
Clinical Effects of Pulmonary Rehabilitation in Very Old Patients with COPD
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
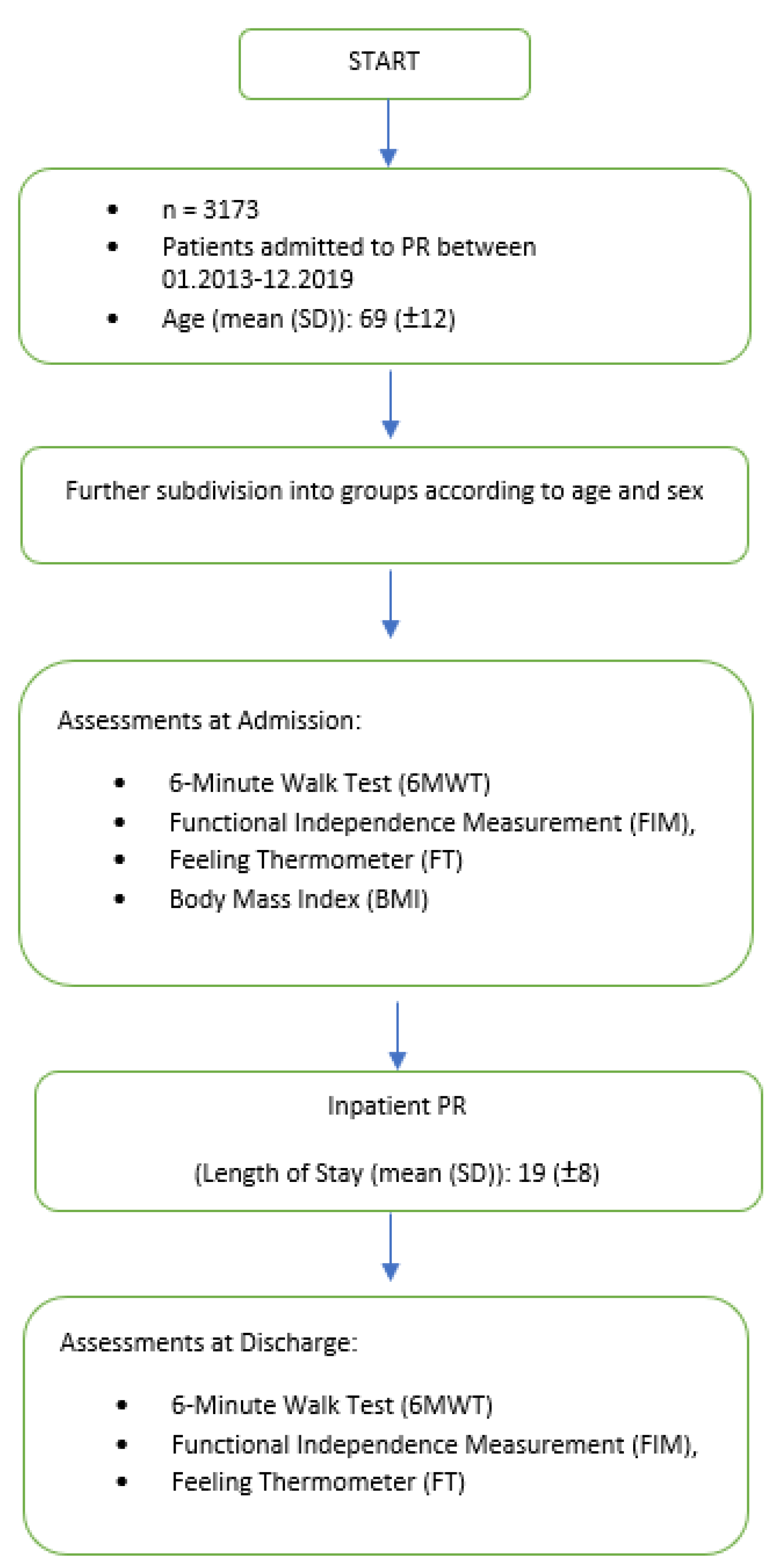
2.1. Design
2.2. PR Intervention
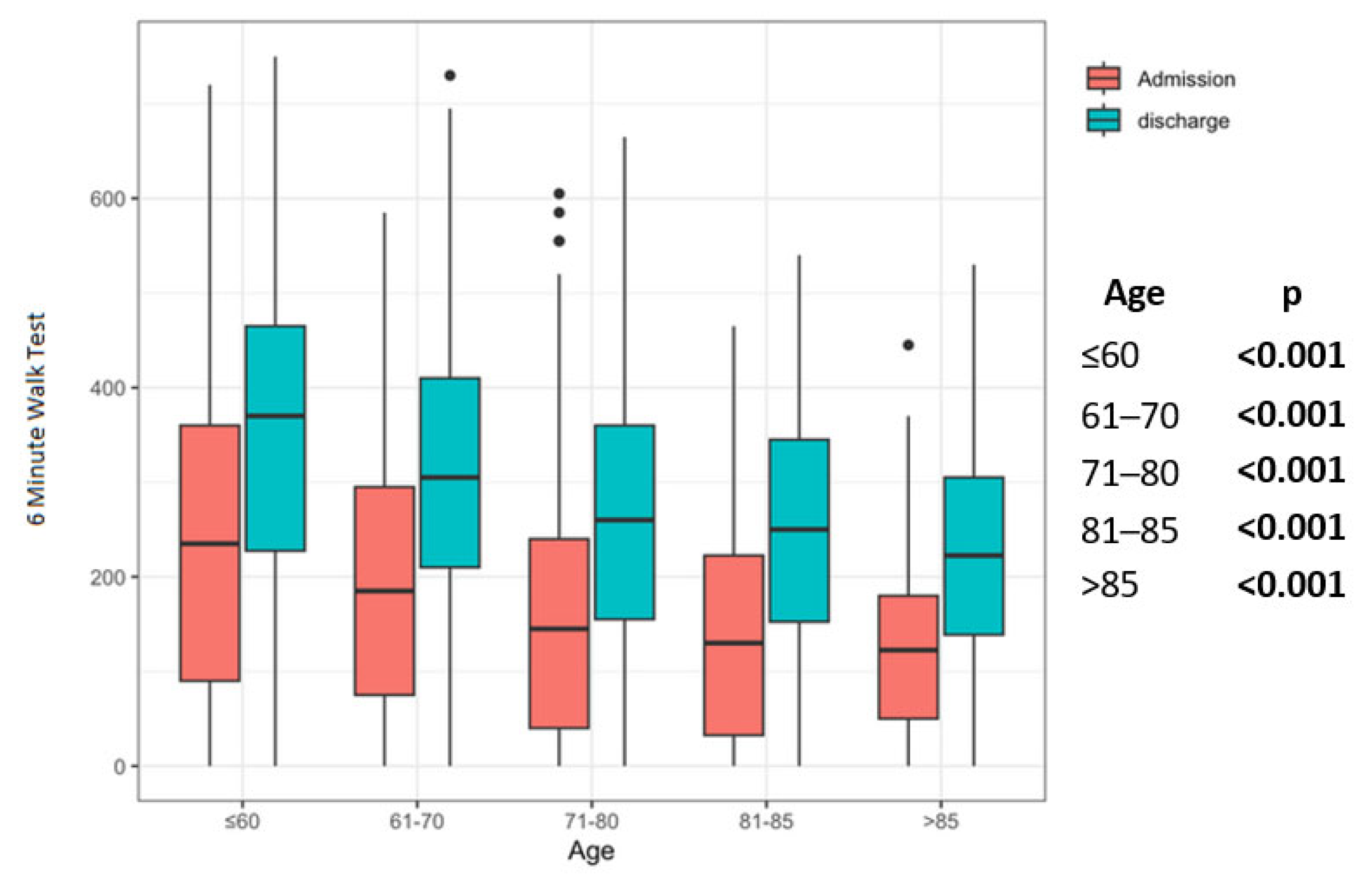
2.3. Exercise Capacity
2.4. Functional Independence Measure
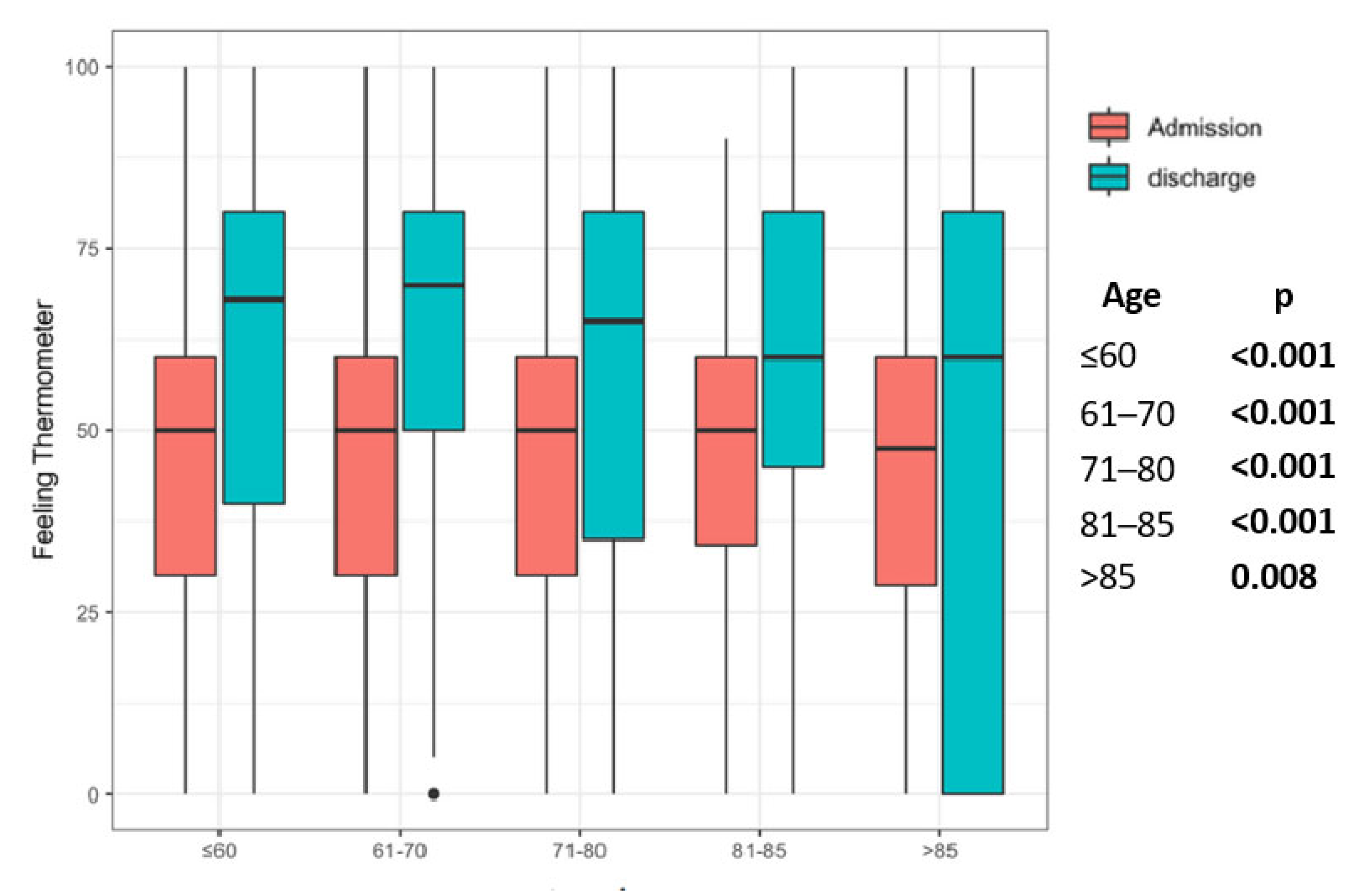
2.5. Feeling Thermometer
2.6. Duration of Inpatient PR
2.7. BMI
2.8. Statistics
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Steiner, M.C.; Lowe, D.; Beckford, K. Socioeconomic deprivation and the outcome of pulmonary rehabilitation in England and Wales. Thorax 2017, 72, 530–537. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pedro, P.I.; Maia-Santos, L.; Braço-Forte, C.; Dias, A.; Cruz, C.; Rodrigues, F. Benefits of pulmonary rehabilitation in patients with chronic obstructive pulmonary disease and interstitial lung disease with the same dyspnea severity. Pulmonology 2019, 25, 117–118. [Google Scholar] [CrossRef] [PubMed]
- McCarthy, B.; Casey, D.; Devane, D.; Murphy, K.; Murphy, E.; Lacasse, Y. Pulmonary rehabilitation for chronic obstructive pulmonary disease. Cochrane Database Syst. Rev. 2015, 2, CD003793. [Google Scholar] [CrossRef] [PubMed]
- Goërtz, Y.M.J.; Vaes, A.W.; Spruit, M.A. COPD and pulmonary rehabilitation: New findings from Brazil. J. Bras. Pneumol. 2021, 46, e20200596. [Google Scholar] [CrossRef]
- Chand, M.; Markova, G. The European Union’s aging population: Challenges for human resource management. Thunderbird Int. Bus. Rev. 2019, 61, 519–529. [Google Scholar] [CrossRef]
- Lowery, E.M.; Brubaker, A.L.; Kuhlmann, E.; Kovacs, E.J. The aging lung. Clin. Interv. Aging 2013, 8, 1489–1496. [Google Scholar]
- Gloeckl, R.; Marinov, B.; Pitta, F. Practical recommendations for exercise training in patients with COPD. Eur. Respir. Rev. 2013, 22, 178–186. [Google Scholar] [CrossRef]
- Bourbeau, J.; Collet, J.P.; Schwartzman, K.; Ducruet, T.; Nault, D.; Bradley, C. Economic benefits of self-management education in COPD. Chest 2006, 130, 1704–1711. [Google Scholar] [CrossRef]
- Hsieh, M.-J.; Yang, T.-M.; Tsai, Y.-H. Nutritional supplementation in patients with chronic obstructive pulmonary disease. J. Formos. Med. Assoc. 2016, 115, 595–601. [Google Scholar] [CrossRef] [Green Version]
- Enright, P.L.; Sherrill, D.L. Reference equations for the six-minute walk in healthy adults. Am. J. Respir. Crit. Care Med. 1998, 158, 1384–1387. [Google Scholar] [CrossRef] [Green Version]
- Holland, A.E.; Spruit, M.A.; Troosters, T.; Puhan, M.A.; Pepin, V.; Saey, D.; McCormack, M.; Carlin, B.W.; Sciurba, F.C.; Pitta, F.; et al. An official European Respiratory Society/American Thoracic Society technical standard: Field walking tests in chronic respiratory disease. Eur. Respir. J. 2014, 44, 1428–1446. [Google Scholar] [CrossRef]
- Chan, K.S.; Pfoh, E.R.; Denehy, L.; Elliott, D.; Holland, A.E.; Dinglas, V.D.; Needham, D.M. Construct Validity and Minimal Important Difference of 6-Minute Walk Distance in Survivors of Acute Respiratory Failure. Chest 2015, 147, 1316–1326. [Google Scholar] [CrossRef] [Green Version]
- Guyatt, G.H.; Thompson, P.J.; Berman, L.B.; Sullivan, M.J.; Townsend, M.; Jones, N.L.; Pugsley, S.O. How should we measure function in patients with chronic heart and lung disease? J. Chronic Dis. 1985, 38, 517–524.37. [Google Scholar] [CrossRef]
- Linacre, J.M.; Heinemann, A.W.; Wright, B.D.; Granger, C.V.; Hamilton, B.B. The structure and stability of the Functional Independence Measure. Arch. Phys. Med. Rehabil. 1994, 75, 127–132. [Google Scholar] [CrossRef]
- Pasqua, F.; Biscione, G.L.; Crigna, G.; Gargano, R.; Cardaci, V.; Ferri, L.; Cesario, A.; Clini, E. Use of functional independence measure in rehabilitation of inpatients with respiratory failure. Respir. Med. 2009, 103, 471–476. [Google Scholar] [CrossRef] [Green Version]
- Lavrakas, P.J. Encyclopedia of Survey Research Methods; SAGE Publications, Inc.: Thousand Oaks, CA, USA, 2008. [Google Scholar] [CrossRef]
- Büsching, G. Den Gesundheitszustand einschätzen. Physiopraxis 2014, 12, 44–45. [Google Scholar] [CrossRef]
- Schünemann, H.J.; Griffith, L.; Jaeschke, R.; Goldstein, R.; Stubbing, D.; Guyatt, G.H. Evaluation of the minimal important difference for the feeling thermometer and the St. George’s Respiratory Questionnaire in patients with chronic airflow obstruction. J. Clin. Epidemiol. 2003, 56, 1170–1176. [Google Scholar] [CrossRef]
- Green, R.H.; Singh, S.J.; Williams, J.; Morgan, M.D. A randomised controlled trial of four weeks versus seven weeks of pulmonary rehabilitation in chronic obstructive pulmonary disease. Thorax 2001, 56, 143–145. [Google Scholar] [CrossRef] [Green Version]
- Sewell, L.; Singh, S.J.; Williams, J.E.A.; Collier, R.; Morgan, M.D.L. How long should outpatient pulmonary rehabilitation be? A randomised controlled trial of 4 weeks versus 7 weeks. Thorax 2006, 61, 767–771. [Google Scholar] [CrossRef] [Green Version]
- Foy, C.G.; Rejeski, W.J.; Berry, M.J.; Zaccaro, D.; Woodard, C.M. Gender moderates the effects of exercise therapy on health-related quality of life among COPD patients. Chest 2001, 119, 70–76. [Google Scholar] [CrossRef] [Green Version]
- Berry, M.J.; Rejeski, W.J.; Adair, N.E.; Ettinger, W.H.; Zaccaro, D.J.; Sevick, M.A. A randomized, controlled trial comparing long-term and short-term exercise in patients with chronic obstructive pulmonary disease. J. Cardiopulm. Rehabil. 2003, 23, 60–68. [Google Scholar] [CrossRef] [PubMed]
- Pehlivan, E.; Balci, A.; Yazar, E.; Niksarlioglu, E.; Kiliç, L. The effect of body mass index on pulmonary rehabilitation outcomes in patients with chronic obstructive pulmonary disease. Eurasian J. Pulmonol. 2018, 20, 150–156. [Google Scholar] [CrossRef]
- WHO. Body Mass Index (BMI). Available online: www.who.int/data/gho/data/themes/topics/topic-details/GHO/body-mass-index (accessed on 14 February 2023).
- O’Donnell, D.E.; Ciavaglia, C.E.; Neder, J.A. When obesity and chronic obstructive pulmonary disease collide. Physiological and clinical consequences. Ann. Am. Thorac. Soc. 2014, 11, 635–644. [Google Scholar] [CrossRef] [PubMed]
- Vagaggini, B.; Costa, F.; Antonelli, S. Clinical predictors of the efficacy of a pulmonary rehabilitation programme in patients with COPD. Respir. Med. 2009, 103, 1224–1230. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnston, K.N.; Young, M.; Grimmer, K.A.; Antic, R.; Frith, P.A. Barriers to, and facilitators for, referral to pulmonary rehabilitation in COPD patients from the perspective of Australian general practitioners: A qualitative study. Prim. Care Respir. J. 2013, 22, 319–324. [Google Scholar] [CrossRef] [Green Version]
- Matata, B.M.; Williamson, S.A. A Review of Interventions to Improve Enrolment and Adherence to Cardiac Rehabilitation Among Patients Aged 65 Years or Above. Curr. Cardiol. Rev. 2017, 13, 252–262. [Google Scholar] [CrossRef]
- King, K.M.; Humen, D.P.; Keo, K.K. Cardiac rehabilitation: The forgotten intervention. Can. J. Cardiol. 1999, 15, 979–985. [Google Scholar]
- Baltzan, M.A.; Kamel, H.; Alter, A.; Rotaple, M.; Wolkove, N. Pulmonary rehabilitation improves functional capacity in patients 80 years of age or older. Can. Respir. J. 2004, 11, 407–413. [Google Scholar] [CrossRef] [Green Version]
- Mkacher, W.; Mekki, M.; Tabka, Z. Effect of 6 months of balance training during pulmonary rehabilitation in patients with COPD. J. Cardiopulm. Rehabil. Prev. 2015, 35, 207–213. [Google Scholar] [CrossRef]
- Beauchamp, M.K.; Janaudis-Ferreira, T.; Parreira, V. A randomized controlled trial of balance training during pulmonary rehabilitation for individuals with COPD. Chest 2013, 144, 1803–1810. [Google Scholar] [CrossRef]
- Costa Boffino, C.; Alves Caporali, A.C.; Boari Coelho, D.; Fagundes Xavier, R.; Berto, C.; Marques Da Silva, C.; Tanaka, C.; Teodoro Ramos, R.; Carvalho, R.F. Age and Disease have a Distinct Influence on Postural Balance of Patients with COPD. COPD J. Chronic Obstr. Pulm. Dis. 2019, 16, 246–253. [Google Scholar] [CrossRef]
- Whitney, S.L.; Jacob, R.G.; Sparto, P.J. Acrophobia and pathological height vertigo: Indications for vestibular physical therapy? Phys. Ther. 2005, 85, 443–458. [Google Scholar] [CrossRef] [Green Version]
- Rosario, E.R.; Kaplan, S.E.; Khonsari, S.; Patterson, D. Predicting and assessing fall risk in an acute inpatient rehabilitation facility. Rehabil. Nurs. 2014, 39, 86–93. [Google Scholar] [CrossRef]
- Brighton, L.J.; Bristowe, K.; Bayly, J.; Ogden, M.; Farquhar, M.; Evans, C.J.; Man, W.D.C.; Maddocks, M. Experiences of Pulmonary Rehabilitation in People Living with Chronic Obstructive Pulmonary Disease and Frailty. A Qualitative Interview Study. Ann. Am. Thorac. Soc. 2020, 17, 1213–1221. [Google Scholar] [CrossRef]
- Puhan, M.A.; Behnke, M.; Devereaux, P.J.; Montori, V.M.; Braendli, O.; Frey, M.; Schünemann, H.J. Measurement of agreement on health-related quality of life changes in response to respiratory rehabilitation by patients and physicians-a prospective study. Respir. Med. 2004, 98, 1195–1202. [Google Scholar] [CrossRef] [Green Version]
- Spruit, M.A.; Singh, S.J.; Garvey, C. ATS/ERS Task Force on Pulmonary Rehabilitation. An official American Thoracic Society/European Respiratory Society statement: Key concepts and advances in pulmonary rehabilitation. Am. J. Respir. Crit. Care Med. 2013, 188, e13–e64, Erratum in Am. J. Respir. Crit. Care Med. 2014, 189, 1570. [Google Scholar] [CrossRef] [Green Version]
- Li, W.; Pu, Y.; Meng, A.; Zhi, X.; Xu, G. Effectiveness of pulmonary rehabilitation in elderly patients with COPD: A systematic review and meta-analysis of randomized controlled trials. Int. J. Nurs. Pract. 2019, 25, e12745. [Google Scholar] [CrossRef]
- Ozmen, I.; Yildirim, E.; Öztürk, M.; Yilmaz, Ö.; Salturk, C.; Aydin, R.; Usgun, N.; Yer, N. Are the gains of pulmonary rehabilitation in young and elderly patients same? Eur. Respir. J. 2016, 48, PA3581. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Osoba, D.; Wu, A.W.; Wyrwich, K.W.; Norman, G.R. Clinical Significance Consensus Meeting Group. Methods to explain the clinical significance of health status measures. Mayo Clin. Proc. 2002, 77, 71–83. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| n | 3173 |
| Diagnosis: ICD-10 J44.00–J44.99 | 3173 |
| Age (mean (SD)) | 69 (12) |
| Age, n (%) | |
| ≤60 | 679 (21) |
| 61–70 | 908 (29) |
| 71–80 | 1167 (37) |
| 81–85 | 299 (9) |
| >85 | 120 (4) |
| Female (%) | 1469 (46) |
| BMI (mean (SD)) | 25.22 (7) |
| BMI, n (%) | |
| <18.5 | 411 (13) |
| 18.5–24.9 | 1309 (42) |
| 25–29.9 | 771 (25) |
| 30–34.9 | 374 (12) |
| 35–39.9 | 145 (5) |
| 40+ | 104 (3) |
| Length of Stay, days, (mean (SD)) | 18.85 (8) |
| Length of Stay, days, n (%) | |
| <14 | 706 (23) |
| <21 | 1747 (57) |
| <28 | 454 (15) |
| ≥28 | 163 (5) |
| ≤60 Years | 61–70 Years | 71–80 Years | 81–85 Years | >85 Years | p | |
|---|---|---|---|---|---|---|
| Total number (n) | 679 | 908 | 1167 | 299 | 120 | |
| FIM increase, % (SD) | 4.94 [0.90, 11.24] | 4.44 [0.00, 10.53] | 4.55 [0.82, 11.40] | 3.88 [0.00, 8.68] | 7.41 [3.90, 15.36] | 0.106 |
| 6MWT increase, % (SD) | 36.10 [9.86, 79.71] | 40.91 [16.13, 83.87] | 43.14 [11.11, 95.29] | 44.23 [15.86, 112.50] | 57.89 [14.13, 125.66] | 0.040 |
| FT increase, % (SD) | 24.04 [0.00, 50.00] | 27.27 [0.00, 60.00] | 28.57 [8.33, 63.07] | 23.08 [0.00, 60.00] | 20.00 [0.00, 57.78] | 0.021 |
| ∆FIM (SD) | 6 (14) | 5 (13) | 4 (18) | 6 (17) | 8 (7) | 0.4 |
| ∆6MWT (SD) | 106 (134) | 110 (119) | 98 (112) | 104 (106) | 92 (101) | 0.2 |
| ∆FT (SD) | 9 (28) | 11 (27) | 13 (27) | 9 (28) | 8 (32) | 0.064 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Spielmanns, M.; Schulze, S.-T.; Guenes, E.; Pekacka-Falkowska, K.; Windisch, W.; Pekacka-Egli, A.M. Clinical Effects of Pulmonary Rehabilitation in Very Old Patients with COPD. J. Clin. Med. 2023, 12, 2513. https://doi.org/10.3390/jcm12072513
Spielmanns M, Schulze S-T, Guenes E, Pekacka-Falkowska K, Windisch W, Pekacka-Egli AM. Clinical Effects of Pulmonary Rehabilitation in Very Old Patients with COPD. Journal of Clinical Medicine. 2023; 12(7):2513. https://doi.org/10.3390/jcm12072513
Chicago/Turabian StyleSpielmanns, Marc, Sofia-Theresia Schulze, Erhan Guenes, Katarzyna Pekacka-Falkowska, Wolfram Windisch, and Anna Maria Pekacka-Egli. 2023. "Clinical Effects of Pulmonary Rehabilitation in Very Old Patients with COPD" Journal of Clinical Medicine 12, no. 7: 2513. https://doi.org/10.3390/jcm12072513