Outcome of Conservative Therapy of Adolescent Idiopathic Scoliosis (AIS) with Chêneau-Brace

 , ,
, ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
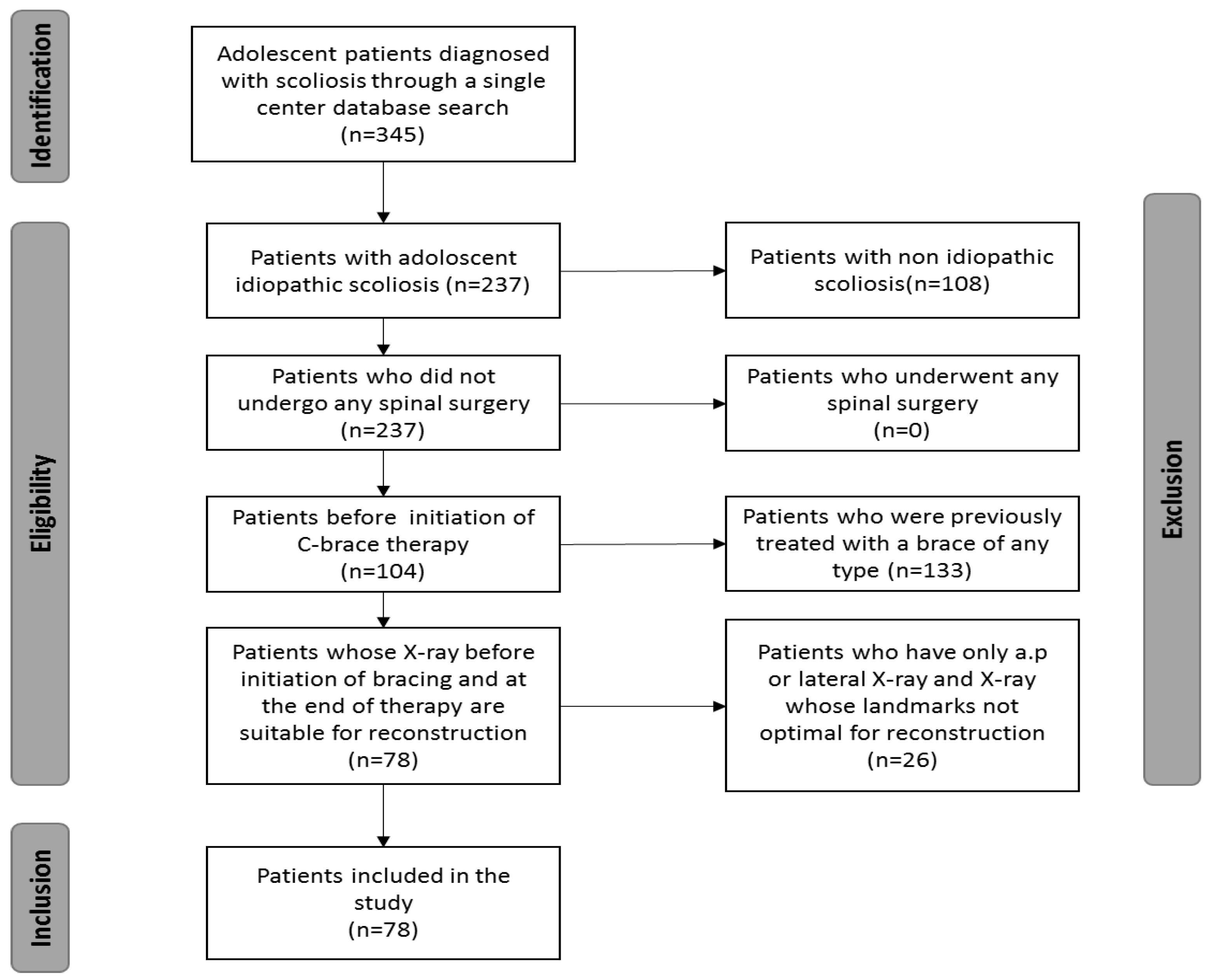
2.1. Study Cohort
2.2. Data Collection and Analysis
2.3. Patient Stratification for Sub-Group Analysis
2.4. Statistical Analysis
3. Results
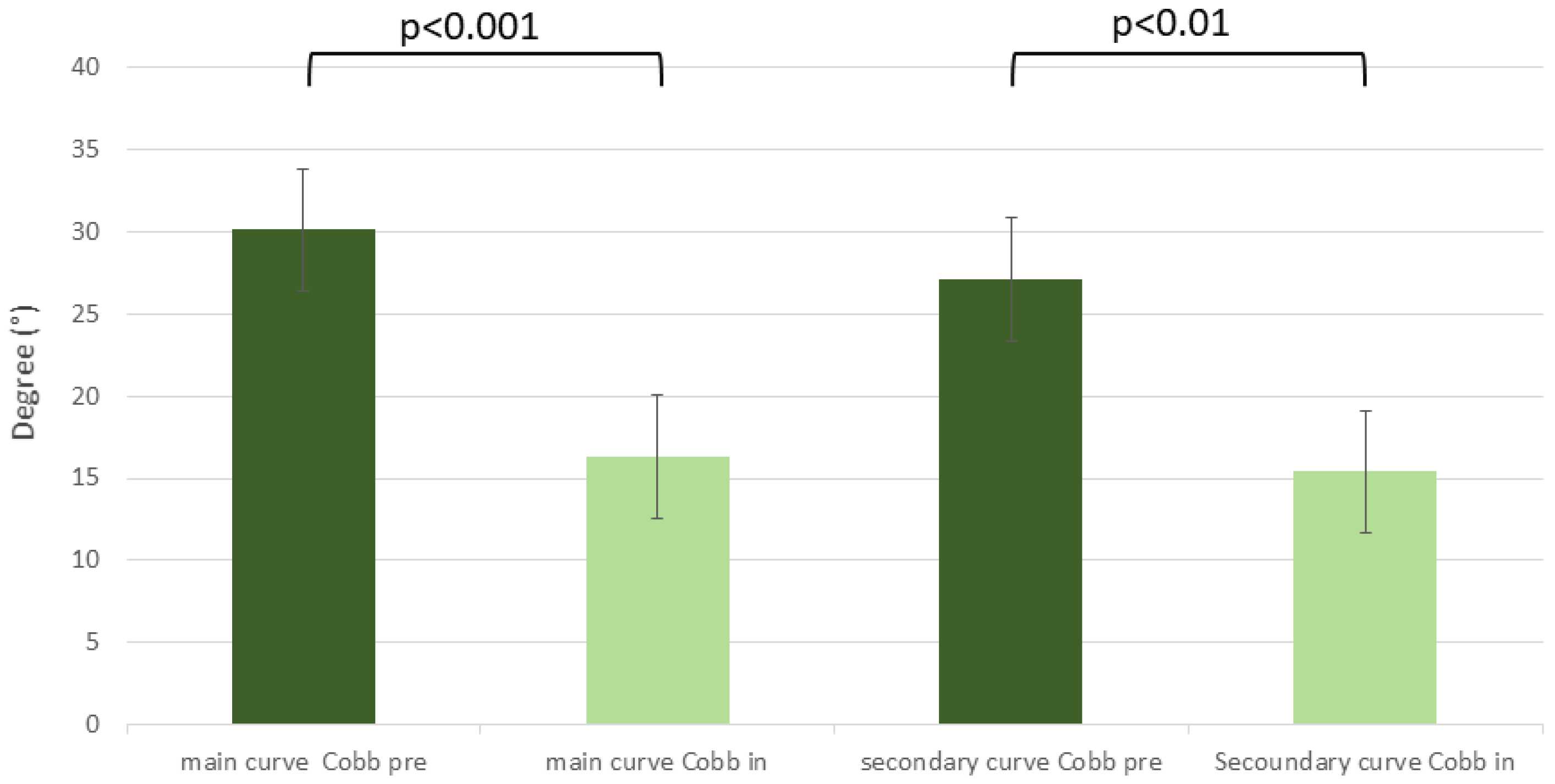
3.1. Global Analysis
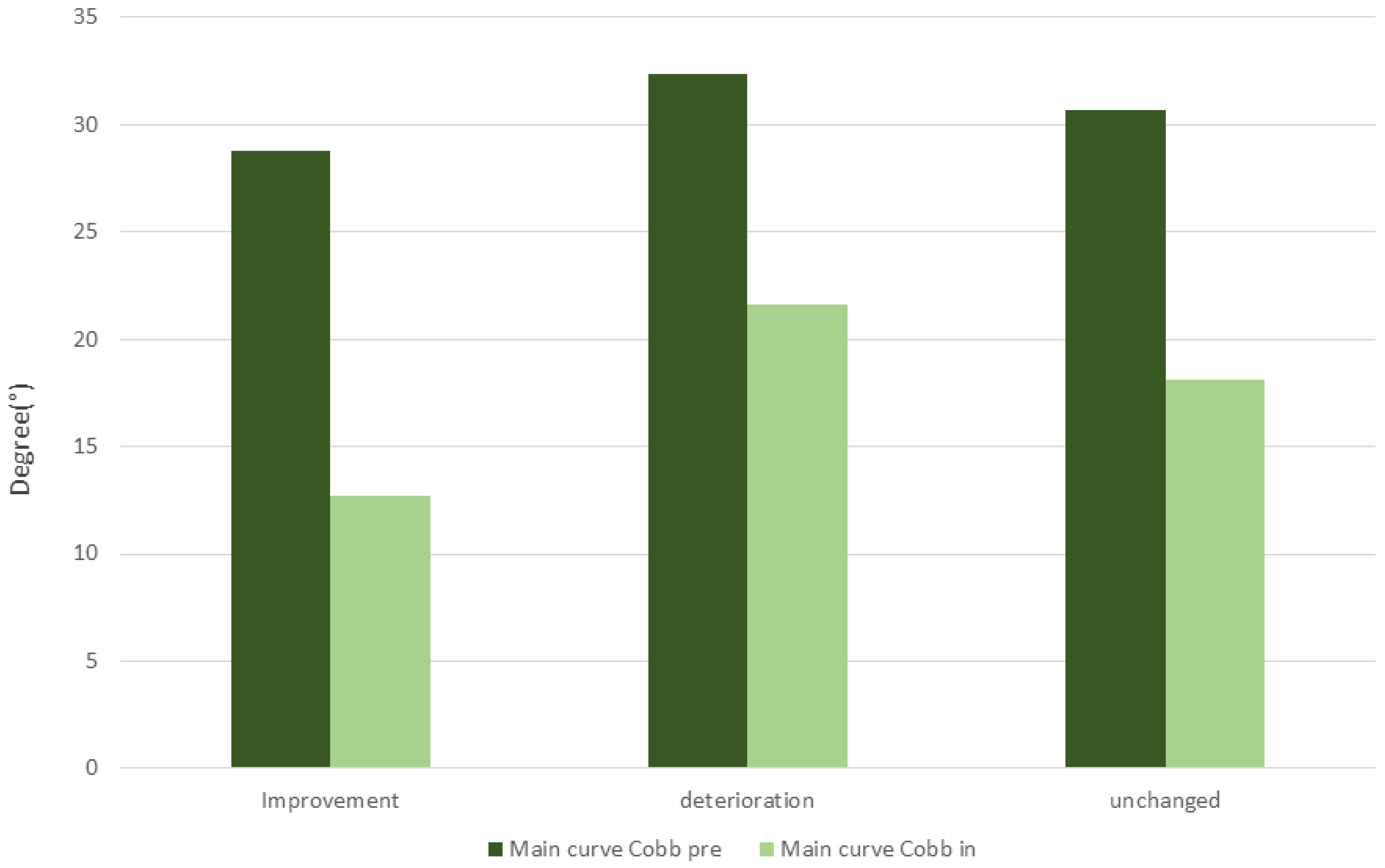
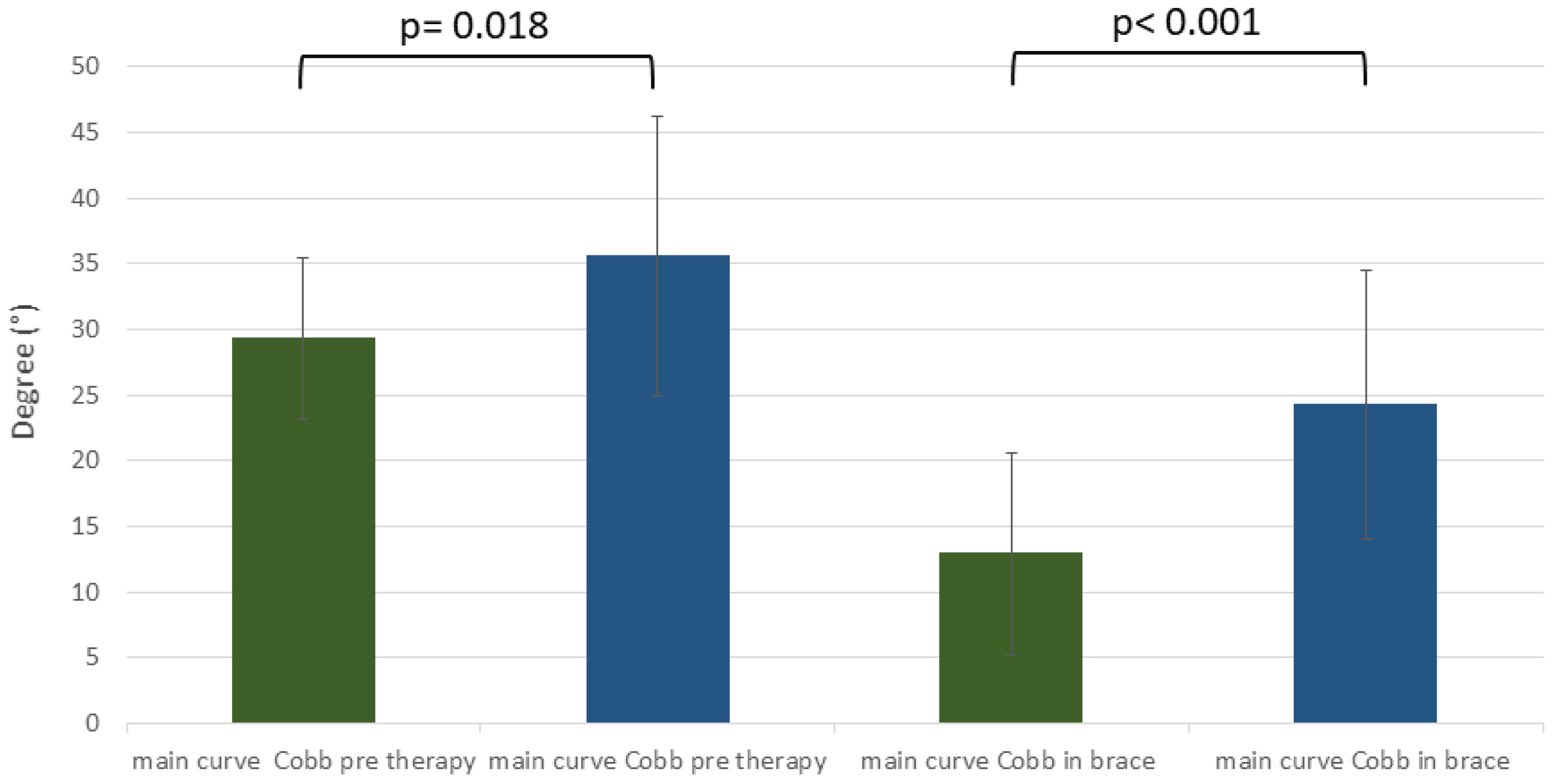
3.2. Sub-Analysis by Increased, Unchanged, and Decreased Cobb Angle
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- De George, F.V.; Fisher, R.L. Idiopathic scoliosis: Genetic and environmental aspects. J. Med. Genet. 1967, 4, 251–257. [Google Scholar] [CrossRef] [Green Version]
- Justice, C.M.; Miller, N.H.; Marosy, B.; Zhang, J.; Wilson, A.F. Familial idiopathic scoliosis: Evidence of an X-linked susceptibility locus. Spine 2003, 28, 589–594. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miller, N.H.; Justice, C.; Marosy, B.; Doheny, K.F.; Pugh, E.; Zhang, J.; Dietz, H.C.; Wilson, A.F. Identification of candidate regions for familial idiopathic scoliosis. Spine 2005, 30, 1181–1187. [Google Scholar] [CrossRef]
- Chan, V.; Fong, G.C.; Luk, K.D.; Yip, B.; Lee, M.-K.; Wong, M.-S.; Lu, D.D.; Chan, T.-K. A genetic locus for adolescent idiopathic scoliosis linked to chromosome 19p13.3. Am. J. Hum. Genet. 2002, 71, 401–406. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miller, N.H.; Mims, B.; Child, A.; Milewicz, D.M.; Sponseller, P.; Mims, B.; Child, A.; Milewicz, D.M.; Blanton, S.H. Genetic analysis of structural elastic fiber and collagen genes in familial adolescent idiopathic scoliosis. J. Orthop. Res. 1996, 14, 994–999. [Google Scholar] [CrossRef] [PubMed]
- Stokes, I.A.F.; Burwell, R.G.; Dangerfield, P.H. Biomechanical spinal growth modulation and progressive adolescent scoliosis—A test of the ‘vicious cycle’ pathogenetic hypothesis: Summary of an electronic focus group debate of the IBSE. Scoliosis 2006, 1, 16. [Google Scholar] [CrossRef]
- Deacon, P.; Flood, B.M.; Dickson, R.A. Idiopathic scoliosis in three dimensions. A radiographic and morphometric analysis. J. Bone Joint Surg. 1984, 66, 509–512. [Google Scholar] [CrossRef] [Green Version]
- Deacon, P.; Archer, I.A.; Dickson, R.A. The anatomy of spinal deformity: A biomechanical analysis. Orthopedics 1987, 10, 897–903. [Google Scholar] [CrossRef]
- Millner, P.A.; Dickson, R.A. Idiopathic scoliosis: Biomechanics and biology. Eur. Spine J. 1996, 5, 362–373. [Google Scholar] [CrossRef]
- Cotterill, P.C.; Kostuik, J.P.; D’Angelo, G.; Fernie, G.R.; Maki, B.E. An anatomical comparison of the human and bovine thoracolumbar spine. J. Orthop. Res. 1986, 4, 298–303. [Google Scholar] [CrossRef]
- Kouwenhoven, J.W.; Castelein, R.M. The pathogenesis of adolescent idiopathic scoliosis: Review of the literature. Spine 2008, 33, 2898–2908. [Google Scholar] [CrossRef] [PubMed]
- Nachemson All, J.E.; Weinstein, S.L. Report of the Prevalence and Natural History Committee of the Scoliosis Research Society. In Proceedings of the Annual Meeting of the Scoliosis Research Society, Denver, CO, USA, 22 September 1982. [Google Scholar]
- Weinstein, S.L.; Dolan, L.A.; Spratt, K.F.; Peterson, K.K.; Spoonamore, M.J.; Ponseti, I.V. Health and function of patients with untreated idiopathic scoliosis: A 50-year natural history study. JAMA 2003, 289, 559–567. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, J.C.; Castelein, R.M.; Chu, W.C.; Danielsson, A.J.; Dobbs, M.B.; Grivas, T.B.; Gurnett, C.A.; Luk, K.D.; Moreau, A.; Newton, P.O.; et al. Adolescent idiopathic scoliosis. Nat. Rev. Dis. Prim. 2015, 1, 15030. [Google Scholar] [CrossRef] [Green Version]
- Fang, M.-Q.; Wang, C.; Xiang, G.-H.; Lou, C.; Tian, N.-F.; Xu, H.-Z. Long-term effects of the Chêneau brace on coronal and sagittal alignment in adolescent idiopathic scoliosis. J. Neurosurg. Spine 2015, 23, 505–509. [Google Scholar] [CrossRef] [Green Version]
- Kotwicki, T.; Cheneau, J. Biomechanical action of a corrective brace on thoracic idiopathic scoliosis: Cheneau 2000 orthosis. Disabil. Rehabil. Assist. Technol. 2008, 3, 146–153. [Google Scholar] [CrossRef]
- Rigo, M.; Reiter, C.; Weiss, H.-R. Effect of conservative management on the prevalence of surgery in patients with adolescent idiopathic scoliosis. Pediatr. Rehabil. 2003, 6, 209–214. [Google Scholar] [CrossRef] [PubMed]
- Weiss, H.-R.; Weiss, G.; Schaar, H.-J. Incidence of surgery in conservatively treated patients with scoliosis. Pediatr. Rehabil. 2003, 6, 111–118. [Google Scholar] [CrossRef] [PubMed]
- Negrini, S.; Grivas, T.B.; Kotwicki, T.; Rigo, M.; Zaina, F.; International Society on Scoliosis Orthopaedic and Rehabilitation Treatment (SOSORT). Guidelines on Standards of management of idiopathic scoliosis with corrective braces in everyday clinics and in clinical research. SOSORT Consensus 2008. Scoliosis 2009, 4, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Richards, B.S.; Bernstein, R.M.; D’Amato, C.R.; Thompson, G.H. Standardization of criteria for adolescent idiopathic scoliosis brace studies: SRS Committee on Bracing and Nonoperative Management. Spine 2005, 30, 2068–2075; discussion 2076–2077. [Google Scholar] [CrossRef] [Green Version]
- Negrini, S.; Minozzi, S.; Bettany-Saltikov, J.; Chockalingam, N.; Grivas, T.B.; Kotwicki, T.; Maruyama, T.; Romano, M.; Zaina, F. Braces for idiopathic scoliosis in adolescents. Spine 2010, 35, 1285–1293. [Google Scholar] [CrossRef]
- Negrini, S.; Minozzi, S.; Bettany-Saltikov, J.; Chockalingam, N.; Grivas, T.B.; Kotwicki, T.; Maruyama, T.; Romano, M.; Zaina, F. Braces for idiopathic scoliosis in adolescents. Cochrane Database Syst. Rev. 2015, 18, CD006850. [Google Scholar] [CrossRef] [Green Version]
- Costa, L.; Schlosser, T.P.C.; Jimale, H.; Homans, J.F.; Kruyt, M.C.; Castelein, R.M. The Effectiveness of Different Concepts of Bracing in Adolescent Idiopathic Scoliosis (AIS): A Systematic Review and Meta-Analysis. J. Clin. Med. 2021, 10, 2145. [Google Scholar] [CrossRef] [PubMed]
- Rigo, M.; Jelačić, M. Brace technology thematic series: The 3D Rigo Chêneau-type brace. Scoliosis Spinal Disord. 2017, 12, 10. [Google Scholar] [CrossRef] [Green Version]
- Ferrero, E.; Lafage, R.; Challier, V.; Diebo, B.; Guigui, P.; Mazda, K.; Schwab, F.; Skalli, W.; Lafage, V. Clinical and stereoradiographic analysis of adult spinal deformity with and without rotatory subluxation. Orthop. Traumatol. Surg. Res. 2015, 101, 613–618. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lafage, R.; Ferrero, E.; Henry, J.K.; Challier, V.; Diebo, B.; Liabaud, B.; Lafage, V.; Schwab, F. Validation of a new computer-assisted tool to measure spino-pelvic parameters. Spine J. 2015, 15, 2493–2502. [Google Scholar] [CrossRef] [PubMed]
- Weiss, H.-R. Measurement of vertebral rotation: Perdriolle versus Raimondi. Eur. Spine J. 1995, 4, 34–38. [Google Scholar] [CrossRef] [PubMed]
- Lebel, D.E.; Al-Aubaidi, Z.; Shin, E.-J.; Howard, A.; Zeller, R. Three dimensional analysis of brace biomechanical efficacy for patients with AIS. Eur. Spine J. 2013, 22, 2445–2448. [Google Scholar] [CrossRef] [Green Version]
- Almansour, H.; Pepke, W.; Bruckner, T.; Diebo, B.G.; Akbar, M. Three-Dimensional Analysis of Initial Brace Correction in the Setting of Adolescent Idiopathic Scoliosis. J. Clin. Med. 2019, 8, 1804. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jonasson-Rajala, E.; Josefsson, E.; Lundberg, B.; Nilsson, H. Boston thoracic brace in the treatment of idiopathic scoliosis. Initial correction. Clin. Orthop. Relat. Res. 1984, 183, 37–41. [Google Scholar] [CrossRef]
- von Deimling, U.; Wagner, U.A.; Schmitt, O. Long-term effect of brace treatment on spinal decompensation in idiopathic scoliosis. A comparison of Milwaukee brace—Cheneau corset. Z. Orthop. Ihre Grenzgeb. 1995, 133, 270–273. [Google Scholar]
- Weiss, H.-R.; Weiss, G.M. Brace treatment during pubertal growth spurt in girls with idiopathic scoliosis (IS): A prospective trial comparing two different concepts. Pediatr. Rehabil. 2005, 8, 199–206. [Google Scholar] [CrossRef] [PubMed]
- De Giorgi, S.; Piazzolla, A.; Tafuri, S.; Borracci, C.; Martucci, A.; De Giorgi, G. Cheneau brace for adolescent idiopathic scoliosis: Long-term results. Can it prevent surgery? Eur. Spine J. 2013, 22 (Suppl. 6), S815–S822. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pasquini, G.; Cecchi, F.; Bini, C.; Molino-Lova, R.; Vannetti, F.; Castagnoli, C.; Paperini, A.; Boni, R.; Macchi, C.; Crusco, B.; et al. The outcome of modified version of the Cheneau brace in Adolescent Idiopathic Scoliosis (AIS) based on SRS and SOSORT criteria: A retrospective study. Eur. J. Phys. Rehabil. Med. 2016, 52, 618–629. [Google Scholar]
- Schmitz, A.; König, R.; Kandyba, J.; Pennekamp, P.; Schmitt, O.; Jaeger, U.E. Visualisation of the brace effect on the spinal profile in idiopathic scoliosis. Eur. Spine J. 2005, 14, 138–143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rigo, M.; Weiss, H.-R. The Chêneau concept of bracing—biomechanical aspects. Stud. Health Technol. Inform. 2008, 135, 303–319. [Google Scholar]
- Pham, V.M.; Herbaux, B.; Schill, A.; Thevenon, A. Evaluation of the Chêneau brace in adolescent idiopathic scoliosis. Ann. Readapt. Med. Phys. 2007, 50, 125–133. [Google Scholar] [CrossRef]
- Pepke, W.; El Zeneiny, A.; Almansour, H.; Bruckner, T.; Hemmer, S.; Akbar, M. Influence of Chêneau-Brace Therapy on Lumbar and Thoracic Spine and Its Interdependency with Cervical Spine Alignment in Patients with Adolescent Idiopathic Scoliosis (AIS). J. Clin. Med. 2021, 10, 1849. [Google Scholar] [CrossRef]
- Mac-Thiong, J.-M.; Labelle, H.; Roussouly, P. Pediatric sagittal alignment. Eur. Spine J. 2011, 20 (Suppl. 5), 586–590. [Google Scholar] [CrossRef] [Green Version]
- Mangione, P.; Gomez, D.; Senegas, J. Study of the course of the incidence angle during growth. Eur. Spine J. 1997, 6, 163–167. [Google Scholar] [CrossRef] [Green Version]
- Marty, C.; Boisaubert, B.; Descamps, H.; Montigny, J.; Hecquet, J.; Legaye, J.; Duval-Beaupère, G. The sagittal anatomy of the sacrum among young adults, infants, and spondylolisthesis patients. Eur. Spine J. 2002, 11, 119–125. [Google Scholar] [CrossRef] [Green Version]
- Katz, D.E.; Durrani, A.A. Factors that influence outcome in bracing large curves in patients with adolescent idiopathic scoliosis. Spine 2001, 26, 2354–2361. [Google Scholar] [CrossRef] [PubMed]
- Castro, F.P. Adolescent idiopathic scoliosis, bracing, and the Hueter-Volkmann principle. Spine J. 2003, 3, 180–185. [Google Scholar] [CrossRef] [PubMed]
- Mao, S.; Shi, B.; Xu, L.; Wang, Z.; Hung, A.L.H.; Lam, T.P.; Yu, F.W.P.; Lee, K.M.; Ng, B.K.W.; Cheng, J.; et al. Initial Cobb angle reduction velocity following bracing as a new predictor for curve progression in adolescent idiopathic scoliosis. Eur. Spine J. 2016, 25, 500–505. [Google Scholar] [CrossRef] [PubMed]
- Goodbody, C.M.; Asztalos, I.B.; Sankar, W.N.; Flynn, J.M. It’s not just the big kids: Both high and low BMI impact bracing success for adolescent idiopathic scoliosis. J. Child. Orthop. 2016, 10, 395–404. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thompson, R.M.; Hubbard, E.W.; Jo, C.-H.; Virostek, D.; Karol, L.A. Brace Success Is Related to Curve Type in Patients with Adolescent Idiopathic Scoliosis. J. Bone Joint Surg. Am. 2017, 99, 923–928. [Google Scholar] [CrossRef]
- Karol, L.A.; Virostek, D.; Felton, K.; Jo, C.; Butler, L. The Effect of the Risser Stage on Bracing Outcome in Adolescent Idiopathic Scoliosis. J. Bone Joint Surg. 2016, 98, 1253–1259. [Google Scholar] [CrossRef] [Green Version]
- Sun, X.; Wu, T.; Liu, Z.; Zhu, Z.; Qian, B.; Zhu, F.; Ma, W.; Yu, Y.; Wang, B.; Qiu, Y. Osteopenia predicts curve progression of adolescent idiopathic scoliosis in girls treated with brace treatment. J. Pediatr. Orthop. 2013, 33, 366–371. [Google Scholar] [CrossRef]
- Zhang, Y.; Yang, Y.; Dang, X.; Zhao, L.; Ren, J.; Zhang, L.; Sun, J. Factors relating to curve progression in female patients with adolescent idiopathic scoliosis treated with a brace. Eur. Spine J. 2015, 24, 244–248. [Google Scholar] [CrossRef]
- Charles, Y.P.; Canavese, F.; Diméglio, A. Curve progression risk in a mixed series of braced and nonbraced patients with idiopathic scoliosis related to skeletal maturity assessment on the olecranon. J. Pediatr. Orthop. B 2017, 26, 240–244. [Google Scholar] [CrossRef]
- Strube, P.; Gunold, M.; Müller, T.; Leimert, M.; Sachse, A.; Pumberger, M.; Putzier, M.; Zippelius, T. Influence of curve morphology and location on the efficacy of rigid conservative treatment in patients with adolescent idiopathic scoliosis. Bone Joint J. 2021, 103-B, 373–381. [Google Scholar] [CrossRef]
- Lenke, L.G.; Edwards, C.C., 2nd; Bridwell, K.H. The Lenke classification of adolescent idiopathic scoliosis: How it organizes curve patterns as a template to perform selective fusions of the spine. Spine 2003, 28, S199–S207. [Google Scholar] [CrossRef] [PubMed]
- Courvoisier, A.; Drevelle, X.; Vialle, R.; Dubousset, J.; Skalli, W. 3D analysis of brace treatment in idiopathic scoliosis. Eur. Spine J. 2013, 22, 2449–2455. [Google Scholar] [CrossRef] [PubMed] [Green Version]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Before Treatment | At Final Follow-Up | Difference | 95%CI | p Value |
|---|---|---|---|---|---|
| Cobb angle (°) | 30.8 ± 8.2 | 29.3 ± 15.2 | 1.5 ± 11.2 | −1.0 to 3.9 | 0.26 |
| TK1 (°) | 33.7 ± 13.7 | 31.2 ± 12.4 | −2.5 ± 9.4 | 0.3 to 4.5 | 0.02 |
| TK2 (°) | 26.7 ± 13.8 | 25.8 ± 12.3 | −0.8 ± 8.9 | −1.1 to 2.9 | 0.38 |
| LL (°) | 57.9 ± 12.1 | 56.0 ± 12.7 | 1.9 ± 9.4 | −4.0 to 0.1 | 0.07 |
| PT (°) | 7.8 ± 8.3 | 8.9 ± 7.9 | 1.0 ± 7.5 | −2.7 to 0.5 | 0.20 |
| PI (°) | 50.6 ± 14.5 | 50.8 ± 14.3 | 0.2 ± 2.5 | −0.7 to 0.3 | 0.49 |
| SS (°) | 42.3 ± 10.0 | 41.1 ± 9.9 | −1.1 ± 6.9 | −0.3 to 2.7 | 0.13 |
| T1SPi (°) | −4.3 ± 3.9 | −4.5 ± 2.3 | −0.1 ± 4.0 | −0.6 to 1.1 | 0.64 |
| T9SPi (°) | −6.2 ± 4.7 | −6.6 ± 3.2 | −0.4 ± 4.5 | −0.6 to 1.4 | 0.42 |
| Raimondi 1 (°) | 17.6 ± 9.4 | 18.0 ± 9.6 | 0.3 ± 9.7 | −2.5 to 1.8 | 0.76 |
| SVA (mm) | −10.1 ± 32.7 | −10.0 ± 22.9 | 0.2 ± 33.3 | −7.5 to 0.9 | 0.98 |
| No. of Patients (%) | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Coronal Parameters | Sagittal Parameters | Axial Rotation | Pelvic Parameters | |||||||||
| Variation | Cobb Angle | CorC7PL | TK1 | TK2 | LL | C1/C2 | T1 Slope | Raimondi 1 | PT | PI | SS | SVA |
| Increased | 15 (19) | 13 (17) | 18 (23) | 23 (29) | 29 (37) | 11 (14) | 18 (23) | 22 (28) | 17 (22) | 2 (2) | 14 (18) | 32 (41) |
| Unchanged | 36 (46) | 33 (42) | 34 (44) | 34 (44) | 35 (45) | 35 (45) | 28 (36) | 38 (49) | 47 (60) | 72 (92) | 50 (64) | 14 (18) |
| Decreased | 27 (35) | 32 (41) | 26 (33) | 21 (27) | 14 (18) | 32 (41) | 32 (41) | 18 (23) | 14 (18) | 4 (5) | 14 (18) | 32 (41) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pepke, W.; Morani, W.; Schiltenwolf, M.; Bruckner, T.; Renkawitz, T.; Hemmer, S.; Akbar, M. Outcome of Conservative Therapy of Adolescent Idiopathic Scoliosis (AIS) with Chêneau-Brace. J. Clin. Med. 2023, 12, 2507. https://doi.org/10.3390/jcm12072507
Pepke W, Morani W, Schiltenwolf M, Bruckner T, Renkawitz T, Hemmer S, Akbar M. Outcome of Conservative Therapy of Adolescent Idiopathic Scoliosis (AIS) with Chêneau-Brace. Journal of Clinical Medicine. 2023; 12(7):2507. https://doi.org/10.3390/jcm12072507
Chicago/Turabian StylePepke, Wojciech, William Morani, Marcus Schiltenwolf, Tom Bruckner, Tobias Renkawitz, Stefan Hemmer, and Michael Akbar. 2023. "Outcome of Conservative Therapy of Adolescent Idiopathic Scoliosis (AIS) with Chêneau-Brace" Journal of Clinical Medicine 12, no. 7: 2507. https://doi.org/10.3390/jcm12072507