gragera, R. Urinary Incontinence and Prostate Cancer: A Progressive Rehabilitation Program Design. Rehabil. Nurs. 2014, 39, 271–280. [Google Scholar] [CrossRef]
- Soto González, M.; Da Cuña Carrera, I.; Gutiérrez Nieto, M.; López García, S.; Ojea Calvo, A.; Lantarón Caeiro, E.M. Early 3-month treatment with comprehensive physical therapy program restores continence in urinary incontinence patients after radical prostatectomy: A randomized controlled trial. Neurourol. Urodyn. 2020, 39, 1529–1537. [Google Scholar] [CrossRef] [PubMed]
- Strojek, K.; Weber-Rajek, M.; Strączyńska, A.; Piekorz, Z.; Pilarska, B.; Jarzemski, P.; Kozakiewicz, M.; Brzoszczyk, B.; Jarzemski, M.; Styczyńska, H.; et al. Randomized-Controlled Trial Examining the Effect of Pelvic Floor Muscle Training in the Treatment of Stress Urinary Incontinence in Men after a Laparoscopic Radical Prostatectomy Pilot Study. J. Clin. Med. 2021, 10, 2946. [Google Scholar] [CrossRef]
- Tantawy, S.A.; Elgohary, H.M.I.; Abdelbasset, W.K.; Kamel, D.M. Effect of 4 weeks of whole-body vibration training in treating stress urinary incontinence after prostate cancer surgery: A randomised controlled trial. Physiotherapy 2019, 105, 338–345. [Google Scholar] [CrossRef]
- Tienforti, D.; Sacco, E.; Marangi, F.; D’Addessi, A.; Racioppi, M.; Gulino, G.; Pinto, F.; Totaro, A.; D’Agostino, D.; Bassi, P. Efficacy of an assisted low-intensity programme of perioperative pelvic floor muscle training in improving the recovery of continence after radical prostatectomy: A randomized controlled trial. BJU Int. 2012, 110, 1004–1010. [Google Scholar] [CrossRef] [PubMed]
- Yamanishi, T.; Mizuno, T.; Watanabe, M.; Honda, M.; Yoshida, K. Randomized, Placebo Controlled Study of Electrical Stimulation with Pelvic Floor Muscle Training for Severe Urinary Incontinence After Radical Prostatectomy. J. Urol. 2010, 184, 2007–2012. [Google Scholar] [CrossRef] [PubMed]
- Yokoyama, T.; Nishiguchi, J.; Watanabe, T.; Nose, H.; Nozaki, K.; Fujita, O.; Inoue, M.; Kumon, H. Comparative study of effects of extracorporeal magnetic innervation versus electrical stimulation for urinary incontinence after radical prostatectomy. Urology 2004, 63, 264–267. [Google Scholar] [CrossRef] [PubMed]
- Zhang, A.Y.; Bodner, D.R.; Fu, A.Z.; Gunzler, D.D.; Klein, E.; Kresevic, D.; Moore, S.M.; Ponsky, L.; Purdum, M.; Strauss, G.; et al. Effects of Patient Centered Interventions on Persistent Urinary Incontinence after Prostate Cancer Treatment: A Randomized, Controlled Trial. J. Urol. 2015, 194, 1675–1681. [Google Scholar] [CrossRef]
- Mungovan, S.F.; Carlsson, S.V.; Gass, G.C.; Graham, P.L.; Sandhu, J.S.; Akin, O.; Scardino, P.T.; Eastham, J.A.; Patel, M.I. Preoperative exercise interventions to optimize continence outcomes following radical prostatectomy. Nat. Rev. Urol. 2021, 18, 259–281. [Google Scholar] [CrossRef]
- Santa Mina, D.; Au, D.; Alibhai, S.M.; Jamnicky, L.; Faghani, N.; Hilton, W.J.; Stefanyk, L.E.; Ritvo, P.; Jones, J.; Elterman, D.; et al. A pilot randomized trial of conventional versus advanced pelvic floor exercises to treat urinary incontinence after radical prostatectomy: A study protocol. BMC Urol. 2015, 15, 94. [Google Scholar] [CrossRef] [Green Version]
- Hsu, L.-F.; Liao, Y.-M.; Lai, F.-C.; Tsai, P.-S. Beneficial effects of biofeedback-assisted pelvic floor muscle training in patients with urinary incontinence after radical prostatectomy: A systematic review and metaanalysis. Int. J. Nurs. Stud. 2016, 60, 99–111. [Google Scholar] [CrossRef]
- Pacik, D.; Fedorko, M. Literature review of factors affecting continence after radical prostatectomy. Saudi Med. J. 2017, 38, 9–17. [Google Scholar] [CrossRef]
- Chughtai, B.; Lee, R.; Sandhu, J.; Te, A.; Kaplan, S. Conservative treatment for postprostatectomy incontinence. Rev. Urol. 2013, 15, 61–66. [Google Scholar] [CrossRef]
- Sandhu, J.S.; Breyer, B.; Comiter, C.; Eastham, J.A.; Gomez, C.; Kirages, D.J.; Kittle, C.; Lucioni, A.; Nitti, V.W.; Stoffel, J.T.; et al. Incontinence after Prostate Treatment: AUA/SUFU Guideline. J. Urol. 2019, 202, 369–378. [Google Scholar] [CrossRef]
- Anderson, C.A.; Omar, M.I.; Campbell, S.E.; Hunter, K.F.; Cody, J.D.; Glazener, C.M. Conservative management for postprostatectomy urinary incontinence. Cochrane Database Syst. Rev. 2015, 1, CD001843. [Google Scholar] [CrossRef] [Green Version]
- Goode, P.S.; Burgio, K.L.; Johnson, T.M., 2nd; Clay, O.J.; Roth, D.L.; Markland, A.D.; Burkhardt, J.H.; Issa, M.M.; Lloyd, L.K. Behavioral Therapy with or Without Biofeedback and Pelvic Floor Electrical Stimulation for Persistent Postprostatectomy Incontinence: A randomized controlled trial. JAMA 2011, 305, 151–159. [Google Scholar] [CrossRef] [Green Version]
- Zaidan, P.; Fernandes Muller, V.J.; de Silva, E.B. Electrical Stimulation, pelvic floor muscle exercises, and urianry incontinence in post-prostatectomy patients: Controlled randomized double-blind exeperiment. Int. J. Curr. Res. 2016, 8, 41859–41863. [Google Scholar]
- Kannan, P.; Winser, S.J.; Fung, B.; Cheing, G. Effectiveness of Pelvic Floor Muscle Training Alone and in Combination with Biofeedback, Electrical Stimulation, or Both Compared to Control for Urinary Incontinence in Men Following Prostatectomy: Systematic Review and Meta-Analysis. Phys. Ther. 2018, 98, 932–945. [Google Scholar] [CrossRef] [Green Version]
- Radadia, K.D.; Farber, N.J.; Shinder, B.; Polotti, C.F.; Milas, L.J.; Tunuguntla, H.S.G.R. Management of Postradical Prostatectomy Urinary Incontinence: A Review. Urology 2018, 113, 13–19. [Google Scholar] [CrossRef] [PubMed]
- Gacci, M.; Sakalis, V.I.; Karavitakis, M.; Cornu, J.-N.; Gratzke, C.; Herrmann, T.R.W.; Kyriazis, I.; Malde, S.; Mamoulakis, C.; Rieken, M.; et al. European Association of Urology Guidelines on Male Urinary Incontinence. Eur. Urol. 2022, 82, 387–398. [Google Scholar] [CrossRef] [PubMed]
- Kondo, K.; Noonan, K.M.; Freeman, M.; Ayers, C.; Morasco, B.J.; Kansagara, D. Efficacy of Biofeedback for Medical Conditions: An Evidence Map. J. Gen. Intern. Med. 2019, 34, 2883–2893. [Google Scholar] [CrossRef]
- Fernández-Cuadros, M.E.; Nieto-Blasco, J.; Geanini-Yagüez, A.; Ciprián-Nieto, D.; Padilla-Fernández, B.; Lorenzo-Gómez, M.F. Male Urinary Incontinence: Associated Risk Factors and Electromyography Biofeedback Results in Quality of Life. Am. J. Men’s Health 2016, 10, NP127–NP135. [Google Scholar] [CrossRef] [Green Version]
- Borkowetz, A. Harninkontinenz nach radikaler Prostatektomie. Der Urologe 2018, 57, 1251–1254. [Google Scholar] [CrossRef]
- Wang, W.; Huang, Q.M.; Liu, F.P.; Mao, Q.Q. Effectiveness of preoperative pelvic floor muscle training for urinary incontinence after radical prostatectomy: A meta-analysis. BMC Urol. 2014, 14, 99. [Google Scholar] [CrossRef] [Green Version]
- Zhu, Y.-P.; Yao, X.-D.; Zhang, S.-L.; Dai, B.; Ye, D.-W. Pelvic Floor Electrical Stimulation for Postprostatectomy Urinary Incontinence: A Meta-Analysis. Urology 2012, 79, 552–555. [Google Scholar] [CrossRef] [PubMed]
- Au, D.; Matthew, A.G.; Alibhai SM, H.; Jones, J.M.; Fleshner, N.E.; Finelli, A.; Elterman, D.; Singal, R.K.; Jamnicky, L.; Faghani, N.; et al. Pfilates and Hypopressives for the Treatment of Urinary Incontinence After Radical Prostatectomy: Results of a Feasibility Randomized Controlled Trial. PM&R 2020, 12, 55–63. [Google Scholar] [CrossRef]
- Bales, G.T.; Gerber, G.S.; Minor, T.X.; Mhoon, D.A.; McFarland, J.M.; Kim, H.L.; Brendler, C.B. Effect of Preoperative Biofeedback/Pelvic Floor Training on Continence in Men Undergoing Radical Prostatectomy. Urology 2000, 56, 627–630. [Google Scholar] [CrossRef]
- Dijkstra-Eshuis, J.; Van den Bos, T.W.; Splinter, R.; Bevers, R.F.; Zonneveld, W.C.; Putter, H.; Pelger, R.C.; Voorham-van der Zalm, P.J. Effect of preoperative pelvic floor muscle therapy with biofeedback versus standard care on stress urinary incontinence and quality of life in men undergoing laparoscopic radical prostatectomy: A randomised control trial. Neurourol. Urodyn. 2015, 34, 144–150. [Google Scholar] [CrossRef]
- Dubbelman, Y.D.; Groen, J.; Wildhagen, M.F.; Rikken, B.; Bosch, J.L. Urodynamic quantification of decrease in sphincter function after radical prostatectomy: Relation to postoperative continence status and the effect of intensive pelvic floor muscle exercises. Neurourol. Urodyn. 2012, 31, 646–651. [Google Scholar] [CrossRef]
- Dubbelman, Y.; Groen, J.; Wildhagen, M.; Rikken, B.; Bosch, R. Quantification of changes in detrusor function and pressure-flow parameters after radical prostatectomy: Relation to postoperative continence status and the impact of intensity of pelvic floor muscle exercises. Neurourol. Urodyn. 2012, 31, 637–641. [Google Scholar] [CrossRef]
- Dubbelman, Y.; Groen, J.; Wildhagen, M.; Rikken, B.; Bosch, R. The recovery of urinary continence after radical retropubic prostatectomy: A randomized trial comparing the effect of physiotherapist-guided pelvic floor muscle exercises with guidance by an instruction folder only. BJU Int. 2010, 106, 515–522. [Google Scholar] [CrossRef]
- Filocamo, M.; Limarzi, V.; Popolo, G.; Cecconi, F.; Marzocco, M.; Tosto, A.; Nicita, G. Effectiveness of Early Pelvic Floor Rehabilitation Treatment for Post-Prostatectomy Incontinence. Eur. Urol. 2005, 48, 734–738. [Google Scholar] [CrossRef] [PubMed]
- Moore, K.N.; Griffiths, D.; Hughton, A. Urinary incontinence after radical prostatectomy: A randomized controlled trial comparing pelvic muscle exercises with or without electrical stimulation. BJU Int. 1999, 83, 57–65. [Google Scholar] [CrossRef] [PubMed]
- Pannek, J.; König, J.E. Clinical usefulness of pelvic floor reeducation for men undergoing radical prostatectomy. Urol. Int. 2005, 74, 38–43. [Google Scholar] [CrossRef] [PubMed]
- Szczygielska, D.; Knapik, A.; Pop, T.; Rottermund, J.; Saulicz, E. The Effectiveness of Pelvic Floor Muscle Training in Men after Radical Prostatectomy Measured with the Insert Test. Int. J. Environ. Res. Public Health 2022, 19, 2890. [Google Scholar] [CrossRef] [PubMed]
- Terzoni, S.; Montanari, E.; Mora, C.; Ricci, C.; Destrebecq, A. Reducing Urine Leakage after Radical Retropubic Prostatectomy: Pelvic Floor Exercises, Magnetic Innervation or No Treatment? A Quasi-Experimental Study. Rehabil. Nurs. 2013, 38, 153–160. [Google Scholar] [CrossRef] [PubMed]
- Terzoni, S.; Ferrara, P.; Mora, C.; Destrebecq, A. Long-term effect of extracorporeal magnetic innervation for post-prostatectomy urinary incontinence: 1-year follow-up. Int. J. Urol. Nurs. 2021, 16, 26–31. [Google Scholar] [CrossRef]
- Wille, S.; Sobottka, A.; Heidenreich, A.; Hofmann, R. Pelvic floor exercises, electrical stimulation and biofeedback after radical prostatectomy: Results of a prospective randomized trial. J. Urol. 2003, 170, 490–493. [Google Scholar] [CrossRef] [PubMed]
- Zhang, A.Y.; Fu, A.Z.; Moore, S.; Zhu, H.; Strauss, G.; Kresevic, D.; Klein, E.; Ponsky, L.; Bodner, D.R. Is a behavioral treatment for urinary incontinence beneficial to prostate cancer survivors as a follow-up care? J. Cancer Surviv. 2017, 11, 24–31. [Google Scholar] [CrossRef] [PubMed]
- Zopf, E.M.; Bloch, W.; Machtens, S.; Zumbé, J.; Rübben, H.; Marschner, S.; Kleinhorst, C.; Schulte-Frei, B.; Herich, L.; Felsch, M.; et al. Effects of a 15-Month Supervised Exercise Program on Physical and Psychological Outcomes in Prostate Cancer Patients Following Prostatectomy: The ProRehab Study. Integr. Cancer Ther. 2015, 14, 409–418. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
{kind=link}
{kind=link}
| Study | PT | TS | Qol | ED | GS | Other | RoB |
|---|---|---|---|---|---|---|---|
| Ahmed [16] | + | + | + | UE | Low | ||
| Allameh [17] | + | + | Some concerns | ||||
| Anan [18] | + | ICIQ-SF, IPSS, UE, OABSS, G8 score | Some concerns | ||||
| Aydin Sayilan [19] | + | + | + | TU | Low | ||
| Bernardes [20] | + | Daily Pad Used | Low | ||||
| Centemero [21] | + | + | + | UE, MMSE, PGI-I, BD | Low | ||
| De Lira [22] | + | + | + | + | Low | ||
| Faithfull [23] | + | IPSS, ICSmaleSF, SESCI | Low | ||||
| Floratos [24] | + | UE | Low | ||||
| Geraerts [25] | + | + | IPSS, VAS | Low | |||
| Gezginci [26] | + | ICIQ-SF, ICIQ-MLUTS | Low | ||||
| Gomes [27] | + | + | + | BD | Low | ||
| Heydenreich [28] | + | + | + | FACT-P | Low | ||
| Kampen [29] | + | + | VAS | Low | |||
| Laurienzo [30] | + | + | + | IPSS | Low | ||
| Laurienzo [31] | + | + | + | + | Low | ||
| Manassero [32] | + | + | + | VAS, IPSS | Low | ||
| Mariotti [33] | + | + | + | Low | |||
| Mariotti [34] | + | + | + | UE | Some concerns | ||
| Milios [35] | + | + | + | IPSS, EPIC-CP, BD | Low | ||
| Moore [36] | + | + | + | IPSS, BD | Low | ||
| Nilssen [37] | + | + | + | + | UCLA-PCI | Low | |
| Oh [38] | + | + | + | + | + | IPSS | Some concerns |
| Overgard [39] | + | + | + | UCLA-PCI | Low | ||
| Pane-Alemany [40] | + | + | ICIQ-SF | Low | |||
| Perez [41] | + | + | Low | ||||
| Pedriali [42] | + | + | BD | Low | |||
| Porru [43] | + | AUA, uroflowmetry, BD | Low | ||||
| Rajkowska-Labon [44] | + | BD | Some concerns | ||||
| Ribeiro [45] | + | Low | |||||
| Santos [46] | + | + | Low | ||||
| Serdà [47] | + | + | + | FACT-P, WP, 8RM, VAS-UI | Low | ||
| Soto González [48] | + | + | BD | Low | |||
| Strojek [49] | + | + | + | MC, EPIC-26, BDI II | Low | ||
| Tantawy [50] | + | + | I-VAS | Low | |||
| Tienforti [51] | + | + | + | UCLA-PCI, IPSS | Low | ||
| Yamanishi [52] | + | + | Low | ||||
| Yokoyama [53] | + | + | + | BD | Low | ||
| Zhang [54] | + | + | + | + | SPSMQ, BD, UCLA-PCI, IPSS, VAS | Some concerns |
| Reference | Main Objective | Participants | Intervention | Follow-Up | Outcomes |
|---|---|---|---|---|---|
| Anan et al. (2020), Japan [18] | Assessment of the impact of preoperative PFMT on improving UI in men after HoLEP | 70 men with BPH GrA: 35 (aged 72, range 62–83 yr) GrB: 35 (aged 73, range 57–86 yr) | GrA: PFMT—preoperatively (28 days), postoperatively (2nd day after HoLEP). GrB: PFMT—postoperatively (2nd day after HoLEP). In both groups—instructions of PFMT, 3 min of PFMT, at least 3× a day. Assessment: ICIQ-SF, urodynamic examination | 3 days after removal of the catheter, 1st, 3rd, and 6th mth after HoLEP | Preoperative PFMT before HoLEP procedure results in a lower rate of urinary incontinence in men, especially 3 months after surgery. |
| Aydın Sayılan et al. (2018), Turkey [19] | Assessment of the impact of PFMT on the occurrence of UI in patients after RP | 60 men after RP Con: 30 (aged 59.93 ± 6.98 yr) Exp: 30 (aged 63 ± 8.61 yr) | Con: no PFMT, breathing exercises, operation info. Exp: 1–4 PFMT sessions (1 h)—activate PMF in functional positions, 20 contractions of 10 s in 3 positions; 3× of PMFE at home 20× daily—6 mth. Assessment: IDQ, ICIQ-SF, PT | 10 days after catheter removal, 1st, 3rd, and 6th mth AS | Regular PFMT performed for 6 months after RP surgery significantly minimizes UI problems in men. |
| Bernardes et al. (2022), Brazil [20] | Assessment of the effectiveness of acupuncture therapy and PFMT in the treatment of UI in men after RP | 63 men after RP Con: 31 (aged 63.93 ± 7.23 yr) Exp: 32 (64.84 ± 6.4 yr) | Con: 8 PFMT sessions with physiotherapist, daily PFMT at home for 8 weeks. Exp: 8 PFMT sessions with physiotherapist, daily PFMT at home for 8 weeks, 8 sessions of acupuncture. Assessment: PT, daily PT, sociodemographic and clinical questionnaire | Before, 4th, and 8th weeks of therapy | Both PFMT and PFMT combined with acupuncture reduce UI in men after RP. However, after 4 and 8 weeks of therapy, a greater improvement was observed in patients using PFMT associated with acupuncture. |
| Centemero et al. (2010) Italy, [21] | Assessment of the benefits of PFMT in men after RP who started therapy before vs. those who started postoperatively | 118 men after RP Con: 59 (aged 57.5, range 46–67 yr) Exp: 59 (aged 60.5, range 48–68 yr) | Con: sPFMT 2× a week for a month AS, daily PFMT at home. Exp: PFMT 30 days BS: sPFMT 2× a week for 30 min, 30 min of PFMT daily at home; AS: sPFMT 2× a week for a month, daily training at home. Assessment: MMSE, PE, urodynamic testing, 3 d bladder diary, ICS-male-SF, PGI-I, QoL, 24 h PT | 1st and 3rd mth AS | Men who started PFMT BS had a lower risk of UI after RP. Early PFMT reduced UI problems compared to men who only exercised AS. |
| Faithfull et al. (2022), United States [23] | Evaluation of the effectiveness of rehabilitation in improving the symptoms of the urinary system in patients with prostate cancer | 63 men with prostate cancer after radiotherapy Con: 32 (aged 72.2 ± 6.7 yr) Exp: 31 (aged 69.9 ± 7.3 yr) | Con: standard care—control visits to the hospital, telephone support. Exp: 4 group sessions (60–90 min), 1 individual session (40 min), 2 phone sessions for 10 weeks—education, PMEs, homework; then 4 months of self-therapy at home. Assessment: IPSS, ICS-male-SF, EORTC QLQ-PR-25, EORTC QLQ-30, SESCI | 2 weeks before physiotherapy (baseline), 3 and 6 mth post-baseline | After 3 months, physiotherapy significantly reduced voiding and incontinence symptoms in men with prostate cancer compared to standard care. Unfortunately, the results did not persist to the 6th month of the study. |
| Gezginci et al. (2022), Turkey [26] | Assessment of perioperative PFMT on UI and QOL levels in men after RP | 60 men after RP Con: 30 (aged 69.2 ± 5.4 yr) Exp: 30 (aged 67.6 ± 6.7 yr) | Con: standard care without physiotherapy. Exp: training on admission to the clinic—PMEs, bladder control technique, lifestyle change; PMEs for surgery and after catheter removal—continuation of PMEs for 3 months at home, telephone check once a week. Assessment: ICIQ-SF, ICIQ-MLUTS | 7 days after catheter removal, 3 mth AS | Men who performed perioperative PMEs had fewer urinary problems than those in the control group. Physiotherapy also improved the quality of life of patients after RP. |
| Heydenreich et al. (2020), Germany [28] | Assessment of the impact of sensorimotor training with an oscillating rod compared to standard PFMT on the reduction of UI level, recovery time and quality of life in men after RP | 184 men after RP Con: 91 (aged 64.3 ± 7.4 yr) Exp: 93 (aged 64.0 ± 6.5 yr) | Con: 30 min relaxation training combined with supervised PFMT. Exp: sPFFT with coordinated use of an oscillating rod (30 min). Supervised PFFT 30 min in both groups, 1 session daily for 3 wk. Assessment: 1 h + 24 h PT, HRQL, FACT-P | Before and 3 wk after therapy | Experimental training—better results and a significant reduction in UI as well as improved quality of life in men after RP. Improvement of continence in both trainings. |
| Van Kampen et al. (2000), Belgium [29] | Assessment of the impact of PMF reeducation on the improvement of continence in patients after RP with UI | 102 men after RP Con: 52 (aged 66.58 ± 0.8 yr) Exp: 50 (aged 64.36 ± 0.81 yr) Eventually, after 1 year, 48 men from Exp. And 50 from Con. Finished the trial. | Con: education about UI after RP, false ES—false interferential current (placebo), 1 session a wk for max. year. Exp: education about PMF and urinary system, sPFMT with BF—patients who could not stretch PMF received AES, 90 contractions of PMF daily at home in 3 positions, activating PMF in daily activities. Supervised training 1× a wk for max. year. Assessment: 1 h + 24 h PT, VAS | BS, 1st, 3rd, 6th, and 12th mth after start therapy | Men who underwent PMF re-education saw faster and better results in the reduction of UI symptoms after RP than in the placebo group. |
| Manassero et al. (2007), Italy [32] | Assessment of the influence of early, intense and long-term PMEs on the incidence of UI in men after bladder-sparing RRP surgery | 107 men after RRP Con: 53 (aged 67.9 ± 5.5 yr) Exp: 54 (aged 66.8 ± 6.3 yr) Eventually, after 1 year, 54 men from Exp. and 40 men from Con. finished the trial. | Con: no intervention. Exp: Verbal feedback to teach PMF, PMEs at home: 45 contractions (3 series of 15×)—max. 90 contractions daily, PMF activation in daily activities. Assessment: 24 h PT, VAS, PE, IPSS, QoL | 1st, 3rd, 6th, and 12th mth AS | PFMT significantly influences the improvement of continence in men after RRP in comparison with control. The therapeutic effect of physiotherapy lasts for at least 12 mth and shows no side effects. |
| Milios et al. (2019), Australia [35] | Assessment of the effectiveness of basic PFMT compared to intense PFMT focused on the activation of slow and fast twitch fibers in men after RP/RALP | 97 men after RP/RALP Con: 47 (aged 63.5 ± 6.8 yr) Exp: 50 (aged 62.2 ± 6.8 yr) | All: 2× 30 min sessions about PFMT. PFMT started 5 wk BS. To learn PMEs was used RTUS with BF. All continued PFMT for 12 wk AS. Con: 3× of PMF: contraction 10 s, relax 10 s (30× per day) in 3 positions. Exp: 6 sessions of 10 quick contractions (1 s) and 10 slow (10 s) with equal relaxation time (120× per day) in standing. Assessment: 24 h PT, bladder diary, IPSS, EPIC-CP, RTUS PFM, QoL | BS, 2nd, 6th, and 12th mth AS | Better effectiveness of therapy, reduction of UI and improvement of QoL in patients who received intensive PFMT therapy compared to patients with basic PFMT training. |
| Nilssen et al. (2012), Norway [37] | Effect of supervised postoperative PFMT on quality of life parameters in patients after RP | 80 men after RP Gr.1: 38 (aged 60, range 48–68 yr) Gr.2: 42 (aged 62, range 49–72 yr) | Gr.1: 45 min sPFMT, 1× a wk up to 12 mth AS; at home: 3 series of PMEs in 3 positions, 10 contractions, 6–8 s each + at the end of each 3–4 quick contractions; men who could not come to the training received a DVD with PFMT (n = 20). Gr.2: instructions of postoperative PFMT, 3 series of 10× per day. Assessment: UCLA-PCI, SF-12 | Before the therapy, 6th wk, and 3rd, 6th, and 12th mth AS | Significant reduction of postoperative UI symptoms in patients undergoing sPFMT compared to the control. No better results were obtained with HRQoL parameters. |
| Pedriali et al. (2015), Brazil [42] | Evaluation of the effectiveness of Pilates exercises in comparison to the traditional PFMT in the treatment of UI in men after RP | 85 men after RP Gr.1: 26 (aged 66.07 ± 5.77 yr) Gr.2: 28 (aged 66.32 ± 5.48 yr) Con: 31 (aged 62.61 ± 7.26 yr) | All men were taught to work with the BF at baseline assessment. Gr.1: 10 supervised sessions of 45 min of Pilates exercises, 3 exercises and 2 Pilates exercises at home every day. Gr.2: 10 individual PFMT sessions in combination with AES, 1× a wk, 40–50 min; SUI: AES—frequency 50 Hz, 20 min; UUI—frequency 4 Hz, 20 min; MUI—both AES parameters; after each AES, 3 series of 10 strong contractions in 3 positions. Con: no intervention. Assessment: 24 h PT, 3 day bladder diary, daily pads usage, ICIQ-SF | 4th wk and 4th mth AS | The Pilates method is as effective as the standard PFMT. There were no statistically significant differences in the number of pads used between men from both intervention groups in the results of the 24 h PT and ICIQ-SF. Both intervention groups achieved greater improvement over Con. |
| Porru et al. (2001), Italy [43] | To evaluate the effect of PFMT on UI, including urinary frequency, postmicturition dribbling, and quality of life in patients after TURP | 58 men Con: 28 (aged 66.0, range 53–71 yr) Exp: 30 (aged 67.5, range 55–73 yr) | Exp: instruction, feedback about contractions, PMEs at home, 3 sessions of 15× daily. Con: no intervention. Assessment: AUA, QoL, ICS male questionnaire, uroflowmetry, digital evaluation of PMF, voiding diary | BS and 30 days AS | Men performing PFMT obtained a significantly higher degree of PMF strength, fewer UI symptoms, and better QoL than the control. |
| De Santana Santos et al. (2017) [46] | Analysis of the effectiveness of physiotherapy with PFMT + BF in the treatment of UI in men after RP | 13 men up to 3 mth after RP Con: 6 (aged 62, range 54–74 yr) Exp: 7 (aged 65.6, range 58–70 yr) | Exp: education + instruction of PMEs at home, 1× wk for 8 wk: BF (20 min) + PMEs. Con: education + instruction of PMEs for home, PMEs in clinic. Assessment: before the start of therapy, on the 5th and 9th visits, 1 h PT | A similar reduction in UI symptoms was observed in both groups after 2 months of treatment. | |
| Strojek et al. (2021), Poland [49] | Assessment of the effectiveness of PFMT in the treatment of SUI in men after RP | 34 men Con: 15 (aged 64.2 ± 4.5 yr) Exp: 19 aged 61.4 ± 7.4 yr) | Con: no intervention. Exp: 24 individual sessions of PFMT in 3 positions, 2× a wk—2 wk AS—number of repetitions—individual; before PFMT: postural correction, mobilization of sacroiliac + sacro-lumbar joints, respiration exercises. Assessment: myostatin concentration, BDI-II, EPIC-26 | At baseline and after 12th wk of therapy | PFMT significantly improves the overall quality of life of men after RP, while the lack of intervention reduces it in the ‘overall urinary problems’ and ‘sexual’ domains. PFMT also reduces the concentration of myostatin and the risk of developing depressive disorders. |
| Overgard et al. (2008), Norway [39] | Assessment of the impact of sPFMT on the occurrence of UI in men after RP | 80 men Exp1: 38 (aged 60.0, range 48–68 yr) Exp2: 42 (aged 62.0, range 49–72 yr) | Exp1: sPFMT, 45 min a wk, at home—3 sessions of 10× in 3 positions—contraction 6–8 s + 3–4 quick contractions; instruction; men who could not come to the training received a DVD with PFMT. Exp2: instruction on postoperative training—3 sessions of 10× of PMEs. Assessment: UCLA-PCI, physiotherapeutic evaluation, 24 h PT, per rectum examination | BS, 6th wk, 3rd, 6th, and 12th mth AS | After 3 mth, no significant differences in UI were found between groups. However, after 12 mth, a significant improvement in urinary continence was observed in men who participated in sPFMT. |
| Tantawy et al. (2019), Egypt [50] | Effect of whole body vibration training on the occurrence of SUI in men after prostate cancer surgery | 61 men Gr.1: 30 (aged 64.3 ± 5 yr) Gr.2: 31 (63.6 ± 5.8 yr) | Gr.1: PFMT + WBVT, 3× a wk for 4 wk: 1–2 session—frequency 20 Hz, peak to peak displacement of 2 mm, duration of each set of 45 s followed by 60 s rest; 3–12 session—a frequency of 40 Hz, peak-to-peak displacement of 4 mm, duration of each set of 60 s followed by 60 s rest. Gr.2: PFMT. All men received the same guidelines for PFMT: PMEs daily, in 3 positions, 10 s of contraction, 10 s of relaxation, 15×; for slow twitch fibers, the time of contraction and relaxation was increased by 1 s every wk; fast twitch fibers—quick contractions and relaxation of PMF, 20×, then 10 s of rest—initially 2 sets, finally 4 sets. Assessment: I-VAS, ICIQ-SF, 24 h PT | Before therapy, after 4 wk of treatment and after 2 mth of observation | Improvement in SUI symptoms was noted in men after both PFMT and WBVT combined therapy, as well as after PFMT alone. |
| Reference | Main Objective | Participants | Intervention | Follow-up | Outcomes |
|---|---|---|---|---|---|
| Allameh et al. (2021), Iran [17] | Assessment of the effectiveness of pre- and postoperative PFMT and BF in the treatment of UI in men after RP | 57 men after RP Con: 19 (aged 70.6 ± 6.8 yr) Exp1: 19 (aged 69.0 ± 5.7 yr) Exp2: 19 (aged 68.4 ± 6.9 yr) | Con: nonfunctional probes of BF before and after RP, instruction of PFMT after RP. Exp1: 30 min of BF 2× a wk before 2 wk of RP, nonfunctional BF after RP, instruction of PFMT after RP. Exp2: nonfunctional BF before RP, 30 min of BF 2× a wk after RP, instruction of PFMT after RP. Assessment: 24 h PT | 1st, 3rd, and 6th mth after catheter removal, | Compared to the lack of therapy, the use of BF before or after surgery significantly improves continence in men within 1 and 3 months after RP. |
| De Lira et al. (2019), Brazil [22] | Assessment of the impact of perioperative PFMT in comparison with standard care on minimizing the symptoms of UI and erectile dysfunction in men after RP | 31 men after RP Con: 15 (aged 63.53 ± 7.62 yr) Exp: 16 (aged 67.3 ± 5.63 yr) | Con: no intervention. Exp: sPFMT + BF: 2 session BS, PFMT at home 3× a day BS and AS. Assessment: ICIQ-SF, IIEF-5, electromyographic recordings of the pelvic floor | Before and 3 mth AS | sPFMT and home training instructions do not minimize UI and erection problems in men after RP. |
| Floratos et al. (2002), the Netherlands [24] | Compare the effectiveness of EMG with verbal instructions as tools for learning PME in the early treatment of UI after RP | 42 men after RP Con: 14 (aged 65.8 ± 4.3 yr) Exp: 28 (aged 63.1 ± 4.0 yr) | Con: palpation + verbal feedback, leaflet about PMEs, telephone consultations, 80–100× PMEs at home daily (4 sessions of 20–25×). Exp: 30 min, 15 series, 3× a wk EMG BF, 50–100× of PMEs daily at home. Assessment: 1 h PT, individual questionnaire, urodynamic examination at mth 6 of men with UI | 1, 2, 3 and 6 mth after start therapy | Verbal feedback and BF combined with EMG are effective methods in learning PMEs in men after RP. Both methods are effective in minimizing the symptoms of UI. |
| Geraerts et al. (2013), Belgium [25] | Comparative evaluation of the effects of PFMT before and after ORP/RARP surgery in the treatment of UI with the effectiveness of only postoperative training | 180 men after ORP/RARP Con: 89 (aged 62.04 ± 6.33 yr) Exp: 91 (aged 61.88 ± 5.90 yr) 12 months after surgery, 85 men were finally evaluated in both groups. | Con: after catheterization—1 sPFMT with EMG BF, information about PMEs, PMF activation in everyday activities. Exp: 3 wk BS—sPFMT EMG BF training, 3× 30 min, 1× a wk, PMEs at home 60 contractions, activation PMF in everyday activities; PFMT 4 days AS. Assessment: 1 h + 24 h PT, VAS, IPSS, KHQ | BS, 1st, 3rd, 6th, and 12th mth AS | Pre- and postoperative as well as exclusively postoperative PFMT show a similar therapeutic effect in the treatment of UI in men after ORP or RARP. |
| Moore et al. (2008), Canada [36] | Assessment of the effectiveness of PFMT in comparison to telemedicine with a urology nurse in men after RP | Con: 77 Exp: 89 | Con: contact with nurse, verbal, and written instruction about PFMT: 5–10 s contraction, 10–20 s relaxation, 12–20 repetitions, 3× a day at home. Exp: verbal and written instructions about PFMT, BF training: 30 min, 1× a wk—strength: 5–10 s contraction, 10–20 s rest, 12–20×; endurance: 50–60% of max strength, 20–60 s contraction and relaxation, 6–8×; speed: 5–10 contraction during 10 s, 20 s rest period; control: contractions in 3 stages, 15 s of slow release, 15 s rest, 6–10×; penile lift exercises + 3× a day at home on nontreatment days. Assessment: 24 h PT, IPSS, IIQ-7 | At baseline, 4th, 8th, 12th, 16th, 26th wk and 1 yr | At individual stages of the assessment, both groups showed a similar improvement of continence in men. |
| Oh et al. (2020), Korea [38] | Evaluation of the effectiveness of the innovative BF device—Anykegel in PFMT in men with UI after RARP | 82 men Con: 42 (aged 65.9 ± 6.8 yr) Exp: 40 (67.5 ± 6.9 yr) | Con: verbal and written instruction—instructions were given in three different way—4× a day, 10 min of exercises, min. 10 s of tension duration and max. tension intensity. Exp: verbal and written instruction + BF Any kegel, 4× a day, 10 min of exercises session, 10 s of tension. Assessment: physical examination, 24 h PT, IPSS, IIEF-5 | BS, 1st, 2nd, and 3rd mth after catheter removal | BF has a significant impact on the treatment of UI in men after RARP, especially in the early postoperative period. |
| Perez et al. (2018), Brazil [41] | Assessment of BF as a preventive measure against UI and erectile dysfunction in men after RP | 52 men after RP Con: 32 (aged 66.3 ± 5.8 yr) Exp: 20 (aged 64.0 ± 4.6 yr) | Con: no intervention. Exp: BF BS; the therapy started with pressure taring—3 max. PMF contractions, followed by 7 min fast and 6 min slow; 10 sessions. Assessment: KHQ, IIEF-5 | Before therapy and AS | Men exercising PFMT with BF before the surgery suffered significantly less for UI and erectile dysfunction than the control. |
| Rajkowska-Labon et al. (2014), Poland [44] | Evaluation of the effectiveness of physiotherapeutic methods in comparison to the lack of therapy in the treatment of UI in men after RP | 81 men after RP Con: 32 (aged 68.3 ± 6.49 yr) Exp1: 23 (aged 66.9 ± 7.07 yr) Exp2: 26 (aged 68.8 ± 6.59 yr) | Con: no intervention. Exp1: PFMT + BF, 1× a wk, 20–30 min; PFMT + SSS, 1× a wk, 30 min; PFMT in 3 positions at home, 3× a day, 15–20 min. Exp2: PFMT + SSS, 2× wk, 30 min; PFMT at home (the same as Exp1.). Assessment: 1 h + 24 h PT, sEMG, patients’ self-reported subjective assessment | Exp 1. + 2: at baseline and end of therapy (max. 1 yr), Con: at baseline and 1 yr AS | Physiotherapeutic treatment significantly reduces the symptoms of RUI after RP compared to no treatment. However, treatment with PFMT + SSS resulted in no UI problems among 92.3% of men, while PFMT + BF only of 39.1%. |
| Serdà et al. (2014), Spain [47] | Design and implementation of the PFMT program to improve UI | 66 men Con: 33 (aged 71.78 ± 6.82 yr) Exp: 33 (aged 71.09 ± 8.1 yr) | Con: no intervention. Exp: global postural re-education, PFMT + BF, exercises to radiate muscular strength—24 wk—16 wk with specialists + 8 wk of autonomous training, 2× for wk, time: 60 min. Assessment: 20-min nappy test, VAS-UI, FACT-P, the waist perimeter, muscular resistance (8RM) | At baseline and at the end of therapy (24 wk) | The rehabilitation program combined with PFMT significantly improves the symptoms of UI in patients with prostate cancer. Improvement of UI problems correlates with an improvement in the quality of life of patients. |
| Tienforti et al. (2012), Italy [51] | Evaluation of the effectiveness of preoperative BF + low-intensity program of postoperative perineal physiokinesitherapy in reducing the frequency, duration and severity of UI in men after RP | 32 men after RRP Con: 16 (aged 67, range 60–74 yr) Exp: 16 (aged 64, range 52–74 yr) | Exp: PMF education, supervised BF training the BS and after catheter removal (BF: 20 min, 1× a month), PFMT instructions, home exercises: 3× 10 min a day, 5 s contraction, 5 s relaxation. Con: standard care, after catheterization: instructions of PMEs at home—3× a day for 10 min until achieved continence. Assessment: ICIQ-Overactive Bladder, UCLA-PCI, IPSS-QOL, ICIQ-UI | Exp. assessed at each mth visit, Con. after 1, 3, and 6 mth after catheter removal | Significant improvement after 3 and 6 mth in the number of pads used and the number of UI episodes in patients in the intervention group compared to the control. |
| Ribeiro et al. (2010), Brazil [45] | Assessment of the effectiveness of PFMT with BF method in improving UI in men within 12 mth after RP | 73 men after RP Con: 37 (aged 65.6 ± 8.0 yr) Exp: 36 (aged 62.2 ± 6.3 yr) 54 patients were included in the final evaluation Con: 28 Exp: 26 | Exp: From the 15th day AS BF-PFMT treatment, 1× a wk, for a max. 12 wk or until the symptoms of UI stop. 30 min session, BF-PFMT with electromyographic machine. Instructions for daily home training in 3 positions. Con: instruction from a urologist, no recommendations. Assessment: number of pads/day, 24 h PT, ICSI, ICST, IIQ-7, QOL, the Oxford scale. | BS, 1st, 3rd, 6th, and 12 mth AS | The implementation of early BF-PFMT in men after RP significantly improves continence, reduces the frequency of episodes, and improves the strength of PFM 12 mth after surgery compared to the control. |
| Zhang et al. (2015), USA [54] | Assessment of the effectiveness of combining PFMT with a symptom self-management in reducing UI symptoms in patients with prostate cancer | 244 men Con: 82 (aged 64.9 ± 8.2 yr) Exp1: 81 (aged 66.8 ± 7.2 yr) Exp2: 81 (aged 64.3 ± 7.3 yr) | Con: usual care, without any intervention. Exp1: PFMT + BF + support group + PST: 3–5 participants, time: 60–75 min; 6 biweekly sessions for 3 mth. Exp2: PFMT + BF + individual telephone contact with a therapist, time + PST: 45 min; 6 biweekly sessions for 3 mth. Assessment: ICSmaleSF, SPMSQ | At baseline, 3 mth after intervention and at 6 mth | Both intervention groups showed a lower frequency of daily leakage of urine after 3 mth (but not 6 mth) than in the control. However, after 6 mth, they reported fewer UI problems than the men in the control group. |
| Reference | Main Objective | Participants | Intervention | Follow up | Outcomes |
|---|---|---|---|---|---|
| Ahmed et al. (2012), Egypt [16] | Assessment of the influence of PFMT, ES and BF on the occurrence of UI in men after RP | 80 men after RP Exp1: 26 (aged 57.2 ± 3.25 yr) Exp2: 26 (aged 58.8 ± 5.4 yr) Exp3.: 28 (aged 56.3 ± 6.8 yr) | Exp1: instructions + leaflet with PMEs—3 series of 15–20× a day. Exp2: 15 min, 2× a wk (12 wk); frequency: 50 Hz; pulse width: 300 μs; intensity: maximum tolerated. Exp3: 15 min BF + 15 min ES, 2× a wk (12 wk), 3× of 10 quick contractions; 3 contractions for 5, 7, or 10 s; 10 contractions on prolonged exhalation. Assessment: 24 h PT, IIQ-7, urodynamic test only in men with UI after 6 mth | wk after catheter removal, at 6 and 12 wk during intervention, and 24 wk after catheterization | Improvement in continence was noted in all study groups. The greatest effect was obtained by men undergoing combined therapy—BF + ES, both for the duration and degree of UI and QoL. |
| Gomes et al. (2018), Brazil [27] | Assessment of the impact of Pilates exercise compared to the conventional PFMT protocol on pelvic floor muscle strength in patients with UI after RP | 104 men after RP Gr.1: 34 (aged 66.62 ± 5.66 yr) Gr.2: 35 (aged 65.83 ± 5.64 yr) Con: 35 (aged 63.11 ± 7.19 yr) | Gr.1: 10 supervised Pilates training—1× a wk, 45 min; instructions for daily home exercises. Gr.2: SUI: AES frequency 50 Hz, 20 min; UUI: frequency 4 Hz, 20 min; MUI: both of the above electrical parameters. All performed after AES PFMT—3× of 10 contractions—10 s, PFMT, once a wk, 45 min; instructions for daily home exercises. Con: no intervention. Assessment: 24 h PT, ICIQ-SF, a manometric perineometry, voiding diary | Before and 4 mth AS | The improvement in PFMT parameters was greater in the actively treated groups compared to the control group. Traditional PFMT combined with AES and the Pilates method have a similar effectiveness in minimizing UI symptoms in men after RP. |
| Laurienzo et al. (2018), Brazil [30] | Assessment of the effect of ES and PFMT on muscle strength, erection, and UI in men with prostate cancer treated with RP | 123 men after RP Con: 40 (aged 57.3 ± 6.5 yr) Gr.1: 41 (aged 58 ± 5.7 yr) Gr.2: 42 (aged 58.5 ± 5.4 yr) | Con: information on postoperative management. Gr.1: 3 types of PMEs at home, 2–3× daily for 6 mth. Gr.2: PMEs (identical to Gr.1), AES, 2× a wk, for 7 wk, frequency 35 Hz, pulse width 1 ms, rise time 2 s, stimulus duration 6 s, fall time 2 s, standing time 12 s, intensity adapted to the patient. Assessment: 1 h PT, ICIQ-SF, IIEF-5, IPSS, perineometer | BS, 1st, 3rd, and 6th mth AS | After 6 months of the study, an improvement in the strength of PMF, a reduction in UI symptoms and erectile dysfunction in men from each group was shown. Nevertheless, no statistical differences were found between the groups. |
| Laurienzo et al. (2013), Brazil [31] | Evaluation of the effectiveness of the use in the treatment of UI of preoperative ES in men after RRP | 49 men after RRP Con: 15 (aged 64.0 ± 8 yr) Gr.1: 17 (62.0 ± 7 yr) Gr.2: 17 (60.0 ± 8 yr) | Con: instruction about PMEs. Gr.1: Kegel exercises. Gr.2: BS: PMEs—5 s contraction in 3 positions for 10× + 10× ES: tonic fibers—frequency 20 Hz, pulse width 700 μs, rise time 2 s, descent time 2 s, working time 6 s, rest time 6 s, time 10 min; phase fibers—frequency 65 Hz, pulse width 150 μs, rise time 2 s, descent time 2 s, working time 6 s, rest time 18 s, time 5 min. Assessment: 1 h PT, ICIQ-SF | 1st, 3rd, and 6th mth AS | There were no significant differences between men in the level of UI and QoL. |
| Mariotti et al. (2009), Italy [33] | Analysis of the benefits of the early FES and BF therapy in terms of recovery time and improvement in continence in men after RP | 60 men after RP Con: 30 (aged 61.43 ± 3.60 yr) Exp: 30 (aged 61.86 ± 3.26 yr) | Con: PMF instruction, written examples of Kegel exercises. Exp: 2 sessions for 6 wk: BF—15 min, FES—frequency 30 Hz for 10 min, then 50 Hz for 10 min—all 20 min, pulse duration 300 μs, max. output 24 mA, intensity adjusted to the patient. Assessment: 24 h PT, ICS-male questionnaire | Before therapy; at 2nd and 4th wk; and 2nd, 3rd, 4th, 5th, and 6th mth after start of therapy | Early, non-invasive physical treatment with the BF and FES of the pelvic floor has a significant positive effect on the improvement of UI in men after RP between the 4th wk and the 6th mth of follow-up. One year AS 58 out of 60 men did not suffer from UI. |
| Mariotti et al. (2015), Italy [34] | Assessment of the effectiveness of FES + BF therapy in terms of recovery time and rate of continence in men with UI after RP | 120 men RP Exp1: 60 (aged 59.61 ± 4.03 yr) Exp2: 60 (aged 59.28 ± 4.19 yr) | In both groups: FES + BF: 2× a wk for 6 wk, BF—15 min + verbal guidance, exercises in 3 positions, FES—20 min—pulsed at 30 Hz (first 10 min) + 50 Hz (second 10 min), square waves—300-μs pulse duration + max. output—24 mA, intensity adjusted to the patient. Exp1: started 14 days after catheter removal. Exp2: AS—verbal and written instruction of PFMT; FES + BF—12 mth AS. Assessment: 24 h PT, ICS-male questionnaire | Time 0—before therapy and 14 days after catheter removal—Exp1. and 12 mth AS—Exp2.; at 2 and 4 wk and 2, 3, 4, 5, and 6 mth after start of treatment | FES + BF therapy significantly reduces the symptoms of UI in men after RP, regardless of the time of its initiation. |
| Pané-Alemany et al. (2021), Spain [40] | Assessment of the effectiveness of transcutaneous perineal electrostimulation and intracavitary electrostimulation in the treatment of UI and the impact on QOL in men after RP | 70 men after RP Con: 35 (aged 62.7 ± 10.2 yr) Exp: 35 (aged 62.9 ± 8.8 yr) | Con: transcutaneous perineal electrostimulation, PFMT. Exp: anal electrostimulation, PFMT. Parameters in both groups: 15 min—10 min, frequency 30 Hz, pulse width 0.25 ms, intensity 10–30 mA, no on-off cycles; 5 min—frequency 50 Hz, pulse width 0.25 ms, intensity 1–50 mA, individually time of on-off cycles; PFMT with physiotherapist and at home: 20 contractions (10× 8–10 s, 10× 3 s), 3× daily for 10 wk. Assessment: physical examination with OXFROD scale, 24 h PT, ICIQ-SF, SF-12, I-QoL test | Baseline, at 6 and 10 session | Regardless of the type of electrostimulation, improvement in continence and quality of life was noted in both groups. |
| Soto-González et al. (2020), Spain [48] | Analysis of the effectiveness of 3-month ES and BF therapy in the treatment of UI in patients after RP | 47 men after RP Con: 22 Exp: 25 | All -instruction of PMF exercises at home. Exp: ES and BF, 3× a wk for 3 months, ES: 15 min, 300 ns pulse duration, maximum intensity 24 mA; BF: 30 min. Con: no intervention. Assessment: 1 h and 24 h PT, urinary diary, ICIQ-SF | Before therapy, after 1st, 2nd, 3rd, and 6th mth of therapy | After 3 months of treatment was observed a positive effect of the combined therapy (ES and BF) on the occurrence of UI in men after RP. Moreover, it also leads to an improvement in the QoL. |
| Yamanishi et al. (2010), Japan [52] | Evaluation of the effectiveness of ES therapy combined with PFMT in the treatment of UI in patients after RP | 56 men after RP Con: 30 (aged 68.0 ± 5.6 yr) Exp: 26 (aged 65.4 ± 5.6 yr) | All performed preoperative PFMT and continued it. Exp: AES: 15 min, 2× a day, frequency 50 Hz, pulse duration 300 μs, max. output 70 mA (5 s on, 5 s off). Con: sham AES: 15 min, 2× a day, frequency 50 Hz, pulse duration 300 μs, max. output 3 mA (2 s on, 13 s off). Assessment: 3-day PT, ICIQ-SF, KHQ | wk after catheterization, 1, 3, 6, and 12 mth from the start of therapy | The continence rate was significantly higher in men with active AES than with sham AES after 1, 3, and 6 mth of treatment. However, similar differences were not shown at 12 mth, while at 6 mth the difference was small. |
| Yokoyama et al. (2004), Japan [53] | Assessment of the effectiveness of ExMI and FES in the treatment of UI in men after RRP | 36 men after RRP FES: 12 (67.2 ± 6.7 yr) ExMI: 12 (68.2 ± 4.9 yr) Con: 12 (66.2 ± 7.6 yr) | FES: 15 min, 2× a day for a mth, pulses of 20 Hz square waves at a 300 s pulse duration and a max. output current of 24 mA. ExMI: 20 min, 2× a wk for 2 months, the frequency 10 Hz, intermittently for 1 min, followed by a rest period of min, a second treatment at 50 Hz intermittently for 10 min. Con: PFMT learning (rectal examination), instructions for home exercises. Assessment: bladder diaries, 24 h PT, quality of life survey | 1, 2 and 4 wk and 2, 3, 4, 5 and 6 mth after catheter removal | FES and ExMI therapy enables faster UI improvement in men after RRP than at home PFMT. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mazur-Bialy, A.; Tim, S.; Kołomańska-Bogucka, D.; Burzyński, B.; Jurys, T.; Pławiak, N. Physiotherapy as an Effective Method to Support the Treatment of Male Urinary Incontinence: A Systematic Review. J. Clin. Med. 2023, 12, 2536. https://doi.org/10.3390/jcm12072536
Mazur-Bialy A, Tim S, Kołomańska-Bogucka D, Burzyński B, Jurys T, Pławiak N. Physiotherapy as an Effective Method to Support the Treatment of Male Urinary Incontinence: A Systematic Review. Journal of Clinical Medicine. 2023; 12(7):2536. https://doi.org/10.3390/jcm12072536
Chicago/Turabian StyleMazur-Bialy, Agnieszka, Sabina Tim, Daria Kołomańska-Bogucka, Bartłomiej Burzyński, Tomasz Jurys, and Natalia Pławiak. 2023. "Physiotherapy as an Effective Method to Support the Treatment of Male Urinary Incontinence: A Systematic Review" Journal of Clinical Medicine 12, no. 7: 2536. https://doi.org/10.3390/jcm12072536