
Survival Outcomes in Squamous Cell Carcinoma of the External Auditory Canal: A Systematic Review and Meta-Analysis

 , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Selection Criteria
2.3. Data Extraction and Quality Assessment
2.4. Statistical Analysis
3. Results
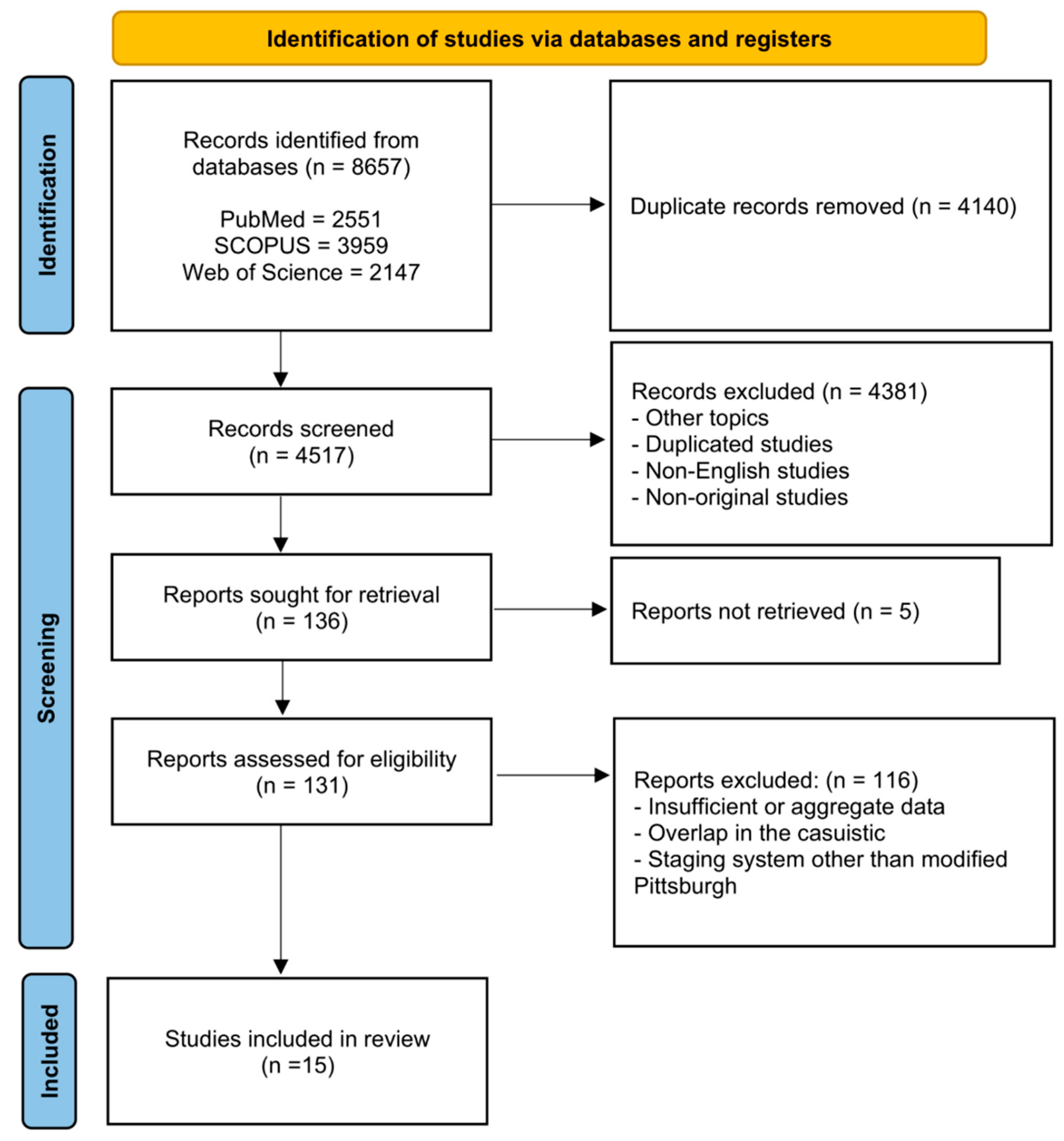
3.1. Search Results and Quality Assessment
3.2. Characteristics of the Studies and Pooled Analysis
3.3. Meta-Analysis for cT Category
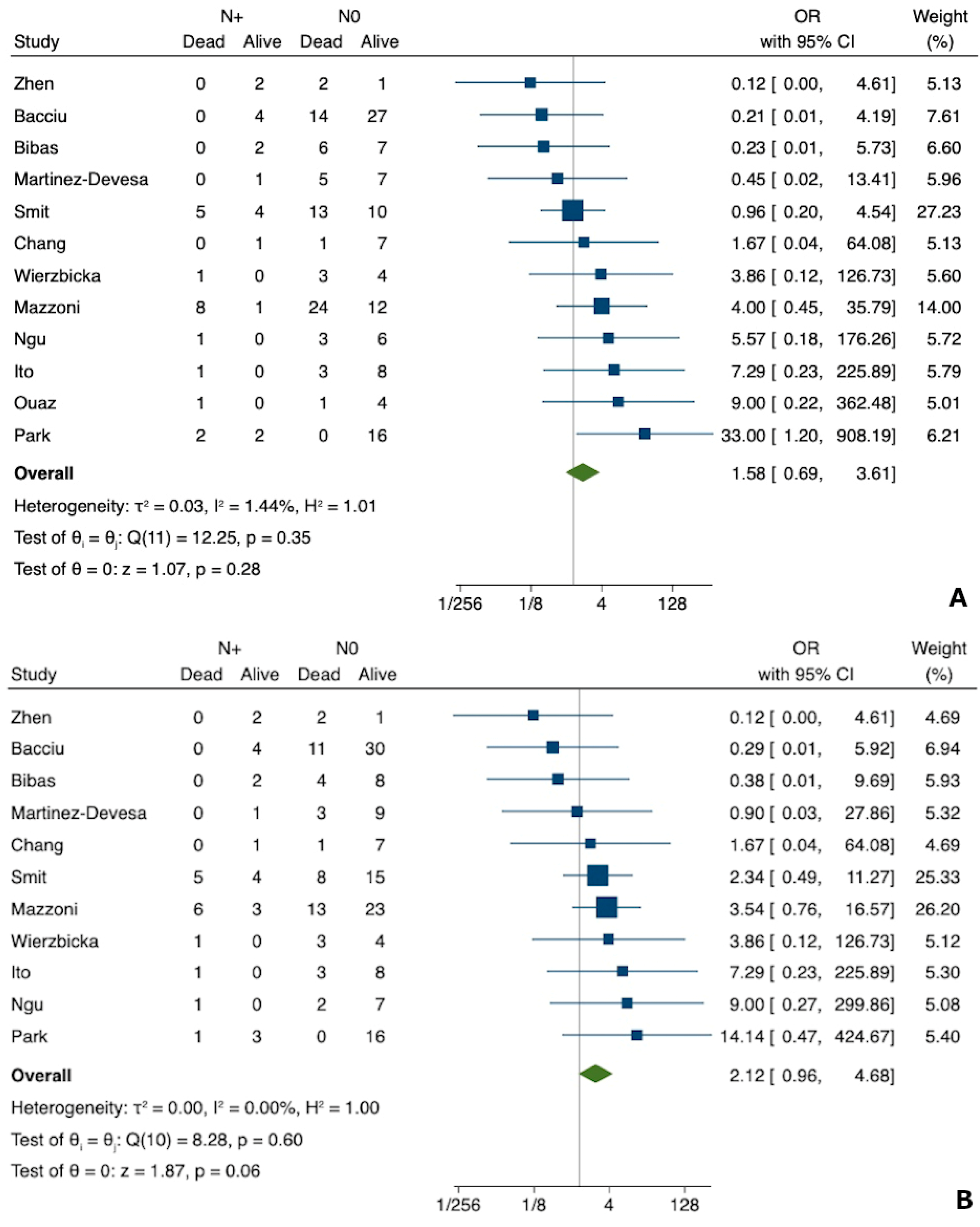
3.4. Meta-Analysis for N Status
4. Discussion
4.1. Summary of Findings
4.2. Comparison with Other Studies
4.3. Principles of Treatment in SCC of the EAC
4.4. Clinical Relevance
4.5. Strengths and Limitations of the Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lovin, B.D.; Gidley, P.W. Squamous cell carcinoma of the temporal bone: A current review. Laryngoscope Investig. Otolaryngol. 2019, 4, 684–692. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lionello, M.; Stritoni, P.; Facciolo, M.C.; Staffieri, A.; Martini, A.; Mazzoni, A.; Zanoletti, E.; Marioni, G. Temporal bone carcinoma. Current diagnostic, therapeutic, and prognostic concepts. J. Surg. Oncol. 2014, 110, 383–392. [Google Scholar] [CrossRef] [PubMed]
- Zanoletti, E.; Marioni, G.; Stritoni, P.; Lionello, M.; Giacomelli, L.; Martini, A.; Mazzoni, A. Temporal bone squamous cell carcinoma: Analyzing prognosis with univariate and multivariate models. Laryngoscope 2014, 124, 1192–1198. [Google Scholar] [CrossRef] [PubMed]
- Mazzoni, A.; Cazzador, D.; Marioni, G.; Zanoletti, E. Treatment of advanced squamous cell carcinoma of the external auditory canal: Critical analysis of persistent failures in diagnosis and surgery with a competing-risk model. Head Neck. 2022, 44, 1918–1926. [Google Scholar] [CrossRef]
- Marioni, G.; Mazzoni, A.; Zanoletti, E. Histopathology-related pitfalls in temporal bone malignancy prognostics. Auris Nasus Larynx. 2019, 46, 958–959. [Google Scholar] [CrossRef]
- Franz, L.; Zanoletti, E.; Mazzoni, A.; Marioni, G. Histological type homogeneity: A cornerstone in analyzing temporal bone malignancies data. Eur. Arch. Otorhinolaryngol. 2020, 277, 3233–3234. [Google Scholar] [CrossRef]
- Morris, L.G.; Mehra, S.; Shah, J.P.; Bilsky, M.H.; Selesnick, S.H.; Kraus, D.H. Predictors of survival and recurrence after temporal bone resection for cancer. Head Neck. 2021, 34, 1231–1239. [Google Scholar] [CrossRef]
- Hayashi, K.; Koto, M.; Demizu, Y.; Saitoh, J.I.; Suefuji, H.; Okimoto, T.; Ohno, T.; Shioyama, Y.; Takagi, R.; Ikawa, H.; et al. A retrospective multicenter study of carbon-ion radiotherapy for external auditory canal and middle ear carcinomas. Cancer Med. 2019, 8, 51–57. [Google Scholar] [CrossRef]
- Seligman, K.L.; Sun, D.Q.; Ten Eyck, P.P.; Schularick, N.M.; Hansen, M.R. Temporal bone carcinoma: Treatment patterns and survival. Laryngoscope. 2020, 130, E11–E20. [Google Scholar] [CrossRef]
- Arriaga, M.; Curtin, H.; Takahashi, H.; Hirsch, B.E.; Kamerer, D.B. Staging proposal for external meatus carcinoma based on preoperative clinical examination and computed tomography findings. Ann. Otol. Rhinol. Laryngol. 1990, 99, 714–721. [Google Scholar] [CrossRef]
- Moody, S.A.; Hirsch, B.E.; Myers, E.N. Squamous cell carcinoma of the external auditory canal: An evaluation of a staging system. Am. J. Otol. 2000, 21, 582–588. [Google Scholar] [PubMed]
- Califano, J.A.; Lydiatt, W.M.; Nehal, K.S.; O’Sullivan, B.; Schmults, C.; Seethala, R.R.; Weber, R.S.; Shah, J.P. Cutaneous Squamous Cell Carcinoma of the Head and Neck, 8th ed.; Amin, M., Edge, S., Greene, F., Eds.; AJCC Cancer Staging Manual; Springer: Berlin/Heidelberg, Germany, 2017; pp. 171–181. [Google Scholar]
- Lavieille, J.; Reyt, E.; Boulat, E.; Righini, C.; Schmerber, S.; Charachon, R. Cancers du conduit auditif externe et de l’oreille moyenne: Indications chirurgicales et nouvelles classification. JFORL 1997, 46, 357–362. [Google Scholar]
- Stell, P.M.; McCormick, M.S. Carcinoma of the external auditory meatus and middle ear. Prognostic factors and a suggested staging system. J. Laryngol. Otol. 1985, 99, 847–850. [Google Scholar] [CrossRef] [PubMed]
- Mazzoni, A.; Zanoletti, E.; Marioni, G.; Martini, A. En bloc temporal bone resections in squamous cell carcinoma of the ear. Technique, principles, and limits. Acta Otolaryngol. 2016, 136, 425–432. [Google Scholar] [CrossRef] [Green Version]
- Zanoletti, E.; Lovato, A.; Stritoni, P.; Martini, A.; Mazzoni, A.; Marioni, G. A critical look at persistent problems in the diagnosis, staging and treatment of temporal bone carcinoma. Cancer Treat. Rev. 2015, 41, 821–826. [Google Scholar] [CrossRef]
- Oya, R.; Takenaka, Y.; Takemura, K.; Ashida, N.; Shimizu, K.; Kitamura, T.; Yamamoto, Y.; Uno, A. Surgery with or without postoperative radiation therapy for early-stage external auditory canal squamous cell carcinoma: A meta-analysis. Otol. Neurotol. 2017, 38, 1333–1338. [Google Scholar] [CrossRef]
- Kiyokawa, Y.; Ariizumi, Y.; Ohno, K.; Ito, T.; Kawashima, Y.; Tsunoda, A.; Kishimoto, S.; Asakage, T.; Tsutsumi, T. Indications for and extent of elective neck dissection for lymph node metastasis from external auditory canal carcinoma. Auris Nasus Larynx. 2021, 48, 745–750. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Wells, G.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. 2014. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 18 January 2023).
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [Green Version]
- Choi, J.Y.; Choi, E.C.; Lee, H.K.; Yoo, J.B.; Kim, S.G.; Lee, W.S. Mode of parotid involvement in external auditory canal carcinoma. J. Laryngol. Otol. 2003, 117, 951–954. [Google Scholar] [CrossRef]
- Martinez-Devesa, P.; Barnes, M.L.; Milford, C.A. Malignant tumors of the ear and temporal bone: A study of 27 patients and review of their management. Skull Base 2008, 18, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bibas, A.G.; Ward, V.; Gleeson, M.J. Squamous cell carcinoma of the temporal bone. J. Laryngol. Otol. 2008, 122, 1156–1161. [Google Scholar] [CrossRef] [PubMed]
- Kunst, H.; Lavieille, J.P.; Marres, H. Squamous cell carcinoma of the temporal bone: Results and management. Otol. Neurotol. 2008, 29, 549–552. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.H.; Shu, M.T.; Lee, J.C.; Leu, Y.S.; Chen, Y.C.; Lee, K.S. Treatments and outcomes of malignant tumors of external auditory canal. Am. J. Otolaryngol. 2009, 30, 44–48. [Google Scholar] [CrossRef] [PubMed]
- Ito, M.; Hatano, M.; Yoshizaki, T. Prognostic factors for squamous cell carcinoma of the temporal bone: Extensive bone involvement or extensive soft tissue involvement? Acta Otolaryngol. 2009, 129, 1313–1319. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bacciu, A.; Clemente, I.A.; Piccirillo, E.; Ferrari, S.; Sanna, M. Guidelines for treating temporal bone carcinoma based on long-term outcomes. Otol. Neurotol. 2013, 34, 898–907. [Google Scholar] [CrossRef]
- Ouaz, K.; Robier, A.; Lescanne, E.; Bobillier, C.; Morinière, S.; Bakhos, D. Cancer of the external auditory canal. Eur. Ann. Otorhinolaryngol. Head Neck Dis. 2013, 130, 175–182. [Google Scholar] [CrossRef] [Green Version]
- Zhen, S.; Fu, T.; Qi, J. Diagnosis and treatment of carcinoma in external auditory canal. J. Otol. 2014, 9, 146–150. [Google Scholar] [CrossRef] [Green Version]
- Wierzbicka, M.; Kopeć, T.; Szyfter, W.; Buczkowska, A.; Borucki, Ł. Efficacy of petrosectomy in malignant invasion of the temporal bone. Br. J. Oral Maxillofac. Surg. 2016, 54, 778–783. [Google Scholar] [CrossRef]
- Park, J.M.; Kong, J.S.; Chang, K.H.; Jun, B.C.; Jeon, E.J.; Park, S.Y. The clinical characteristics and surgical outcomes of carcinoma of the external auditory canal: A multicenter study. J. Int. Adv. Otol. 2018, 14, 278–284. [Google Scholar] [CrossRef]
- Ngu, C.Y.V.; Mohd Saad, M.S.; Tang, I.P. Temporal bone squamous cell carcinoma: A change in treatment. Med. J. Malaysia 2021, 76, 725–730. [Google Scholar] [PubMed]
- Saijo, K.; Ueki, Y.; Tanaka, R.; Yokoyama, Y.; Omata, J.; Takahashi, T.; Ota, H.; Shodo, R.; Yamazaki, K.; Togashi, T.; et al. Treatment outcome of external auditory canal carcinoma: The utility of lateral temporal bone resection. Front. Surg. 2021, 8, 708245. [Google Scholar] [CrossRef] [PubMed]
- Smit, C.F.; de Boer, N.; Lissenberg-Witte, B.I.; Merkus, P.; Hensen, E.F.; Leemans, C.R. Surgical treatment for squamous cell carcinoma of the temporal bone: Predictors of survival. Acta Otorhinolaryngol. Ital. 2021, 41, 308–316. [Google Scholar] [CrossRef] [PubMed]
- McCracken, M.; Pai, K.; Cabrera, C.I.; Johnson, B.R.; Tamaki, A.; Gidley, P.W.; Manzoor, N.F. Temporal bone resection for squamous cell carcinoma of the lateral skull base: Systematic review and meta-analysis. Otolaryngol. Head Neck Surg. 2022, 168, 154–164. [Google Scholar] [CrossRef] [PubMed]
- Lechner, M.; Sutton, L.; Murkin, C.; Masterson, L.; O’Flynn, P.; Wareing, M.J.; Tatla, T.; Saeed, S. Squamous cell cancer of the temporal bone: A review of the literature. Eur. Arch. Otorhinolaryngol. 2021, 278, 2225–2228. [Google Scholar] [CrossRef]
- Borsetto, D.; Vijendren, A.; Franchin, G.; Donnelly, N.; Axon, P.; Smith, M.; Masterson, L.; Bance, M.; Saratziotis, A.; Polesel, J.; et al. Prevalence of occult nodal metastases in squamous cell carcinoma of the temporal bone: A systematic review and meta-analysis. Eur. Arch. Otorhinolaryngol. 2022, 279, 5573–5581. [Google Scholar] [CrossRef]
- Zanoletti, E.; Marioni, G.; Nicolai, P.; Mazzoni, A. The contribution of oncological lateral skull base surgery to the management of advanced head-neck tumors. Acta Oto-Laryngol. 2023, 143, 101–105. [Google Scholar] [CrossRef]
- Komune, N.; Kuga, D.; Matsuo, S.; Miyazaki, M.; Noda, T.; Sato, K.; Hongo, T.; Koike, K.; Uchi, R.; Kogo, R.; et al. Clinical analysis of en bloc resection for advanced temporal bone squamous cell carcinoma. J. Neurol. Surg. B Skull Base 2021, 83 (Suppl. S2), e40–e48. [Google Scholar] [CrossRef]
- Zanoletti, E.; Danesi, G. The problem of nodal disease in squamous cell carcinoma of the temporal bone. Acta Otolaryngol. 2010, 130, 913–916. [Google Scholar] [CrossRef]
- Zhang, T.; Li, W.; Dai, C.; Chi, F.; Wang, S.; Wang, Z. Evidence-based surgical management of T1 or T2 temporal bone malignancies. Laryngoscope 2013, 123, 244–248. [Google Scholar] [CrossRef]
- Pfreundner, L.; Schwager, K.; Willner, J.; Baier, K.; Bratengeier, K.; Brunner, F.X.; Flentje, M. Carcinoma of the external auditory canal and middle ear. Int. J Radiat. Oncol. Biol Phys. 1999, 44, 777–788. [Google Scholar] [CrossRef] [PubMed]
- Prabhu, R.; Hinerman, R.W.; Indelicato, D.J.; Morris, C.G.; Werning, J.W.; Vaysberg, M.; Amdur, R.J.; Kirwan, J.; Mendenhall, W.M. Squamous cell carcinoma of the external auditory canal: Long-term clinical outcomes using surgery and external-beam radiotherapy. Am. J Clin. Oncol. 2009, 32, 401–404. [Google Scholar] [CrossRef] [PubMed]
- Laskar, S.G.; Sinha, S.; Pai, P.; Nair, D.; Budrukkar, A.; Swain, M.; Kumar, A.; Moiyadi, A.; Shetty, P.; Ray, V.; et al. Definitive and adjuvant radiation therapy for external auditory canal and temporal bone squamous cell carcinomas: Long term outcomes. Radiother. Oncol. 2022, 170, 151–158. [Google Scholar] [CrossRef] [PubMed]
- Zanoletti, E.; Marioni, G.; Franchella, S.; Lovato, A.; Giacomelli, L.; Martini, A.; Mazzoni, A. Recurrent squamous cell carcinoma of the temporal bone: Critical analysis of cases with a poor prognosis. Am. J Otolaryngol. 2015, 36, 352–355. [Google Scholar] [CrossRef]
- Zhong, S.; Zuo, W. Treatment strategies for malignancies of the external auditory canal. Curr Treat Options Oncol. 2022, 23, 43–53. [Google Scholar] [CrossRef]
- Zhang, T.; Dai, C.; Wang, Z. The misdiagnosis of external auditory canal carcinoma. Eur. Arch. Otorhinolaryngol. 2013, 270, 1607–1613. [Google Scholar] [CrossRef]
- Wang, Z.; Zheng, M.; Xia, S. The contribution of CT and MRI in staging, treatment planning and prognosis prediction of malignant tumors of external auditory canal. Clin. Imaging. 2016, 40, 1262–1268. [Google Scholar] [CrossRef]
- The International Collaboration for Cancer Classification and Research. Available online: https://ic3r.iarc.who.int/ (accessed on 7 February 2023).
- Riley, R.D.; Jackson, D.; Salanti, G.; Burke, D.L.; Price, M.; Kirkham, J.; White, I.R. Multivariate and network meta-analysis of multiple outcomes and multiple treatments: Rationale, concepts, and examples. BMJ 2017, 358, j3932. [Google Scholar] [CrossRef] [Green Version]
- White, I.R.; Barrett, J.K.; Jackson, D.; Higgins, J.P. Consistency and inconsistency in network meta-analysis: Model estimation using multivariate meta-regression. Res. Synth. Methods 2012, 3, 111–125. [Google Scholar] [CrossRef] [Green Version]
- Zanoletti, E.; Franz, L.; Favaretto, N.; Cazzador, D.; Franchella, S.; Calvanese, L.; Nicolai, P.; Mazzoni, A.; Marioni, G. Primary temporal bone squamous cell carcinoma: Comparing the prognostic value of the American Joint Committee on Cancer TNM classification (8th edition) with the revised Pittsburgh staging system. Head Neck 2022, 44, 889–896. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Year of Publication | Country | Total Number Patients | Number of Patients Included in the Meta-Analysis * | Study Design |
|---|---|---|---|---|---|
| Choi et al. [22] | 2003 | Korea | 21 | 11 | CS |
| Martinez-Devesa et al. [23] | 2007 | UK | 27 | 13 | CS |
| Bibas et al. [24] | 2008 | UK | 17 | 15 | CS |
| Kunst et al. [25] | 2008 | Netherlands–France | 28 | 28 | CS |
| Chang et al. [26] | 2009 | China | 12 | 9 | CS |
| Ito et al. [27] | 2009 | Japan | 16 | 12 | CS |
| Bacciu et al. [28] | 2013 | Italy | 45 | 45 | CS |
| Ouaz et al. [29] | 2013 | France | 10 | 6 | CS |
| Zhen et al. [30] | 2014 | China | 16 | 5 | CS |
| Wierzbicka et al. [31] | 2016 | Poland | 20 | 8 | CS |
| Park et al. [32] | 2018 | Korea | 31 | 20 | CS |
| Ngu et al. [33] | 2021 | Malaysia | 10 | 10 | CS |
| Sajio et al. [34] | 2021 | Japan | 52 | 23 | CS |
| Smit et al. [35] | 2021 | Netherlands | 49 | 32 | CS |
| Mazzoni et al. [4] | 2022 | Italy | 45 | 45 | CS |
| Variable | N (%) |
|---|---|
| Patients | 282 |
| Age, mean ± SD, years | 61.2 ± 13.2 |
| Sex Male Female Missing | 131 (46.5) 108 (38.3) 43 (15.2) |
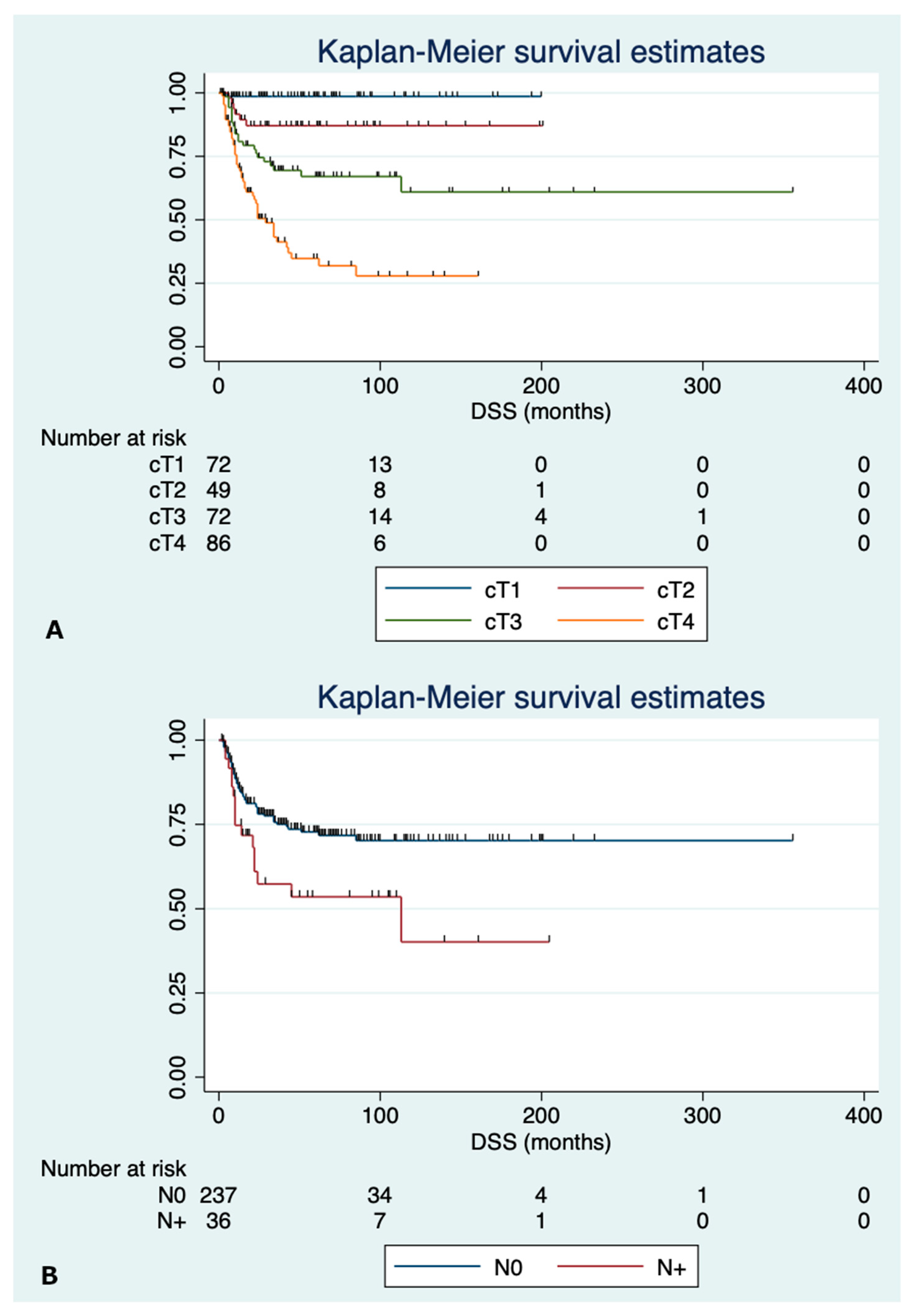
| cT category 1 2 3 4 | 72 (25.5) 49 (17.4) 75 (26.6) 86 (30.5) |
| N category N0 N+ Missing | 240 (85.1) 36 (12.8) 6 (2.1) |
| Type of surgical resection SR LTBR STBR TTBR | 31 (11.0) 154 (54.6) 87 (30.9) 10 (3.5) |
| Neck dissection No Yes Missing | 149 (52.8) 99 (35.1) 34 (12.1) |
| Parotidectomy No Yes Missing | 117 (41.5) 149 (52.8) 16 (5.7) |
| Surgical margins Negative Positive Missing | 86 (30.5) 72 (25.5) 124 (44.0) |
| Adjuvant treatments None RT CRT Missing | 80 (28.4) 195 (69.1) 6 (2.1) 1 (0.4) |
| Patterns of recurrence Local Nodal Distant | 91 (32.3) 11 (3.9) 2 (0.7) |
| Survival NED AWD DOD DOC | 159 (56.4) 15 (5.3) 79 (28.0) 29 (10.3) |
| Survival time, mean ± SD, months | 50.8 ± 51.8 |
| Variable | Univariate Analysis | Multivariable Analysis * | ||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p-Value | HR | 95% CI | p-Value | |
| Age, years ≤62 >62 | 0.83 Ref. | 0.51–1.36 - | 0.47 - | |||
| Sex Male Female | Ref. 1.28 | - 0.76–2.16 | - 0.35 | |||
| cT category 1 2 3 4 | Ref. 1.35 2.68 5.76 | - 0.59–3.05 1.35–5.25 3.06–10.8 | - 0.47 0.004 <0.001 | Ref. 1.33 2.65 5.51 | - 0.58–3.02 1.34–5.22 2.76–10.5 | - 0.5 0.005 <0.001 |
| N category N0 N+ | Ref. 1.71 | - 1.05–2.80 | - 0.03 | Ref. 1.09 | - 0.66–1.80 | - 0.74 |
| Type of surgical resection SR LTBR STBR/TTBR | Ref. 1.78 4.65 | - 0.71–4.50 1.86–11.6 | - 0.22 0.001 | |||
| Surgical margins Negative Positive | Ref. 2.38 | - 1.36–4.16 | - 0.002 | |||
| Adjuvant treatments None RT/CRT | Ref. 1.60 | - 0.99–2.55 | - 0.052 | |||
| Variable | Univariate Analysis | Multivariable Analysis * | ||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p-Value | HR | 95% CI | p-Value | |
| Age, years ≤62 >62 | 1.20 Ref. | 0.71–2.05 - | 0.49 - | |||
| Sex Male Female | Ref. 1.37 | - 0.78–2.40 | - 0.27 | |||
| cT category 1 2 3 4 | Ref. 8.99 24.4 58.8 | - 1.08–74.7 3.29–181.1 8.10–426.4 | - 0.042 0.002 <0.001 | Ref. 8.90 23.8 56.0 | - 1.07–73.9 3.20–177.8 7.67–409.1 | - 0.043 0.002 <0.001 |
| N category N0 N+ | Ref. 1.97 | - 1.13–3.42 | - 0.017 | Ref. 1.07 | - 0.61–1.87 | - 0.81 |
| Type of surgical resection SR LTBR STBR/TTBR | Ref. 1.85 6.85 | - 0.56–6.10 2.13–22.0 | - 0.31 0.001 | |||
| Surgical margins Negative Positive | Ref. 3.55 | - 1.85–6.84 | - <0.001 | |||
| Adjuvant treatments None RT/CRT | Ref. 2.33 | - 1.26–4.31 | - 0.007 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cazzador, D.; Franz, L.; Tealdo, G.; Carobbio, A.L.C.; Ferraro, M.; Mazzoni, A.; Marioni, G.; Zanoletti, E. Survival Outcomes in Squamous Cell Carcinoma of the External Auditory Canal: A Systematic Review and Meta-Analysis. J. Clin. Med. 2023, 12, 2490. https://doi.org/10.3390/jcm12072490
Cazzador D, Franz L, Tealdo G, Carobbio ALC, Ferraro M, Mazzoni A, Marioni G, Zanoletti E. Survival Outcomes in Squamous Cell Carcinoma of the External Auditory Canal: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2023; 12(7):2490. https://doi.org/10.3390/jcm12072490
Chicago/Turabian StyleCazzador, Diego, Leonardo Franz, Giulia Tealdo, Andrea Luigi Camillo Carobbio, Maria Ferraro, Antonio Mazzoni, Gino Marioni, and Elisabetta Zanoletti. 2023. "Survival Outcomes in Squamous Cell Carcinoma of the External Auditory Canal: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 12, no. 7: 2490. https://doi.org/10.3390/jcm12072490