
Immunotherapy vs. Chemotherapy in Subsequent Treatment of Malignant Pleural Mesothelioma: Which Is Better?

Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction and Study Outcomes
2.4. Risk of Bias for Articles in the Meta-Analysis
2.5. Statistical Analysis
3. Results
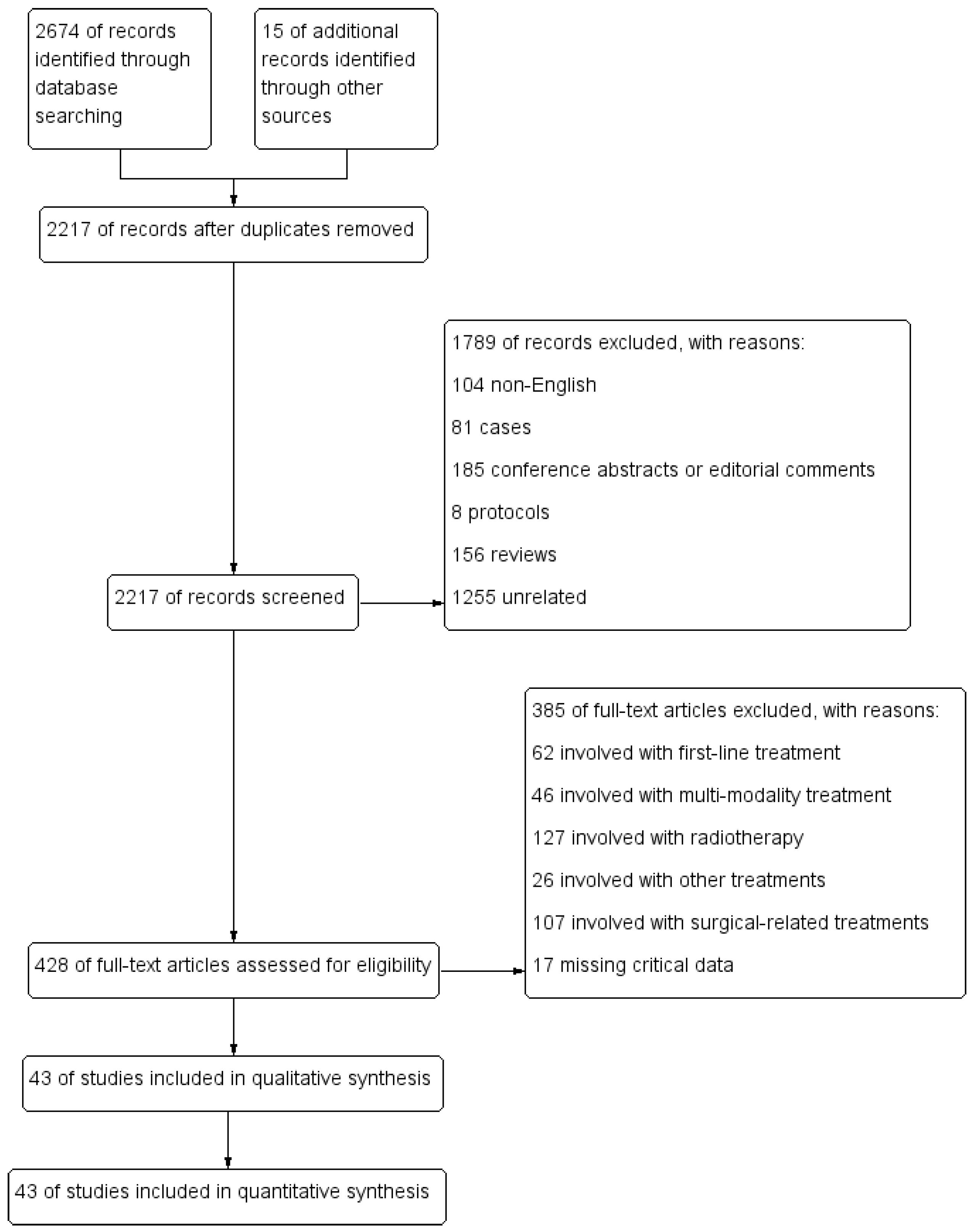
3.1. Article Selection
3.2. Characteristics of Included Studies
3.3. Risk of Bias
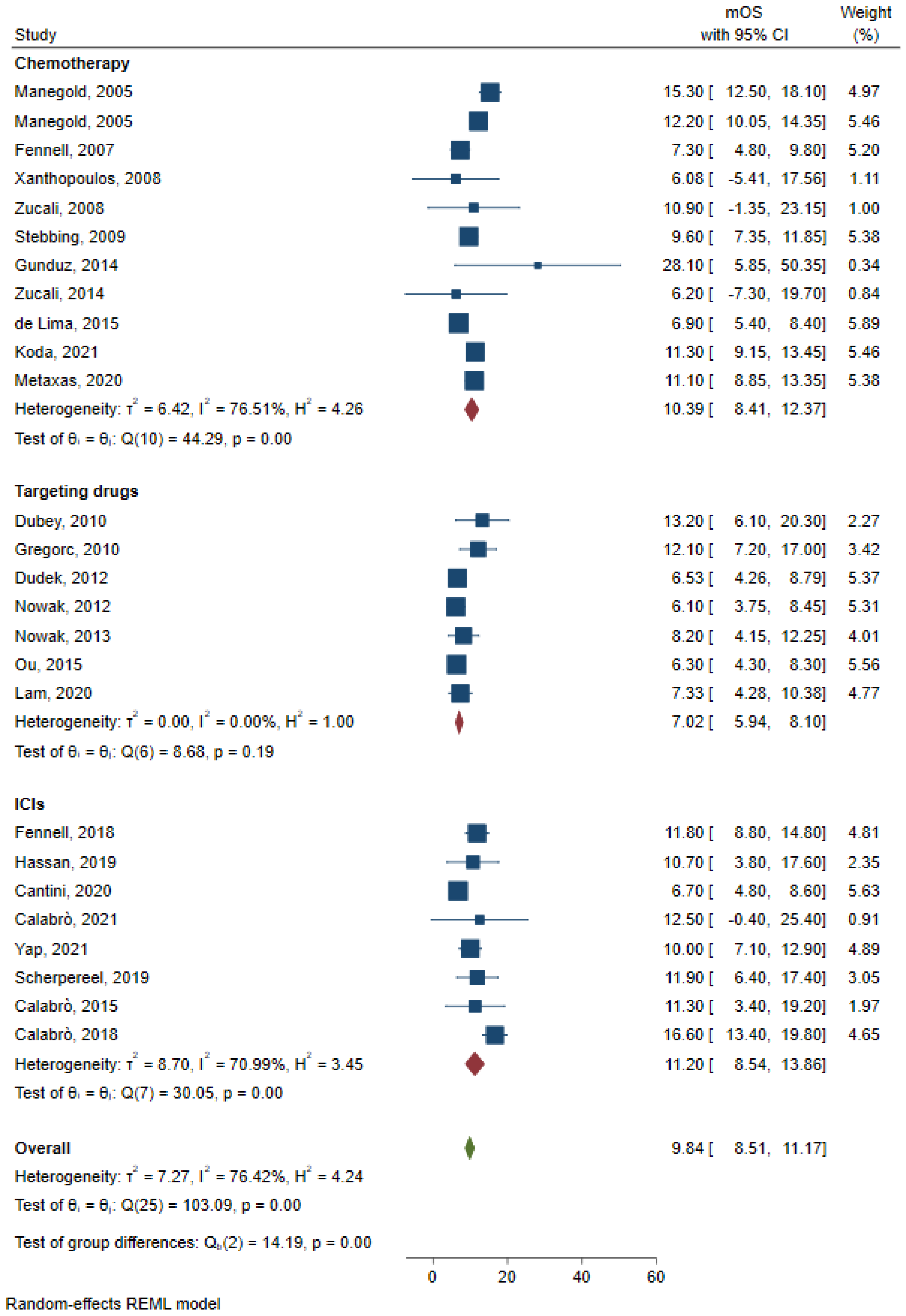
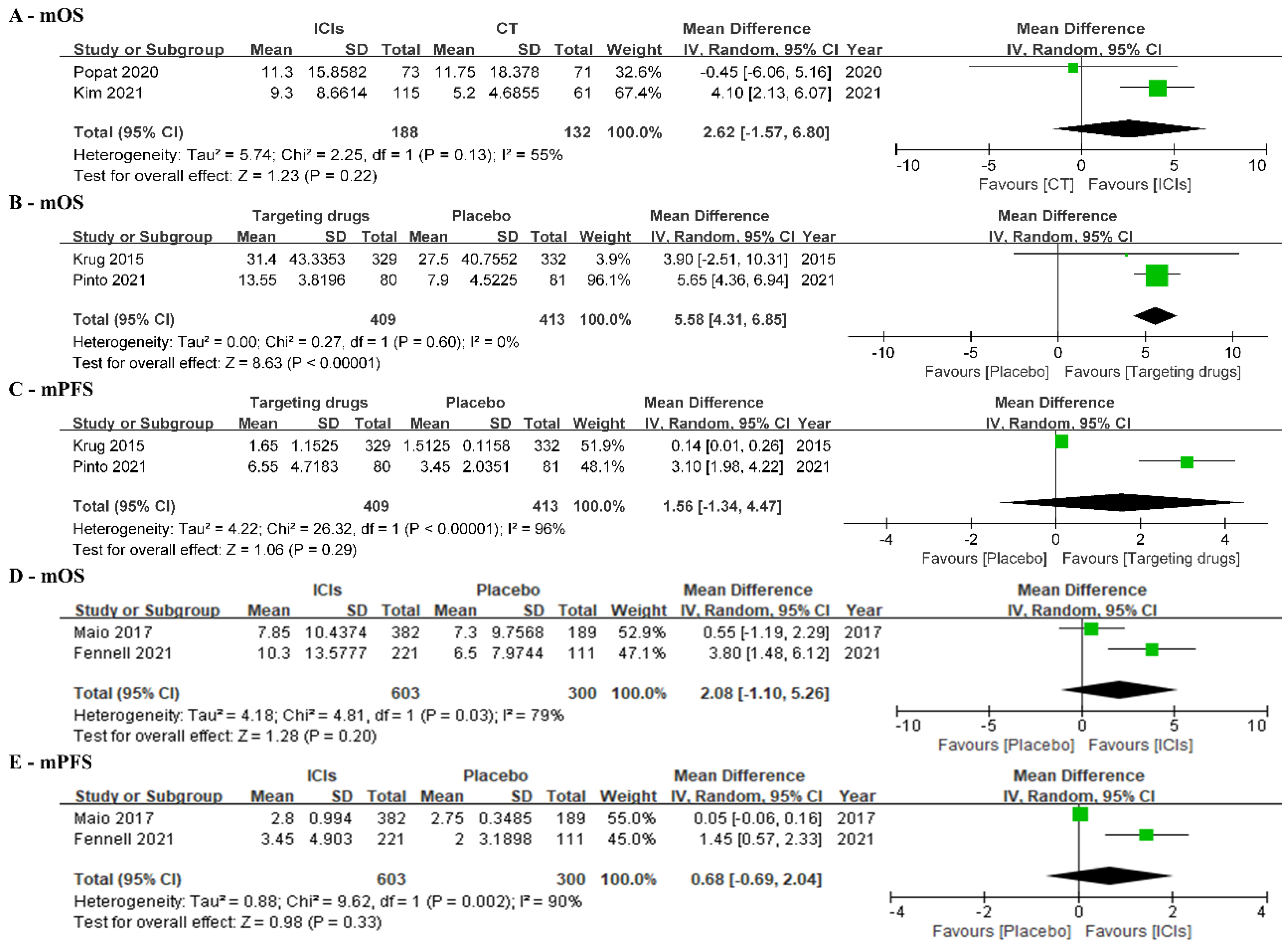
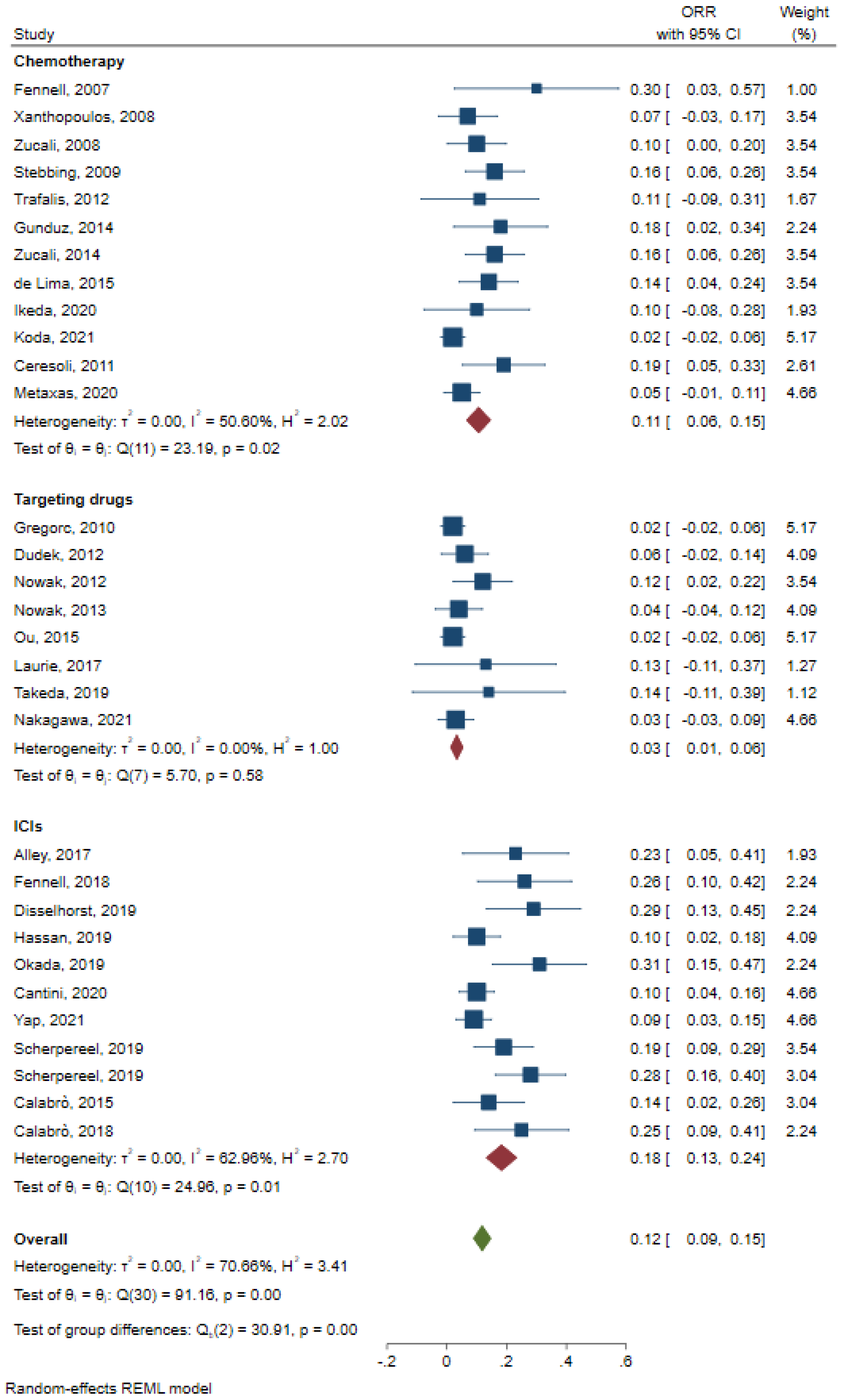
3.4. Primary Outcomes
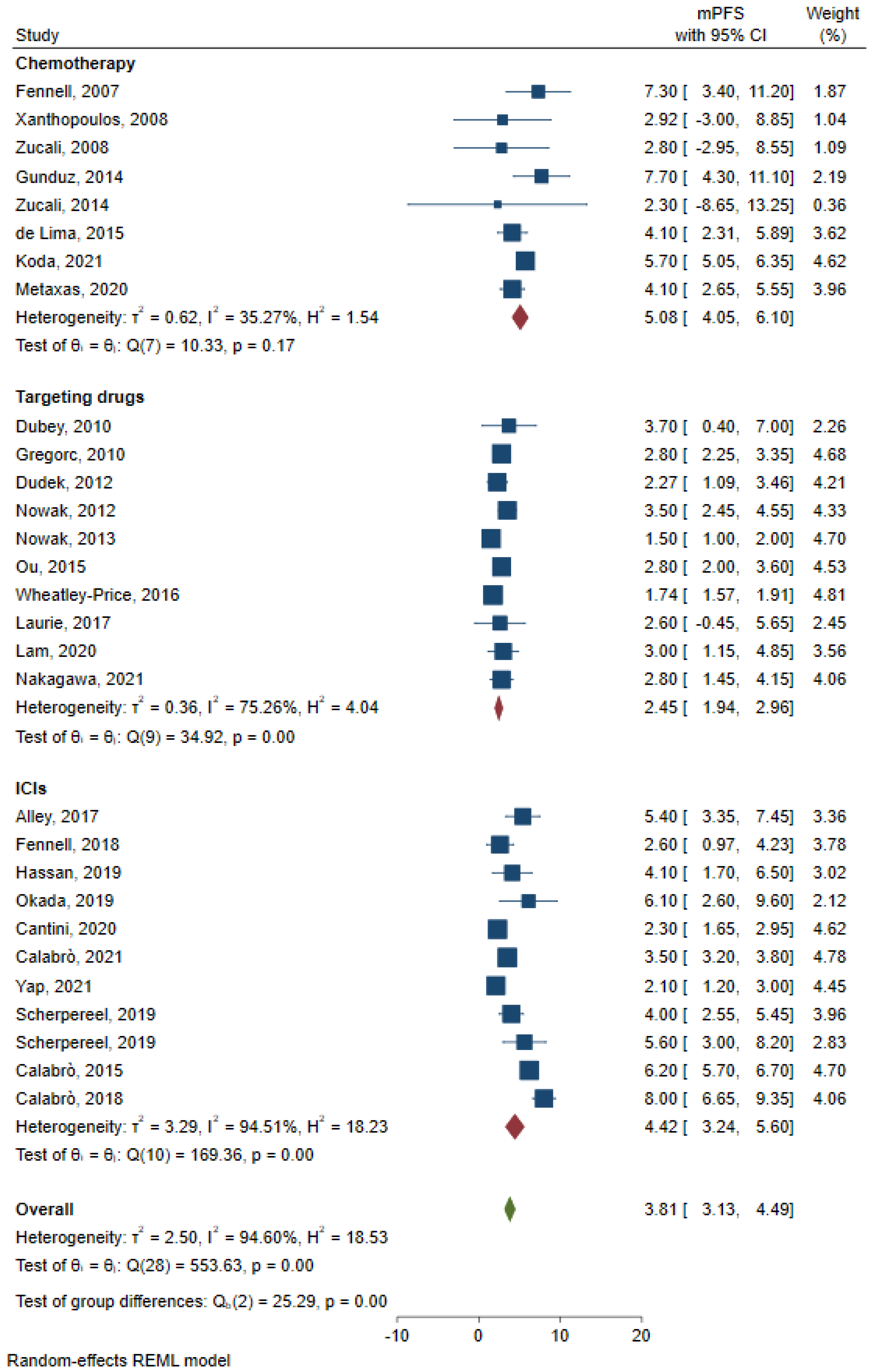
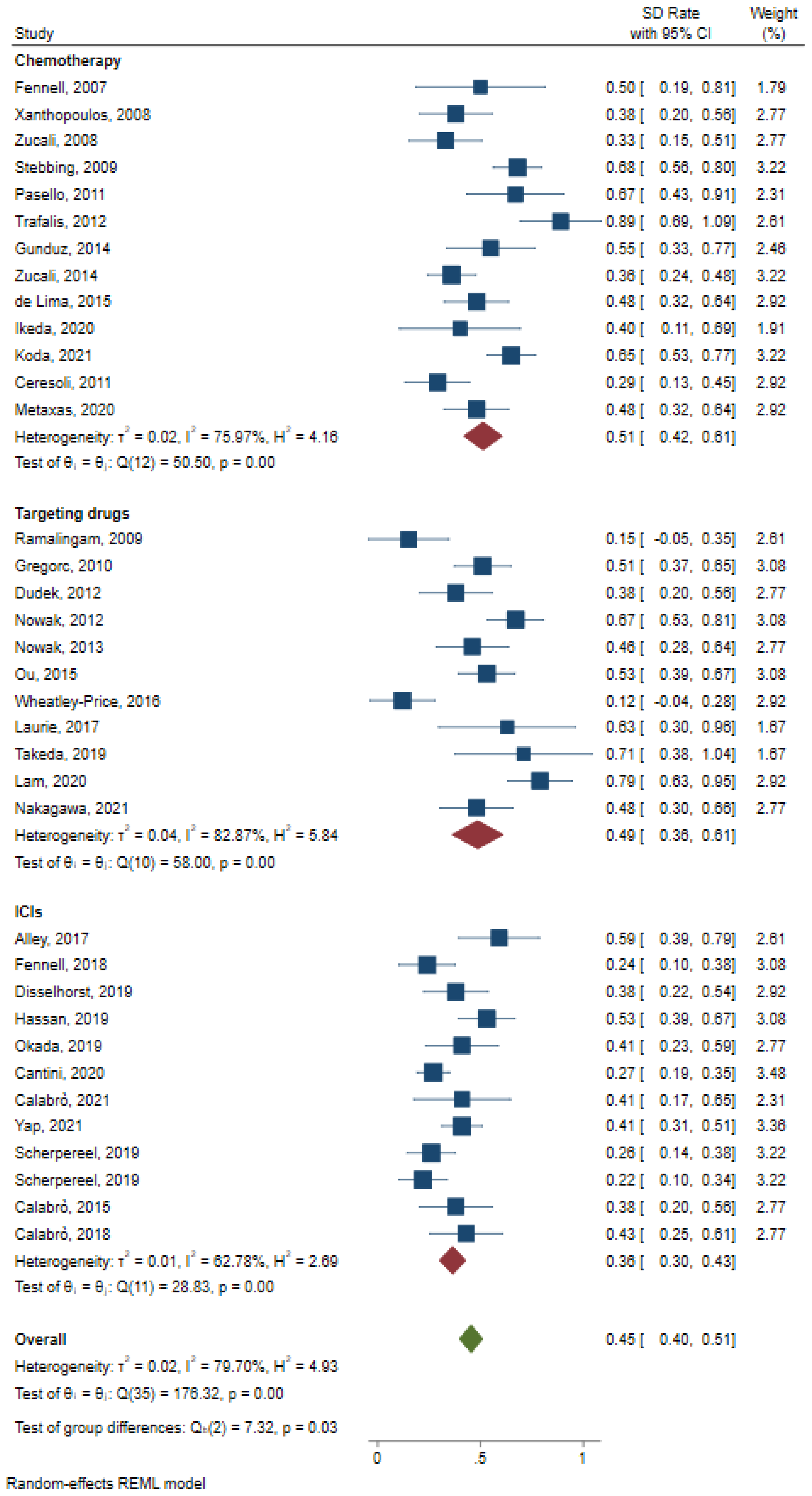
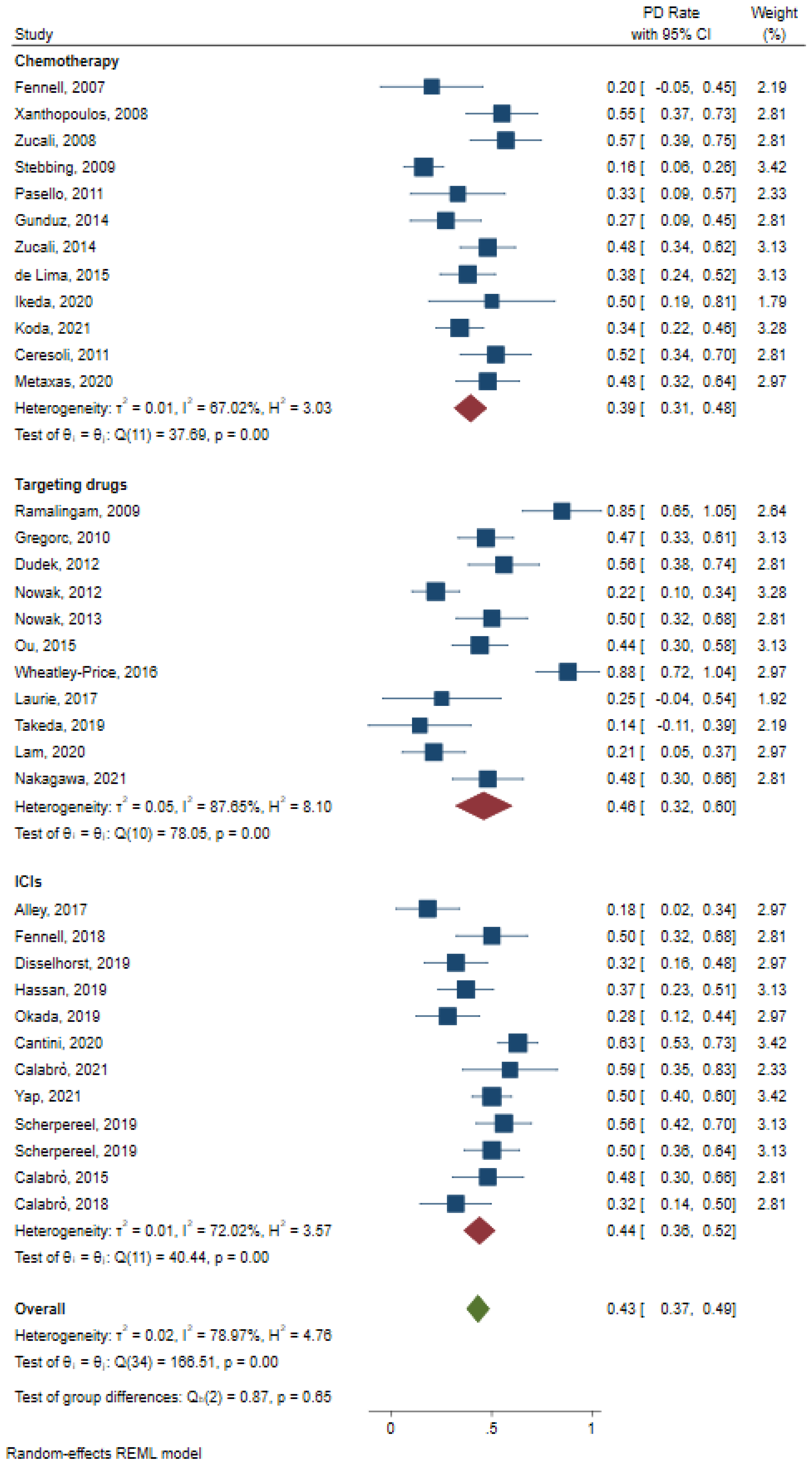
3.5. Secondary Outcomes
4. Discussion
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Brims, F. Epidemiology and Clinical Aspects of Malignant Pleural Mesothelioma. Cancers 2021, 13, 4194. [Google Scholar] [CrossRef]
- Janes, S.M.; Alrifai, D.; Fennell, D.A. Perspectives on the Treatment of Malignant Pleural Mesothelioma. N. Engl. J. Med. 2021, 385, 1207–1218. [Google Scholar] [CrossRef] [PubMed]
- Mazurek, J.M.; Syamlal, G.; Wood, J.M.; Hendricks, S.A.; Weston, A. Malignant Mesothelioma Mortality—United States, 1999–2015. MMWR Morb. Mortal. Wkly. Rep. 2017, 66, 214–218. [Google Scholar] [CrossRef]
- Sekido, Y. Molecular pathogenesis of malignant mesothelioma. Carcinogenesis 2013, 34, 1413–1419. [Google Scholar] [CrossRef] [PubMed]
- Vogelzang, N.J.; Rusthoven, J.J.; Symanowski, J.; Denham, C.; Kaukel, E.; Ruffie, P.; Gatzemeier, U.; Boyer, M.; Emri, S.; Manegold, C.; et al. Phase III study of pemetrexed in combination with cisplatin versus cisplatin alone in patients with malignant pleural mesothelioma. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2003, 21, 2636–2644. [Google Scholar] [CrossRef]
- Eberst, G.; Anota, A.; Scherpereel, A.; Mazieres, J.; Margery, J.; Greillier, L.; Audigier-Valette, C.; Moro-Sibilot, D.; Molinier, O.; Léna, H.; et al. Health-Related Quality of Life Impact from Adding Bevacizumab to Cisplatin-Pemetrexed in Malignant Pleural Mesothelioma in the MAPS IFCT-GFPC-0701 Phase III Trial. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2019, 25, 5759–5765. [Google Scholar] [CrossRef]
- Scherpereel, A.; Mazieres, J.; Greillier, L.; Lantuejoul, S.; Dô, P.; Bylicki, O.; Monnet, I.; Corre, R.; Audigier-Valette, C.; Locatelli-Sanchez, M.; et al. Nivolumab or nivolumab plus ipilimumab in patients with relapsed malignant pleural mesothelioma (IFCT-1501 MAPS2): A multicentre, open-label, randomised, non-comparative, phase 2 trial. Lancet Oncol. 2019, 20, 239–253. [Google Scholar] [CrossRef]
- Manegold, C.; Symanowski, J.; Gatzemeier, U.; Reck, M.; von Pawel, J.; Kortsik, C.; Nackaerts, K.; Lianes, P.; Vogelzang, N.J. Second-line (post-study) chemotherapy received by patients treated in the phase III trial of pemetrexed plus cisplatin versus cisplatin alone in malignant pleural mesothelioma. Ann. Oncol. 2005, 16, 923–927. [Google Scholar] [CrossRef] [PubMed]
- Fennell, D.A.; Steele, J.P.C.; Shamash, J.; Evans, M.T.; Wells, P.; Sheaff, M.T.; Rudd, R.M.; Stebbing, J. Efficacy and safety of first- or second-line irinotecan, cisplatin, and mitomycin in mesothelioma. Cancer 2007, 109, 93–99. [Google Scholar] [CrossRef]
- Xanthopoulos, A.; Bauer, T.T.; Blum, T.G.; Kollmeier, J.; Schönfeld, N.; Serke, M. Gemcitabine combined with oxaliplatin in pretreated patients with malignant pleural mesothelioma: An observational study. J. Occup. Med. Toxicol. 2008, 3, 34. [Google Scholar] [CrossRef] [Green Version]
- Zucali, P.A.; Ceresoli, G.L.; Garassino, I.; De Vincenzo, F.; Cavina, R.; Campagnoli, E.; Cappuzzo, F.; Salamina, S.; Soto Parra, H.J.; Santoro, A. Gemcitabine and vinorelbine in pemetrexed-pretreated patients with malignant pleural mesothelioma. Cancer 2008, 112, 1555–1561. [Google Scholar] [CrossRef]
- Ramalingam, S.S.; Belani, C.P.; Ruel, C.; Frankel, P.; Gitlitz, B.; Koczywas, M.; Espinoza-Delgado, I.; Gandara, D. Phase II study of belinostat (PXD101), a histone deacetylase inhibitor, for second line therapy of advanced malignant pleural mesothelioma. J. Thorac. Oncol. Off. Publ. Int. Assoc. Study Lung Cancer 2009, 4, 97–101. [Google Scholar] [CrossRef] [Green Version]
- Stebbing, J.; Powles, T.; McPherson, K.; Shamash, J.; Wells, P.; Sheaff, M.T.; Slater, S.; Rudd, R.M.; Fennell, D.; Steele, J.P.C. The efficacy and safety of weekly vinorelbine in relapsed malignant pleural mesothelioma. Lung Cancer 2009, 63, 94–97. [Google Scholar] [CrossRef] [PubMed]
- Dubey, S.; Jänne, P.A.; Krug, L.; Pang, H.; Wang, X.; Heinze, R.; Watt, C.; Crawford, J.; Kratzke, R.; Vokes, E.; et al. A phase II study of sorafenib in malignant mesothelioma: Results of Cancer and Leukemia Group B 30307. J. Thorac. Oncol. Off. Publ. Int. Assoc. Study Lung Cancer 2010, 5, 1655–1661. [Google Scholar] [CrossRef] [Green Version]
- Gregorc, V.; Zucali, P.A.; Santoro, A.; Ceresoli, G.L.; Citterio, G.; De Pas, T.M.; Zilembo, N.; De Vincenzo, F.; Simonelli, M.; Rossoni, G.; et al. Phase II study of asparagine-glycine-arginine-human tumor necrosis factor alpha, a selective vascular targeting agent, in previously treated patients with malignant pleural mesothelioma. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2010, 28, 2604–2611. [Google Scholar] [CrossRef]
- Ceresoli, G.L.; Zucali, P.A.; De Vincenzo, F.; Gianoncelli, L.; Simonelli, M.; Lorenzi, E.; Ripa, C.; Giordano, L.; Santoro, A. Retreatment with pemetrexed-based chemotherapy in patients with malignant pleural mesothelioma. Lung Cancer 2011, 72, 73–77. [Google Scholar] [CrossRef] [PubMed]
- Pasello, G.; Nicotra, S.; Marulli, G.; Rea, F.; Bonanno, L.; Carli, P.; Magro, C.; Jirillo, A.; Favaretto, A. Platinum-based doublet chemotherapy in pre-treated malignant pleural mesothelioma (MPM) patients: A mono-institutional experience. Lung Cancer 2011, 73, 351–355. [Google Scholar] [CrossRef] [PubMed]
- Dudek, A.Z.; Pang, H.; Kratzke, R.A.; Otterson, G.A.; Hodgson, L.; Vokes, E.E.; Kindler, H.L. Phase II study of dasatinib in patients with previously treated malignant mesothelioma (cancer and leukemia group B 30601): A brief report. J. Thorac. Oncol. Off. Publ. Int. Assoc. Study Lung Cancer 2012, 7, 755–759. [Google Scholar] [CrossRef] [Green Version]
- Nowak, A.K.; Millward, M.J.; Creaney, J.; Francis, R.J.; Dick, I.M.; Hasani, A.; Van Der Schaaf, A.; Segal, A.; Musk, A.W.; Byrne, M.J. A phase ii study of intermittent sunitinib malate as second-line therapy in progressive malignant pleural mesothelioma. J. Thorac. Oncol. 2012, 7, 1449–1456. [Google Scholar] [CrossRef] [Green Version]
- Trafalis, D.T.; Alifieris, C.; Krikelis, D.; Tzogkas, N.; Stathopoulos, G.P.; Athanassiou, A.E.; Sitaras, N.M. Topotecan and pegylated liposomal doxorubicin combination as palliative treatment in patients with pretreated advanced malignant pleural mesothelioma. Int. J. Clin. Pharmacol. Ther. 2012, 50, 490–499. [Google Scholar] [CrossRef] [PubMed]
- Nowak, A.K.; Brown, C.; Millward, M.J.; Creaney, J.; Byrne, M.J.; Hughes, B.; Kremmidiotis, G.; Bibby, D.C.; Leske, A.F.; Mitchell, P.L.R.; et al. A phase II clinical trial of the vascular disrupting agent BNC105P as second line chemotherapy for advanced malignant pleural mesothelioma. Lung Cancer 2013, 81, 422–427. [Google Scholar] [CrossRef] [PubMed]
- Gunduz, S.; Mutlu, H.; Goksu, S.S.; Arslan, D.; Tatli, A.M.; Uysal, M.; Coskun, H.S.; Bozcuk, H.; Ozdogan, M.; Savas, B. Oral cyclophosphamide and etoposide in treatment of malignant pleural mesothelioma. Asian Pac. J. Cancer Prev. APJCP 2014, 15, 8843–8846. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zucali, P.A.; Perrino, M.; Lorenzi, E.; Ceresoli, G.L.; De Vincenzo, F.; Simonelli, M.; Gianoncelli, L.; De Sanctis, R.; Giordano, L.; Santoro, A. Vinorelbine in pemetrexed-pretreated patients with malignant pleural mesothelioma. Lung Cancer 2014, 84, 265–270. [Google Scholar] [CrossRef] [PubMed]
- Calabrò, L.; Morra, A.; Fonsatti, E.; Cutaia, O.; Fazio, C.; Annesi, D.; Lenoci, M.; Amato, G.; Danielli, R.; Altomonte, M.; et al. Efficacy and safety of an intensified schedule of tremelimumab for chemotherapy-resistant malignant mesothelioma: An open-label, single-arm, phase 2 study. Lancet Respir. Med. 2015, 3, 301–309. [Google Scholar] [CrossRef]
- de Lima, V.A.B.; Sorensen, J.B. Third-line chemotherapy with carboplatin, gemcitabine and liposomised doxorubicin for malignant pleural mesothelioma. Med. Oncol. 2015, 32, 11. [Google Scholar] [CrossRef] [PubMed]
- Krug, L.M.; Kindler, H.L.; Calvert, H.; Manegold, C.; Tsao, A.S.; Fennell, D.; Öhman, R.; Plummer, R.; Eberhardt, W.E.; Fukuoka, K.; et al. Vorinostat in patients with advanced malignant pleural mesothelioma who have progressed on previous chemotherapy (VANTAGE-014): A phase 3, double-blind, randomised, placebo-controlled trial. Lancet Oncol. 2015, 16, 447–456. [Google Scholar] [CrossRef] [PubMed]
- Ou, S.H.; Moon, J.; Garland, L.L.; Mack, P.C.; Testa, J.R.; Tsao, A.S.; Wozniak, A.J.; Gandara, D.R. SWOG S0722: Phase II study of mTOR inhibitor everolimus (RAD001) in advanced malignant pleural mesothelioma (MPM). J. Thorac. Oncol. Off. Publ. Int. Assoc. Study Lung Cancer 2015, 10, 387–391. [Google Scholar] [CrossRef] [Green Version]
- Wheatley-Price, P.; Chu, Q.; Bonomi, M.; Seely, J.; Gupta, A.; Goss, G.; Hilton, J.; Feld, R.; Lee, C.W.; Goffin, J.R.; et al. A Phase II Study of PF-03446962 in Patients with Advanced Malignant Pleural Mesothelioma. CCTG Trial IND.207. J. Thorac. Oncol. Off. Publ. Int. Assoc. Study Lung Cancer 2016, 11, 2018–2021. [Google Scholar] [CrossRef] [Green Version]
- Alley, E.W.; Lopez, J.; Santoro, A.; Morosky, A.; Saraf, S.; Piperdi, B.; van Brummelen, E. Clinical safety and activity of pembrolizumab in patients with malignant pleural mesothelioma (KEYNOTE-028): Preliminary results from a non-randomised, open-label, phase 1b trial. Lancet Oncol. 2017, 18, 623–630. [Google Scholar] [CrossRef]
- Laurie, S.A.; Hao, D.; Leighl, N.B.; Goffin, J.; Khomani, A.; Gupta, A.; Addison, C.L.; Bane, A.; Seely, J.; Filion, M.L.; et al. A phase II trial of dovitinib in previously-treated advanced pleural mesothelioma: The Ontario Clinical Oncology Group. Lung Cancer 2017, 104, 65–69. [Google Scholar] [CrossRef]
- Maio, M.; Scherpereel, A.; Calabrò, L.; Aerts, J.; Perez, S.C.; Bearz, A.; Nackaerts, K.; Fennell, D.A.; Kowalski, D.; Tsao, A.S.; et al. Tremelimumab as second-line or third-line treatment in relapsed malignant mesothelioma (DETERMINE): A multicentre, international, randomised, double-blind, placebo-controlled phase 2b trial. Lancet Oncol. 2017, 18, 1261–1273. [Google Scholar] [CrossRef] [PubMed]
- Calabrò, L.; Morra, A.; Giannarelli, D.; Amato, G.; D’Incecco, A.; Covre, A.; Lewis, A.; Rebelatto, M.C.; Danielli, R.; Altomonte, M.; et al. Tremelimumab combined with durvalumab in patients with mesothelioma (NIBIT-MESO-1): An open-label, non-randomised, phase 2 study. Lancet Respir. Med. 2018, 6, 451–460. [Google Scholar] [CrossRef]
- Fennell, D.A. Programmed Death 1 Blockade With Nivolumab in Patients With Recurrent Malignant Pleural Mesothelioma. J. Thorac. Oncol. Off. Publ. Int. Assoc. Study Lung Cancer 2018, 13, 1436–1437. [Google Scholar] [CrossRef] [Green Version]
- Disselhorst, M.J.; Quispel-Janssen, J.; Lalezari, F.; Monkhorst, K.; de Vries, J.F.; van der Noort, V.; Harms, E.; Burgers, S.; Baas, P. Ipilimumab and nivolumab in the treatment of recurrent malignant pleural mesothelioma (INITIATE): Results of a prospective, single-arm, phase 2 trial. Lancet Respir. Med. 2019, 7, 260–270. [Google Scholar] [CrossRef]
- Hassan, R.; Thomas, A.; Nemunaitis, J.J.; Patel, M.R.; Bennouna, J.; Chen, F.L.; Delord, J.P.; Dowlati, A.; Kochuparambil, S.T.; Taylor, M.H.; et al. Efficacy and Safety of Avelumab Treatment in Patients With Advanced Unresectable Mesothelioma: Phase 1b Results From the JAVELIN Solid Tumor Trial. JAMA Oncol. 2019, 5, 351–357. [Google Scholar] [CrossRef]
- Okada, M.; Kijima, T.; Aoe, K.; Kato, T.; Fujimoto, N.; Nakagawa, K.; Takeda, Y.; Hida, T.; Kanai, K.; Imamura, F.; et al. Clinical efficacy and safety of nivolumab: Results of a multicenter, open-label, single-arm, Japanese phase II study in malignant pleural mesothelioma (MERIT). Clin. Cancer Res. 2019, 25, 5485–5492. [Google Scholar] [CrossRef] [Green Version]
- Takeda, M.; Ohe, Y.; Horinouchi, H.; Hida, T.; Shimizu, J.; Seto, T.; Nosaki, K.; Kishimoto, T.; Miyashita, I.; Yamada, M.; et al. Phase I study of YS110, a recombinant humanized monoclonal antibody to CD26, in Japanese patients with advanced malignant pleural mesothelioma. Lung Cancer 2019, 137, 64–70. [Google Scholar] [CrossRef] [PubMed]
- Cantini, L.; Belderbos, R.A.; Gooijer, C.J.; Dumoulin, D.W.; Cornelissen, R.; Baart, S.; Burgers, J.A.; Baas, P.; Aerts, J. Nivolumab in pre-treated malignant pleural mesothelioma: Real-world data from the Dutch expanded access program. Transl. Lung Cancer Res. 2020, 9, 1169–1179. [Google Scholar] [CrossRef] [PubMed]
- Ikeda, T.; Takemoto, S.; Senju, H.; Gyotoku, H.; Taniguchi, H.; Shimada, M.; Dotsu, Y.; Umeyama, Y.; Tomono, H.; Kitazaki, T.; et al. Amrubicin in previously treated patients with malignant pleural mesothelioma: A phase II study. Thorac. Cancer 2020, 11, 1972–1978. [Google Scholar] [CrossRef] [PubMed]
- Lam, W.S.; Creaney, J.; Chen, F.K.; Chin, W.L.; Muruganandan, S.; Arunachalam, S.; Attia, M.S.; Read, C.; Murray, K.; Millward, M.; et al. A phase II trial of single oral FGF inhibitor, AZD4547, as second or third line therapy in malignant pleural mesothelioma. Lung Cancer 2020, 140, 87–92. [Google Scholar] [CrossRef] [PubMed]
- Metaxas, Y.; Früh, M.; Eboulet, E.I.; Grosso, F.; Pless, M.; Zucali, P.A.; Ceresoli, G.L.; Mark, M.; Schneider, M.; Maconi, A.; et al. Lurbinectedin as second- or third-line palliative therapy in malignant pleural mesothelioma: An international, multi-centre, single-arm, phase II trial (SAKK 17/16). Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2020, 31, 495–500. [Google Scholar] [CrossRef]
- Popat, S.; Curioni-Fontecedro, A.; Dafni, U.; Shah, R.; O’Brien, M.; Pope, A.; Fisher, P.; Spicer, J.; Roy, A.; Gilligan, D.; et al. A multicentre randomised phase III trial comparing pembrolizumab versus single-agent chemotherapy for advanced pre-treated malignant pleural mesothelioma: The European Thoracic Oncology Platform (ETOP 9-15) PROMISE-meso trial. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2020, 31, 1734–1745. [Google Scholar] [CrossRef]
- Calabrò, L.; Rossi, G.; Morra, A.; Rosati, C.; Cutaia, O.; Daffinà, M.G.; Altomonte, M.; Di Giacomo, A.M.; Casula, M.; Fazio, C.; et al. Tremelimumab plus durvalumab retreatment and 4-year outcomes in patients with mesothelioma: A follow-up of the open label, non-randomised, phase 2 NIBIT-MESO-1 study. Lancet Respir. Med. 2021, 9, 969–976. [Google Scholar] [CrossRef]
- Fennell, D.A.; Ewings, S.; Ottensmeier, C.; Califano, R.; Hanna, G.G.; Hill, K.; Danson, S.; Steele, N.; Nye, M.; Johnson, L.; et al. Nivolumab versus placebo in patients with relapsed malignant mesothelioma (CONFIRM): A multicentre, double-blind, randomised, phase 3 trial. Lancet Oncol. 2021, 22, 1530–1540. [Google Scholar] [CrossRef] [PubMed]
- Kim, R.Y.; Li, Y.; Marmarelis, M.E.; Vachani, A. Comparative effectiveness of second-line immune checkpoint inhibitor therapy versus chemotherapy for malignant pleural mesothelioma. Lung Cancer 2021, 159, 107–110. [Google Scholar] [CrossRef] [PubMed]
- Koda, Y.; Kuribayashi, K.; Doi, H.; Kitajima, K.; Nakajima, Y.; Ishigaki, H.; Nakamura, A.; Minami, T.; Takahashi, R.; Yokoi, T.; et al. Irinotecan and Gemcitabine as Second-Line Treatment in Patients with Malignant Pleural Mesothelioma following Platinum plus Pemetrexed Chemotherapy: A Retrospective Study. Oncology 2021, 99, 161–168. [Google Scholar] [CrossRef]
- Nakagawa, K.; Kijima, T.; Okada, M.; Morise, M.; Kato, M.; Hirano, K.; Fujimoto, N.; Takenoyama, M.; Yokouchi, H.; Ohe, Y.; et al. Phase 2 Study of YS110, a Recombinant Humanized Anti-CD26 Monoclonal Antibody, in Japanese Patients With Advanced Malignant Pleural Mesothelioma. JTO Clin. Res. Rep. 2021, 2, 100178. [Google Scholar] [CrossRef]
- Pinto, C.; Zucali, P.A.; Pagano, M.; Grosso, F.; Pasello, G.; Garassino, M.C.; Tiseo, M.; Soto Parra, H.; Grossi, F.; Cappuzzo, F.; et al. Gemcitabine with or without ramucirumab as second-line treatment for malignant pleural mesothelioma (RAMES): A randomised, double-blind, placebo-controlled, phase 2 trial. Lancet Oncol. 2021, 22, 1438–1447. [Google Scholar] [CrossRef] [PubMed]
- Yap, T.A.; Nakagawa, K.; Fujimoto, N.; Kuribayashi, K.; Guren, T.K.; Calabrò, L.; Shapira-Frommer, R.; Gao, B.; Kao, S.; Matos, I.; et al. Efficacy and safety of pembrolizumab in patients with advanced mesothelioma in the open-label, single-arm, phase 2 KEYNOTE-158 study. Lancet Respir. Med. 2021, 9, 613–621. [Google Scholar] [CrossRef]
- Aprile, V.; Lenzini, A.; Lococo, F.; Bacchin, D.; Korasidis, S.; Mastromarino, M.G.; Guglielmi, G.; Palmiero, G.; Ambrogi, M.C.; Lucchi, M. Hyperthermic Intrathoracic Chemotherapy for Malignant Pleural Mesothelioma: The Forefront of Surgery-Based Multimodality Treatment. J. Clin. Med. 2021, 10, 3801. [Google Scholar] [CrossRef] [PubMed]
- Bueno, R.; Stawiski, E.W.; Goldstein, L.D.; Durinck, S.; De Rienzo, A.; Modrusan, Z.; Gnad, F.; Nguyen, T.T.; Jaiswal, B.S.; Chirieac, L.R.; et al. Comprehensive genomic analysis of malignant pleural mesothelioma identifies recurrent mutations, gene fusions and splicing alterations. Nat. Genet. 2016, 48, 407–416. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Year | Author | Design | Sample Size | First-Line Treatment | Current Treatment | Median Follow-Up, m | Score |
|---|---|---|---|---|---|---|---|
| 2005 | Manegold [8] | Single-arm | 189 | Pem/Cis 84 Cis 105 | PSC | - | 14 * |
| 2007 | Fennell [9] | Single-arm | 13 | Vinorelbine Vinorelbine/Oxaliplatin Pem/Cis | Irinotecan/Cis/Mitomycin | - | 16 * |
| 2008 | Xanthopoulos [10] | Single-arm | 29 | Pem/Platinum | Oxaliplatin/Gem 25 Oxaliplatin 4 | 6.075 | 14 * |
| 2008 | Zucali [11] | Single-arm | 30 | Pem Pem/Platinum | Gem/Vinorelbine | 10.8 | 14 * |
| 2009 | Ramalingam [12] | Single-arm | 13 | Pem Pem/Platinum | Belinostat | - | 15 * |
| 2009 | Stebbing [13] | Single-arm | 63 | - | Vinorelbine | - | 16 * |
| 2010 | Dubey [14] | Single-arm | 30 | - | Sorafenib | - | 16 * |
| 2010 | Gregorc [15] | Single-arm | 57 | Pem/Platinum Gem/Cis | NGR-hTNF | 17.9 | 15 * |
| 2011 | Pasello [17] | Single-arm | 17 | Pem/Platinum | Gem Gem/Cis | - | 14 * |
| 2011 | Ceresoli, G. L. [16] | Single-arm | 31 | Pem-Based CT | Pem-Based CT | - | 14 * |
| 2012 | Dudek [18] | Single-arm | 43 | Pem-Based CT | Dasatinib | 21 | 15 * |
| 2012 | Nowak [19] | Single-arm | 53 | Pem 42 Gem 11 | Sunitinib | - | 16 * |
| 2012 | Trafalis [20] | Single-arm | 9 | Pem/Cis | Topotecan/PLD | - | 13 * |
| 2013 | Nowak [21] | Single-arm | 30 | Pem/Platinum | BNC105P | 10.4 | 16 * |
| 2014 | Gunduz [22] | Single-arm | 22 | Pem/Platinum | CTX/Etoposide | 39.1 | 14 * |
| 2014 | Zucali [23] | Single-arm | 59 | Pem-Based CT | Vinorelbine | 18.1 | 14 * |
| 2015 | de Lima [25] | Single-arm | 43 | Pem/Platinum 42 Pem/Vinorelbine 1 | CCG | - | 14 * |
| 2015 | Krug [26] | RCT | 329 vs. 332 | - | Vorinostat vs. Placebo | 6.5 vs. 5.77 | 5 ** |
| 2015 | Ou [27] | Single-arm | 59 | - | Everolimus | - | 16 * |
| 2015 | Calabrò [24] | Single-arm | 29 | Platinum-Based CT | Tremelimumab | 21.3 | 16 * |
| 2016 | Wheatley-Price [28] | Single-arm | 17 | - | PF-03446962 | - | 12 * |
| 2017 | Alley [29] | Single-arm | 25 | Platinum/Pem/Gem/Vinorelbine | Pembrolizumab | 18.7 | 16 * |
| 2017 | Laurie [30] | Single-arm | 12 | Platinum-Based CT | Dovitinib | - | 16 * |
| 2017 | Maio [31] | RCT | 382 vs. 189 | - | Tremelimumab vs. Placebo | - | 5 ** |
| 2018 | Fennell [33] | Single-arm | 34 | - | Nivolumab | 27.5 | 16 * |
| 2018 | Calabrò, L. [32] | Single-arm | 28 | Platinum-Based CT | Tremelimumab/Durvalumab | 19·2 | 16 * |
| 2019 | Disselhorst [34] | Single-arm | 35 | Platinum-Based CT | Ipilimumab/Nivolumab | 14.3 | 15 * |
| 2019 | Hassan [35] | Single-arm | 53 | - | Avelumab | 24.8 | 16 * |
| 2019 | Okada [36] | Single-arm | 34 | - | Nivolumab | 16.8 | 16 * |
| 2019 | Takeda [37] | Single-arm | 9 | - | YS110 | - | 13 * |
| 2019 | Scherpereel [7] | Single-arm | 125 | Platinum-Based CT | Nivolumab Nivolumab/Ipilimumab | 20.1 | 15 * |
| 2020 | Cantini [38] | Single-arm | 107 | - | Nivolumab | 10.1 | 14 * |
| 2020 | Ikeda [39] | Single-arm | 10 | Pem/Platinum | Amrubicin | - | 15 * |
| 2020 | Lam [40] | Single-arm | 24 | Platinum-Based CT | AZD4547 | - | 16 * |
| 2020 | Popat [42] | RCT | 73 vs. 71 | Platinum-Based CT | Pembrolizumab vs. Gem/Vinorelbine | - | 5 ** |
| 2020 | Metaxas, Y. [41] | Single-arm | 42 | Pem/Platinum CT ± Immunotherapy | Lurbinectedin | 15.8 | 16 * |
| 2021 | Calabrò [43] | Single-arm | 17 | Pem/Platinum13 ICIs 4 | Tremelimumab/Durvalumab | 24 | 14 * |
| 2021 | Kim [45] | Cohort study | 115 vs. 61 | Platinum-Based CT | Pembrolizumab/Nivolumab/Ipilimumab vs. Gem/Vinorelbine | - | 9 *** |
| 2021 | Koda [46] | Single-arm | 62 | Pem/Platinum Pem | Irinotecan/Gem | 5.7 | 14 * |
| 2021 | Nakagawa [47] | Single-arm | 31 | Platinum-Based CT | YS110 | 9.7 | 16 * |
| 2021 | Pinto [48] | RCT | 80 vs. 81 | Pem/Platinum | Ramucirumab/Gem vs. Placebo/Gem | 21.9 | 16 * |
| 2021 | Yap [49] | Single-arm | 118 | CT | Pembrolizumab | 38.5 | 16 * |
| 2021 | Fennell, D. A. [44] | RCT | 221 vs. 111 | Platinum-Based CT | Nivolumab vs. Placebo | 11.6 | 5 ** |
| Year | Author | Design | Sample Size | Age (Median) | Sex | Asbestos Exposure | Histology | Stage | PS | PD-L1 |
|---|---|---|---|---|---|---|---|---|---|---|
| 2005 | Manegold [8] | Single-arm | 189 | 59.3 | Male 152 Female 37 | / | Epithelioid 138 Sarcomatoid 16 Biphasic 29 Other 6 | I–III 41 IV 146 | KPS ≥ 90: 123 KPS < 90: 66 | / |
| 2007 | Fennell [9] | Single-arm | 13 | 56 | Male 11 Female 2 | / | Epithelioid 10 Sarcomatoid 2 Biphasic 1 | I–III 3 IV 10 | ECOG 0: 2 ECOG 1: 4 ECOG 2: 7 | / |
| 2008 | Xanthopoulos [10] | Single-arm | 29 | 64.6 | Male 27 Female 2 | Yes 17 No 1 Unknown 11 | Epithelioid 27 Sarcomatoid 1 Biphasic 1 | / | ECOG 0: 5 ECOG 1: 18 ECOG 2: 3 ECOG 3: 3 | / |
| 2008 | Zucali [11] | Single-arm | 30 | 66 | Male 22 Female 8 | / | Epithelioid 21 Sarcomatoid 2 Biphasic 5 Other 2 | / | ECOG 0: 9 ECOG 1: 16 ECOG 2: 5 | / |
| 2009 | Ramalingam [12] | Single-arm | 13 | 73 | Male 8 Female 5 | / | Epithelioid 7 Sarcomatoid 1 Other 5 | / | ECOG 0: 4 ECOG 1: 8 ECOG 2: 1 | / |
| 2009 | Stebbing [13] | Single-arm | 63 | 59 | Male 59 Female 4 | / | Epithelioid 39 Sarcomatoid 7 Biphasic 17 | I–III 43 IV 20 | ECOG 0: 23 ECOG 1: 26 ECOG 2: 14 | / |
| 2010 | Dubey [14] | Single-arm | 50 | 69 | Male 35 Female 15 | / | Epithelioid 37 Sarcomatoid 4 Biphasic 7 Unknown 2 | / | ECOG 0: 11 ECOG 1: 39 | / |
| 2010 | Gregorc [15] | Cohort study | 57 | / | Male 35 Female 22 | / | Epithelioid 45 Non-epithelioid 12 | ECOG 0–1: 48 ECOG 2: 9 | / | |
| 2011 | Pasello [17] | Single-arm | 17 | 61 | Male 12 Female 5 | / | Epithelioid 12 Sarcomatoid 4 Biphasic 1 | / | ECOG 0: 0 ECOG 1: 15 ECOG 2: 2 | / |
| 2011 | Ceresoli, G. L. [16] | Single-arm | 31 | 65 | Male 21 Female 10 | / | Epithelioid 27 Biphasic 4 | / | ECOG 0: 12 ECOG 1: 18 Unknown: 1 | / |
| 2012 | Dudek [18] | Single-arm | 43 | 68 | Male 31 Female 12 | / | Epithelioid 33 Sarcomatoid 5 Biphasic 2 Missing 3 | / | ECOG 0: 19 ECOG 1: 24 ECOG 2: 0 | / |
| 2012 | Nowak [19] | Single-arm | 53 | 66 | Male 44 Female 9 | / | Epithelioid 39 Sarcomatoid1 Biphasic 10 Unknown 3 | / | ECOG 0: 14 ECOG 1: 39 ECOG 2: 0 | / |
| 2012 | Trafalis [20] | Single-arm | 9 | 57.5 | Male 7 Female 2 | / | Epithelioid 7 Sarcomatoid 1 Biphasic 1 | I–III: 0 IV: 9 | / | / |
| 2013 | Nowak [21] | Single-arm | 30 | 64 | Male 27 Female 3 | / | Epithelioid 20 Sarcomatoid 2 Biphasic 3 Other 5 | / | ECOG 0: 7 ECOG 1: 23 ECOG 2: 0 | / |
| 2014 | Gunduz [22] | Single-arm | 22 | 55 | Male 13 Female 9 | / | Epithelioid 12 Sarcomatoid 4 Biphasic 1 | I–III: 15 IV: 7 | / | / |
| 2014 | Zucali [23] | Single-arm | 59 | 69 | Male 38 Female 21 | / | Epithelioid 53 Non-Epithelioid 6 | / | ECOG 0: 28 ECOG > 1: 30 Unknown: 1 | / |
| 2015 | de Lima [25] | Single-arm | 43 | 67 | Male 31 Female 12 | Yes 34 No 6 Unknown 3 | Epithelioid 25 Sarcomatoid 2 Biphasic 13 Other 3 | I–II: 8 III: 8 IV: 27 | ECOG 0: 2 ECOG 1: 37 ECOG 2: 4 | / |
| 2015 | Krug [26] | RCT | Vorinostat: 329 Placebo: 332 | Vorinostat: 64 Placebo: 65 | Vorinostat: Male 283 Female 46 Placebo: Male 270 Female 62 | / | Vorinostat: Epithelioid 274 Non-Epithelioid 55 Placebo: Epithelioid 269 Non-Epithelioid 63 | Vorinostat: I–II: 32 III–IV: 297 Placebo: I–II: 29 III–IV: 303 | Vorinostat: KPS > 80: 163 Placebo: KPS > 80: 162 | / |
| 2015 | Ou [27] | Single-arm | 59 | 67 | Male 45 Female 14 | / | Epithelioid 36 Sarcomatoid 0 Biphasic 4 Other: 17 Missing: 2 | I–III: 5 IV: 54 | ECOG 0: 13 ECOG 1: 46 ECOG 2: 0 | / |
| 2015 | Calabrò [24] | Single-arm | 29 | 65 | Male 20 Female 9 | / | Epithelioid 21 Sarcomatoid 1 Biphasic 6 Other 1 | I–III: 11 IV: 8 | ECOG 0: 4 ECOG 1: 19 ECOG 2: 6 | / |
| 2016 | Wheatley-Price [28] | Single-arm | 17 | 68 | Male 12 Female 5 | / | Epithelioid 12 Non-Epithelioid 5 | / | ECOG 0: 5 ECOG 1: 10 ECOG 2: 2 | / |
| 2017 | Alley [29] | Single-arm | 25 | 65 | Male 17 Female 8 | / | Epithelioid 18 Sarcomatoid 2 Biphasic 2 Unknown 3 | / | ECOG 0: 9 ECOG 1: 16 ECOG 2: 0 | / |
| 2017 | Laurie [30] | Single-arm | 12 | 67 | Male 10 Female 2 | / | Epithelioid 12 Sarcomatoid 4 Biphasic 1 | / | ECOG 0: 4 ECOG 1: 8 | / |
| 2017 | Maio [31] | RCT | Tremelimumab: 382 Placebo: 189 | Tremelimumab: 66 Placebo: 67 | Tremelimumab: Male 283 Female 99 Placebo: Male 151 Female 38 | / | Tremelimumab: Epithelioid 318 Sarcomatoid 22 Biphasic 40 Missing 2 Placebo: Epithelioid 157 Sarcomatoid 16 Biphasic 16 | Tremelimumab: I: 1 II: 14 III: 95 IV: 263 Unknown: 9 Placebo: I: 4 II: 7 III: 39 IV: 133 Unknown: 6 | Tremelimumab: ECOG 0: 106 ECOG 1: 273 Missing: 3 Placebo: ECOG 0: 57 ECOG 1: 132 Missing: 0 | / |
| 2018 | Fennell [33] | Single-arm | 34 | 67 | Male 28 Female 6 | / | Epithelioid 28 Sarcomatoid 2 Biphasic 4 | I–III: 24 IV: 10 | ECOG 0: 18 ECOG 1: 16 | / |
| 2018 | Calabrò, L. [32] | Single-arm | 40 | 64 | Male 29 Female 11 | / | Epithelioid 32 Sarcomatoid 2 Biphasic 5 Undefined 1 | III: 11 IV: 29 | EORTC Good: 30 Poor: 10 | <1% 18 ≥1% 20 Not Scored 2 |
| 2019 | Disselhorst [34] | Single-arm | 35 | 65 | Male 27 Female 8 | / | Epithelioid 30 Sarcomatoid 3 Biphasic 2 | I–III: 21 IV: 14 | ECOG 0: 10 ECOG 1: 25 | <1% 19 ≥1% 15 Not Scored 1 |
| 2019 | Hassan [35] | Single-arm | 53 | 67 | Male 32 Female 21 | / | Epithelioid 43 Sarcomatoid 2 Biphasic 6 Unknown 2 | / | ECOG 0: 14 ECOG 1: 39 | <1% 21 ≥1% 22 Not Scored 10 |
| 2019 | Okada [36] | Single-arm | 34 | 68 | Male 29 Female 5 | / | Epithelioid 27 Sarcomatoid 3 Biphasic 4 | / | ECOG 0: 13 ECOG 1: 21 | <1% 20 ≥1% 12 Not Scored 2 |
| 2019 | Takeda [37] | Single-arm | 9 | 62.2 | Male 7 Female 2 | / | Epithelioid 7 Sarcomatoid 0 Biphasic 2 | I–III: 2 IV: 7 | ECOG 0: 5 ECOG 1: 4 | / |
| 2019 | Scherpereel [7] | Single-arm | 125 | Nivolumab: 63 Nivolumab + Ipilimumab: 62 | Nivolumab: Male 16 Female 47 Nivolumab + Ipilimumab: Male 9 Female 53 | / | Nivolumab: Epithelioid 52 Non-Epithelioid 11 Nivolumab + Ipilimumab: Epithelioid 53 Non-Epithelioid 9 | Nivolumab: I–II: 7 III–IV: 56 Nivolumab + Ipilimumab: I–II: 11 III–IV: 51 | Nivolumab: ECOG 0: 19 ECOG 1: 42 ECOG 2: 0 Nivolumab + Ipilimumab: ECOG 0: 25 ECOG 1: 36 ECOG 2: 1 | Nivolumab: Negative 31 ≥1% 19 ≥25% 2 ≥50% 0 Not Available 13 Nivolumab + Ipilimumab: Negative 27 ≥1% 22 ≥25% 5 ≥50% 3 Not Available 13 |
| 2020 | Cantini [38] | Single-arm | 107 | 69 | Male 95 Female 12 | / | Epithelioid 78 Non-Epithelioid 29 | I–II: 32 III–IV: 70 Unknown: 5 | ECOG 0: 20 ECOG 1: 68 ECOG 2: 6 Unknown: 13 | Negative 22 Positive 11 Unknown 74 |
| 2020 | Ikeda [39] | Single-arm | 10 | 67 | Male 9 Female 1 | / | Epithelioid 4 Sarcomatoid 3 Biphasic 3 | I: 0 II: 1 III: 4 IV: 4 Recur: 1 | ECOG 0: 0 ECOG 1: 10 | / |
| 2020 | Lam [40] | Single-arm | 24 | 69.5 | Male 21 Female 3 | / | Epithelioid 20 Sarcomatoid 2 Biphasic 2 | / | ECOG 0: 0 ECOG 1: 24 | / |
| 2020 | Popat [42] | RCT | Pembrolizumab: 73 CT: 71 | Pembrolizumab: 69 CT: 71 | Pembrolizumab: Male 58 Female 15 CT: Male 60 Female 11 | / | Pembrolizumab: Epithelioid 66 Non-Epithelioid 7 CT: Epithelioid 62 Non-Epithelioid 9 | / | Pembrolizumab: ECOG 0: 21 ECOG 1: 51 ECOG 2: 1 CT: ECOG 0: 14 ECOG 1: 57 ECOG 2: 0 | Pembrolizumab: <1% 36 1–20% 20 ≥20% 11 Not Evaluable 2 CT: <1% 30 1–20% 18 ≥20% 14 Not Evaluable 4 |
| 2020 | Metaxas, Y. [41] | Single-arm | 42 | 68 | Male 35 Female 7 | / | Epithelioid 33 Sarcomatoid 5 Biphasic 4 | / | ECOG 0: 20 ECOG 1: 22 | / |
| 2021 | Calabrò [43] | Single-arm | 17 | 65 | Male 11 Female 6 | / | Epithelioid 14 Sarcomatoid 0 Biphasic 3 | / | ECOG 0: 10 ECOG 1: 7 | / |
| 2021 | Kim [45] | Cohort study | Chemo 61 ICI 115 | CT: 47–69: 22 70–75: 16 76–79: 12 80–85: 11 ICIs: 47–69: 30 70–75: 29 76–79: 23 80–85: 33 | CT: Male 48 Female 13 ICIs: Male 83 Female 32 | / | CT: Epithelioid 12 Non-Epithelioid 20 ICIs: Epithelioid 77 Non-Epithelioid 38 | / | CT: ECOG 0–1: 38 ECOG 2–4: 11 Missing: 12 ICIs: ECOG 0–1: 84 ECOG 2–4: 11 Missing: 20 | / |
| 2021 | Koda [46] | Single-arm | 62 | 65 | Male 47 Female 15 | Yes 47 No 15 | Epithelioid 48 Sarcomatoid 6 Biphasic 6 Desmoplastic 2 | I: 13 II: 10 III: 18 IV: 21 | ECOG 0: 17 ECOG 1: 43 ECOG 2: 2 | / |
| 2021 | Nakagawa [47] | Single-arm | 31 | 68 | Male 28 Female 3 | / | Epithelioid 26 Sarcomatoid 2 Biphasic 3 | II: 3 III: 8 IV: 20 | ECOG 0: 12 ECOG 1: 19 | CD26 expression <20% 3 ≥20% 28 |
| 2021 | Pinto [48] | RCT | Gem + Ramucirumab: 80 Gem + Placebo: 81 | Gem + Ramucirumab: 69 Gem + Placebo: 69 | Gem + Ramucirumab: Male 59 Female 21 Gem + Placebo: Male 60 Female 21 | / | Gem + Ramucirumab: Epithelioid 68 Non-Epithelioid 12 Gem + Placebo: Epithelioid 70 Non-Epithelioid 11 | / | Gem + Ramucirumab: ECOG 0: 50 ECOG 1: 29 ECOG 2: 1 Gem + Placebo: ECOG 0: 46 ECOG 1: 34 ECOG 2: 1 | / |
| 2021 | Yap [49] | Single-arm | 118 | 68 | Male 85 Female 33 | / | Epithelioid 82 Sarcomatoid 10 Biphasic 9 Unknown 17 | I–III 60 IV 58 | ECOG 0: 44 ECOG 1: 74 | Positive 77 Negative 31 Not Evaluable 10 |
| 2021 | Fennell, D. A. [44] | RCT | Nivolumab: 221 Placebo: 111 | Nivolumab: 70 Placebo: 71 | Nivolumab: Male 167 Female 54 Placebo: Male 86 Female 25 | Nivolumab: Yes 150 No 65 Missing 6 Placebo: Yes 80 No 30 Missing 1 | Nivolumab: Epithelioid 195 Non-Epithelioid 26 Placebo: Epithelioid 98 Non-Epithelioid 13 | / | ECOG 0: 0 ECOG 1: 15 ECOG 2: 2 | Nivolumab: <1% 101 ≥1% 60 Missing 60 Placebo: <1% 65 ≥1% 26 Missing 20 |
| Year | Author | Study | Design | Sample Size | Comparison | mPFS (95% CI), m | mOS (95% CI), m |
|---|---|---|---|---|---|---|---|
| 2015 | Krug [26] | VANTAGE-014 | RCT | 329 vs. 332 | Targeting drugs vs. Placebo | 1.575 (1.525–1.775) vs. 1.525 (1.5–1.525) | 7.675 (6.675–9.025) vs. 6.775 (5.775–7.975) |
| 2017 | Maio [31] | DETERMINE | RCT | 382 vs. 189 | ICIs vs. Placebo | 2.8 (2.8–2.8) vs. 2.7 (2.7–2.8) | 7.7 (6.8–8.9) vs. 7.3 (5.9–8.7) |
| 2020 | Popat [42] | PROMISE-meso | RCT | 73 vs. 71 | ICIs vs. CT | 2.5 (2.1–4.2) vs. 3.4 (2.2–4.3) | 10.7 (7.6–15) vs. 12.4 (7.4–16.1) |
| 2021 | Kim [45] | - | Cohort study | 115 vs. 61 | ICIs vs. CT | - | 8.7 (7.7–10.9) vs. 5.0 (4.0–6.4) |
| 2021 | Pinto [48] | RAMES | RCT | 80 vs. 81 | Targeting drugs vs. Placebo | 6.4 (5.5–7.6) vs. 3.3 (3.0–3.9) | 13.8 (12.7–14.4) vs. 7.5 (6.9–8.9) |
| 2021 | Fennell [44] | CONFIRM | RCT | 221 vs. 111 | ICIs vs. Placebo | 3.0 (2.8–4.1) vs. 1.8 (1.4–2.6) | 10.2 (8.5–12.1) vs. 6.9 (5.0–8.0) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guo, X.; Lin, L.; Zhu, J. Immunotherapy vs. Chemotherapy in Subsequent Treatment of Malignant Pleural Mesothelioma: Which Is Better? J. Clin. Med. 2023, 12, 2531. https://doi.org/10.3390/jcm12072531
Guo X, Lin L, Zhu J. Immunotherapy vs. Chemotherapy in Subsequent Treatment of Malignant Pleural Mesothelioma: Which Is Better? Journal of Clinical Medicine. 2023; 12(7):2531. https://doi.org/10.3390/jcm12072531
Chicago/Turabian StyleGuo, Xiaotong, Lede Lin, and Jiang Zhu. 2023. "Immunotherapy vs. Chemotherapy in Subsequent Treatment of Malignant Pleural Mesothelioma: Which Is Better?" Journal of Clinical Medicine 12, no. 7: 2531. https://doi.org/10.3390/jcm12072531