
Effectiveness of Repetitive Transcranial Magnetic Stimulation (rTMS) Add-On Therapy to a Standard Treatment in Individuals with Multiple Sclerosis and Concomitant Symptoms of Depression—Results from a Randomized Clinical Trial and Pilot Study



Abstract
:1. Introduction
2. Method
2.1. Participants
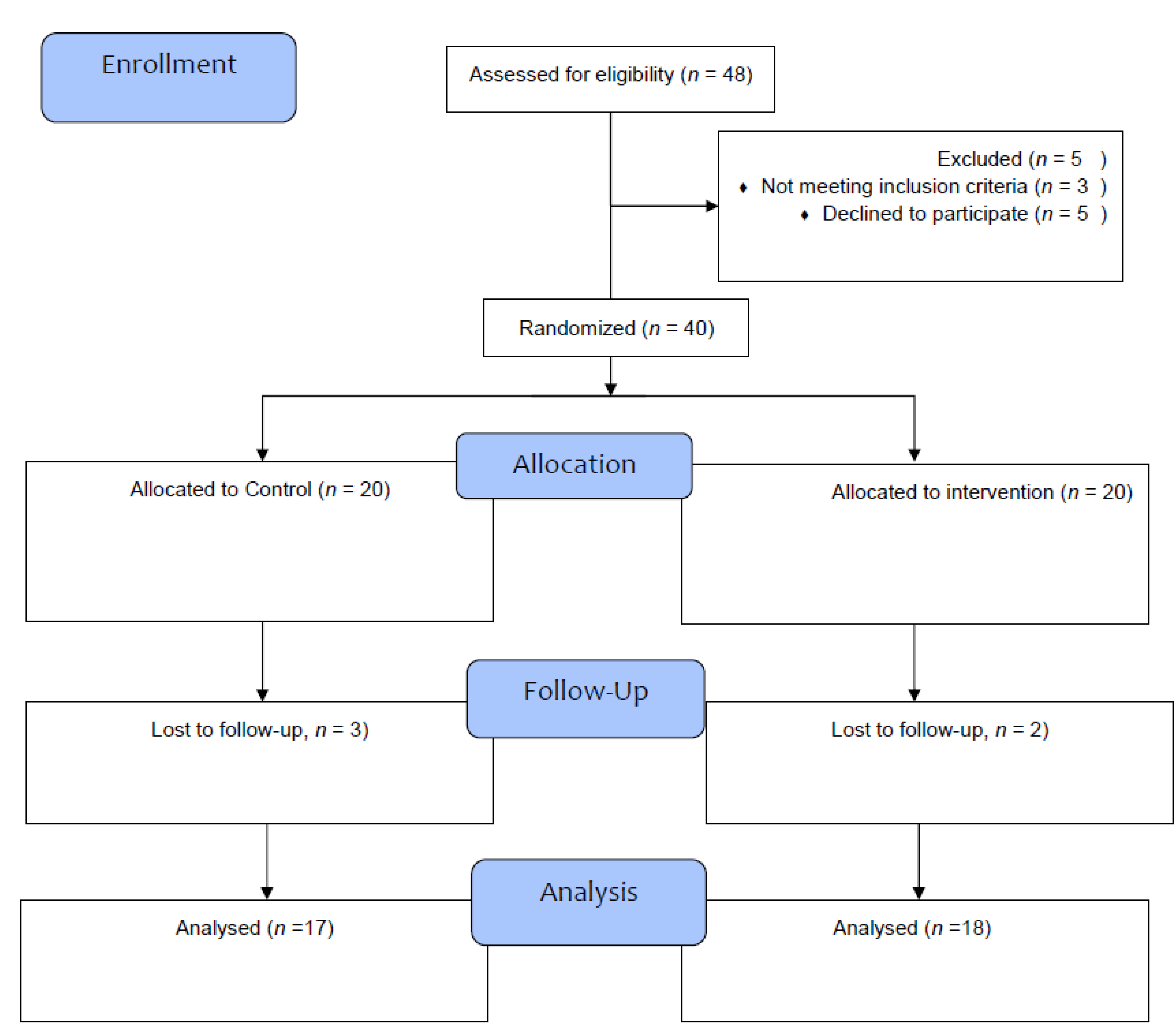
2.2. Procedure
2.3. Sample Size Calculations
2.4. Measures
2.4.1. Sociodemographic and MS-Related Information
2.4.2. Fatigue
2.4.3. Depression Severity
2.4.4. Cognitive Performance
2.4.5. Degree of Disability
3. Interventions
3.1. Medications
3.2. Repetitive Transcranial Magnetic Stimulation
3.3. Statistical Analysis
4. Results
4.1. General Information
4.2. Symptoms of Depression, Fatigue, Cognitive Performance, and Degree of Disability from the Beginning to the End of the Study and between Participants in the Active rTMS and rTMS Sham-Condition
5. Discussion
5.1. rTMS and Depression
5.2. rTMS and Fatigue
5.3. rTMS and Cognitive Performance
5.4. rTMS and Disability
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dobson, R.; Giovannoni, G. Multiple sclerosis—A review. Eur. J. Neurol. 2019, 26, 27–40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McGinley, M.P.; Goldschmidt, C.H.; Rae-Grant, A.D. Diagnosis and Treatment of Multiple Sclerosis: A Review. JAMA 2021, 325, 765–779. [Google Scholar] [CrossRef] [PubMed]
- Kaminska, J.; Koper, O.M.; Piechal, K.; Kemona, H. Multiple sclerosis—Etiology and diagnostic potential. Adv. Hyg. Exp. Med. 2017, 71, 551–563. [Google Scholar] [CrossRef] [PubMed]
- McKay, K.A.; Kwan, V.; Duggan, T.; Tremlett, H. Risk factors associated with the onset of relapsing-remitting and primary progressive multiple sclerosis: A systematic review. BioMed Res. Int. 2015, 2015, 817238. [Google Scholar] [CrossRef] [Green Version]
- Nicholas, R.; Rashid, W. Multiple sclerosis. Am. Fam. Physician 2013, 87, 712–714. [Google Scholar]
- Owens, B. Multiple sclerosis. Nature 2016, 540, S1. [Google Scholar] [CrossRef]
- Burns, M.N.; Nawacki, E.; Siddique, J.; Pelletier, D.; Mohr, D.C. Prospective examination of anxiety and depression before and during confirmed and pseudoexacerbations in patients with multiple sclerosis. Psychosom. Med. 2013, 75, 76–82. [Google Scholar] [CrossRef] [Green Version]
- Boeschoten, R.E.; Braamse, A.M.J.; Beekman, A.T.F.; Cuijpers, P.; van Oppen, P.; Dekker, J.; Uitdehaag, B.M.J. Prevalence of depression and anxiety in Multiple Sclerosis: A systematic review and meta-analysis. J. Neurol. Sci. 2017, 372, 331–341. [Google Scholar] [CrossRef]
- Peres, D.S.; Rodrigues, P.; Viero, F.T.; Frare, J.M.; Kudsi, S.Q.; Meira, G.M.; Trevisan, G. Prevalence of depression and anxiety in the different clinical forms of multiple sclerosis and associations with disability: A systematic review and meta-analysis. Brain Behav. Immun. Health 2022, 24, 100484. [Google Scholar] [CrossRef]
- Faguy, K. Multiple Sclerosis: An Update. Radiol. Technol. 2016, 87, 529–550. [Google Scholar]
- Prakash, R.S.; Schirda, B.; Valentine, T.R.; Crotty, M.; Nicholas, J.A. Emotion dysregulation in multiple sclerosis: Impact on symptoms of depression and anxiety. Mult. Scler. Relat. Disord. 2019, 36, 101399. [Google Scholar] [CrossRef] [PubMed]
- Wallis, O.; Bol, Y.; Kohler, S.; van Heugten, C. Anxiety in multiple sclerosis is related to depressive symptoms and cognitive complaints. Acta Neurol. Scand. 2019, 141, 212–218. [Google Scholar] [CrossRef] [PubMed]
- Yadav, R.; Zigmond, A.S. Temporal lobe lesions and psychosis in multiple sclerosis. BMJ Case Rep. 2010, 2010, bcr0120102651. [Google Scholar] [CrossRef] [PubMed]
- Doogan, C.; Playford, E.D. Supporting work for people with multiple sclerosis. Mult. Scler. J. 2014, 20, 646–650. [Google Scholar] [CrossRef] [PubMed]
- Benedict, R.H.; Rodgers, J.D.; Emmert, N.; Kininger, R.; Weinstock-Guttman, B. Negative work events and accommodations in employed multiple sclerosis patients. Mult. Scler. J. 2014, 20, 116–119. [Google Scholar] [CrossRef]
- Kordovski, V.M.; Frndak, S.E.; Fisher, C.S.; Rodgers, J.; Weinstock-Guttman, B.; Benedict, R.H.B. Identifying employed multiple sclerosis patients at-risk for job loss: When do negative work events pose a threat? Mult. Scler. Relat. Disord. 2015, 4, 409–413. [Google Scholar] [CrossRef]
- Niedermoser, D.W.; Kalak, N.; Kiyhankhadiv, A.; Brand, S.; Walter, C.; Schweinfurth, N.; Lang, U.E. Workplace-Related Interpersonal Group Psychotherapy to Improve Life at Work in Individuals with Major Depressive Disorders: A Randomized Interventional Pilot Study. Front. Psychiatry 2020, 11, 168. [Google Scholar] [CrossRef] [PubMed]
- Marck, C.H.; Aitken, Z.; Simpson, S., Jr.; Weiland, T.J.; Kavanagh, A.; Jelinek, G.A. Predictors of Change in Employment Status and Associations with Quality of Life: A Prospective International Study of People with Multiple Sclerosis. J. Occup. Rehabil. 2020, 30, 105–114. [Google Scholar] [CrossRef] [Green Version]
- Fiest, K.M.; Walker, J.R.; Bernstein, C.N.; Graff, L.A.; Zarychanski, R.; Abou-Setta, A.M.; Patten, S.B.; Sareen, J.; Bolton, J.M.; Marriott, J.J.; et al. Systematic review and meta-analysis of interventions for depression and anxiety in persons with multiple sclerosis. Mult. Scler. Relat. Disord. 2016, 5, 12–26. [Google Scholar] [CrossRef] [Green Version]
- Taylor, R.; Galvez, V.; Loo, C. Transcranial magnetic stimulation (TMS) safety: A practical guide for psychiatrists. Australas. Psychiatry 2018, 26, 189–192. [Google Scholar] [CrossRef]
- Matsumoto, H.; Ugawa, Y. Repetitive Transcranial Magnetic Stimulation for Parkinson’s Disease: A Review. Brain Nerve 2017, 69, 219–225. [Google Scholar] [CrossRef] [PubMed]
- Höppner, J.; Schulz, M.; Irmisch, G.; Mau, R.; Schläfke, D.; Richter, J. Antidepressant efficacy of two different rTMS procedures. High frequency over left versus low frequency over right prefrontal cortex compared with sham stimulation. Eur. Arch. Psychiatry Clin. Neurosci. 2003, 253, 103–109. [Google Scholar] [CrossRef] [PubMed]
- Godfrey, K.E.M.; Muthukumaraswamy, S.D.; Stinear, C.M.; Hoeh, N. Effect of rTMS on GABA and glutamate levels in treatment-resistant depression: An MR spectroscopy study. Psychiatry Res. Neuroimaging 2021, 317, 111377. [Google Scholar] [CrossRef] [PubMed]
- Palm, U.; Ayache, S.S.; Padberg, F.; Lefaucheur, J.P. Non-invasive brain stimulation therapy in multiple sclerosis: A review of tDCS, rTMS and ECT results. Brain Stimul. 2014, 7, 849–854. [Google Scholar] [CrossRef] [PubMed]
- Iodice, R.; Manganelli, F.; Dubbioso, R. The therapeutic use of non-invasive brain stimulation in multiple sclerosis—A review. Restor. Neurol. Neurosci. 2017, 35, 497–509. [Google Scholar] [CrossRef]
- Somaa, F.A.; de Graaf, T.A.; Sack, A.T. Transcranial Magnetic Stimulation in the Treatment of Neurological Diseases. Front. Neurol. 2022, 13, 793253. [Google Scholar] [CrossRef]
- Fregni, F.; Pascual-Leone, A. Transcranial magnetic stimulation for the treatment of depression in neurologic disorders. Curr. Psychiatry Rep. 2005, 7, 381–390. [Google Scholar] [CrossRef]
- Kan, R.L.D.; Xu, G.X.J.; Shu, K.T.; Lai, F.H.Y.; Kranz, G.; Kranz, G.S. Effects of non-invasive brain stimulation in multiple sclerosis: Systematic review and meta-analysis. Adv. Chronic Dis. 2022, 13, 20406223211069198. [Google Scholar] [CrossRef]
- Polman, C.H.; Reingold, S.C.; Banwell, B.; Clanet, M.; Cohen, J.A.; Filippi, M.; Fujihara, K.; Havrdova, E.; Hutchinson, M.; Kappos, L. Diagnostic criteria for multiple sclerosis: 2010 revisions to the McDonald criteria. Ann. Neurol. 2011, 69, 292–302. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thompson, A.J.; Banwell, B.L.; Barkhof, F.; Carroll, W.M.; Coetzee, T.; Comi, G.; Correale, J.; Fazekas, F.; Filippi, M.; Freedman, M.S.; et al. Diagnosis of multiple sclerosis: 2017 revisions of the McDonald criteria. Lancet Neurol. 2018, 17, 162–173. [Google Scholar] [CrossRef]
- Meyer-Moock, S.; Feng, Y.S.; Maeurer, M.; Dippel, F.W.; Kohlmann, T. Systematic literature review and validity evaluation of the Expanded Disability Status Scale (EDSS) and the Multiple Sclerosis Functional Composite (MSFC) in patients with multiple sclerosis. BMC Neurol. 2014, 14, 58. [Google Scholar] [CrossRef] [Green Version]
- First, M. Structured Clinical Interview for the DSM (SCID). Encycl. Clin. Psychol. 2015, 1–6. [Google Scholar] [CrossRef]
- Kim, D.R.; Wang, E.; McGeehan, B.; Snell, J.; Ewing, G.; Iannelli, C.; O’Reardon, J.P.; Sammel, M.D.; Epperson, C.N. Randomized controlled trial of transcranial magnetic stimulation in pregnant women with major depressive disorder. Brain Stimul. 2019, 12, 96–102. [Google Scholar] [CrossRef] [PubMed]
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G* Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef] [PubMed]
- Krupp, L.B.; LaRocca, N.G.; Muir-Nash, J.; Steinberg, A.D. The fatigue severity scale. Application to patients with multiple sclerosis and systemic lupus erythematosus. Arch. Neurol. 1989, 46, 1121–1123. [Google Scholar] [CrossRef]
- Ahmadpanah, M.; Sheikhbabaei, M.; Haghighi, M.; Roham, F.; Jahangard, L.; Akhondi, A.; Sadeghi Bahmani, D.; Bajoghli, H.; Holsboer-Trachsler, E.; Brand, S. Validity and test-retest reliability of the Persian version of the Montgomery-Asberg Depression Rating Scale. Neuropsychiatr. Dis. Treat. 2016, 12, 603–607. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Montgomery, S.A.; Asberg, M. A new depression scale designed to be sensitive to change. Br. J. Psychiatry J. Ment. Sci. 1979, 134, 382–389. [Google Scholar] [CrossRef]
- Nasreddine, Z.S.; Phillips, N.A.; Bedirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A brief screening tool for mild cognitive impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef]
- Hobson, J. The Montreal Cognitive Assessment (MoCA). Occup. Med. 2015, 65, 764–765. [Google Scholar] [CrossRef] [Green Version]
- Kurtzke, J.F. On the origin of EDSS. Mult. Scler. Relat. Disord. 2015, 4, 95–103. [Google Scholar] [CrossRef]
- Haghighi, M.; Ludyga, S.; Rahimi, B.; Jahangard, L.; Ahmadpanah, M.; Torabian, S.; Esnaashari, F.; Nazaribadie, M.; Bajoghli, H.; Sadeghi Bahmani, D.; et al. In patients suffering from major depressive disorders, quantitative EEG showed favorable changes in left and right prefrontal cortex. Psychiatry Res. 2017, 251, 137–141. [Google Scholar] [CrossRef] [PubMed]
- Shayganfard, M.; Jahangard, L.; Nazaribadie, M.; Haghighi, M.; Ahmadpanah, M.; Sadeghi Bahmani, D.; Bajoghli, H.; Holsboer-Trachsler, E.; Brand, S. Repetitive Transcranial Magnetic Stimulation Improved Symptoms of Obsessive-Compulsive Disorders but Not Executive Functions: Results from a Randomized Clinical Trial with Crossover Design and Sham Condition. Neuropsychobiology 2016, 74, 115–124. [Google Scholar] [CrossRef] [PubMed]
- Jahangard, L.; Haghighi, M.; Shyayganfard, M.; Ahmadpanah, M.; Sadeghi Bahmani, D.; Bajoghli, H.; Holsboer-Trachsler, E.; Brand, S. Repetitive Transcranial Magnetic Stimulation Improved Symptoms of Obsessive-Compulsive Disorder, but Also Cognitive Performance: Results from a Randomized Clinical Trial with a Cross-Over Design and Sham Condition. Neuropsychobiology 2016, 73, 224–232. [Google Scholar] [CrossRef] [PubMed]
- Chail, A.; Saini, R.K.; Bhat, P.S.; Srivastava, K.; Chauhan, V. Transcranial magnetic stimulation: A review of its evolution and current applications. Ind. Psychiatry J. 2018, 27, 172–180. [Google Scholar] [CrossRef]
- Groppa, S.; Oliviero, A.; Eisen, A.; Quartarone, A.; Cohen, L.G.; Mall, V.; Kaelin-Lang, A.; Mima, T.; Rossi, S.; Thickbroom, G.W.; et al. A practical guide to diagnostic transcranial magnetic stimulation: Report of an IFCN committee. Clin. Neurophysiol. 2012, 123, 858–882. [Google Scholar] [CrossRef] [Green Version]
- Hordacre, B.; Chau, A.; Graetz, L.; Hillier, S. Extended Repetitive Transcranial Magnetic Stimulation Therapy for Post-stroke Depression in a Patient with a Pre-frontal Cortical Lesion: A Case Study. Front. Neurol. 2022, 13, 869248. [Google Scholar] [CrossRef]
- Johnson, K.A.; Baig, M.; Ramsey, D.; Lisanby, S.H.; Avery, D.; McDonald, W.M.; Li, X.; Bernhardt, E.R.; Haynor, D.R.; Holtzheimer, P.E.; et al. Prefrontal rTMS for treating depression: Location and intensity results from the OPT-TMS multi-site clinical trial. Brain Stimul. 2013, 6, 108–117. [Google Scholar] [CrossRef] [Green Version]
- Sparing, R.; Buelte, D.; Meister, I.G.; Paus, T.; Fink, G.R. Transcranial magnetic stimulation and the challenge of coil placement: A comparison of conventional and stereotaxic neuronavigational strategies. Hum. Brain Mapp. 2008, 29, 82–96. [Google Scholar] [CrossRef]
- Feffer, K.; Lee, H.H.; Mansouri, F.; Giacobbe, P.; Vila-Rodriguez, F.; Kennedy, S.H.; Daskalakis, Z.J.; Blumberger, D.M.; Downar, J. Early symptom improvement at 10 sessions as a predictor of rTMS treatment outcome in major depression. Brain Stimul. 2018, 11, 181–189. [Google Scholar] [CrossRef] [Green Version]
- Spitz, N.A.; Pace, B.D.; Ten Eyck, P.; Trapp, N.T. Early Improvement Predicts Clinical Outcomes Similarly in 10 Hz rTMS and iTBS Therapy for Depression. Front. Psychiatry 2022, 13, 863225. [Google Scholar] [CrossRef]
- Mirman, A.M.; Corlier, J.; Wilson, A.C.; Tadayonnejad, R.; Marder, K.G.; Pleman, C.M.; Krantz, D.E.; Wilke, S.A.; Levitt, J.G.; Ginder, N.D.; et al. Absence of early mood improvement as a robust predictor of rTMS nonresponse in major depressive disorder. Depress Anxiety 2022, 39, 123–133. [Google Scholar] [CrossRef] [PubMed]
- Kazemi, R.; Ghazanfari, F.; Gholamrezaei, S. Effectiveness of Bilateral Repetitive Transcranial Magnetic Stimulation on Anhedonia and Depression Symptoms in Major Depressive Disorder Patients. J. Clin. Psychol. 2018, 10, 23–33. [Google Scholar] [CrossRef]
- Brunelin, J.; Poulet, E.; Boeuve, C.; Zeroug-vial, H.; d’Amato, T.; Saoud, M. Efficacy of repetitive transcranial magnetic stimulation (rTMS) in major depression: A review. L’Encephale 2007, 33, 126–134. [Google Scholar] [CrossRef] [PubMed]
- Croarkin, P.E.; Nakonezny, P.A.; Wall, C.A.; Murphy, L.L.; Sampson, S.M.; Frye, M.A.; Port, J.D. Transcranial magnetic stimulation potentiates glutamatergic neurotransmission in depressed adolescents. Psychiatry Res. Neuroimaging 2016, 247, 25–33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McClintock, S.M.; Reti, I.M.; Carpenter, L.L.; McDonald, W.M.; Dubin, M.; Taylor, S.F.; Cook, I.A.; O’Reardon, J.; Husain, M.M.; Wall, C.; et al. Consensus Recommendations for the Clinical Application of Repetitive Transcranial Magnetic Stimulation (rTMS) in the Treatment of Depression. J. Clin. Psychiatry 2018, 79, 3651. [Google Scholar] [CrossRef]
- Liu, S.; Wang, X.; Yu, R.; Sun, Y. Effect of transcranial magnetic stimulation on treatment effect and immune function. Saudi J. Biol. Sci. 2022, 29, 379–384. [Google Scholar] [CrossRef]
- Colasanto, M.; Madigan, S.; Korczak, D.J. Depression and inflammation among children and adolescents: A meta-analysis. J. Affect. Disord. 2020, 277, 940–948. [Google Scholar] [CrossRef]
- Osimo, E.F.; Baxter, L.J.; Lewis, G.; Jones, P.B.; Khandaker, G.M. Prevalence of low-grade inflammation in depression: A systematic review and meta-analysis of CRP levels. Psychol. Med. 2019, 49, 1958–1970. [Google Scholar] [CrossRef]
- Rapaport, M.H.; Nierenberg, A.A.; Schettler, P.J.; Kinkead, B.; Cardoos, A.; Walker, R.; Mischoulon, D. Inflammation as a predictive biomarker for response to omega-3 fatty acids in major depressive disorder: A proof-of-concept study. Mol. Psychiatry 2016, 21, 71–79. [Google Scholar] [CrossRef] [Green Version]
- Tolkien, K.; Bradburn, S.; Murgatroyd, C. An anti-inflammatory diet as a potential intervention for depressive disorders: A systematic review and meta-analysis. Clin. Nutr. 2019, 38, 2045–2052. [Google Scholar] [CrossRef] [Green Version]
- Bhattacharyya, P.; Anand, A.; Lin, J.; Altinay, M. Left Dorsolateral Prefrontal Cortex Glx/tCr Predicts Efficacy of High Frequency 4- to 6-Week rTMS Treatment and Is Associated with Symptom Improvement in Adults with Major Depressive Disorder: Findings From a Pilot Study. Front. Psychiatry 2021, 12, 665347. [Google Scholar] [CrossRef] [PubMed]
- Liu, M.; Fan, S.; Xu, Y.; Cui, L. Non-invasive brain stimulation for fatigue in multiple sclerosis patients: A systematic review and meta-analysis. Mult. Scler. Relat. Disord. 2019, 36, 101375. [Google Scholar] [CrossRef] [PubMed]
- Krogh, S.; Jønsson, A.B.; Aagaard, P.; Kasch, H. Efficacy of repetitive transcranial magnetic stimulation for improving lower limb function in individuals with neurological disorders: A systematic review and meta-analysis of randomized sham-controlled trials. J. Rehabil. Med. 2022, 54, jrm00256. [Google Scholar] [CrossRef]
- Korzhova, J.; Bakulin, I.; Sinitsyn, D.; Poydasheva, A.; Suponeva, N.; Zakharova, M.; Piradov, M. High-frequency repetitive transcranial magnetic stimulation and intermittent theta-burst stimulation for spasticity management in secondary progressive multiple sclerosis. Eur. J. Neurol. 2019, 26, 680-e44. [Google Scholar] [CrossRef] [PubMed]
- Mori, F.; Ljoka, C.; Magni, E.; Codecà, C.; Kusayanagi, H.; Monteleone, F.; Sancesario, A.; Bernardi, G.; Koch, G.; Foti, C.; et al. Transcranial magnetic stimulation primes the effects of exercise therapy in multiple sclerosis. J. Neurol. 2011, 258, 1281–1287. [Google Scholar] [CrossRef]
- Nasios, G.; Messinis, L.; Dardiotis, E.; Papathanasopoulos, P. Repetitive Transcranial Magnetic Stimulation, Cognition, and Multiple Sclerosis: An Overview. Behav. Neurol. 2018, 2018, 8584653. [Google Scholar] [CrossRef] [Green Version]
- Sadeghi Bahmani, D.; Faraji, P.; Faraji, R.; Lang, U.E.; Holsboer-Trachsler, E.; Brand, S. Is emotional functioning related to academic achievement among university students? Results from a cross-sectional Iranian sample. Rev. Bras. Psiquiatr. 2018, 40, 290–295. [Google Scholar] [CrossRef] [Green Version]
- Rock, P.L.; Roiser, J.P.; Riedel, W.J.; Blackwell, A.D. Cognitive impairment in depression: A systematic review and meta-analysis. Psychol. Med. 2014, 44, 2029–2040. [Google Scholar] [CrossRef] [Green Version]
- Roca, M.; Vives, M.; Lopez-Navarro, E.; Garcia-Campayo, J.; Gili, M. Cognitive impairments and depression: A critical review. Actas Esp. De Psiquiatr. 2015, 43, 187–193. [Google Scholar]
- Sadeghi Bahmani, D.; Gerber, M.; Kalak, N.; Lemola, S.; Clough, P.J.; Calabrese, P.; Shaygannejad, V.; Puhse, U.; Holsboer-Trachsler, E.; Brand, S. Mental toughness, sleep disturbances, and physical activity in patients with multiple sclerosis compared to healthy adolescents and young adults. Neuropsychiatr. Dis. Treat. 2016, 12, 1571–1579. [Google Scholar] [CrossRef]
- Sadeghi Bahmani, D.; Gonzenbach, R.; Kesselring, J.; Bansi, J.; Motl, R.W.; Cordier, D.; Rothen, O.; Niedermoser, D.; Gerber, M.; Brand, S. Among Persons with Multiple Sclerosis (MS), Objective Sleep, Psychological Functioning, and Higher Physical Activity Scores Remained Stable Over 2 Years-Results From a Small Study Under Naturalistic Conditions. Front. Psychiatry 2020, 11, 586244. [Google Scholar] [CrossRef]
- Sadeghi Bahmani, D.; Razazian, N.; Farnia, V.; Alikhani, M.; Tatari, F.; Brand, S. Compared to an active control condition, in persons with multiple sclerosis two different types of exercise training improved sleep and depression, but not fatigue, paresthesia, and intolerance of uncertainty. Mult. Scler. Relat. Disord. 2019, 36, 101356. [Google Scholar] [CrossRef] [PubMed]
- Sadeghi Bahmani, D.; Razazian, N.; Motl, R.W.; Farnia, V.; Alikhani, M.; Pühse, U.; Gerber, M.; Brand, S. Physical activity interventions can improve emotion regulation and dimensions of empathy in persons with multiple sclerosis: An exploratory study. Mult. Scler. Relat. Disord. 2020, 37, 101380. [Google Scholar] [CrossRef] [PubMed]
- Sadeghi Bahmani, D.; Esmaeili, L.; Shaygannejad, V.; Gerber, M.; Kesselring, J.; Lang, U.E.; Holsboer-Trachsler, E.; Brand, S. Stability of Mental Toughness, Sleep Disturbances, and Physical Activity in Patients with Multiple Sclerosis (MS)-A Longitudinal and Pilot Study. Front. Psychiatry 2018, 9, 182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sadeghi Bahmani, D.; Gonzenbach, R.; Motl, R.W.; Bansi, J.; Rothen, O.; Niedermoser, D.; Gerber, M.; Brand, S. Better Objective Sleep Was Associated with Better Subjective Sleep and Physical Activity; Results from an Exploratory Study under Naturalistic Conditions among Persons with Multiple Sclerosis. Int. J. Environ. Res. Public Health 2020, 17, 3522. [Google Scholar] [CrossRef]
- Sadeghi Bahmani, D.; Kesselring, J.; Papadimitriou, M.; Bansi, J.; Puhse, U.; Gerber, M.; Shaygannejad, V.; Holsboer-Trachsler, E.; Brand, S. In Patients with Multiple Sclerosis, Both Objective and Subjective Sleep, Depression, Fatigue, and Paresthesia Improved after 3 Weeks of Regular Exercise. Front. Psychiatry 2019, 10, 265. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Study Conditions | Statistics | |||
|---|---|---|---|---|
| Variable | rTMS | Sham | ||
| N | 20 | 20 | ||
| M (SD) | M (SD) | |||
| Age (years) | 32.05 (6.82) | 31.95 (6.93) | t(38) = 0.05 | |
| Duration disease (years) | 8.88 (2.88) | 7.67 (2.04) | t(38) = 1.52 | |
| n (%) | n (%) | |||
| Gender | Female | 12 (30) | 11 (27.5) | X2(N = 40, df = 1) = 0.10 |
| Male | 8 (20) | 9 (22.5) | ||
| Marital status | Married | 15 (37.5) | 13 (32.5) | X2(N = 40, df = 1) = 0.48 |
| Single | 5 (12.5) | 7 (17.5) | ||
| Education | Under diploma | 6 (15) | 3 (7.5) | X2(N = 40, df = 2) = 1.30 |
| Diploma | 8 (20) | 10 (25) | ||
| Academic degree | 6 (15) | 7 (17.5) | ||
| Baseline | Study End | |||
|---|---|---|---|---|
| rTMS | Sham | I rTMS | Sham | |
| N | 20 | 20 | 20 | 20 |
| M (SD) | M (SD) | M (SD) | M (SD) | |
| Depression | 28.72 (2.72) | 28.94 (2.97) | 23.17 (2.92) | 25.86 (4.06) |
| Fatigue | 6.17 (0.75) | 6.29 (0.59) | 5.75 (0.97) | 6.26 (0.62) |
| Cognitive performance | 24.22 (1.80) | 24.88 (1.58) | 26.00 (1.78) | 25.70 (1.80) |
| Median (range) | Median (range) | Median (range) | Median (range) | |
| Disability 1 | 4.75 (2.00–6.50) | 3.50 (2.50–6.00) | 3.50 (2.00–5.50) | 3.50 (3.00–5.50) |
| Inferential Statistics | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Time | Group | Time × Group Interaction | |||||||
| F | [ES] | F | [ES] | F | [ES] | ||||
| Depression | F(1, 33) = 44.08 *** | 0.572 [L] | F(1, 33) = 10.95 *** | 0.249 [L] | F(1, 33) = 37.20 *** | 0.530 [L] | |||
| Fatigue | F(1, 33) = 9.03 ** | 0.215 [L] | F(1, 33) = 1.75 | 0.05 [T] | F(1, 33) = 6.80 * | 0.171 [L] | |||
| Cognitive performance | F(1, 33) = 9.50 ** | 0.223 [L] | F(1, 33) = 0.19 | 0.00 [T] | F(1, 33) = 1.28 | 0.037 [S] | |||
| Disability 1 | F(1, 33) = 10.82 ** | 0.222 [L] | F(1, 33)= 0.00 | 0.00 [T] | F(1, 33) = 7.24 ** | 0.162 [L] | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ahmadpanah, M.; Amini, S.; Mazdeh, M.; Haghighi, M.; Soltanian, A.; Jahangard, L.; Keshavarzi, A.; Brand, S. Effectiveness of Repetitive Transcranial Magnetic Stimulation (rTMS) Add-On Therapy to a Standard Treatment in Individuals with Multiple Sclerosis and Concomitant Symptoms of Depression—Results from a Randomized Clinical Trial and Pilot Study. J. Clin. Med. 2023, 12, 2525. https://doi.org/10.3390/jcm12072525
Ahmadpanah M, Amini S, Mazdeh M, Haghighi M, Soltanian A, Jahangard L, Keshavarzi A, Brand S. Effectiveness of Repetitive Transcranial Magnetic Stimulation (rTMS) Add-On Therapy to a Standard Treatment in Individuals with Multiple Sclerosis and Concomitant Symptoms of Depression—Results from a Randomized Clinical Trial and Pilot Study. Journal of Clinical Medicine. 2023; 12(7):2525. https://doi.org/10.3390/jcm12072525
Chicago/Turabian StyleAhmadpanah, Mohammad, Shiva Amini, Mehrdokht Mazdeh, Mohammad Haghighi, Alireza Soltanian, Leila Jahangard, Amir Keshavarzi, and Serge Brand. 2023. "Effectiveness of Repetitive Transcranial Magnetic Stimulation (rTMS) Add-On Therapy to a Standard Treatment in Individuals with Multiple Sclerosis and Concomitant Symptoms of Depression—Results from a Randomized Clinical Trial and Pilot Study" Journal of Clinical Medicine 12, no. 7: 2525. https://doi.org/10.3390/jcm12072525