

Efficacy and Safety of Leadless Pacemakers for Atrioventricular Synchronous Pacing: A Systematic Review and Meta-Analysis
Abstract
:1. Introduction
2. Methods
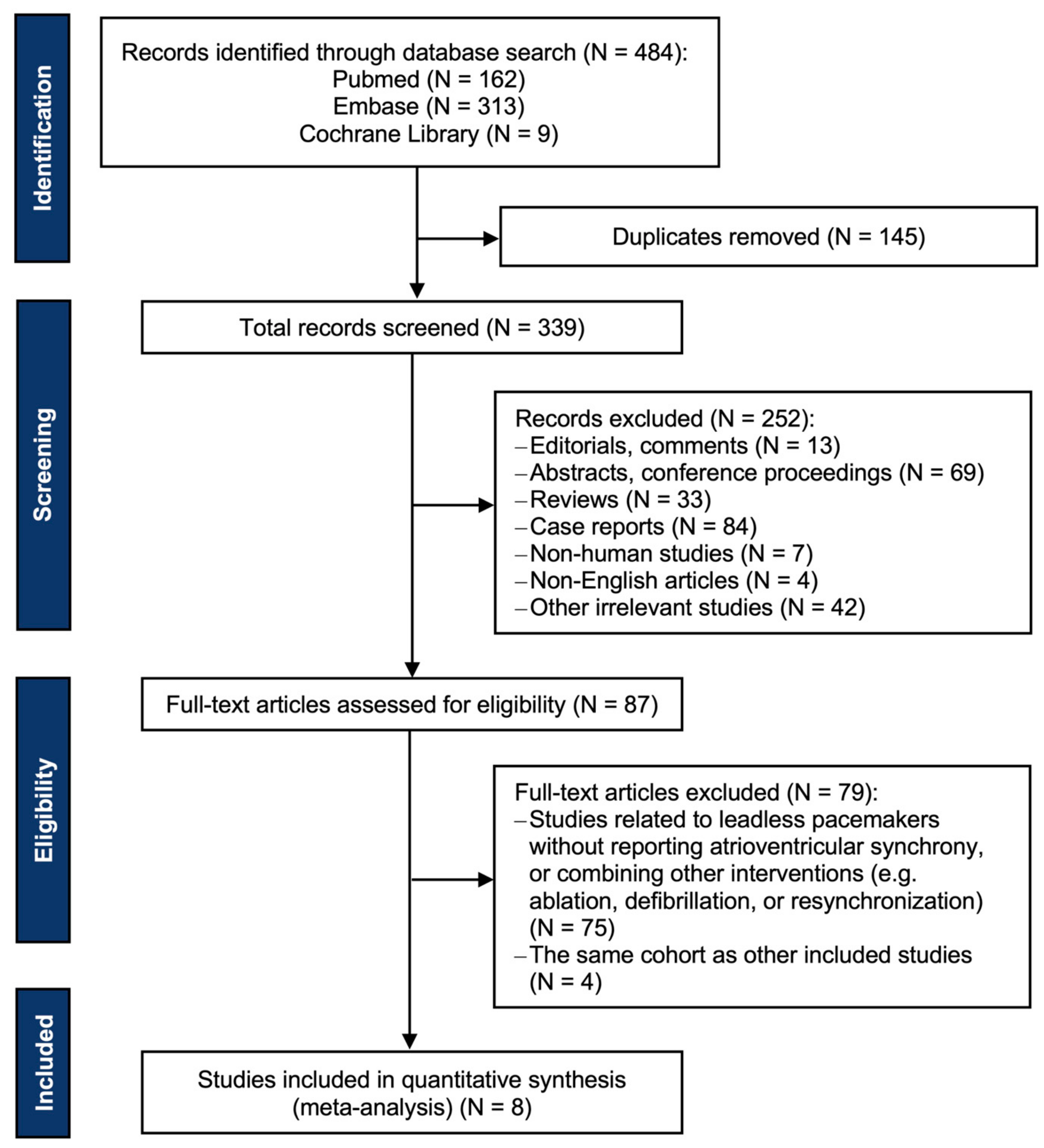
2.1. Data Sources and Searches
2.2. Inclusion and Exclusion Criteria
2.3. Outcome Measures
2.4. Data Extraction and Quality Assessments
2.5. Data Synthesis and Analysis
3. Results
3.1. Study and Patient Characteristics
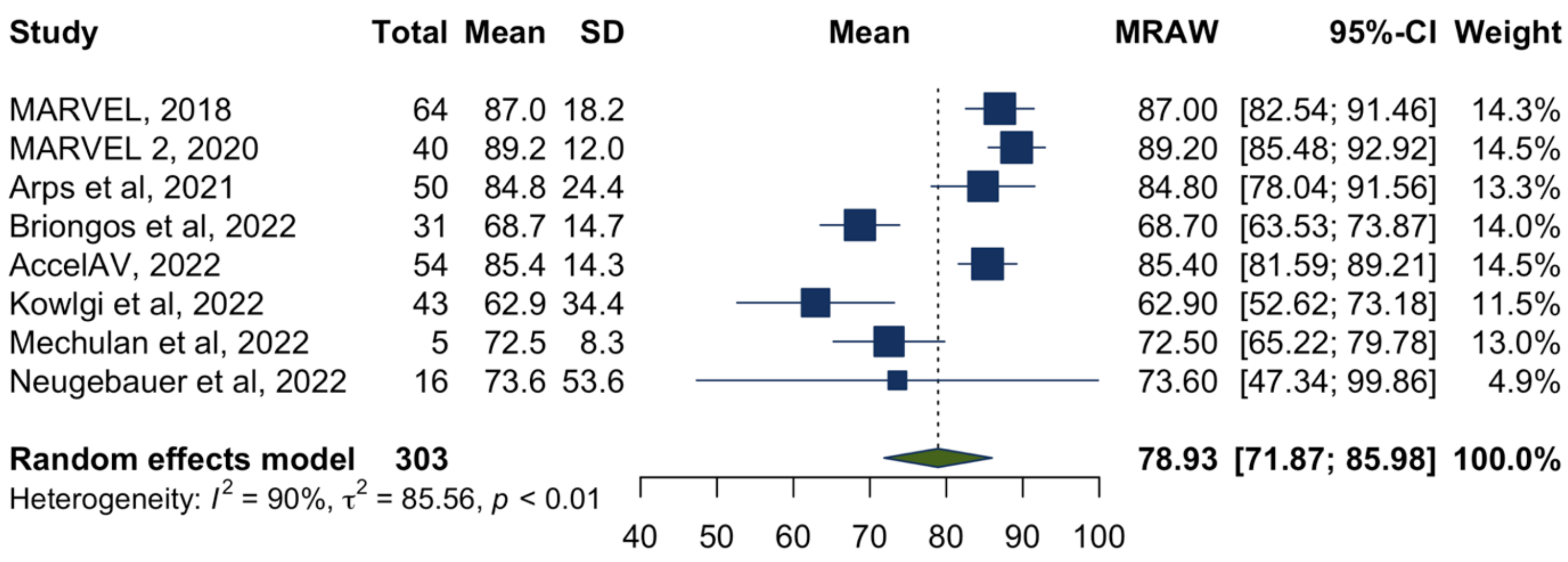
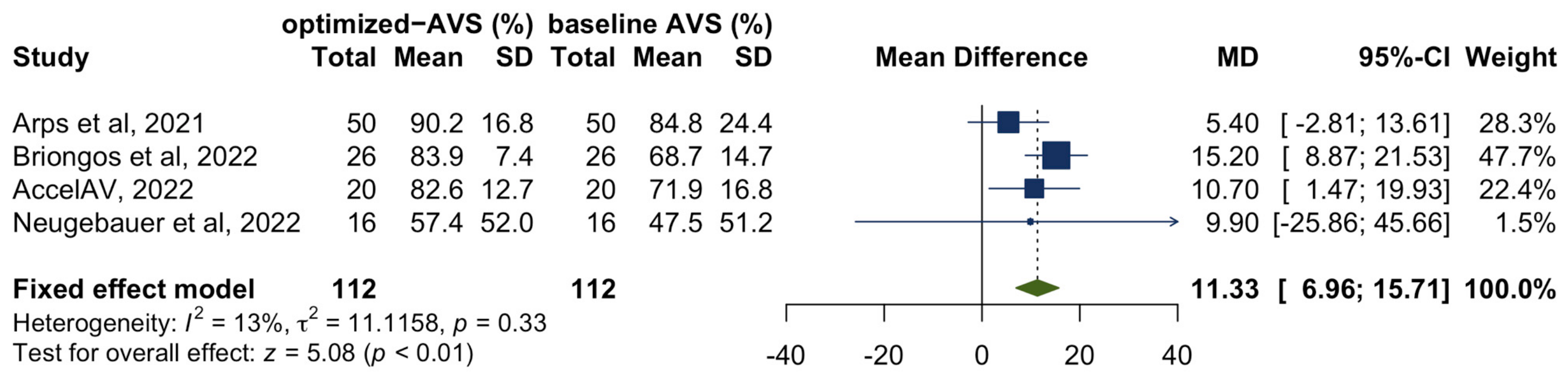
3.2. Atrioventricular Synchrony
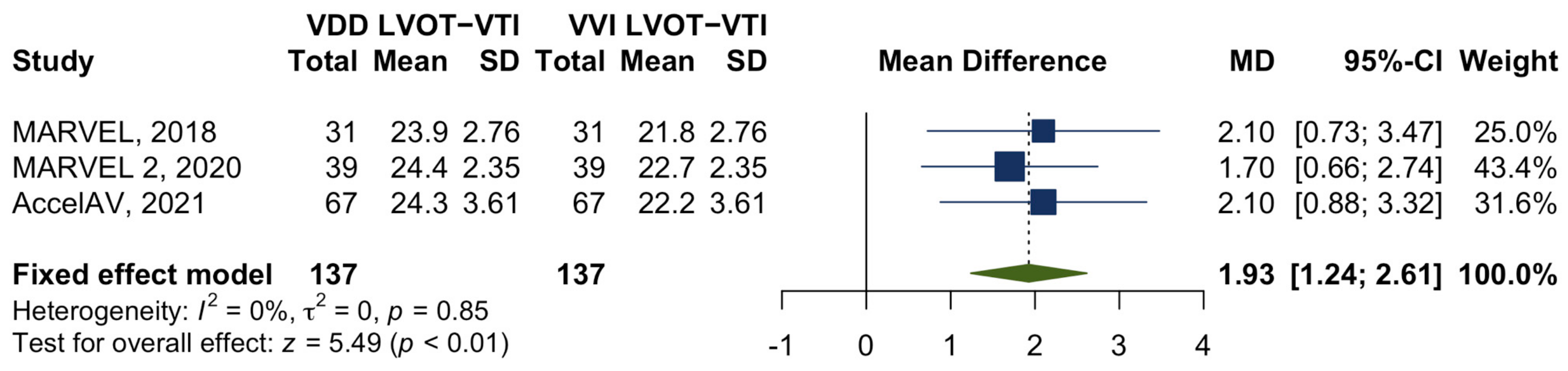
3.3. Cardiac Output
3.4. Safety of Leadless Atrioventricular Synchronous Pacing
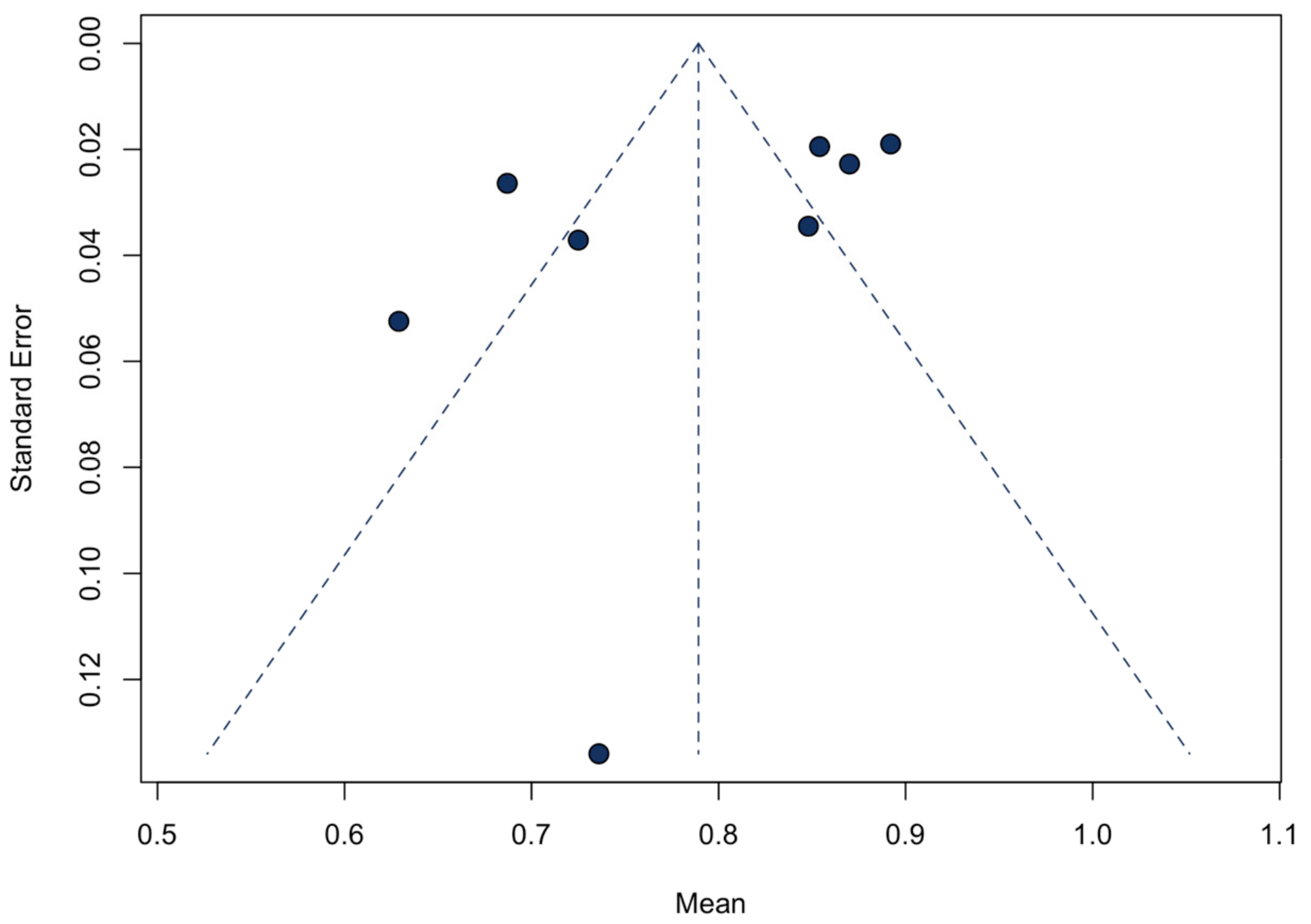
3.5. Sensitivity Analyses and Publication Bias
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hauser, R.G.; Hayes, D.L.; Kallinen, L.M.; Cannom, D.S.; Epstein, A.E.; Almquist, A.K.; Song, S.L.; Tyers, G.F.; Vlay, S.C.; Irwin, M. Clinical experience with pacemaker pulse generators and transvenous leads: An 8-year prospective multicenter study. Heart Rhythm. 2007, 4, 154–160. [Google Scholar] [CrossRef] [PubMed]
- Pakarinen, S.; Oikarinen, L.; Toivonen, L. Short-term implantation-related complications of cardiac rhythm management device therapy: A retrospective single-centre 1-year survey. Europace 2010, 12, 103–108. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, D.; Duray, G.Z.; Omar, R.; Soejima, K.; Neuzil, P.; Zhang, S.; Narasimhan, C.; Steinwender, C.; Brugada, J.; Lloyd, M.; et al. A Leadless Intracardiac Transcatheter Pacing System. N. Engl. J. Med. 2016, 374, 533–541. [Google Scholar] [CrossRef] [PubMed]
- Duray, G.Z.; Ritter, P.; El-Chami, M.; Narasimhan, C.; Omar, R.; Tolosana, J.M.; Zhang, S.; Soejima, K.; Steinwender, C.; Rapallini, L.; et al. Long-term performance of a transcatheter pacing system: 12-Month results from the Micra Transcatheter Pacing Study. Heart Rhythm. 2017, 14, 702–709. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- El-Chami, M.F.; Al-Samadi, F.; Clementy, N.; Garweg, C.; Martinez-Sande, J.L.; Piccini, J.P.; Iacopino, S.; Lloyd, M.; Viñolas Prat, X.; Jacobsen, M.D.; et al. Updated performance of the Micra transcatheter pacemaker in the real-world setting: A comparison to the investigational study and a transvenous historical control. Heart Rhythm. 2018, 15, 1800–1807. [Google Scholar] [CrossRef] [Green Version]
- Chinitz, L.; Ritter, P.; Khelae, S.K.; Iacopino, S.; Garweg, C.; Grazia-Bongiorni, M.; Neuzil, P.; Johansen, J.B.; Mont, L.; Gonzalez, E.; et al. Accelerometer-based atrioventricular synchronous pacing with a ventricular leadless pacemaker: Results from the Micra atrioventricular feasibility studies. Heart Rhythm. 2018, 15, 1363–1371. [Google Scholar] [CrossRef]
- Steinwender, C.; Khelae, S.K.; Garweg, C.; Chan, J.Y.S.; Ritter, P.; Johansen, J.B.; Sagi, V.; Epstein, L.M.; Piccini, J.P.; Pascual, M.; et al. Atrioventricular Synchronous Pacing Using a Leadless Ventricular Pacemaker: Results From the MARVEL 2 Study. JACC Clin. Electrophysiol. 2020, 6, 94–106. [Google Scholar] [CrossRef]
- Briongos-Figuero, S.; Estévez Paniagua, Á.; Hernández, A.S.; Jiménez, S.; Mariscal, E.G.; Motos, A.A.; Muñoz-Aguilera, R. Optimizing atrial sensing parameters in leadless pacemakers: Atrioventricular synchrony achievement in real world. Heart Rhythm. 2022, 19, 2011–2018. [Google Scholar] [CrossRef]
- Kowlgi, G.N.; Tseng, A.S.; Tempel, N.D.; Henrich, M.J.; Venkatachalam, K.L.; Scott, L.; Shen, W.K.; Deshmukh, A.J.; Madhavan, M.; Lee, H.C.; et al. A real-world experience of atrioventricular synchronous pacing with leadless ventricular pacemakers. J. Cardiovasc. Electrophysiol. 2022, 33, 982–993. [Google Scholar] [CrossRef]
- Neugebauer, F.; Noti, F.; van Gool, S.; Roten, L.; Baldinger, S.H.; Seiler, J.; Madaffari, A.; Servatius, H.; Ryser, A.; Tanner, H.; et al. Leadless atrioventricular synchronous pacing in an outpatient setting: Early lessons learned on factors affecting atrioventricular synchrony. Heart Rhythm. 2022, 19, 748–756. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef] [Green Version]
- National Heart, Lung, and Blood Institute. Study Quality Assessment Tools. Available online: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (accessed on 1 October 2022).
- Higgins, J.P.T.; Deeks, J.J. (Eds.) Chapter 7: Selecting studies and collecting data. In Cochrane Handbook for Systematic Reviews of Interventions, 5th ed.; The Cochrane Collaboration: London, UK, 2008; Available online: www.cochrane-handbook.org (accessed on 1 October 2022).
- Arps, K.; Piccini, J.P.; Yapejian, R.; Leguire, R.; Smith, B.; Al-Khatib, S.M.; Bahnson, T.D.; Daubert, J.P.; Hegland, D.D.; Jackson, K.P.; et al. Optimizing mechanically sensed atrial tracking in patients with atrioventricular-synchronous leadless pacemakers: A single-center experience. Heart Rhythm O2 2021, 2, 455–462. [Google Scholar] [CrossRef]
- Chinitz, L.A.; El-Chami, M.F.; Sagi, V.; Garcia, H.; Hackett, F.K.; Leal, M.; Whalen, P.; Henrikson, C.A.; Greenspon, A.J.; Sheldon, T.; et al. Ambulatory atrioventricular synchronous pacing over time using a leadless ventricular pacemaker: Primary results from the AccelAV study. Heart Rhythm. 2022, 20, 46–54. [Google Scholar] [CrossRef]
- Mechulan, A.; Prevot, S.; Peret, A.; Nait-Saidi, L.; Miliani, I.; Leong-Feng, L.; Leude-Vaillant, E.; Vaillant, A.; Cornen, A.; Latiere, B.; et al. Micra AV leadless pacemaker implantation after transcatheter aortic valve implantation. Pacing Clin. Electrophysiol. 2022, 45, 1310–1315. [Google Scholar] [CrossRef]
- Mitacchione, G.; Schiavone, M.; Gasperetti, A.; Viecca, M.; Curnis, A.; Forleo, G.B. Atrioventricular synchronous leadless pacemaker: State of art and broadened indications. Rev. Cardiovasc. Med. 2021, 22, 395–401. [Google Scholar] [CrossRef]
- Folino, A.F.; Buja, G.; Ruzza, L.; Nava, A. Long-term follow-up of patients with single lead VDD stimulation. Pacing Clin. Electrophysiol. 1994, 17, 1854–1858. [Google Scholar] [CrossRef]
- Tse, H.F.; Lau, C.P. Long-term effect of right ventricular pacing on myocardial perfusion and function. J. Am. Coll. Cardiol. 1997, 29, 744–749. [Google Scholar] [CrossRef] [Green Version]
- Sweeney, M.O.; Hellkamp, A.S.; Ellenbogen, K.A.; Greenspon, A.J.; Freedman, R.A.; Lee, K.L.; Lamas, G.A. Adverse effect of ventricular pacing on heart failure and atrial fibrillation among patients with normal baseline QRS duration in a clinical trial of pacemaker therapy for sinus node dysfunction. Circulation 2003, 107, 2932–2937. [Google Scholar] [CrossRef] [Green Version]
- Mitacchione, G.; Schiavone, M.; Gasperetti, A.; Ruggiero, D.; Denora, M.; Viecca, M.; Forleo, G.B. Micra-AV leadless pacemaker and atrioventricular (dys)synchrony: A stepwise process. Pacing Clin. Electrophysiol. 2021, 44, 1738–1742. [Google Scholar] [CrossRef] [PubMed]
- El-Chami, M.F.; Bhatia, N.K.; Merchant, F.M. Atrio-ventricular synchronous pacing with a single chamber leadless pacemaker: Programming and trouble shooting for common clinical scenarios. J. Cardiovasc. Electrophysiol. 2021, 32, 533–539. [Google Scholar] [CrossRef]
- Stack, M.F.; Rader, B.; Sobol, B.J.; Farber, S.J.; Eichna, L.W. Cardiovascular hemodynamic functions in complete heart block and the effect of isopropylnorepinephrine. Circulation 1958, 17, 526–536. [Google Scholar] [CrossRef] [Green Version]
- Udo, E.O.; Zuithoff, N.P.; van Hemel, N.M.; de Cock, C.C.; Hendriks, T.; Doevendans, P.A.; Moons, K.G. Incidence and predictors of short- and long-term complications in pacemaker therapy: The FOLLOWPACE study. Heart Rhythm. 2012, 9, 728–735. [Google Scholar] [CrossRef] [PubMed]
- Cantillon, D.J.; Exner, D.V.; Badie, N.; Davis, K.; Gu, N.Y.; Nabutovsky, Y.; Doshi, R. Complications and Health Care Costs Associated With Transvenous Cardiac Pacemakers in a Nationwide Assessment. JACC Clin. Electrophysiol. 2017, 3, 1296–1305. [Google Scholar] [CrossRef] [PubMed]
- Hauser, R.G.; Gornick, C.C.; Abdelhadi, R.H.; Tang, C.Y.; Casey, S.A.; Sengupta, J.D. Major adverse clinical events associated with implantation of a leadless intracardiac pacemaker. Heart Rhythm. 2021, 18, 1132–1139. [Google Scholar] [CrossRef]
- Mitacchione, G.; Schiavone, M.; Gasperetti, A.; Arabia, G.; Breitenstein, A.; Cerini, M.; Palmisano, P.; Montemerlo, E.; Ziacchi, M.; Gulletta, S.; et al. Outcomes of leadless pacemaker implantation following transvenous lead extraction in high-volume referral centers: Real-world data from a large international registry. Heart Rhythm. 2023, 20, 395–404. [Google Scholar] [CrossRef]
- Israel, C.W. The role of pacing mode in the development of atrial fibrillation. Europace 2006, 8, 89–95. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Year | Single/Multicenter | Design | No. of Subjects | Study Quality |
|---|---|---|---|---|---|
| MARVEL [6] | 2018 | Multicenter | Prospective observational | 70 | Good |
| MARVEL 2 [7] | 2020 | Multicenter | Prospective observational | 77 | Good |
| Arps et al. [14] | 2021 | Single-center | Retrospective observational | 50 | Fair |
| Briongos et al. [8] | 2022 | Single-center | Prospective observational | 32 | Good |
| AccelAV [15] | 2022 | Multicenter | Prospective observational | 152 | Good |
| Kowlgi et al. [9] | 2022 | Single-center | Retrospective observational | 43 | Fair |
| Mechulan et al. [16] | 2022 | Single-center | Prospective observational | 20 | Fair |
| Neugebauer et al. [10] | 2022 | Single-center | Prospective observational | 20 | Good |
| Study | a Age (y) | Female (%) | b VP% | a Estimated Atrioventricular Synchrony, % | a Estimated LVOT-VTI (cm) | Complications | |
|---|---|---|---|---|---|---|---|
| VVI Mode | VDD Mode | ||||||
| MARVEL [6] | 71.3 ± 15.1 | 24(34.3) | NA | 87.0 ± 18.2 | 21.8 ± 2.76 | 23.9 ± 2.76 | None |
| MARVEL 2 [7] | 77.6 ± 11.8 | 31(40.3) | NA | 89.2 ± 12.0 | 22.7 ± 2.35 | 24.4 ± 2.35 | None |
| Arps et al. [14] | 69.0 ± 16.8 | 24(48.0) | 10% (0, 92%) | 84.8 ± 24.4 | NA | NA | |
| Briongos et al. [8] | 78.0 ± 15.1 | 14(43.8) | NA | 68.7 ± 14.7 | NA | None | |
| AccelAV [15] | 77.2 ± 10.8 | 73(48.0) | c 100% (99.7%, 100%) | 85.4 ± 14.3 | 22.2 ± 3.61 | 24.3 ± 3.61 | 4 pericardial effusions, 4 cardiac rhythm disorder, 1 elevated threshold, 5 others |
| Kowlgi et al. [9] | 76.4 ± 10.0 | 21(48.8) | AsVP ≥ 70%: 45.8 ± 46%; AsVP < 70%: 73.4 ± 34.6% | 62.9 ± 34.4 | NA | 1 dislodgement | |
| Mechulan et al. [16] | 81.2 ± 6.8 | 5(25.0) | 46.6 ± 40.1% | 72.5 ± 8.3 | NA | 2 atrial under-sensing | |
| Neugebauer et al. [10] | 80.0 ± 8.0 | 11(55.0) | NA | 73.6 ± 53.6 | NA | 4 atrial fibrillation, 1 death | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, S.; Jin, Y.; Lu, W.; Chen, Z.; Dai, Y.; Chen, K. Efficacy and Safety of Leadless Pacemakers for Atrioventricular Synchronous Pacing: A Systematic Review and Meta-Analysis. J. Clin. Med. 2023, 12, 2512. https://doi.org/10.3390/jcm12072512
Wu S, Jin Y, Lu W, Chen Z, Dai Y, Chen K. Efficacy and Safety of Leadless Pacemakers for Atrioventricular Synchronous Pacing: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2023; 12(7):2512. https://doi.org/10.3390/jcm12072512
Chicago/Turabian StyleWu, Sijin, Yuanhao Jin, Wenzhao Lu, Zhongli Chen, Yan Dai, and Keping Chen. 2023. "Efficacy and Safety of Leadless Pacemakers for Atrioventricular Synchronous Pacing: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 12, no. 7: 2512. https://doi.org/10.3390/jcm12072512