
Opioids in the Treatment of Chronic Idiopathic Diarrhea in Humans—A Systematic Review and Treatment Guideline
 , , and
, , and
Abstract
:1. Introduction
2. Methods
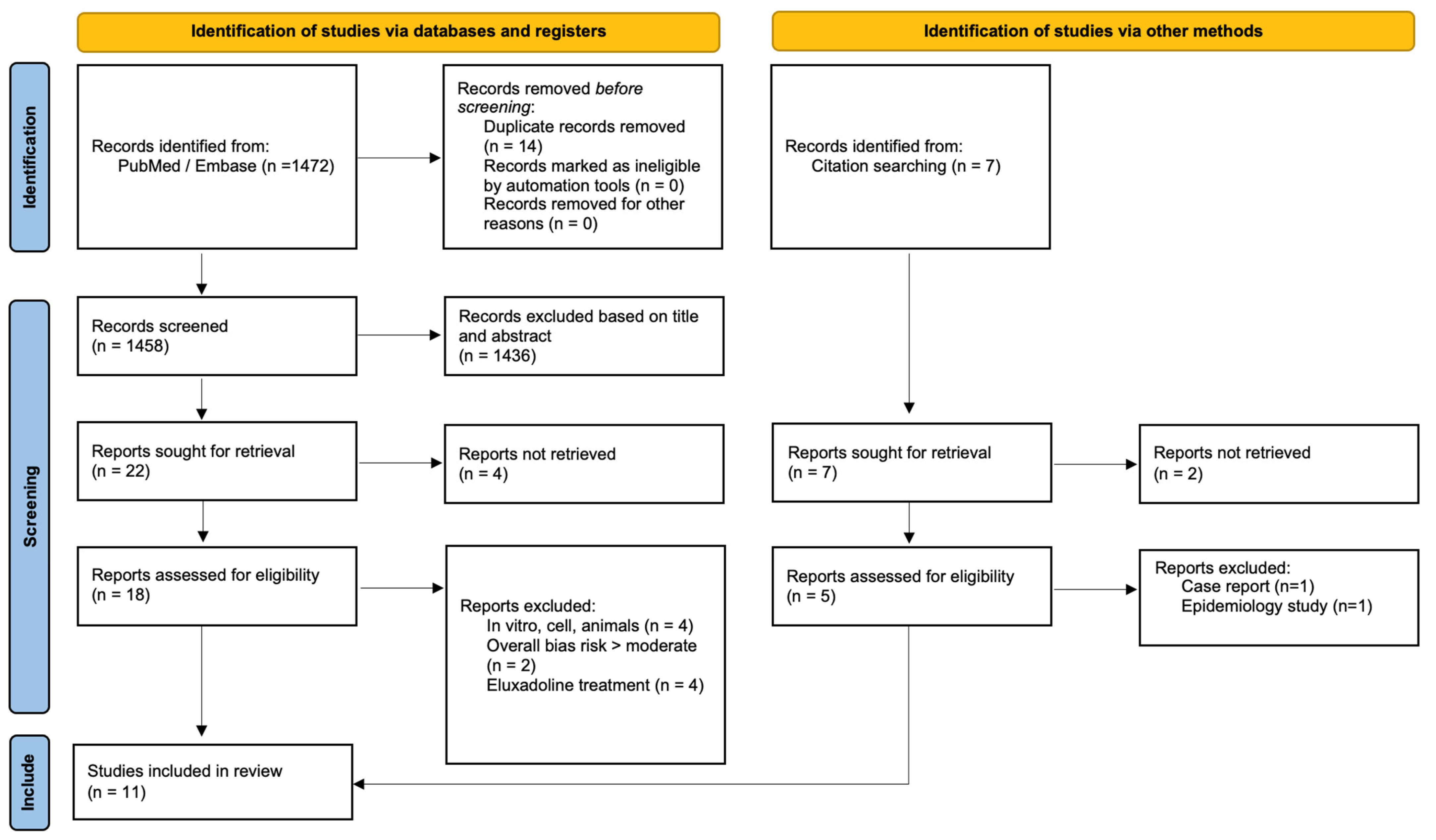
2.1. Search Strategy
2.2. Inclusion Criteria
2.3. Exclusion Criteria
2.4. Data Extraction
2.5. Quality Assessment
3. Results
3.1. Opioid Receptor Agonist Effects on Bowel Movement Frequency
3.2. Opioid Receptor Agonist Effects on Transit Time
3.3. Opioid Receptor Agonist Effects on Stool Consistency
3.4. Opioid Receptor Agonist Effect on Subjective Improvement
3.5. Adverse Effects
4. Discussion
4.1. Opioid Agonistic Effects on the Gastrointestinal Tract
4.2. Safety and Potential for Abuse
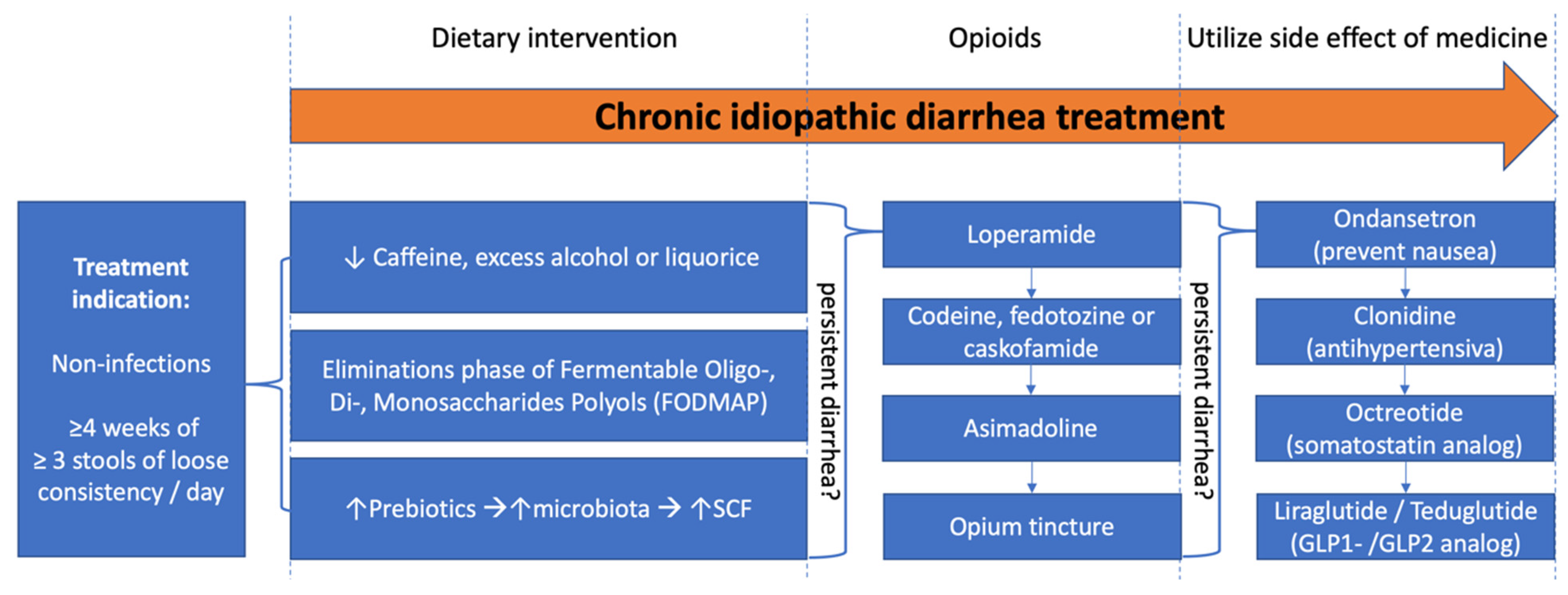
4.3. Guidelines for Treatment of Chronic Idiopathic Diarrhea
4.4. Strengths and Limitation
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Chu, C.; Rotondo-Trivette, S.; Michail, S. Chronic diarrhea. Curr. Probl. Pediatr. Adolesc. Health Care 2020, 50, 100841. [Google Scholar] [CrossRef]
- Schiller, L.R. Evaluation of chronic diarrhea and irritable bowel syndrome with diarrhea in adults in the era of precision medicine. Am. J. Gastroenterol. 2018, 113, 660–669. [Google Scholar] [CrossRef] [PubMed]
- Mönnikes, H. Quality of life in patients with irritable bowel syndrome. J. Clin. Gastroenterol. 2011, 45 (Suppl. 2), S98–S101. [Google Scholar] [CrossRef]
- Talley, N.J.; Zinsmeister, A.R.; Melton, L.J. Irritable Bowel Syndrome in a Community: Symptom Subgroups, Risk Factors, and Health Care Utilization. Am. J. Epidemiol. 1995, 142, 76–83. [Google Scholar] [CrossRef]
- Schiller, L.R.; Pardi, D.S.; Sellin, J.H. Chronic Diarrhea: Diagnosis and Management. Clin. Gastroenterol. Hepatol. 2017, 15, 182–193.e3. [Google Scholar] [CrossRef] [Green Version]
- Camilleri, M. What’s new in functional and motility disorders in the lower GI tract? Malta Med. J. 2017, 29, 3–13. Available online: https://www.embase.com/search/results?subaction=viewrecord&id=L618521852&from=export (accessed on 12 December 2022).
- Kurz, A.; Sessler, D.I. Opioid-induced bowel dysfunction: Pathophysiology and potential new therapies. Drugs 2003, 63, 649–671. [Google Scholar] [CrossRef] [PubMed]
- Sternini, C.; Patierno, S.; Selmer, I.S.; Kirchgessner, A. The opioid system in the gastrointestinal tract. Neurogastroenterol. Motil. 2004, 16 (Suppl. 2), 3–16. [Google Scholar] [CrossRef]
- Holzer, P. Treatment of opioid-induced gut dysfunction. Expert Opin. Investig. Drugs 2007, 16, 181–194. [Google Scholar] [CrossRef] [PubMed]
- Holden, J.E.; Jeong, Y.; Forrest, J.M. The endogenous opioid system and clinical pain management. AACN Clin. Issues 2005, 16, 291–301. [Google Scholar] [CrossRef]
- Holzer, P. Opioid receptors in the gastrointestinal tract. Regul. Pept. 2009, 155, 11–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Drewes, A.M.; Munkholm, P.; Simrén, M.; Breivik, H.; Kongsgaard, U.E.; Hatlebakk, J.G.; Agreus, L.; Friedrichsen, M.; Christrup, L.L. Definition, diagnosis and treatment strategies for opioid-induced bowel dysfunction-Recommendations of the Nordic Working Group. Scand. J. Pain 2016, 11, 111–122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Drossman, D.A.; Hasler, W.L. Rome IV-Functional GI Disorders: Disorders of Gut-Brain Interaction. Gastroenterology 2016, 150, 1257–1261. [Google Scholar] [CrossRef]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yeoh, E.K.; Horowitz, M.; Russo, A.; Muecke, T.; Robb, T.; Chatterton, B.E. Gastrointestinal function in chronic radiation enteritis-effects of loperamide-N-oxide. Gut 1993, 34, 476–482. [Google Scholar] [CrossRef] [Green Version]
- Mainguet, P.; Fiasse, R. Double blind placebo controlled study of loperamide (Imodium) in chronic diarrhoea caused by ileocolic disease or resection. Gut 1977, 18, 575–579. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Read, M.; Read, N.W.; Barber, D.C.; Duthie, H.L. Effects of loperamide on anal sphincter function in patients complaining of chronic diarrhea with fecal incontinence and urgency. Dig. Dis. Sci. 1982, 27, 807–814. [Google Scholar] [CrossRef]
- Efskind, P.S.; Bernklev, T.; Vatn, M.H. A double-blind placebo-controlled trial with loperamide in irritable bowel syndrome. Scand. J. Gastroenterol. 1996, 31, 463–468. [Google Scholar] [CrossRef]
- Bengt Lävo, B.; Stenstam, M.; Nielsen, A.L. Loperamide in treatment of irritable bowel syndrome–A double-blind placebo controlled study. Scand. J. Gastroenterol. 1987, 22, 77–80. [Google Scholar] [CrossRef]
- Cann, P.A.; Read, N.W.; Holdsworth, C.D.; Barends, D. Role of loperamide and placebo in management of irritable bowel syndrome (IBS). Dig. Dis. Sci. 1984, 29, 239–247. [Google Scholar] [CrossRef] [PubMed]
- Pelemans, W.; Vantrappen, G. A Double Blind Crossover Comparison of Loperamide with Diphenoxylate in the Symptomatic Treatment of Chronic Diarrhea. Gastroenterology 1976, 70, 1030–1034. [Google Scholar] [CrossRef]
- Mangel, A.W.; Bornstein, J.D.; Hamm, L.R.; Buda, J.; Wang, J.; Irish, W.; Urso, D. Clinical trial: Asimadoline in the treatment of patients with irritable bowel syndrome. Aliment. Pharmacol. Ther. 2008, 28, 239–249. [Google Scholar] [CrossRef] [PubMed]
- Barrow, L.; Steed, K.P.; Spiller, R.C.; Maskell, N.A.; Brown, J.K.; Watts, P.J.; Melia, C.D.; Davies, M.C.; Wilson, C.G. Quantitative, noninvasive assessment of antidiarrheal actions of codeine using an experimental model of diarrhea in man. Dig. Dis. Sci. 1993, 38, 996–1003. [Google Scholar] [CrossRef] [PubMed]
- Schulte-Frohlinde, E.; Reindl, W.; Bierling, D.; Lersch, C.; Brantl, V.; Teschemacher, H.; Schusdziarra, V. Effects of oral casokefamide on plasma levels, tolerance, and intestinal transit in man. Peptides 2000, 21, 439–442. [Google Scholar] [CrossRef]
- Lewis, S.J.; Heaton, K.W. Stool form scale as a useful guide to intestinal transit time. Scand. J. Gastroenterol. 1997, 32, 920–924. [Google Scholar] [CrossRef]
- Mangel, A.W.; Fehnel, S.E. Design of treatment trials in irritable bowel syndrome: Opioid agonists and atypical benzodiazepine antagonists. Neurogastroenterol. Motil. 2008, 20, 1086–1093. [Google Scholar] [CrossRef]
- Dapoigny, M.; Abitbol, J.-L.; Fraitag, B. Efficacy of peripheral kappa agonist fedotozine versus placebo in treatment of irritable bowel syndrome: A multicenter dose-response study. Dig. Dis. Sci. 1995, 40, 2244–2249. [Google Scholar] [CrossRef] [PubMed]
- Crockett, S.D.; Greer, K.B.; Heidelbaugh, J.J.; Falck-Ytter, Y.; Hanson, B.J.; Sultan, S. American Gastroenterological Association Institute Guideline on the Medical Management of Opioid-Induced Constipation. Gastroenterology 2019, 156, 218–226. [Google Scholar] [CrossRef] [Green Version]
- Thomas, J. Opioid-Induced Bowel Dysfunction. J. Pain Symptom Manag. 2008, 35, 103–113. [Google Scholar] [CrossRef]
- Barrett, K.E.; Keely, S.J. Chloride secretion by the intestinal epithelium: Molecular basis and regulatory aspects. Annu. Rev. Physiol. 2000, 62, 535–572. [Google Scholar] [CrossRef]
- Galligan, J.J.; Akbarali, H.I. Molecular Physiology of Enteric Opioid Receptors. Am. J. Gastroenterol. Suppl. 2014, 2, 17–21. [Google Scholar] [CrossRef] [PubMed]
- Galligan, J.J.; North, R.A. Pharmacology and function of nicotinic acetylcholine and P2X receptors in the enteric nervous system. Neurogastroenterol. Motil. 2004, 16 (Suppl. 1), 64–70. [Google Scholar] [CrossRef] [PubMed]
- Gerok, W. Pathophysiology of chronic diarrhea. Praxis 2000, 89, 1635–1641. [Google Scholar] [PubMed]
- Kromer, W. Endogenous and exogenous opioids in the control of gastrointestinal motility and secretion. Pharmacol. Rev. 1988, 40, 121–162. [Google Scholar] [PubMed]
- Glad, H.; Ainsworth, M.A.; Svendsen, P.; Fahrenkrug, J.; Schaffalitzky De Muckadell, O.B. Effect of vasoactive intestinal peptide and pituitary adenylate cyclase-activating polypeptide on pancreatic, hepatic and duodenal mucosal bicarbonate secretion in the pig. Digestion 2003, 67, 56–66. [Google Scholar] [CrossRef] [PubMed]
- Roy, S.; Liu, H.C.; Loh, H.H. μ-Opioid receptor-knockout mice: The role of mu-opioid receptor in gastrointestinal transit. Brain Res. Mol. Brain Res. 1998, 56, 281–283. [Google Scholar] [CrossRef]
- Weiss, N.; Zamponi, G.W. Opioid Receptor Regulation of Neuronal Voltage-Gated Calcium Channels. Cell. Mol. Neurobiol. 2021, 41, 839–847. [Google Scholar] [CrossRef]
- Kraichely, R.E.; Arora, A.S.; Murray, J.A. Opiate-induced oesophageal dysmotility. Aliment. Pharmacol. Ther. 2010, 31, 601–606. [Google Scholar] [CrossRef] [Green Version]
- Penagini, R.; Allocca, M.; Cantù, P.; Mangano, M.; Savojardo, D.; Carmagnola, S.; Bianchi, P.A. Relationship between motor function of the proximal stomach and transient lower oesophageal sphincter relaxation after morphine. Gut 2004, 53, 1227. [Google Scholar] [CrossRef] [Green Version]
- Wood, J.D.; Galligan, J.J. Function of opioids in the enteric nervous system. Neurogastroenterol. Motil. 2004, 16 (Suppl. 2), 17–28. [Google Scholar] [CrossRef]
- Gonenne, J.; Camilleri, M.; Ferber, I.; Burton, D.; Baxter, K.; Keyashian, K.; Foss, J.; Wallin, B.; Du, W.; Zinsmeister, A.R. Effect of alvimopan and codeine on gastrointestinal transit: A randomized controlled study. Clin. Gastroenterol. Hepatol. 2005, 3, 784–791. [Google Scholar] [CrossRef]
- Wilder-Smith, C.H. The balancing act: Endogenous modulation of pain in functional gastrointestinal disorders. Gut 2011, 60, 1589–1599. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, W.M.; Read, N.W.; Verlinden, M. Effects of loperamide oxide on gastrointestinal transit time and anorectal function in patients with chronic diarrhoea and faecal incontinence. Scand. J. Gastroenterol. 1997, 32, 34–38. [Google Scholar] [CrossRef]
- Hawkes, N.D.; Rhodes, J.; Evans, B.K.; Rhodes, P.; Hawthorne, A.B.; Thomas, G.A.O. Naloxone treatment for irritable bowel syndrome--a randomized controlled trial with an oral formulation. Aliment. Pharmacol. Ther. 2002, 16, 1649–1654. [Google Scholar] [CrossRef] [PubMed]
- Mark, E.B.; Nedergaard, R.B.; Hansen, T.M.; Nissen, T.D.; Frøkjær, J.B.; Scott, S.M.; Krogh, K.; Drewes, A.M. Tapentadol results in less deterioration of gastrointestinal function and symptoms than standard opioid therapy in healthy male volunteers. Neurogastroenterol. Motil. 2021, 33, e14131. [Google Scholar] [CrossRef] [PubMed]
- Mark, E.B.; Frøkjær, J.B.; Hansen, T.M.; Nedergaard, R.B.; Drewes, A.M. Although tapentadol and oxycodone both increase colonic volume, tapentadol treatment resulted in softer stools and less constipation: A mechanistic study in healthy volunteers. Scand. J. Pain 2021, 21, 406–414. [Google Scholar] [CrossRef]
- Mark, E.B.; Bødker, M.B.; Grønlund, D.; Østergaard, L.R.; Frøkjær, J.B.; Drewes, A.M. MRI analysis of fecal volume and dryness: Validation study using an experimental oxycodone-induced constipation model. J. Magn. Reson. Imaging 2019, 50, 733–745. [Google Scholar] [CrossRef] [PubMed]
- Mark, E.B.; Poulsen, J.L.; Haase, A.M.; Espersen, M.; Gregersen, T.; Schlageter, V.; Scott, S.M.; Krogh, K.; Drewes, A.M. Ambulatory assessment of colonic motility using the electromagnetic capsule tracking system. Neurogastroenterol. Motil. 2019, 31, e13451. [Google Scholar] [CrossRef]
- Poulsen, J.L.; Mark, E.B.; Brock, C.; Frøkjær, J.B.; Krogh, K.; Drewes, A.M. Colorectal Transit and Volume During Treatment With Prolonged-release Oxycodone/Naloxone Versus Oxycodone Plus Macrogol 3350. J. Neurogastroenterol. Motil. 2018, 24, 119–127. [Google Scholar] [CrossRef] [Green Version]
- Poulsen, J.L.; Nilsson, M.; Brock, C.; Sandberg, T.H.; Krogh, K.; Drewes, A.M. The Impact of Opioid Treatment on Regional Gastrointestinal Transit. J. Neurogastroenterol. Motil. 2016, 22, 282–291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nilsson, M.; Poulsen, J.L.; Brock, C.; Sandberg, T.H.; Gram, M.; Frøkjr, J.B.; Krogh, K.; Drewes, A.M. Opioid-induced bowel dysfunction in healthy volunteers assessed with questionnaires and MRI. Eur. J. Gastroenterol. Hepatol. 2016, 28, 514–524. [Google Scholar] [CrossRef]
- Poulsen, J.L.; Brock, C.; Olesen, A.E.; Nilsson, M.; Drewes, A.M. Evolving paradigms in the treatment of opioid-induced bowel dysfunction. Therap. Adv. Gastroenterol. 2015, 8, 360–372. [Google Scholar] [CrossRef] [Green Version]
- Regnard, C.; Twycross, R.; Mihalyo, M.; Wilcock, A. Loperamide: A pharmacological review. J. Pain Symptom Manag. 2011, 42, 319–323. [Google Scholar] [CrossRef] [PubMed]
- Eggleston, W.; Clark, K.H.; Marraffa, J.M. Loperamide Abuse Associated With Cardiac Dysrhythmia and Death. Ann. Emerg. Med. 2017, 69, 83–86. [Google Scholar] [CrossRef] [PubMed]
- Miller, H.; Panahi, L.; Tapia, D.; Tran, A.; Bowman, J.D. Loperamide misuse and abuse. J. Am. Pharm. Assoc. 2017, 57, S45–S50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Powell, J.W.; Presnell, S.E. Loperamide as a Potential Drug of Abuse and Misuse: Fatal Overdoses at the Medical University of South Carolina. J. Forensic Sci. 2019, 64, 1726–1730. [Google Scholar] [CrossRef]
- Gerostamoulos, J.; Burke, M.P.; Drummer, O.H. Involvement of codeine in drug-related deaths. Am. J. Forensic Med. Pathol. 1996, 17, 327–335. [Google Scholar] [CrossRef]
- De Vasconcelos Generoso, S.; Lages, P.C.; Correia, M.I.T.D. Fiber, prebiotics, and diarrhea: What, why, when and how. Curr. Opin. Clin. Nutr. Metab. Care 2016, 19, 388–393. [Google Scholar] [CrossRef]
- Davani-Davari, D.; Negahdaripour, M.; Karimzadeh, I.; Seifan, M.; Mohkam, M.; Masoumi, S.J.; Berenjian, A.; Ghasemi, Y. Prebiotics: Definition, Types, Sources, Mechanisms, and Clinical Applications. Foods 2019, 8, 92. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Author, Year | Study Design | Study Population | Inclusion Criteria | Investigational Product vs. Comparator | Main Findings |
|---|---|---|---|---|---|
| E. K. Yeoh, 1993 [16] | Randomized, double-blind, cross-over study | Patients with chronic radiation enteritis (n = 20) + Healthy subjects (n = 18) | >14 stools/week | Loperamide oxide vs. placebo | Loperamide reduced 31% to a mean of 13/week compared with placebo 19/week (p < 0.001) |
| P. Mainguet, 1977 [17] | Randomized, double-blind, cross-over study | Patients with ileo-colic disease or resection (n = 18) | >3 months of diarrhea | Loperamide vs. placebo | 1.5 liquid + loose stool/day (loperamide) 4.5 liquid + loose stool/day (placebo) (p < 0.001) |
| M. Read, 1982 [18] | Randomized, double-blind, cross-over study | Patients with chronic diarrhea and fecal incontinence (n = 26) | >3 months of diarrhea and complained of episodes of fecal incontinence and severe urgency sufficient to limit lifestyle | Loperamide vs. placebo | Loperamide reduced 35% to a mean of 11/week compared with placebo 17/week (p < 0.001) |
| P.S. Efskind, 1996 [19] | Randomized, double-blind, parallel study | Patients with symptoms of IBS (n = 69) + Healthy subjects (n = 33) | Weekly symptoms >3 months of abdominal pain and changing stool pattern and consistency | Loperamide vs. placebo | 36% reduction in stool frequency compared with placebo and with baseline throughout 5 weeks of treatment (p < 0.001) |
| B. Lävo, 1987 [20] | Randomized, double-blind, parallel study | Patients with symptoms of IBS (n = 21) | >3 months of diarrhea with no demonstrable organic bowel disease | Loperamide vs. placebo | Loperamide promising with respect to decreased stool frequency, no difference between treatments |
| P.A. Cann, 1984 [21] | Randomized, double-blind, cross-over study | Patients with symptoms of IBS (n = 28) | Symptoms (abdominal pain and bowel disturbances) present >6 months and >3 days/week | Loperamide vs. placebo | 1.3 ± 0.1 stool/day (loperamide) 1.9 ± 0.2 stool/day (placebo) (p < 0.001) |
| W. Pelemans, 1993 [22] | Randomized, double-blind, cross-over study | Patients with colectomy and ileostomy and documented chronic diarrhea of diverse origin | >3 unformed stools/day for 3 consecutive days | Loperamide and diphenoxylate vs. drug free | 1.4 liquid + loose stool/day (loperamide) 2.7 liquid + loose stool/day (diphenoxylate) 4.6 liquid + loose stool/day (drug-free mean) (p < 0.001) |
| A.W. Mangel, 2008 [23] | Randomized, double-blind, parallel study | Patients with IBS-D diagnosis (n~198) | Meeting Rome II Criteria for IBS and have predominant symptoms of diarrhea | Asimadoline vs. placebo | 2.3 stool/day (asimadoline) 2.6 stool/day (placebo) (p < 0.005) |
| L. Barrow, 1993 [24] | Randomized, cross-over study | Healthy subjects (n = 12) | Lactulose-induced diarrhea | Codeine phosphate | 1.2 stool/day (lactulose + codeine) 2.4 stool/day (lactulose only) (p < 0.01) |
| Author, Year | Study Design | Study Population | Inclusion Criteria | Investigational Product vs. Comparator | Main Findings |
|---|---|---|---|---|---|
| P. Mainguet, 1977 [17] | Randomized, double-blind, cross-over study | Patients with ileo-colic disease or resection (n = 18) | >3 months of diarrhea | Loperamide vs. placebo | 1.5 unformed stools/day (loperamide) 4.5 unformed stools/day (placebo) (p < 0.001) |
| M. Read, 1982 [18] | Randomized, double-blind, cross-over study | Patients with chronic diarrhea and fecal incontinence (n = 26) | >3 months diarrhea with episodes of fecal incontinence and severe urgency limit lifestyle | Loperamide vs. placebo | 29% unformed stools/week (loperamide) 62% unformed stools/week (placebo) (p < 0.001) |
| P.S. Efskind, 1996 [19] | Randomized, double-blind, parallel-group study | Patients with symptoms of IBS (n = 69) + Healthy subjects (n = 33) | Weekly symptoms >3 months abdominal pain and changing stool pattern and consistency | Loperamide vs. placebo | Loperamide improved stool consistency compared with placebo |
| B. Lävo, 1987 [20] | Randomized, double-blind study | Patients with symptoms of IBS (n = 21) | >3 months of diarrhea with no demonstrable organic bowel disease | Loperamide vs. placebo | Loperamide reduced weekly number of unformed stools compared with placebo |
| P.A. Cann, 1984 [21] | Randomized, double-blind, cross-over study | Patients with symptoms of IBS (n = 28) | Symptoms (abdominal pain and bowel disturbances) present >6 months and >3 days/week | Loperamide vs. placebo | Loperamide reduced weekly percentage of unformed stools compared with placebo |
| W. Pelemans, 1993 [22] | Randomized, double-blind, cross-over study | Patients with colectomy and ileostomy and chronic diarrhea of diverse origin | >3 unfirmed stools/day for 3 consecutive days | Loperamide and diphenoxylate | Loperamide and diphenoxylate improved stool consistency; loperamide significantly better than diphenoxylate |
| A.W. Mangel, 2008 [23] | Randomized, double-blind study | Patients with IBS-D diagnosis (n~198) | Rome II criteria of IBS and predominant symptoms of diarrhea | Asimadoline vs. placebo | No improvement of fecal consistency in patients on asimadoline at any dose vs. placebo |
| Author, Year | Study Design | Study Population | Inclusion Criteria | Investigational Product vs. Comparator | Main Findings |
|---|---|---|---|---|---|
| P. Mainguet, 1977 [17] | Randomized, double-blind, cross-over study | Patients with ileo-colic disease or resection (n = 18) | >3 months of diarrhea | Loperamide vs. placebo | 4.6 h whole gut transit (loperamide) 2.2 h whole gut transit (placebo) (p < 0.001) |
| E.K. Yeoh, 1993 [16] | Randomized, double-blinded, cross-over study | Patients with chronic radiation enteritis (n = 20) + Healthy subjects (n = 18) | >14 stools/week | Loperamide oxide vs. placebo | Loperamide oxide decreased gastric emptying time, and increased small bowel and whole gut transit time compared with placebo Gastric emptying time decreased with loperamide in healthy subjects |
| P.A. Cann, 1984 [21] | Randomized, double-blind, cross-over study | Patients with symptoms of IBS (n = 28) | Symptoms (abdominal pain and bowel disturbances) present >6 months and >3 days/week | Loperamide vs. placebo | Loperamide decreased gastric emptying time, and increased small bowel and whole gut transit time compared with placebo 56 ± 5 h whole gut transit (loperamide) 42 ± 4 h whole gut transit (placebo) (p < 0.01) |
| E. Schulte-Frohlinde, 2000 [25] | Prospective, open dose–response study | Healthy male volunteers (n = 10) | No diarrhea | Casokefamide vs. placebo | Casokefamide showed a trend toward prolongation of oro–cecal transit time |
| L. Barrow, 1993 [24] | Randomized, cross-over study | Healthy subjects (n = 12) | Lactulose-induced diarrhea | Codeine phosphate | Codeine increased mouth-to-ileal and colonic transit time primarily in the ascending colon 5.3 ± 3.2 h whole gut transit (codeine) 2.8 ± 1.0 h whole gut transit (placebo) (p < 0.02) |
| Author, Year | Study Design | Study Population | Inclusion Criteria | Investigational Product vs. Comparator | Main Findings |
|---|---|---|---|---|---|
| E.K. Yeoh, 1993 [16] | Randomized, double-blinded, cross-over study | Patients with chronic radiation enteritis (n = 20) + Healthy subjects (n = 18) | >14 stools/week | Loperamide oxide vs. placebo | Gastrointestinal symptoms not different between loperamide and placebo |
| P.A. Cann, 1984 [21] | Randomized, double-blind, cross-over study | Patients with symptoms of IBS (n = 28) | Symptoms (abdominal pain and bowel disturbances) >6 months and >3 days/week | Loperamide vs. placebo | Diarrhea, urgency and borborygmi significantly improved during loperamide compared with placebo |
| P.S. Efskind, 1996 [19] | Randomized, double-blind, parallel-group study | Patients with symptoms of IBS (n = 69) + Healthy subjects (n = 33) | Weekly symptoms >3 months of abdominal pain and changing stool pattern and consistency | Loperamide vs. placebo | Loperamide reduced pain intensity, but increased nighttime pain compared with placebo |
| B. Lävo, 1987 [20] | Randomized, double-blind study | Patients with symptoms of IBS (n = 21) | >3 months of diarrhea with no demonstrable organic bowel disease | Loperamide vs. placebo | Less urgency and pain with loperamide compared with placebo |
| A.W. Mangel, 2008 [23] | Randomized, double-blind study | Patients with IBS-D diagnosis (n~198) | Rome II criteria for IBS and predominant symptoms of diarrhea | Asimadoline vs. placebo | Asimadoline relieved IBS pain and diarrhea compared with placebo |
| M. Dapoigny (9) [28] | Randomized, double-blind, parallel-group study | Patients with symptoms suggestive of IBS diagnosis (n = 313) | Abdominal pain ≥moderate intensity and ≥2 additional gastrointestinal symptoms | Fedotozine vs. placebo | Adominal pain and bloating significantly reduced with fedotozine compared with placebo |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Graven-Nielsen, C.S.; Knoph, C.S.; Okdahl, T.; Høyer, K.L.; Krogh, K.; Hellström, P.M.; Drewes, A.M. Opioids in the Treatment of Chronic Idiopathic Diarrhea in Humans—A Systematic Review and Treatment Guideline. J. Clin. Med. 2023, 12, 2488. https://doi.org/10.3390/jcm12072488
Graven-Nielsen CS, Knoph CS, Okdahl T, Høyer KL, Krogh K, Hellström PM, Drewes AM. Opioids in the Treatment of Chronic Idiopathic Diarrhea in Humans—A Systematic Review and Treatment Guideline. Journal of Clinical Medicine. 2023; 12(7):2488. https://doi.org/10.3390/jcm12072488
Chicago/Turabian StyleGraven-Nielsen, Christoffer S., Cecilie S. Knoph, Tina Okdahl, Katrine L. Høyer, Klaus Krogh, Per M. Hellström, and Asbjørn M. Drewes. 2023. "Opioids in the Treatment of Chronic Idiopathic Diarrhea in Humans—A Systematic Review and Treatment Guideline" Journal of Clinical Medicine 12, no. 7: 2488. https://doi.org/10.3390/jcm12072488