
Use of Long-Acting Injectable Antipsychotics in a Clinical Sample of Community-Dwelling Patients with Schizophrenia-Spectrum Disorders in Rural Greece

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. The Treatment Setting
2.2. Patient Sample
2.3. Statistical Analysis
3. Results
4. Discussion
Limitations and Strengths
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Peritogiannis, V.; Gogou, A.; Samakouri, M. Very long-term outcome of psychotic disorders. Int. J. Soc. Psychiatry 2020, 66, 633–641. [Google Scholar] [CrossRef]
- GBD 2017 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1789–1858. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schneider-Thoma, J.; Chalkou, K.; Dörries, C.; Bighelli, I.; Ceraso, A.; Huhn, M.; Siafis, S.; Davis, J.M.; Cipriani, A.; Furukawa, T.A.; et al. Comparative efficacy and tolerability of 32 oral and long-acting injectable antipsychotics for the maintenance treatment of adults with schizophrenia: A systematic review and network meta-analysis. Lancet 2022, 399, 824–836. [Google Scholar] [CrossRef] [PubMed]
- Katona, L.; Bitter, I.; Czobor, P. A meta-analysis of effectiveness of real-world studies of antipsychotics in schizophrenia: Are the results consistent with the findings of randomized controlled trials? Transl. Psychiatry 2021, 11, 510. [Google Scholar] [CrossRef] [PubMed]
- Correll, C.U.; Rubio, J.M.; Kane, J.M. What is the risk-benefit ratio of long-term antipsychotic treatment in people with schizophrenia? World Psychiatry 2018, 17, 149–160. [Google Scholar] [CrossRef] [Green Version]
- Correll, C.U.; Martin, A.; Patel, C.; Benson, C.; Goulding, R.; Kern-Sliwa, J.; Joshi, K.; Schiller, E.; Kim, E. Systematic literature review of schizophrenia clinical practice guidelines on acute and maintenance management with antipsychotics. Schizophrenia 2022, 8, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Wagner, E.; Siafis, S.; Fernando, P.; Falkai, P.; Honer, W.G.; Röh, A.; Siskind, D.; Leucht, S.; Hasan, A. Efficacy and safety of clozapine in psychotic disorders—A systematic quantitative meta-review. Transl. Psychiatry 2021, 11, 1–18. [Google Scholar] [CrossRef]
- Kreyenbuhl, J.; Nossel, I.R.; Dixon, L.B. Disengagement From Mental Health Treatment Among Individuals With Schizophrenia and Strategies for Facilitating Connections to Care: A Review of the Literature. Schizophr. Bull. 2009, 35, 696–703. [Google Scholar] [CrossRef]
- Yaegashi, H.; Kirino, S.; Remington, G.; Misawa, F.; Takeuchi, H. Adherence to Oral Antipsychotics Measured by Electronic Adherence Monitoring in Schizophrenia: A Systematic Review and Meta-analysis. CNS Drugs 2020, 34, 579–598. [Google Scholar] [CrossRef]
- Cho, S.J.; Kim, J.; Lee, J.Y.; Sohn, J.H. Adherence to Antipsychotic Drugs by Medication Possession Ratio for Schizophrenia and Similar Psychotic Disorders in the Republic of Korea: A Retrospective Cohort Study. Clin. Psychopharmacol. Neurosci. 2022, 20, 491–497. [Google Scholar] [CrossRef]
- Kane, J.M.; Kishimoto, T.; Correll, C.U. Non-adherence to medication in patients with psychotic disorders: Epidemiology, contributing factors and management strategies. World Psychiatry 2013, 12, 216–226. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lieslehto, J.; Tiihonen, J.; Lähteenvuo, M.; Tanskanen, A.; Taipale, H. Primary Nonadherence to Antipsychotic Treatment Among Persons with Schizophrenia. Schizophr. Bull. 2022, 48, 655–663. [Google Scholar] [CrossRef] [PubMed]
- Haddad, P.M.; Brain, C.; Scott, J. Nonadherence with antipsychotic medication in schizophrenia: Challenges and management strategies. Patient Relat. Outcome Meas. 2014, 5, 43–62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higashi, K.; Medic, G.; Littlewood, K.; Diez, T.; Granström, O.; De Hert, M. Medication adherence in schizophrenia: Factors influencing adherence and consequences of nonadherence, a systematic literature review. Ther. Adv. Psychopharmacol. 2013, 3, 200–218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abdellati, K.E.; De Picker, L.; Morrens, M. Antipsychotic Treatment Failure: A Systematic Review on Risk Factors and Interventions for Treatment Adherence in Psychosis. Front. Neurosci. 2020, 14, 531763. [Google Scholar] [CrossRef] [PubMed]
- Ostuzzi, G.; Bertolini, F.; Del Giovane, C.; Tedeschi, F.; Bovo, C.; Gastaldon, C.; Nosé, M.; Ogheri, F.; Papola, D.; Purgato, M.; et al. Maintenance Treatment With Long-Acting Injectable Antipsychotics for People With Nonaffective Psychoses: A Network Meta-Analysis. Am. J. Psychiatry 2021, 178, 424–436. [Google Scholar] [CrossRef]
- Kishimoto, T.; Hagi, K.; Kurokawa, S.; Kane, J.M.; Correll, C.U. Long-acting injectable versus oral antipsychotics for the maintenance treatment of schizophrenia: A systematic review and comparative meta-analysis of randomised, cohort, and pre–post studies. Lancet Psychiatry 2021, 8, 387–404. [Google Scholar] [CrossRef]
- Zhornitsky, S.; Stip, E. Oral versus Long-Acting Injectable Antipsychotics in the Treatment of Schizophrenia and Special Popula-tions at Risk for Treatment Nonadherence: A Systematic Review. Schizophr. Res. Treat. 2012, 2012, 407171. [Google Scholar]
- Bossie, C.A.; Alphs, L.D.; Correll, C.U. Long-acting injectable versus daily oral antipsychotic treatment trials in schizophrenia: Pragmatic versus explanatory study designs. Int. Clin. Psychopharmacol. 2015, 30, 272. [Google Scholar] [CrossRef] [Green Version]
- Taipale, H.; Mittendorfer-Rutz, E.; Alexanderson, K.; Majak, M.; Mehtälä, J.; Hoti, F.; Jedenius, E.; Enkusson, D.; Leval, A.; Sermon, J.; et al. Antipsychotics and mortality in a nationwide cohort of 29,823 patients with schizophrenia. Schizophr. Res. 2018, 197, 274–280. [Google Scholar] [CrossRef]
- Huang, C.-Y.; Fang, S.-C.; Shao, Y.-H.J. Comparison of Long-Acting Injectable Antipsychotics With Oral Antipsychotics and Suicide and All-Cause Mortality in Patients With Newly Diagnosed Schizophrenia. JAMA Netw. Open 2021, 4, e218810. [Google Scholar] [CrossRef]
- Peralta, V.; Cuesta, M.J. Delusional disorder and schizophrenia: A comparative study across multiple domains. Psychol. Med. 2016, 46, 2829–2839. [Google Scholar] [CrossRef]
- González-Rodríguez, A.; Seeman, M.V. Differences between delusional disorder and schizophrenia: A mini narrative review. World J. Psychiatry 2022, 12, 683–692. [Google Scholar] [CrossRef]
- González-Rodríguez, A.; Seeman, M.V.; Díaz-Pons, A.; Ayesa-Arriola, R.; Natividad, M.; Calvo, E.; Monreal, J.A. Do Sex/Gender and Menopause Influence the Psychopathology and Comorbidity Observed in Delusional Disorders? J. Clin. Med. 2022, 11, 4550. [Google Scholar] [CrossRef] [PubMed]
- Lähteenvuo, M.; Taipale, H.; Tanskanen, A.; Mittendorfer-Rutz, E.; Tiihonen, J. Effectiveness of pharmacotherapies for delusional disorder in a Swedish national cohort of 9076 patients. Schizophr. Res. 2021, 228, 367–372. [Google Scholar] [CrossRef] [PubMed]
- Verdoux, H.; Pambrun, E.; Tournier, M.; Bezin, J.; Pariente, A. Antipsychotic long-acting injections: A community-based study from 2007 to 2014 of prescribing trends and characteristics associated with initiation. Schizophr. Res. 2016, 178, 58–63. [Google Scholar] [CrossRef]
- Gallego, J.A.; Bonetti, J.; Zhang, J.; Kane, J.M.; Correll, C.U. Prevalence and correlates of antipsychotic polypharmacy: A systematic review and meta-regression of global and regional trends from the 1970s to 2009. Schizophr. Res. 2012, 138, 18–28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berardi, L.; Antonazzo, I.C.; Piccinni, C.; Raschi, E.; Forcesi, E.; Fioritti, A.; Berardi, D.; De Ponti, F.; Piazza, A.; Poluzzi, E. Long-acting in-jectable antipsychotics: Six-month follow-up of new outpatient treatments in Bologna Community Mental Health Centres. PLoS ONE 2019, 14, e0211938. [Google Scholar] [CrossRef] [PubMed]
- Arango, C.; Baeza, I.; Bernardo, M.; Cañas, F.; de Dios, C.; Díaz-Marsá, M.; García-Portilla, M.P.; Gutiérrez-Rojas, L.; Olivares, J.M.; Ri-co-Villademoros, F.; et al. Long-acting injectable antipsychotics for the treatment of schizophrenia in Spain. Rev. Psiquiatr. Salud Ment. 2019, 12, 92–105. [Google Scholar] [CrossRef]
- Reymann, S.; Schoretsanitis, G.; Egger, S.T.; Mohonko, A.; Kirschner, M.; Vetter, S.; Homan, P.; Seifritz, E.; Burrer, A. Use of Long-Acting Injectable Antipsychotics in Inpatients with Schizophrenia Spectrum Disorder in an Academic Psychiatric Hospital in Switzerland. J. Pers. Med. 2022, 12, 441. [Google Scholar] [CrossRef]
- Camacho, A.; Ng, B.; Galangue, B.; Feifel, D. Use of risperidone long-acting injectable in a rural border community clinic in southern california. Psychiatry 2008, 5, 43–49. [Google Scholar] [PubMed]
- Padmavati, R.; Raghavan, V.; Cherubal, A.G.; John, S. Comparison of cost-effectiveness of long-acting depot injection antipsychotics and oral antipsychotics in patients with schizophrenia in a rural community in South India. Indian J. Psychiatry 2020, 62, 747–748. [Google Scholar] [CrossRef]
- Peritogiannis, V.; Mavreas, V. Community mental health teams in Greece: The paradigm of mobile mental health units. Arch. Hell. Med. 2014, 31, 71–76. [Google Scholar]
- Peritogiannis, V.; Fragouli-Sakellaropoulou, A.; Stavrogiannopoulos, M.; Filla, I.; Garmpi, A.; Pantelidou, S.; Samakouri, M.; Coordinating Committee of the Mobile Mental Health Units. The role of the Mobile Mental Health Units in mental healthcare delivery in rural areas in Greece: Current challenges and prospects. Psychiatriki 2022, 33, 301. [Google Scholar] [CrossRef]
- Samakouri, M.; Evagorou, O.; Frangouli-Sakellaropoulou, A. The Contribution of Mobile Mental Health Units to Community Psychiatric Care in Greece. Psych 2022, 4, 100–104. [Google Scholar] [CrossRef]
- Peritogiannis, V.; Mantas, C.; Alexiou, D.; Fotopoulou, V.; Mouka, V.; Hyphantis, T. The contribution of a mobile mental health unit to the promotion of primary mental health in rural areas in Greece: A 2-year follow-up. Eur. Psychiatry 2011, 26, 425–427. [Google Scholar] [CrossRef] [PubMed]
- Peritogiannis, V.; Manthopoulou, T.; Gogou, A.; Mavreas, V. Mental Healthcare Delivery in Rural Greece: A 10-year Account of a Mobile Mental Health Unit. J. Neurosci. Rural Pract. 2017, 8, 556–561. [Google Scholar] [CrossRef] [Green Version]
- Peritogiannis, V.; Tsoli, F. The Greek Hybrid Version of the Assertive Community Treatment Model: A Perspective View between Challenges and Limitations. Psych 2021, 3, 792–799. [Google Scholar] [CrossRef]
- Haro, J.M.; Edgell, E.T.; Frewer, P.; Alonso, J.; Jones, P.B.; on behalf of the SOHO Study Group. The European Schizophrenia Outpatient Health Outcomes Study: Baseline findings across country and treatment. Acta Psychiatr. Scand. 2003, 107, 7–15. [Google Scholar] [CrossRef]
- Papageorgiou, G.; Canas, F.; Zink, M.; Rossi, A. Country differences in patient characteristics and treatment in schizophrenia: Data from a physician-based survey in Europe. Eur. Psychiatry 2011, 26, 17–28. [Google Scholar] [CrossRef]
- Peritogiannis, V.; Mantas, C.; Tatsioni, A.; Mavreas, V. Rates of First Episode of Psychosis in a Defined Catchment Area in Greece. Clin. Pract. Epidemiol. Ment. Health 2013, 9, 251–254. [Google Scholar] [CrossRef] [Green Version]
- Wei, Y.; Li, W.; Zhang, L.; Zhu, J.-H.; Zhu, X.-J.; Ma, X.-Y.; Dong, Q.-L.; Zhao, W.-L.; Pan, W.-M.; Jiang, X.; et al. Unmedicated patients with schizophrenia in economically underdeveloped areas of China. Asian J. Psychiatry 2020, 47, 101865. [Google Scholar] [CrossRef]
- Peritogiannis, V.; Samakouri, M. Research on psychotic disorders in rural areas: Recent advances and ongoing challenges. Int. J. Soc. Psychiatry 2021, 67, 1046–1057. [Google Scholar] [CrossRef]
- Kane, J.M.; McEvoy, J.P.; Correll, C.U.; Llorca, P.-M. Controversies Surrounding the Use of Long-Acting Injectable Antipsychotic Medications for the Treatment of Patients with Schizophrenia. CNS Drugs 2021, 35, 1189–1205. [Google Scholar] [CrossRef]
- Garbi, A.; Tiniakos, I.; Mikelatou, Z.; Drakatos, I. Decrease of Hospitalizations and Length of Hospital Stay in Patients with Schiz-ophrenia Spectrum Disorders or Bipolar Disorder Treated in a Mobile Mental Health Service in Insular Greece. Psych 2021, 3, 780–791. [Google Scholar] [CrossRef]
- Peritogiannis, V.; Gioti, P.; Gogou, A.; Samakouri, M. Decrease of hospitalizations and length of hospital stay in patients with schizophrenia spectrum disorders treated in a community mental health service in rural Greece. Int. J. Soc. Psychiatry 2020, 66, 693–699. [Google Scholar] [CrossRef] [PubMed]
- Howard, L.M.; Trevillion, K.; Khalifeh, H.; Woodall, A.; Agnew-Davies, R.; Feder, G. Domestic violence and severe psychiatric disorders: Prevalence and interventions. Psychol. Med. 2010, 40, 881–893. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.H.; Phillips, M.R.; Li, X.; Yu, G.; Zhang, J.; Shi, Q.; Song, Z.; Ding, Z.; Pang, S.; Susser, E. Marriage outcome and relationship with urban versus rural context for individuals with psychosis in a population-based study in China. Soc. Psychiatry Psychiatr. Epidemiol. 2015, 50, 1501–1509. [Google Scholar] [CrossRef] [Green Version]
- Bakola, M.; Peritogiannis, V.; Stuckler, D.; Kitsou, K.S.; Gourzis, P.; Hyphantis, T.; Jelastopulu, E. Who is coercively admitted to psychiatric wards? Epidemiological analysis of inpatient records of involuntary psychiatric admissions to a University General Hospital in Greece for the years 2008–2017. Int. J. Soc. Psychiatry 2023, 69, 267–276. [Google Scholar] [CrossRef]
- Bilanakis, N.; Kalampokis, G.; Christou, K.; Peritogiannis, V. Use of Coercive Physical Measures in a Psychiatric Ward of a General Hospital in Greece. Int. J. Soc. Psychiatry 2010, 56, 402–411. [Google Scholar] [CrossRef] [PubMed]
- Veyej, N.; Moosa, M.Y. Prescribing patterns of long-acting injectable antipsychotics in a community setting in South Africa. S. Afr. J. Psychiatry 2022, 28, 9. [Google Scholar] [CrossRef]
- Peritogiannis, V.; Manthopoulou, T.; Mavreas, V. Long-term Benzodiazepine Treatment in Patients with Psychotic Disorders Attending a Mental Health Service in Rural Greece. J. Neurosci. Rural Pract. 2016, 7, S026–S030. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bilanakis, N.; Vratsista, A.; Kalampokis, G.; Papamichael, G.; Peritogiannis, V. The Greek version of the MacArthur competence assessment tool for treatment: Reliability and validity. Evaluation of capacity for treatment decisions in Greek psychiatric patients. Ann. Gen. Psychiatry 2013, 12, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bilanakis, N.; Peritogiannis, V.; Vratsista, A. Treatment decision-making capacity in hospitalized patients with schizophrenia. Psychiatriki 2017, 28, 37–45. [Google Scholar] [CrossRef] [PubMed]
- Nystazaki, M.; Pikouli, K.; Tsapakis, E.; Karanikola, M.; Ploumpidis, D.; Alevizopoulos, G. Decision-making Capacity for Treatment of Psychotic Patients on Long Acting Injectable Antipsychotic Treatment. Arch. Psychiatr. Nurs. 2018, 32, 300–304. [Google Scholar] [CrossRef]
- González-Rodríguez, A.; Monreal, J.A.; Natividad, M.; Seeman, M.V. Seventy Years of Treating Delusional Disorder with An-tipsychotics: A Historical Perspective. Biomedicines 2022, 10, 3281. [Google Scholar] [CrossRef]
- Miron, A.A.; Ifteni, P.I.; Teodorescu, A.; Petric, P.S. Long-Acting Injectable Antipsychotics (LAIs) Prescribing Trends during the COVID-19 Pandemic in Romania. Healthcare 2022, 10, 1265. [Google Scholar] [CrossRef]
- Zhdanava, M.; Starr, H.L.; Totev, T.I.; Lefebvre, P.; Shah, A.; Sheng, K.; Pilon, D. Impact of COVID-19 Pandemic on Prescribing of Long-Acting Injectable Antipsychotics for Schizophrenia: Results from a United States Prescriber Survey. Neuropsychiatr. Dis. Treat. 2022, 18, 2003–2019. [Google Scholar] [CrossRef] [PubMed]
- Barlati, S.; Nibbio, G.; Bianchi, F.; Gigli, E.B.L.; Calzavara-Pinton, I.; Cerati, C.; Fiori, J.; Lisoni, J.; Deste, G.; Vita, A. Long-acting Injectable Antipsychotics during the COVID-19 pandemic in schizophrenia: An observational study in a real-world clinical setting. Psychiatry Res. 2022, 317, 114878. [Google Scholar] [CrossRef]
- McKee, K.A.; Crocker, C.E.; Tibbo, P.G. Long-acting injectable antipsychotic (LAI) prescribing trends during COVID-19 restrictions in Canada: A retrospective observational study. BMC Psychiatry 2021, 21, 633. [Google Scholar] [CrossRef]
- Alevizopoulos, G.; Nystazaki, M. Long Acting Injectable Antipsychotics: Ongoing use during the COVID-19 pandemic and suc-cessful use of internet-based support in Greece. Eur. J. Psychiatry 2021, 35, 204–205. [Google Scholar] [CrossRef]
- Peritogiannis, V.; Tatsioni, A.; Menti, N.; Grammeniati, A.; Fotopoulou, V.; Mavreas, V. Treatment Engagement of Psychotic Patients with a Mobile Mental Health Unit in Rural Areas in Greece: A Five-Year Study. Schizophr. Res. Treat. 2013, 2013, 1–6. [Google Scholar] [CrossRef]
- Peritogiannis, V.; Rousoudi, S.; Vorvolakos, T.; Gioti, P.; Gogou, A.; Arre, A.; Samakouri, M. A comparative study of two Mobile Mental Health Units in different catchment rural areas in Greece. Int. J. Soc. Psychiatry 2022, 68, 324–333. [Google Scholar] [CrossRef] [PubMed]
- Peritogiannis, V.; Grammeniati, A.; Gogou, A.; Gioti, P.; Mavreas, V. Very Long-Term Outcome of Community-Dwelling Patients With Schizophrenia Spectrum Disorders in Rural Greece. J. Nerv. Ment. Dis. 2019, 207, 1012–1018. [Google Scholar] [CrossRef] [PubMed]
- Peritogiannis, V.; Nikolaou, P. Functioning in community-dwelling patients with schizophrenia spectrum disorders in rural Greece. Int. J. Soc. Psychiatry 2020, 66, 111–117. [Google Scholar] [CrossRef]
- Peritogiannis, V.; Gioti, P. The scope of the interventions of an interdisciplinary mental health service in the treatment of psychotic disorders in rural Greece. Dialogues Clin. Neurosci. Ment. Health 2021, 4, 225–231. [Google Scholar]


{kind=link}
| Age (years, mean ± SD) | 54.4 ± 12.1 | ||
| Illness duration (years, mean ± SD) | 28.0 ± 14.4 | ||
| Hospitalizations (mean ± SD) | 3.4 ± 4.5 | ||
| Follow-up duration (years, mean ± SD) | 7.0 ± 4.9 | ||
| n | % | ||
| Antipsychotic medication | Oral | 61 | 70.1 |
| LAI | 26 | 29.9 | |
| Biological sex | Female | 28 | 32.2 |
| Male | 59 | 67.8 | |
| Treatment regimen | Monotherapy | 63 | 72.4 |
| Combination | 24 | 27.6 | |
| History of alcohol/substance abuse | No | 61 | 70.1 |
| Yes | 26 | 29.9 | |
| Carer | No | 19 | 21.8 |
| Yes | 54 | 62.1 | |
| Family with other patients with SMI | 14 | 16.1 | |
| Benzodiazepines | No | 58 | 66.7 |
| Yes | 29 | 33.3 | |
| Antidepressants | No | 65 | 74.7 |
| Yes | 22 | 25.3 | |
| Generic Drug Name | Oral Treatment | LAI Formulation |
|---|---|---|
| Olanzapine | 20 | 5 |
| Risperidone | 16 | 2 |
| Paliperidone | 1 | 13 |
| Aripiprazole | 12 | - |
| Quetiapine | 12 | NA |
| Amisulpride | 8 | NA |
| Asenapine | 1 | NA |
| Haloperidol | 6 | 4 |
| Chlorpromazine | 1 | NA |
| Zuclopenthixol | - | 2 |
| Trifluoperazine | 1 | NA |
| Clozapine | 7 | NA |
| Patients on Oral Antipsychotics (n = 61) | Patients on LAI (n = 26) | Statistical Test | p | |
|---|---|---|---|---|
| Age (years, mean, SD) | 54.3 (12.9) | 54.6 (10.4) | t(85) = −0.112 | NSS |
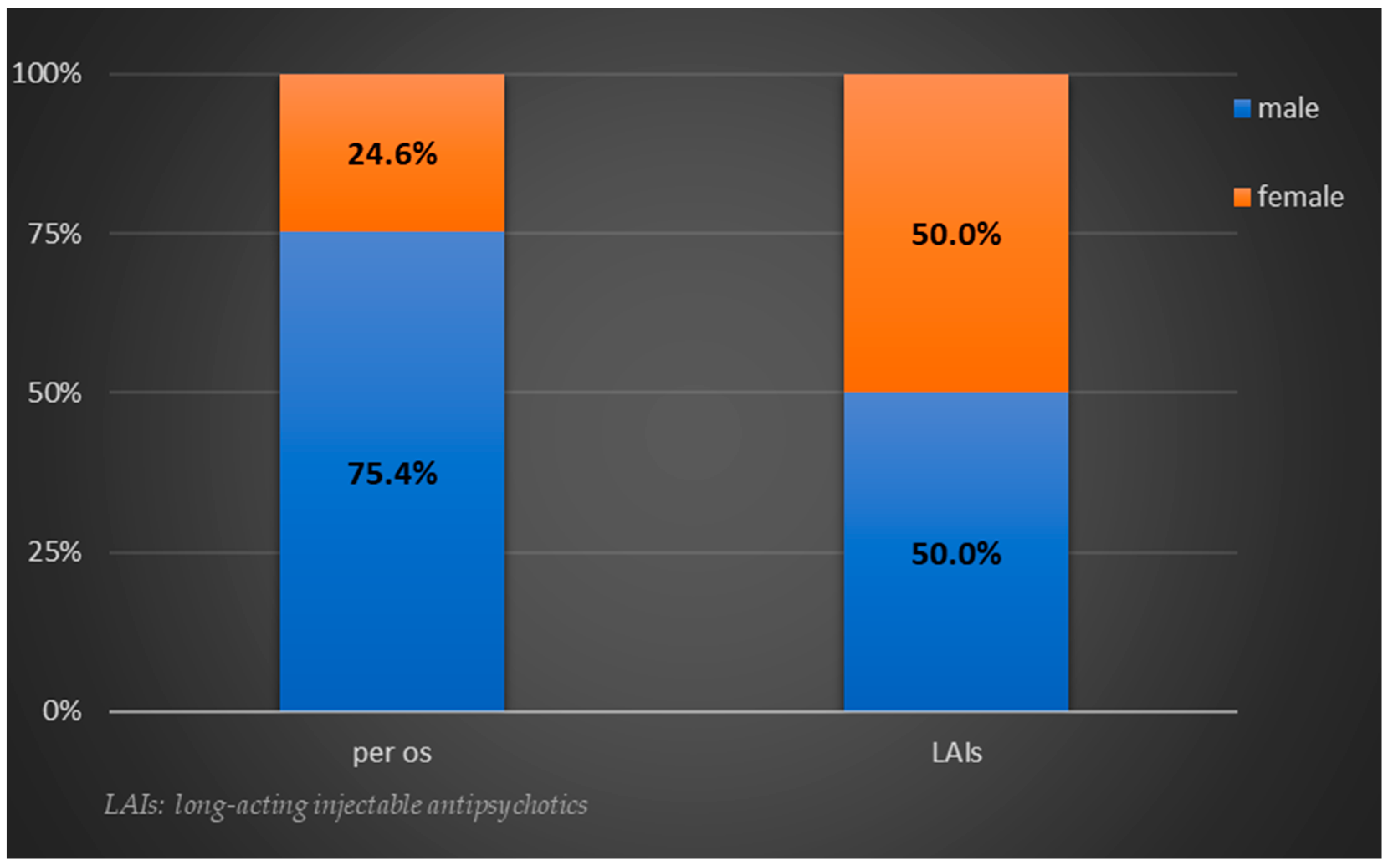
| Biological sex (male/female) | 46/15 | 13/13 | χ2(1) = 5.393 | 0.02 |
| Illness duration (years, mean, SD) | 27.6 (15) | 28.8 (13.8) | t(85) = −0.338 | NSS |
| Hospitalizations (mean, SD) | 3.7 (5.2) | 2.7 (2.2) | t(85) = 0.975 | NSS |
| History of alcohol/substance abuse | 17 | 9 | χ2(1) = 0.396 | NSS |
| Follow-up duration (years, mean, SD) | 7.1 (4.7) | 6.8 (5.5) | t(85) = 0.260, | NSS |
| Monotherapy vs. antipsychotic combination | 46 vs. 15 | 17 vs. 9 | χ2(1) = 0.917 | NSS |
| Concomitant benzodiazepine | 24 | 5 | χ2(1) = 3.319 | NSS |
| Concomitant antidepressant | 19 | 3 | χ2(1) = 3.710 | NSS |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Peritogiannis, V.; Tsoli, F.; Gioti, P.; Bakola, M.; Jelastopulu, E. Use of Long-Acting Injectable Antipsychotics in a Clinical Sample of Community-Dwelling Patients with Schizophrenia-Spectrum Disorders in Rural Greece. J. Clin. Med. 2023, 12, 2508. https://doi.org/10.3390/jcm12072508
Peritogiannis V, Tsoli F, Gioti P, Bakola M, Jelastopulu E. Use of Long-Acting Injectable Antipsychotics in a Clinical Sample of Community-Dwelling Patients with Schizophrenia-Spectrum Disorders in Rural Greece. Journal of Clinical Medicine. 2023; 12(7):2508. https://doi.org/10.3390/jcm12072508
Chicago/Turabian StylePeritogiannis, Vaios, Fotini Tsoli, Panagiota Gioti, Maria Bakola, and Eleni Jelastopulu. 2023. "Use of Long-Acting Injectable Antipsychotics in a Clinical Sample of Community-Dwelling Patients with Schizophrenia-Spectrum Disorders in Rural Greece" Journal of Clinical Medicine 12, no. 7: 2508. https://doi.org/10.3390/jcm12072508