
Alliance for Sleep Clinical Practice Guideline on Switching or Deprescribing Hypnotic Medications for Insomnia
 , and
, and
Abstract
:1. Introduction
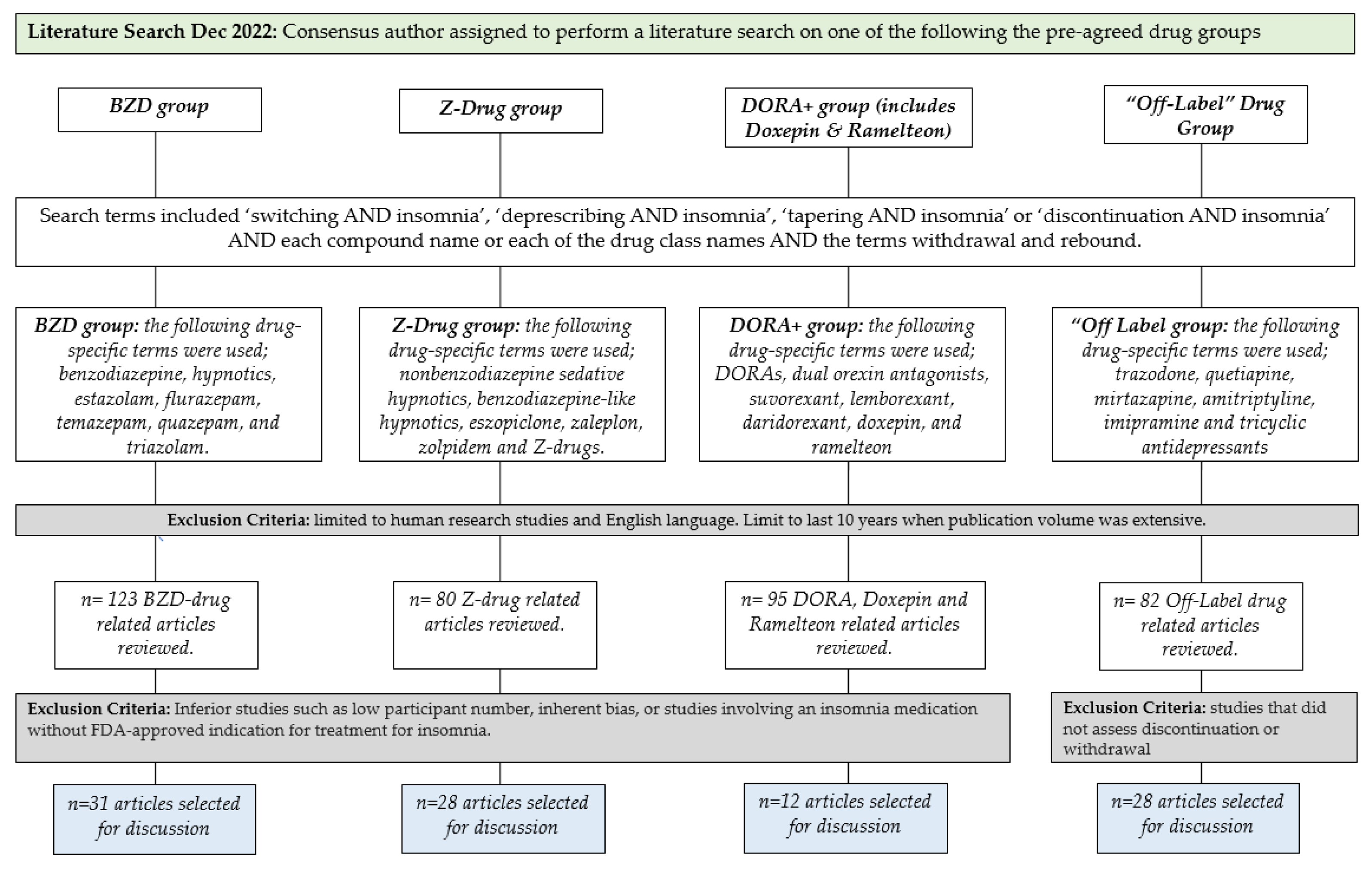
2. Materials and Methods
3. Results
3.1. Literature Review
3.1.1. BZD Drug Discontinuation
3.1.2. Risk of Adverse Effects of BZD Drug Discontinuation
3.1.3. Best Practices for BZD Discontinuation
3.2. Z-Drug Discontinuation
3.2.1. Risk of Adverse Effects of Z-Drug Discontinuation
Zolpidem
Zaleplon
Eszopiclone
3.2.2. Best Practices for Z-Drug Discontinuation
3.3. DORAs, Doxepin, and Ramelteon Discontinuation
3.3.1. Risk of Adverse Effects of DORAs, Doxepin, or Ramelteon Discontinuation
DORAs
Low-Dose Doxepin
Ramelteon
3.3.2. Best Practices for DORAs, Doxepin, or Ramelteon Discontinuation
3.4. “Off-LABEL” Drugs in the Treatment of Insomnia
3.4.1. Risk of Adverse Effects of “Off-Label” Drug Discontinuation
Trazodone
Mirtazapine and Esmirtazapine
Doxepin (Antidepressant-Approved Doses)
Trimipramine
Quetiapine
3.4.2. Best Practices for Discontinuation of Off-Label Drugs for Insomnia
4. Discussion
5. Final Recommendations
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sateia, M.J.; Buysse, D.J.; Krystal, A.D.; Neubauer, D.N.; Heald, J.L. Clinical practice guideline for the pharmacologic treatment of chronic insomnia in adults: An american academy of sleep medicine clinical practice guideline. J. Clin. Sleep Med. 2017, 13, 307–349. [Google Scholar] [CrossRef]
- Morin, C.M.; Jarrin, D.C. Epidemiology of insomnia: Prevalence, course, risk factors, and public health burden. Sleep Med. Clin. 2022, 17, 173–191. [Google Scholar] [CrossRef]
- Morin, C.M.; LeBlanc, M.; Daley, M.; Gregoire, J.P.; Merette, C. Epidemiology of insomnia: Prevalence, self-help treatments, consultations, and determinants of help-seeking behaviors. Sleep Med. 2006, 7, 123–130. [Google Scholar] [CrossRef]
- Khan, M.S.; Aouad, R. The effects of insomnia and sleep loss on cardiovascular disease. Sleep Med. Clin. 2022, 17, 193–203. [Google Scholar] [CrossRef] [PubMed]
- Espie, C.A.; Pawlecki, B.; Waterfield, D.; Fitton, K.; Radocchia, M.; Luik, A.I. Insomnia symptoms and their association with workplace productivity: Cross-sectional and pre-post intervention analyses from a large multinational manufacturing company. Sleep Health 2018, 4, 307–312. [Google Scholar] [CrossRef]
- Erickson, E.A.; Stahlman, S.; McNellis, M.G. Insomnia and motor vehicle accident-related injuries, active component, U.S. Armed Forces, 2007–2016. MSMR 2017, 24, 2–11. [Google Scholar]
- Sorscher, A.J. Insomnia: Getting to the cause, facilitating relief. J. Fam. Pract. 2017, 66, 216–225. [Google Scholar]
- Lack, L.; Sweetman, A. Diagnosis and treatment of insomnia comorbid with obstructive sleep apnea. Sleep Med. Clin. 2016, 11, 379–388. [Google Scholar] [CrossRef]
- Alfoldi, P.; Wiklund, T.; Gerdle, B. Comorbid insomnia in patients with chronic pain: A study based on the Swedish quality registry for pain rehabilitation (SQRP). Disabil. Rehabil. 2014, 36, 1661–1669. [Google Scholar] [CrossRef] [PubMed]
- Jeon, B.; Luyster, F.S.; Callan, J.A.; Chasens, E.R. Depressive symptoms in comorbid obstructive sleep apnea and insomnia: An integrative review. West. J. Nurs. Res. 2021, 193945921989656. [Google Scholar] [CrossRef] [PubMed]
- Khurshid, K.A. Comorbid insomnia and psychiatric disorders: An update. Innov. Clin. Neurosci. 2018, 15, 28–32. [Google Scholar] [PubMed]
- Neubauer, D.N. Current and new thinking in the management of comorbid insomnia. Am. J. Manag. Care 2009, 15, S24–S32. [Google Scholar] [PubMed]
- Van Gastel, A. Drug-induced insomnia and excessive sleepiness. Sleep Med. Clin. 2022, 17, 471–484. [Google Scholar] [CrossRef] [PubMed]
- Trauer, J.M.; Qian, M.Y.; Doyle, J.S.; Rajaratnam, S.M.; Cunnington, D. Cognitive Behavioral Therapy for Chronic Insomnia: A Systematic Review and Meta-analysis. Ann. Intern. Med. 2015, 163, 191–204. [Google Scholar] [CrossRef]
- Kaufmann, C.N.; Spira, A.P.; Alexander, G.C.; Rutkow, L.; Mojtabai, R. Trends in prescribing of sedative-hypnotic medications in the USA: 1993-2010. Pharmacoepidemiol. Drug. Saf. 2016, 25, 637–645. [Google Scholar] [CrossRef] [Green Version]
- Ford, E.S.; Wheaton, A.G.; Cunningham, T.J.; Giles, W.H.; Chapman, D.P.; Croft, J.B. Trends in outpatient visits for insomnia, sleep apnea, and prescriptions for sleep medications among US adults: Findings from the National Ambulatory Medical Care survey 1999-2010. Sleep 2014, 37, 1283–1293. [Google Scholar] [CrossRef] [Green Version]
- Cascade, E.; Kalali, A.H.; Kwentus, J.A.; Bharmal, M. Trends in CNS prescribing following the economic slowdown. Psychiatry (Edgmont) 2009, 6, 15–17. [Google Scholar]
- Bertisch, S.M.; Herzig, S.J.; Winkelman, J.W.; Buettner, C. National use of prescription medications for insomnia: NHANES 1999–2010. Sleep 2014, 37, 343–349. [Google Scholar] [CrossRef] [Green Version]
- Tannenbaum, C.; Farrell, B.; Shaw, J.; Morgan, S.; Trimble, J.; Currie, J.; Turner, J.; Rochon, P.; Silvius, J. An ecological approach to reducing potentially inappropriate medication use: Canadian deprescribing network. Can. J. Aging 2017, 36, 97–107. [Google Scholar] [CrossRef] [Green Version]
- By the American Geriatrics Society Beers Criteria Update Expert Panel. American Geriatrics Society 2015 Updated Beers criteria for potentially inappropriate medication use in older adults. J. Am. Geriatr. Soc. 2015, 63, 2227–22246. [Google Scholar] [CrossRef]
- Riemann, D.; Baglioni, C.; Bassetti, C.; Bjorvatn, B.; Dolenc Groselj, L.; Ellis, J.G.; Espie, C.A.; Garcia-Borreguero, D.; Gjerstad, M.; Gonçalves, M.; et al. European guideline for the diagnosis and treatment of insomnia. J. Sleep Res. 2017, 26, 675–700. [Google Scholar] [CrossRef] [PubMed]
- Sweetman, A.; Lovato, N.; Chai-Coetzer, C.L.; Saini, B. De-prescribing long-term use of benzodiazepines in primary care practice: Where to next? Sleep 2023, zsad015, Epub ahead of print. [Google Scholar] [CrossRef]
- Grant, M.J.; Booth, A. A typology of reviews: An analysis of 14 review types and associated methodologies. Health Inf. Libr J. 2009, 26, 91–108. [Google Scholar] [CrossRef]
- Hintze, J.P.; Edinger, J.D. Hypnotic discontinuation in chronic insomnia. Sleep Med. Clin. 2022, 17, 523–530. [Google Scholar] [CrossRef] [PubMed]
- Soldatos, C.R.; Dikeos, D.G.; Whitehead, A. Tolerance and rebound insomnia with rapidly eliminated hypnotics: A meta-analysis of sleep laboratory studies. Int. Clin. Psychopharmacol. 1999, 14, 287–303. [Google Scholar] [CrossRef]
- Gillin, J.C.; Spinweber, C.L.; Johnson, L.C. Rebound insomnia: A critical review. J. Clin. Psychopharmacol. 1989, 9, 161–172. [Google Scholar] [CrossRef] [Green Version]
- Lader, M. Rebound insomnia and newer hypnotics. Psychopharmacology 1992, 108, 248–255. [Google Scholar] [CrossRef]
- Morgan, K.; Oswald, I. Anxiety caused by a short-life hypnotic. Br. Med. J. (Clin. Res. Ed.) 1982, 284, 942. [Google Scholar] [CrossRef] [Green Version]
- Kales, A.; Vgontzas, A.N.; Bixler, E.O. A reassessment of triazolam. Int. J. Risk Saf. Med. 1996, 9, 7–27. [Google Scholar] [CrossRef] [PubMed]
- Lerner, A.; Klein, M. Dependence, withdrawal and rebound of CNS drugs: An update and regulatory considerations for new drugs development. Brain Commun. 2019, 1, fcz025. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hatano, M.; Kamei, H.; Inagaki, R.; Matsuzaki, H.; Hanya, M.; Yamada, S.; Iwata, N. Assessment of switching to suvorexant versus the use of add-on suvorexant in combination with benzodiazepine receptor agonists in insomnia patients: A retrospective study. Clin. Psychopharmacol. Neurosci. 2018, 16, 184–189. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suzuki, H.; Hibino, H. Characteristics of patients who were able to switch from benzodiazepine hypnotics to lemborexant. SAGE Open. Med. 2021, 9, 20503121211037903. [Google Scholar] [CrossRef] [PubMed]
- Shigetsura, Y.; Imai, S.; Endo, H.; Shimizu, Y.; Ueda, K.; Murai, T.; Itohara, K.; Nakagawa, S.; Yonezawa, A.; Ikemi, Y.; et al. Assessment of suvorexant and eszopiclone as alternatives to benzodiazepines for treating insomnia in patients with major depressive disorder. Clin. Neuropharmacol. 2022, 45, 52–60. [Google Scholar] [CrossRef]
- Wright, A.; Diebold, J.; Otal, J.; Stoneman, C.; Wong, J.; Wallace, C.; Duffett, M. The effect of melatonin on benzodiazepine discontinuation and sleep quality in adults attempting to discontinue benzodiazepines: A systematic review and meta-analysis. Drugs Aging 2015, 32, 1009–1018. [Google Scholar] [CrossRef] [PubMed]
- Morera-Fumero, A.L.; Fernandez-Lopez, L.; Abreu-Gonzalez, P. Melatonin and melatonin agonists as treatments for benzodiazepines and hypnotics withdrawal in patients with primary insomnia. A systematic review. Drug. Alcohol. Depend. 2020, 212, 107994. [Google Scholar] [CrossRef] [PubMed]
- An, J.H.; Park, M.J.; Fava, M.; Mischoulon, D.; Kim, H.; Jang, J.; Hong, J.P.; Park, J.S.; Jeon, H.J. Comparisons between successful versus unsuccessful switches from benzodiazepines or zolpidem (z-drug) to controlled-release melatonin in patients with major depressive disorder and insomnia. Front. Psychiatry 2020, 11, 444. [Google Scholar] [CrossRef]
- Lemoine, P.; Ohayon, M.M. Is hypnotic withdrawal facilitated by the transitory use of a substitute drug? Prog. Neuropsychopharmacol. Biol. Psychiatry 1997, 21, 111–124. [Google Scholar] [CrossRef]
- Pat-Horenczyk, R.; Hacohen, D.; Herer, P.; Lavie, P. The effects of substituting zopiclone in withdrawal from chronic use of benzodiazepine hypnotics. Psychopharmacology (Berl.) 1998, 140, 450–457. [Google Scholar] [CrossRef]
- Roehrs, T.; Lamphere, J.; Paxton, C.; Wittig, R.; Zorick, F.; Roth, T. Temazepam’s efficacy in patients with sleep onset insomnia. Br. J. Clin. Pharmacol. 1984, 17, 691–696. [Google Scholar] [CrossRef] [Green Version]
- Ankier, S.I.; Goa, K.L. Quazepam. A preliminary review of its pharmacodynamic and pharmacokinetic properties, and therapeutic efficacy in insomnia. Drugs 1988, 35, 42–62. [Google Scholar] [CrossRef]
- Kales, A.; Bixler, E.O.; Soldatos, C.R.; Vela-Bueno, A.; Jacoby, J.A.; Kales, J.D. Quazepam and temazepam: Effects of short- and intermediate-term use and withdrawal. Clin. Pharmacol. Ther. 1986, 39, 345–352. [Google Scholar] [CrossRef] [PubMed]
- Mamelak, M.; Csima, A.; Price, V. A comparative 25-night sleep laboratory study on the effects of quazepam and triazolam on chronic insomniacs. J. Clin. Pharmacol. 1984, 24, 65–75. [Google Scholar] [CrossRef] [PubMed]
- Greenblatt, D.J.; Harmatz, J.S.; Zinny, M.A.; Shader, R.I. Effect of gradual withdrawal on the rebound sleep disorder after discontinuation of triazolam. N. Engl. J. Med. 1987, 317, 722–728. [Google Scholar] [CrossRef] [PubMed]
- Bixler, E.O.; Kales, J.D.; Kales, A.; Jacoby, J.A.; Soldatos, C.R. Rebound insomnia and elimination half-life: Assessment of individual subject response. J. Clin. Pharmacol. 1985, 25, 115–124. [Google Scholar] [CrossRef]
- Mauri, M.C.; Gianetti, S.; Pugnetti, L.; Altamura, A.C. Quazepam versus triazolam in patients with sleep disorders: A double-blind study. Int. J. Clin. Pharmacol. Res. 1993, 13, 173–177. [Google Scholar]
- Scharf, M.B. Feasibility of an every-other-night regimen in insomniac patients: Subjective hypnotic effectiveness of quazepam, triazolam, and placebo. J. Clin. Psychiatry. 1993, 54, 33–38. [Google Scholar]
- Kales, A.; Kales, J.D. Sleep laboratory studies of hypnotic drugs: Efficacy and withdrawal effects. J. Clin. Psychopharmacol. 1983, 3, 140–150. [Google Scholar] [CrossRef]
- Voderholzer, U.; Riemann, D.; Hornyak, M.; Backhaus, J.; Feige, B.; Berger, M.; Hohagen, F. A double-blind, randomized and placebo-controlled study on the polysomnographic withdrawal effects of zopiclone, zolpidem and triazolam in healthy subjects. Eur. Arch. Psychiatry Clin. Neurosci. 2001, 251, 117–123. [Google Scholar] [CrossRef]
- Kales, A.; Manfredi, R.L.; Vgontzas, A.N.; Bixler, E.O.; Vela-Bueno, A.; Fee, E.C. Rebound insomnia after only brief and intermittent use of rapidly eliminated benzodiazepines. Clin. Pharmacol. Ther. 1991, 49, 468–476. [Google Scholar] [CrossRef]
- Pottie, K.; Thompson, W.; Davies, S.; Grenier, J.; Sadowski, C.A.; Welch, V.; Holbrook, A.; Boyd, C.; Swenson, R.; Ma, A.; et al. Deprescribing benzodiazepine receptor agonists: Evidence-based clinical practice guideline. Can. Fam. Physician 2018, 64, 339–351. [Google Scholar]
- Reeve, E.; Ong, M.; Wu, A.; Jansen, J.; Petrovic, M.; Gnjidic, D. A systematic review of interventions to deprescribe benzodiazepines and other hypnotics among older people. Eur. J. Clin. Pharmacol. 2017, 73, 927–935. [Google Scholar] [CrossRef]
- Paquin, A.M.; Zimmerman, K.; Rudolph, J.L. Risk versus risk: A review of benzodiazepine reduction in older adults. Expert Opin. Drug. Saf. 2014, 13, 919–934. [Google Scholar] [CrossRef] [PubMed]
- Takaesu, Y.; Utsumi, T.; Okajima, I.; Shimura, A.; Kotorii, N.; Kuriyama, K.; Yamashita, H.; Suzuki, M.; Watanabe, N.; Mishima, K. Psychosocial intervention for discontinuing benzodiazepine hypnotics in patients with chronic insomnia: A systematic review and meta-analysis. Sleep Med. Rev. 2019, 48, 101214. [Google Scholar] [CrossRef]
- Asnis, G.M.; Chakraburtty, A.; DuBoff, E.A.; Krystal, A.; Londborg, P.D.; Rosenberg, R.; Roth-Schechter, B.; Scharf, M.B.; Walsh, J.K. Zolpidem for persistent insomnia in SSRI-treated depressed patients. J. Clin. Psychiatry 1999, 60, 668–676. [Google Scholar] [CrossRef] [PubMed]
- Walsh, J.K.; Soubrane, C.; Roth, T. Efficacy and safety of zolpidem extended release in elderly primary insomnia patients. Am. J. Geriatr. Psychiatry 2008, 16, 44–57. [Google Scholar] [CrossRef] [PubMed]
- Zammit, G. Comparative tolerability of newer agents for insomnia. Drug. Saf. 2009, 32, 735–748. [Google Scholar] [CrossRef] [PubMed]
- Roehrs, T.A.; Randall, S.; Harris, E.; Maan, R.; Roth, T. Twelve months of nightly zolpidem does not lead to rebound insomnia or withdrawal symptoms: A prospective placebo-controlled study. J. Psychopharmacol. 2012, 26, 1088–1095. [Google Scholar] [CrossRef] [Green Version]
- Ware, J.C.; Walsh, J.K.; Scharf, M.B.; Roehrs, T.; Roth, T.; Vogel, G.W. Minimal rebound insomnia after treatment with 10-mg zolpidem. Clin. Neuropharmacol. 1997, 20, 116–125. [Google Scholar] [CrossRef]
- Rosenberg, R.; Amchin, J.; Kumar, D.; Perdomo, C.; Atkins, N., Jr.; Moline, M.; Malhotra, M. 335 Evaluation of dose transition from zolpidem to lemborexant across 14 weeks: Results from a multicenter open-label pilot study. Sleep 2021, 44, A134. [Google Scholar] [CrossRef]
- Ancoli-Israel, S.; Walsh, J.K.; Mangano, R.M.; Fujimori, M.; Zaleplon, A. novel nonbenzodiazepine hypnotic, effectively treats insomnia in elderly patients without causing rebound effects. Prim care companion. J. Clin. Psychiatry 1999, 1, 114–120. [Google Scholar] [CrossRef] [Green Version]
- Fry, J.; Scharf, M.; Mangano, R.; Fujimori, M. Zaleplon improves sleep without producing rebound effects in outpatients with insomnia. Zaleplon Clinical Study Group. Int. Clin. Psychopharmacol. 2000, 15, 141–152. [Google Scholar] [CrossRef]
- Ancoli-Israel, S.; Richardson, G.S.; Mangano, R.M.; Jenkins, L.; Hall, P.; Jones, W.S. Long-term use of sedative hypnotics in older patients with insomnia. Sleep Med. 2005, 6, 107–113. [Google Scholar] [CrossRef]
- Zammit, G.K.; McNabb, L.J.; Caron, J.; Amato, D.A.; Roth, T. Efficacy and safety of eszopiclone across 6-weeks of treatment for primary insomnia. Curr. Med. Res. Opin. 2004, 20, 1979–1991. [Google Scholar] [CrossRef] [PubMed]
- Ancoli-Israel, S.; Krystal, A.D.; McCall, W.V.; Schaefer, K.; Wilson, A.; Claus, R.; Rubens, R.; Roth, T. A 12-week, randomized, double-blind, placebo-controlled study evaluating the effect of eszopiclone 2 mg on sleep/wake function in older adults with primary and comorbid insomnia. Sleep 2010, 33, 225–234. [Google Scholar] [CrossRef] [PubMed]
- Inoue, Y.; Takaesu, Y.; Koebis, M. Prevalence of and factors associated with acute withdrawal symptoms after 24 weeks of eszopiclone treatment in patients with chronic insomnia: A prospective, interventional study. BMC Psychiatry 2021, 21, 193. [Google Scholar] [CrossRef]
- Krystal, A.; Fava, M.; Rubens, R.; Wessel, T.; Caron, J.; Wilson, P.; Roth, T.; McCall, W.V. Evaluation of eszopiclone discontinuation after cotherapy with fluoxetine for insomnia with coexisting depression. J. Clin. Sleep Med. 2007, 3, 48–55. [Google Scholar]
- Pollack, M.; Kinrys, G.; Krystal, A.; McCall, W.V.; Roth, T.; Schaefer, K.; Rubens, R.; Roach, J.; Huang, H.; Krishnan, R. Eszopiclone coadministered with escitalopram in patients with insomnia and comorbid generalized anxiety disorder. Arch. Gen. Psychiatry 2008, 65, 551–562. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rösner, S.; Englbrecht, C.; Wehrle, R.; Hajak, G.; Soyka, M. Eszopiclone for insomnia. Cochrane Database Syst. Rev. 2018, 10, CD010703. [Google Scholar] [CrossRef]
- Pollmann, A.S.; Murphy, A.L.; Bergman, J.C.; Gardner, D.M. Deprescribing benzodiazepines and Z-drugs in community-dwelling adults: A scoping review. BMC Pharmacol. Toxicol. 2015, 16, 19. [Google Scholar] [CrossRef] [Green Version]
- Green, A.R.; Aschmann, H.; Boyd, C.M.; Schoenborn, N. Assessment of patient-preferred language to achieve goal-aligned deprescribing in older adults. JAMA Netw. Open. 2021, 4, e212633. [Google Scholar] [CrossRef]
- Kuntz, J.L.; Kouch, L.; Christian, D.; Hu, W.; Peterson, P.L. Patient education and pharmacist consultation influence on nonbenzodiazepine sedative medication deprescribing success for older adults. Perm. J. 2019, 18–161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Belleville, G.; Morin, C.M. Hypnotic discontinuation in chronic insomnia: Impact of psychological distress, readiness to change, and self-efficacy. Health Psychol. 2008, 27, 239–248. [Google Scholar] [CrossRef] [PubMed]
- Park, K.M.; Kim, T.H.; Kim, W.J.; An, S.K.; Namkoong, K.; Lee, E. Cognitive Behavioral Therapy for Insomnia Reduces Hypnotic Prescriptions. Psychiatry Investig. 2018, 15, 499–504. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Michelson, D.; Snyder, E.; Paradis, E.; Chengan-Liu, M.; Snavely, D.B.; Hutzelmann, J.; Walsh, J.K.; Krystal, A.D.; Benca, R.M.; Cohn, M.; et al. Safety and efficacy of suvorexant during 1- year treatment of insomnia with subsequent abrupt treatment discontinuation: A phase3 randomised, double-blind, placebo-controlled trial. Lancet Neurol. 2014, 13, 461–471. [Google Scholar] [CrossRef] [PubMed]
- Herring, W.J.; Connor, K.M.; Ivgy-May, N.; Snyder, E.; Liu, K.; Snavely, D.B.; Krystal, A.D.; Walsh, J.K.; Benca, R.M.; Rosenberg, R.; et al. Suvorexant in patients with insomnia: Results from two 3-month randomized controlled clinical trials. Biol. Psychiatry 2016, 79, 136–148. [Google Scholar] [CrossRef] [PubMed]
- Herring, W.J.; Connor, K.M.; Snyder, E.; Snavely, D.B.; Zhang, Y.; Hutzelmann, J.; Matzura-Wolfe, D.; Benca, R.M.; Krystal, A.D.; Walsh, J.K.; et al. Suvorexant in elderly patients with insomnia: Pooled analyses of data from phase iii randomized controlled clinical trials. Am. J. Geriatr. Psychiatry 2017, 25, 791–802. [Google Scholar] [CrossRef]
- Yardley, J.; Kärppä, M.; Inoue, Y.; Pinner, K.; Perdomo, C.; Ishikawa, K.; Filippov, G.; Kubota, N.; Moline, M. Long-term effectiveness and safety of lemborexant in adults with insomnia disorder: Results from a phase 3 randomized clinical trial. Sleep Med. 2021, 80, 333–342. [Google Scholar] [CrossRef]
- Takaesu, Y.; Suzuki, M.; Moline, M.; Pinner, K.; Inabe, K.; Nishi, Y.; Kuriyama, K. Effect of discontinuation of lemborexant following long-term treatment of insomnia disorder: Secondary analysis of a randomized clinical trial. Clin. Transl. Sci. 2022. Epub ahead of print. [Google Scholar] [CrossRef]
- Kunz, D.; Dauvilliers, Y.; Benes, H.; García-Borreguero, D.; Plazzi, G.; Seboek Kinter, D.; Coloma, P.; Rausch, M.; Sassi-Sayadi, M.; Thein, S. Long-term safety and tolerability of daridorexant in patients with insomnia disorder. CNS Drugs 2022, 9. Epub ahead of print. [Google Scholar] [CrossRef]
- Krystal, A.D.; Lankford, A.; Durrence, H.H.; Ludington, E.; Jochelson, P.; Rogowski, R.; Roth, T. Efficacy and safety of doxepin 3 and 6 mg in a 35-day sleep laboratory trial in adults with chronic primary insomnia. Sleep 2011, 34, 1433–1442. [Google Scholar] [CrossRef] [Green Version]
- Mayer, G.; Wang-Weigand, S.; Roth-Schechter, B.; Lehmann, R.; Staner, C.; Partinen, M. Efficacy and safety of 6-month nightly ramelteon administration in adults with chronic primary insomnia. Sleep 2009, 32, 351–360. [Google Scholar] [CrossRef] [PubMed]
- Uchiyama, M.; Hamamura, M.; Kuwano, T.; Nagata, H.; Hashimoto, T.; Ogawa, A.; Uchimura, N. Long- term safety and efficacy of ramelteon in Japanese patients with chronic insomnia. Sleep Med. 2011, 12, 127–133. [Google Scholar] [CrossRef] [PubMed]
- Zammit, G.; Erman, M.; Wang-Weigand, S.; Sainati, S.; Zhang, J.; Roth, T. Evaluation of the efficacy and safety of ramelteon in subjects with chronic insomnia. J. Clin. Sleep Med. 2007, 3, 495–504, Erratum in J. Clin. Sleep Med. 2007, 3, table of contents. Erratum in J. Clin. Sleep Med. 2008, 4. [Google Scholar] [CrossRef]
- Roth, T.; Seiden, D.; Sainati, S.; Wang-Weigand, S.; Zhang, J.; Zee, P. Effects of ramelteon on patient- reported sleep latency in older adults with chronic insomnia. Sleep Med. 2006, 312–318. [Google Scholar] [CrossRef]
- Desyrel (trazodone) Prescribing Information. Pragma Pharmaceuticals, LLC. June 2017. (Prescription Data Source: Medical Expenditure Panel Survey (MEPS) 2013–2020. Agency for Healthcare Research and Quality) (AHRQ), Rockville, MD. ClinCalc DrugStats Database version 2022.08. Available online: https://clincalc.com/DrugStats/Top300Drugs.aspx (accessed on 2 February 2023).
- Parrino, L.; Spaggiari, M.C.; Boselli, M.; Di Giovanni, G.; Terzano, M.G. Clinical and polysomnographic effects of trazodone CR in chronic insomnia associated with dysthymia. Psychopharmacology (Berl) 1994, 116, 389–395. [Google Scholar] [CrossRef]
- Wichniak, A.; Wierzbicka, A.; Jernajczyk, W. Patients with insomnia and subthreshold depression show marked worsening of insomnia after discontinuation of sleep promoting medication. Prog. Neuropsychopharmacol. Biol. Psychiatry 2011, 35, 1671–1676. [Google Scholar] [CrossRef]
- Menza, M.A. Withdrawal syndrome in a depressed patient treated with trazodone. Am. J. Psychiatry 1986, 143, 1195. [Google Scholar] [CrossRef]
- Montalbetti, D.J.; Zis, A.P. Cholinergic rebound following trazodone withdrawal? J. Clin. Psychopharmacol. 1988, 73. [Google Scholar] [CrossRef]
- Otani, K.; Tanaka, O.; Kaneko, S.; Ishida, M.; Yasui, N.; Fukushima, Y. Mechanisms of the development of trazodone withdrawal symptoms. Int. Clin. Psychopharmacol. 1994, 9, 31–33. [Google Scholar] [CrossRef] [PubMed]
- Remeron (mirtazapine) Prescribing Information. Merck. 2020. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2020/020415s034s036,021208s024s026lbl.pdf (accessed on 1 February 2023).
- Ivgy-May, N.; Roth, T.; Ruwe, F.; Walsh, J. Esmirtazapine in non-elderly adult patients with primary insomnia: Efficacy and safety from a 2-week randomized outpatient trial. Sleep Med. 2015, 831–837. [Google Scholar] [CrossRef]
- Ivgy-May, N.; Ruwe, F.; Krystal, A.; Roth, T. Esmirtazapine in non-elderly adult patients with primary insomnia: Efficacy and safety from a randomized, 6-week sleep laboratory trial. Sleep Med. 2015, 16, 838–844. [Google Scholar] [CrossRef] [PubMed]
- Ivgy-May, N.; Hajak, G.; van Osta, G.; Braat, S.; Chang, Q.; Roth, T. Efficacy and safety of esmirtazapine in adult outpatients with chronic primary insomnia: A randomized, double-blind placebo-controlled study and open-label extension. J. Clin. Sleep Med. 2020, 16, 1455–1467. [Google Scholar] [CrossRef] [PubMed]
- Hajak, G.; Rodenbeck, A.; Voderholzer, U.; Riemann, D.; Cohrs, S.; Hohagen, F.; Berger, M.; Rüther, E. Doxepin in the treatment of primary insomnia: A placebo-controlled, double-blind, polysomnographic study. J. Clin. Psychiatry 2001, 62, 453–463. [Google Scholar] [CrossRef]
- Hohagen, F.; Montero, R.F.; Weiss, E.; Lis, S.; Schönbrunn, E.; Dressing, H.; Riemann, D.; Berger, M. Treatment of primary insomnia with trimipramine: An alternative to benzodiazepine hypnotics? Eur. Arch. Psychiatry Clin. Neurosci. 1994, 244, 65–72. [Google Scholar] [CrossRef]
- Riemann, D.; Voderholzer, U.; Cohrs, S.; Rodenbeck, A.; Hajak, G.; Rüther, E.; Wiegand, M.H.; Laakmann, G.; Baghai, T.; Fischer, W.; et al. Trimipramine in primary insomnia: Results of a polysomnographic double-blind controlled study. Pharmacopsychiatry 2002, 35, 165–174. [Google Scholar] [CrossRef] [PubMed]
- Monahan, K.; Cuzens-Sutton, J.; Siskind, D.; Kisely, S. Quetiapine withdrawal: A systematic review. Aust. N. Z. J. Psychiatry 2021, 55, 772–783. [Google Scholar] [CrossRef] [PubMed]
- Thurstone, C.C.; Alahi, P. A possible case of quetiapine withdrawal syndrome. J. Clin. Psychiatry 2000, 61, 602–603. [Google Scholar] [CrossRef] [Green Version]
- Kim, D.R.; Staab, J.P. Quetiapine discontinuation syndrome. Am. J. Psychiatry 2005, 162, 1020. [Google Scholar] [CrossRef]
- Seroquel (quetiapine) Prescribing Information. AstraZeneca. 2020. Available online: www.accessdata.fda.gov/drugsatfda_docs/label/2013/020639s061,022047s034lbl.pdf (accessed on 2 February 2023).
- Dilsaver, S.C.; Greden, J.F. Antidepressant withdrawal phenomena. Biol. Psychiatry 1984, 19, 237–256. [Google Scholar]
- Zwiebel, S.J.; Viguera, A.C. Discontinuing antidepressants: Pearls and pitfalls. Cleve Clin. J. Med. 2022, 89, 18–26. [Google Scholar] [CrossRef]
- Perlis, M.L.; Posner, D.; Riemann, D.; Bastien, C.H.; Teel, J.; Thase, M. Insomnia. Lancet 2022, 400, 1047–1060. [Google Scholar] [CrossRef]
- Petursson, H. The benzodiazepine withdrawal syndrome. Addiction 1994, 89, 1455–1459. [Google Scholar] [CrossRef] [PubMed]
- Pourshams, M.; Malakouti, S.K. Zolpidem abuse and dependency in an elderly patient with major depressive disorder: A case report. Daru 2014, 22, 54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davies, J.; Read, J. A systematic review into the incidence, severity and duration of antidepressant withdrawal effects: Are guidelines evidence-based? Addict. Behav. 2019, 97, 111–121. [Google Scholar] [CrossRef] [PubMed]
- Brandt, L.; Bschor, T.; Henssler, J.; Müller, M.; Hasan, A.; Heinz, A.; Gutwinski, S. Antipsychotic Withdrawal Symptoms: A Systematic Review and Meta-Analysis. Front. Psychiatry 2020, 11, 569912. [Google Scholar] [CrossRef] [PubMed]
- Mignot, E.; Mayleben, D.; Fietze, I.; Leger, D.; Zammit, G.; Bassetti, C.L.A.; Pain, S.; Seboek Kinter, D.; Roth, T.; Investigators. Safety and efficacy of daridorexant in patients with insomnia disorder: Results from two multicentre, randomised, double-blind, placebo-controlled, phase 3 trials. Lancet Neurol. 2022, 21, 125–139. [Google Scholar] [CrossRef]
- Kuntz, J.; Kouch, L.; Christian, D.; Peterson, P.L.; Gruss, I. Barriers and facilitators to the deprescribing of nonbenzodiazepine sedative medications among older adults. Perm. J. 2018, 22, 17–157. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Initial Drug/Group | No Change in Sleep on Discontinuation | Revert to Baseline or Improved over Baseline | Sleep Worse than Baseline Indicating Rebound | New Symptoms, e.g., Anxiety/ Seizures Indicating Withdrawal |
|---|---|---|---|---|
| Short-acting BZDs (e.g., triazolam) | Not on night 1 | May take several days | Yes | Anxiety, terminal insomnia may occur with use; more severe withdrawal/seizures may occur with abrupt withdrawal, particularly with higher doses |
| Mid-acting BZDs (e.g., temazepam) | More sleep disruption in some studies | Yes | Sometimes | Not usually at therapeutic doses; withdrawal/seizures may occur with higher doses, abrupt withdrawal |
| Long-acting BZDs (e.g., quazepam, flurazepam) | Yes | Yes | No | Not usually at therapeutic doses; withdrawal/seizures may occur with higher doses, abrupt withdrawal |
| Zolpidem | Not on night 1 | By the second night | For 1 night | Yes: traditional withdrawal symptoms observed only when using structured instruments. Seizures only with doses exceeding recommended amount. |
| Zaleplon | Mostly | Yes on night 1 | No | No |
| Eszopiclone | Not on night 1 | Yes on night 1 | Not generally | Yes when using structured instruments. No when getting spontaneous reports. |
| DORA—Suvorexant | For higher dosages than FDA approved, means worse than end of double-blind treatment but not tested statistically | For dosages higher than FDA approved, means remained better than baseline for 2 months after discontinuation but not tested statistically | 2/3 studies at doses above those used clinically | 2/3 studies at doses above those used clinically |
| DORA—Lemborexant | Significantly worse than end of double-blind treatment for two weeks after discontinuation for SOL, but for WASO, was only significantly worse than end of double-blind treatment for the first week. During the second week, the mean was higher but not above 95% confidence limits. | Significantly better for at least 2 weeks after discontinuation | No | No |
| DORA—Daridorexant | Average worse but not tested statistically | Significantly improved over baseline for at least 7 days after discontinuation | No | No |
| Ramelteon | Yes | Significantly improved over baseline for at least 7 nights | No | No |
| Doxepin | Means worse but not tested statistically | Improved over baseline for at least 2 nights | No | No |
| Trazodone | No | Yes | Yes | Nausea, sweating, irritability, agitation, dizziness, sensory disturbances, tremor, anxiety, confusion, headache, lethargy, hypomania, and seizures, among others |
| Mirtazapine | Yes | Yes | No | Dizziness, sensory disturbances, agitation, anxiety, fatigue, confusion, headache, tremor, nausea, vomiting, and sweating, among others |
| TCAs | Yes | Yes | No | Nausea, headache, malaise, irritability, and restlessness, among others |
| Quetiapine | No | No | Yes | Nausea, vomiting, agitation, restlessness, diaphoresis, irritability, anxiety, tachycardia, hypertension, and dizziness, among others |
| Initial Drug Class/Group | Consensus Recommendation for Different Class Switching | Grading of Evidence | Consensus Recommendation for Within-Class Switching | Grading of Evidence |
|---|---|---|---|---|
| BZDs | Slow taper method/cross taper | B /C | Direct switch | B |
| Zolpidem | Taper and then wait 1–2 days | B | Taper and then wait 1–2 days | B |
| Zaleplon | Direct switch | B | Direct switch | B |
| Eszopiclone | Taper and then wait 1–2 days | B | Taper and then wait 1–2 days | B |
| Suvorexant | Direct switch | B | Direct switch | B |
| Lemborexant | Direct switch | B | Direct switch | B |
| Daridorexant | Direct switch | B | Direct switch | B |
| Ramelteon | Direct switch | B | N/A | |
| Doxepin 3–6 mg | Direct switch | B | N/A | |
| Trazodone | Slow taper method /cross taper | D | Not recommended | E |
| Mirtazapine | Slow taper method /cross taper | E | Not recommended | E |
| TCAs | Slow taper method /cross taper | D | Not recommended | E |
| Quetiapine | Slow taper method /cross taper | D | Not recommended | E |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Watson, N.F.; Benca, R.M.; Krystal, A.D.; McCall, W.V.; Neubauer, D.N. Alliance for Sleep Clinical Practice Guideline on Switching or Deprescribing Hypnotic Medications for Insomnia. J. Clin. Med. 2023, 12, 2493. https://doi.org/10.3390/jcm12072493
Watson NF, Benca RM, Krystal AD, McCall WV, Neubauer DN. Alliance for Sleep Clinical Practice Guideline on Switching or Deprescribing Hypnotic Medications for Insomnia. Journal of Clinical Medicine. 2023; 12(7):2493. https://doi.org/10.3390/jcm12072493
Chicago/Turabian StyleWatson, Nathaniel F., Ruth M. Benca, Andrew D. Krystal, William V. McCall, and David N. Neubauer. 2023. "Alliance for Sleep Clinical Practice Guideline on Switching or Deprescribing Hypnotic Medications for Insomnia" Journal of Clinical Medicine 12, no. 7: 2493. https://doi.org/10.3390/jcm12072493