
Distinct Sleep Alterations in Alcohol Use Disorder Patients with and without Korsakoff’s Syndrome: Relationship with Episodic Memory
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
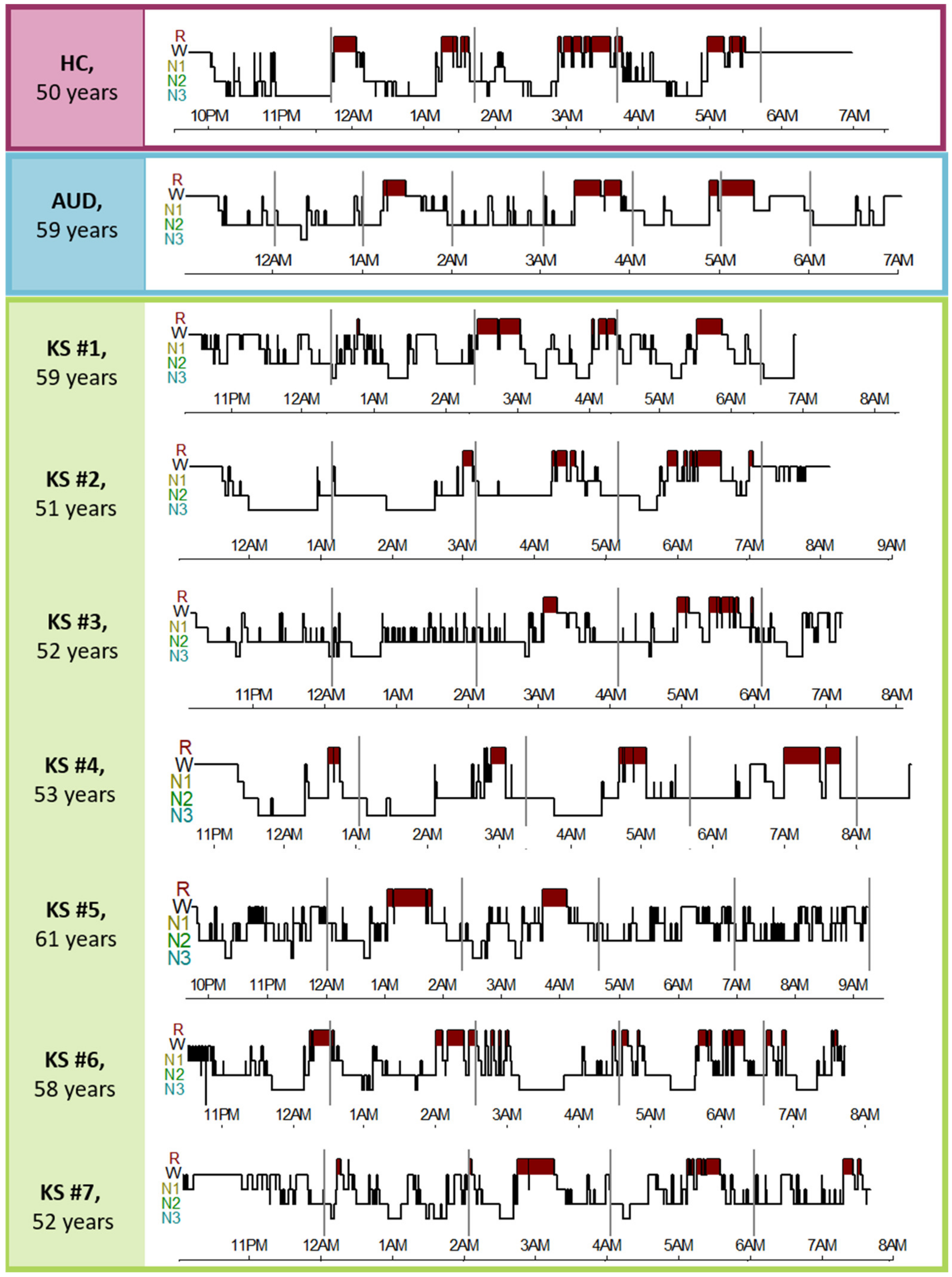
2.2. Sleep Recording
2.3. Neuropsychological Assessment
2.4. Statistical Analyses
3. Results
3.1. Between-Group Comparisons on Demographic and Clinical Variables
3.2. Between-Group Comparisons on Sleep Measures
3.3. Between-Group Comparisons on Cognitive Performance
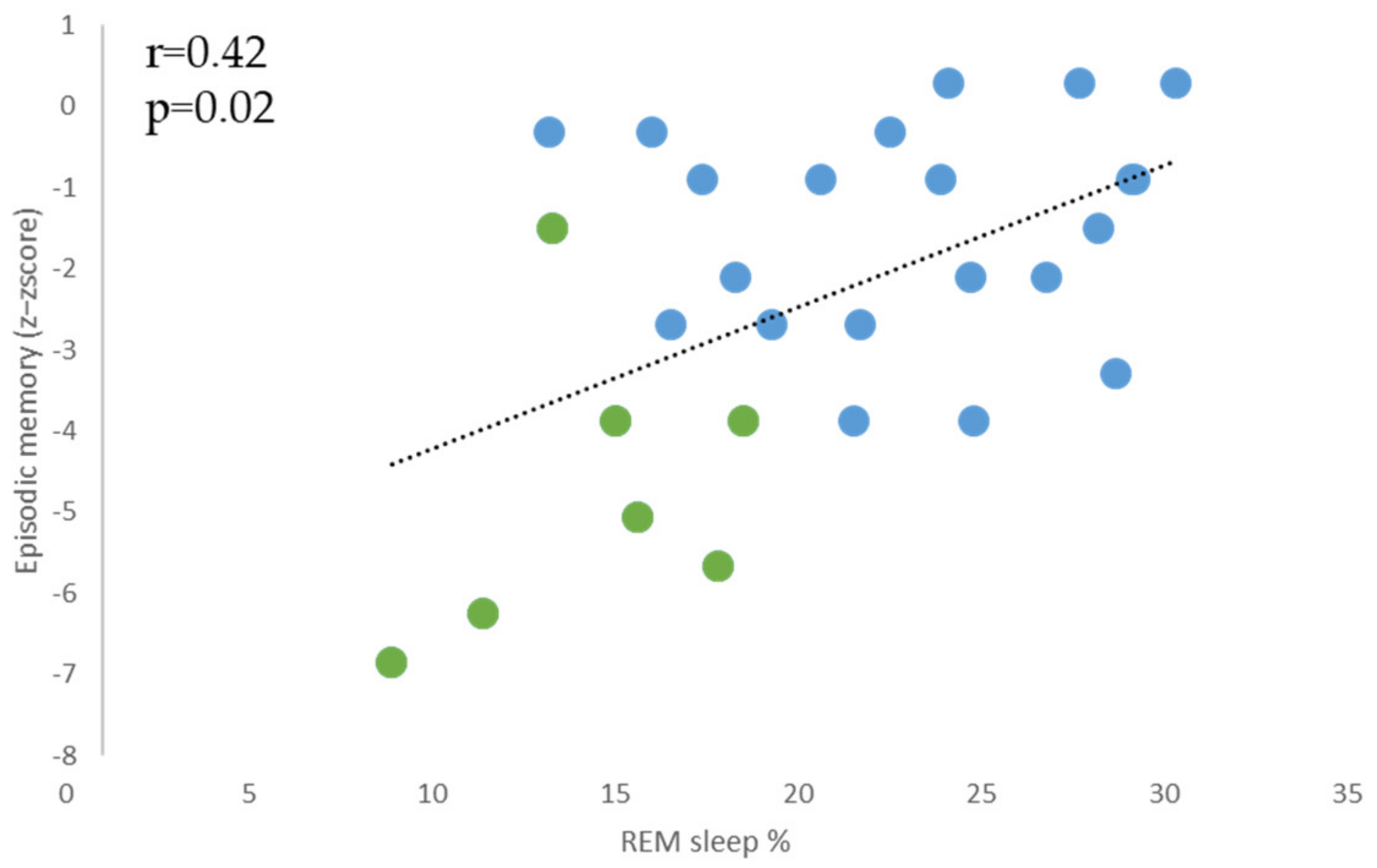
3.4. Relationships between Episodic Memory Performance and REM Sleep Parameters in the Entire Group of Patients
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Statistics | Post-Hoc Comparisons | |
|---|---|---|
| Sleep onset latency | F(2, 40) = 2.6, p = 0.08 | NS |
| Sleep efficiency % | F(2, 40) = 0.52, p = 0.59 | NS |
| Total sleep time (min) | F(2, 40) = 5.49, p = 0.008 | (HC = AUD) < KS |
| WASO (min) | F(2, 40) = 0.53, p = 0.59 | NS |
| Stage shifts to N1 sleep (nb/h) | F(2, 40) = 2.02, p = 0.15 | NS |
| N1 sleep (% of total sleep time) | F(2, 40) = 2.02, p = 0.14 | NS |
| N2 sleep (% of total sleep time) | F(2, 40) = 1.63, p = 0.21 | NS |
| N3 sleep (% of total sleep time) | F(2, 40) = 1.09, p = 0.35 | NS |
| REM sleep (% of total sleep time) | F(2, 40) = 9.38, p = 0.0005 | (HC = AUD) > KS |
| Statistics | Post-Hoc Comparisons | |
|---|---|---|
| Sleep onset latency | F(2, 40) = 2.59, p = 0.09 | NS |
| Sleep efficiency % | F(2, 40) = 0.25, p = 0.77 | NS |
| Total sleep time (min) | F(2, 40) = 3.27, p = 0.05 | NS |
| WASO (min) | F(2, 40) = 0.42, p = 0.65 | NS |
| Stage shifts to N1 sleep (nb/h) | F(2, 40) = 5.87, p = 0.006 | HC < (AUD = KS) |
| N1 sleep (% of total sleep time) | F(2, 40) = 7.45, p = 0.002 | HC < (AUD = KS) |
| N2 sleep (% of total sleep time) | F(2, 40) = 1.59, p = 0.21 | NS |
| N3 sleep (% of total sleep time) | F(2, 40) = 5.20, p = 0.009 | HC > AUD; HC = KS; AUD = KS |
| REM sleep (% of total sleep time) | F(2, 40) = 5.09, p = 0.01 | (HC = AUD) > KS |
| Statistics | Post-Hoc Comparisons | |
|---|---|---|
| Sleep onset latency | F(2, 40) = 3.69, p = 0.03 | HC > KS; HC = AUD; AUD = KS |
| Sleep efficiency % | F(2, 40) = 0.23, p = 0.79 | NS |
| Total sleep time (min) | F(2, 40) = 3.03, p = 0.06 | NS |
| WASO (min) | F(2, 40) = 1, p = 0.37 | NS |
| Stage shifts to N1 sleep (nb/h) | F(2, 40) = 9.36, p < 0.001 | HC < (AUD = KS) |
| N1 sleep (% of total sleep time) | F(2, 40) = 8.70, p < 0.001 | HC < (AUD = KS) |
| N2 sleep (% of total sleep time) | F(2, 40) = 1.63, p = 0.2 | NS |
| N3 sleep (% of total sleep time) | F(2, 40) = 4.52, p = 0.01 | HC > AUD; HC = KS; AUD = KS |
| REM sleep (% of total sleep time) | F(2, 40) = 3.54, p = 0.03 | HC = AUD; HC = KS; KS < AUD |
References
- Savage, L.M.; Hall, J.M.; Resende, L.S. Translational Rodent Models of Korsakoff Syndrome Reveal the Critical Neuroanatomical Substrates of Memory Dysfunction and Recovery. Neuropsychol. Rev. 2012, 22, 195–209. [Google Scholar] [CrossRef] [Green Version]
- Kopelman, M.D.; Thomson, A.D.; Guerrini, I.; Marshall, E.J. The Korsakoff Syndrome: Clinical Aspects, Psychology and Treatment. Alcohol Alcohol. 2009, 44, 148–154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arts, N.J.; Walvoort, S.J.; Kessels, R.P. Korsakoff’s Syndrome: A Critical Review. Neuropsychiatr. Dis. Treat. 2017, 13, 2875–2890. [Google Scholar] [CrossRef] [Green Version]
- Fein, G.; Torres, J.; Price, L.J.; Di Sclafani, V. Cognitive Performance in Long-Term Abstinent Alcoholic Individuals. Alcohol. Clin. Exp. Res. 2006, 30, 1538–1544. [Google Scholar] [CrossRef] [Green Version]
- Pitel, A.L.; Rivier, J.; Beaunieux, H.; Vabret, F.; Desgranges, B.; Eustache, F. Changes in the Episodic Memory and Executive Functions of Abstinent and Relapsed Alcoholics Over a 6-Month Period. Alcohol. Clin. Exp. Res. 2009, 33, 490–498. [Google Scholar] [CrossRef] [PubMed]
- Brion, M.; Pitel, A.-L.; Beaunieux, H.; Maurage, P. Revisiting the Continuum Hypothesis: Toward an In-Depth Exploration of Executive Functions in Korsakoff Syndrome. Front. Hum. Neurosci. 2014, 8, 498. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koob, G.F.; Colrain, I.M. Alcohol Use Disorder and Sleep Disturbances: A Feed-Forward Allostatic Framework. Neuropsychopharmacology 2020, 45, 141–165. [Google Scholar] [CrossRef] [PubMed]
- Aldrich, M.S.; Brower, K.J.; Hall, J.M. Sleep-Disordered Breathing in Alcoholics. Alcohol. Clin. Exp. Res. 1999, 23, 134–140. [Google Scholar] [CrossRef]
- Chakravorty, S.; Chaudhary, N.S.; Brower, K.J. Alcohol Dependence and Its Relationship with Insomnia and Other Sleep Disorders. Alcohol. Clin. Exp. Res. 2016, 40, 2271–2282. [Google Scholar] [CrossRef]
- Junghanns, K.; Horbach, R.; Ehrenthal, D.; Blank, S.; Backhaus, J. Chronic and High Alcohol Consumption Has a Negative Impact on Sleep and Sleep-Associated Consolidation of Declarative Memory. Alcohol. Clin. Exp. Res. 2009, 33, 893–897. [Google Scholar] [CrossRef]
- Laniepce, A.; Segobin, S.; Lannuzel, C.; Boudehent, C.; Ritz, L.; Urso, L.; Vabret, F.; Eustache, F.; Beaunieux, H.; Rauchs, G.; et al. Neuropsychological and Neuroimaging Examinations of Self-Reported Sleep Quality in Alcohol Use Disorder With and Without Korsakoff’s Syndrome. Alcohol. Clin. Exp. Res. 2019, 43, 952–964. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lairie, M.; Pottier, M. Quelques Remarques a Propos Du Sommeil Dans Le Syndrome de Korsakoff. Rev. Electroencephalogr. Neurophysiol. Clin. 1979, 9, 277–285. [Google Scholar] [CrossRef]
- Greenberg, R.; Hartmann, E.; Brooks, R.; Mayer, R. Dreaming and Korsakoff’s Psychosis. Arch. Gen. Psychiatry 1968, 18, 203–209. [Google Scholar] [CrossRef]
- Martin, P.R.; Loewenstein, R.J.; Kaye, W.H.; Ebert, M.H.; Weingartner, H.; Gillin, J.C. Sleep EEG in Korsakoff’s Psychosis and Alzheimer’s Disease. Neurology 1986, 36, 411. [Google Scholar] [CrossRef] [PubMed]
- Cathala, H.P.; Laffont, F.; Esnault, S.; Sereni, C.; Siksou, M. Sommeil et Reves Dans l’amnesie de Korsakoff d’origine Alcoolique. Neurophysiol. Clin./Clin. Neurophysiol. 1988, 18, 173–186. [Google Scholar] [CrossRef]
- Walvoort, S.J.W.; van der Heijden, P.T.; Wester, A.J.; Kessels, R.P.C.; Egger, J.I.M. Self-Awareness of Cognitive Dysfunction: Self-Reported Complaints and Cognitive Performance in Patients with Alcohol-Induced Mild or Major Neurocognitive Disorder. Psychiatry Res. 2016, 245, 291–296. [Google Scholar] [CrossRef] [PubMed]
- Wirz-Justice, A.; Schröder, C.M.; Gasio, P.F.; Cajochen, C.; Savaskan, E. The Circadian Rest-Activity Cycle in Korsakoff Psychosis. Am. J. Geriatr. Psychiatry 2010, 18, 33–41. [Google Scholar] [CrossRef]
- Kamphuis, J.; Meerlo, P.; Koolhaas, J.M.; Lancel, M. Poor Sleep as a Potential Causal Factor in Aggression and Violence. Sleep Med. 2012, 13, 327–334. [Google Scholar] [CrossRef]
- Lowe, C.J.; Safati, A.; Hall, P.A. The Neurocognitive Consequences of Sleep Restriction: A Meta-Analytic Review. Neurosci. Biobehav. Rev. 2017, 80, 586–604. [Google Scholar] [CrossRef]
- Beck, A.T.; Ward, C.H.; Mendelson, M.; Mock, J.; Erbaugh, J. An Inventory for Measuring Depression. Arch. Gen. Psychiatry 1961, 4, 561–571. [Google Scholar] [CrossRef] [Green Version]
- Spielberger, C.D.; Gorsuch, R.L.; Lushene, R.; Vagg, P.R.; Jacobs, G.A. State-Trait Anxiety Inventory for Adults (Form Y); Mind Garden, Inc.: Menlo Park, CA, USA, 1983. [Google Scholar] [CrossRef]
- American Psychiatric Association DSM-5 Diagnostic Classification. In Diagnostic and Statistical Manual of Mental Disorders; American Psychiatric Association: Washington, DC, USA, 2013.
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-Mental State”. A Practical Method for Grading the Cognitive State of Patients for the Clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef] [PubMed]
- Maillard, A.; Laniepce, A.; Cabé, N.; Boudehent, C.; Chételat, G.; Urso, L.; Eustache, F.; Vabret, F.; Segobin, S.; Pitel, A.L. Temporal Cognitive and Brain Changes in Korsakoff Syndrome. Neurology 2021, 96, e1987–e1998. [Google Scholar] [CrossRef]
- Cushman, P.; Forbes, R.; Lemer, W.; Stewart, M. Alcohol Withdrawal Syndromes: Clinical Management with Lofexidine. Alcohol. Clin. Exp. Res. 1985, 9, 103–108. [Google Scholar] [CrossRef] [PubMed]
- Pfefferbaum, A.; Rosenbloom, M.; Crusan, K.; Jernigan, T.L. Brain CT Changes in Alcoholics: Effects of Age and Alcohol Consumption. Alcohol. Clin. Exp. Res. 1988, 12, 81–87. [Google Scholar] [CrossRef] [PubMed]
- Gache, P.; Michaud, P.; Landry, U.; Accietto, C.; Arfaoui, S.; Wenger, O.; Daeppen, J.-B. The Alcohol Use Disorders Identification Test (AUDIT) as a Screening Tool for Excessive Drinking in Primary Care: Reliability and Validity of a French Version. Alcohol. Clin. Exp. Res. 2005, 29, 2001–2007. [Google Scholar] [CrossRef] [PubMed]
- Poisnel, G.; Arenaza-Urquijo, E.; Collette, F.; Klimecki, O.M.; Marchant, N.L.; Wirth, M.; La Sayette, V.; Rauchs, G.; Salmon, E.; Vuilleumier, P.; et al. The Age-Well Randomized Controlled Trial of the Medit-Ageing European Project: Effect of Meditation or Foreign Language Training on Brain and Mental Health in Older Adults. Alzheimer’s Dement. Transl. Res. Clin. Interv. 2018, 4, 714–723. [Google Scholar] [CrossRef]
- Mattis, S. Mental Status Examination for Organic Mental Syndrome in the Elderly Patient. In Geriatric Psychiatry. A Hand Book for Psychiatrics and Primary Care Physicians; Grune & Stratton: New York, NY, USA, 1976. [Google Scholar]
- Buysse, D.J.; Reynolds, C.F.; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A New Instrument for Psychiatric Practice and Research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Johns, M.W. A New Method for Measuring Daytime Sleepiness: The Epworth Sleepiness Scale. Sleep 1991, 14, 540–545. [Google Scholar] [CrossRef] [Green Version]
- Berry, R.B.; Brooks, R.; Gamaldo, C.; Harding, S.M.; Lloyd, R.M.; Quan, S.F.; Troester, M.T.; Vaughn, B.V. AASM Scoring Manual Updates for 2017 (Version 2.4). J. Clin. Sleep Med. 2017, 13, 665–666. [Google Scholar] [CrossRef]
- Laniepce, A.; Cabé, N.; André, C.; Bertran, F.; Boudehent, C.; Lahbairi, N.; Maillard, A.; Mary, A.; Segobin, S.; Vabret, F.; et al. The Effect of Alcohol Withdrawal Syndrome Severity on Sleep, Brain and Cognition. Brain Commun. 2020, 2, fcaa123. [Google Scholar] [CrossRef]
- Reitan, R.M.; Wolfson, D. The Halstead–Reitan Neuropsycholgical Test Battery: Therapy and Clinical Interpretation. In Comprehensive Handbook of Psychological Assessment; Springer Science+Business Media: New York, NY, USA, 1985. [Google Scholar]
- Stroop, J.R. Studies of Interference in Serial Verbal Reactions. J. Exp. Psychol. 1935, 18, 643–662. [Google Scholar] [CrossRef]
- Wechsler, D. WAIS-III Administration and Scoring Manual; Psychological Corporation: San Antonio, TX, USA, 1997; ISBN 0158981030/9780158981031. [Google Scholar]
- Van der Linden, M.; Coyette, F.; Poitrenaud, J.; Kalafat, M.; Calicis, F.; Wyns, C.; Adam, S. L’épreuve de Rappel Libre/Rappel Indicé à 16 Items (RL/RI-16). In L’évaluation des Troubles de la Mémoire: Présentation de Quatre Tests de Mémoire Episodique Avec Leur Etalonnage; Solal: Marseille, France, 2004; pp. 25–42. ISBN 2-914513-60-7. [Google Scholar]
- Fritz, C.O.; Morris, P.E.; Richler, J.J. Effect Size Estimates: Current Use, Calculations, and Interpretation. J. Exp. Psychol. Gen. 2012, 141, 2–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sateia, M.J. International Classification of Sleep Disorders-Third Edition Highlights and Modifications. Chest 2014, 146, 1387–1394. [Google Scholar] [CrossRef]
- Krishnan, V.; Collop, N.A. Gender Differences in Sleep Disorders. Curr. Opin. Pulm. Med. 2006, 12, 383–389. [Google Scholar] [CrossRef]
- Le Bon, O.; Verbanck, P.; Hoffmann, G.; Murphy, J.R.; Staner, L.; De Groote, D.; Mampunza, S.; Den Dulk, A.; Vacher, C.; Kornreich, C.; et al. Sleep in Detoxified Alcoholics: Impairment of Most Standard Sleep Parameters and Increased Risk for Sleep Apnea, but Not for Myoclonias—A Controlled Study. J. Stud. Alcohol 1997, 58, 30–36. [Google Scholar] [CrossRef]
- Geer, J.H.; Hilbert, J. Gender Issues in Obstructive Sleep Apnea. Yale J. Biol. Med. 2021, 94, 487–496. [Google Scholar]
- Bublitz, M.; Adra, N.; Hijazi, L.; Shaib, F.; Attarian, H.; Bourjeily, G. A Narrative Review of Sex and Gender Differences in Sleep Disordered Breathing: Gaps and Opportunities. Life 2022, 12, 2003. [Google Scholar] [CrossRef] [PubMed]
- Huang, X.; Tang, S.; Lyu, X.; Yang, C.; Chen, X. Structural and Functional Brain Alterations in Obstructive Sleep Apnea: A Multimodal Meta-Analysis. Sleep Med. 2019, 54, 195–204. [Google Scholar] [CrossRef] [PubMed]
- Olaithe, M.; Bucks, R.S.; Hillman, D.R.; Eastwood, P.R. Cognitive Deficits in Obstructive Sleep Apnea: Insights from a Meta-Review and Comparison with Deficits Observed in COPD, Insomnia, and Sleep Deprivation. Sleep Med. Rev. 2018, 38, 39–49. [Google Scholar] [CrossRef] [Green Version]
- Gaspar, L.S.; Álvaro, A.R.; Moita, J.; Cavadas, C. Obstructive Sleep Apnea and Hallmarks of Aging. Trends Mol. Med. 2017, 23, 675–692. [Google Scholar] [CrossRef]
- Lavie, P.; Lavie, L. Cardiovascular Morbidity and Mortality in Obstructive Sleep Apnea. Curr. Pharm. Des. 2008, 14, 3466–3473. [Google Scholar] [CrossRef] [PubMed]
- Laniepce, A.; Lahbairi, N.; Cabé, N.; Pitel, A.-L.; Rauchs, G. Contribution of Sleep Disturbances to the Heterogeneity of Cognitive and Brain Alterations in Alcohol Use Disorder. Sleep Med. Rev. 2021, 58, 101435. [Google Scholar] [CrossRef] [PubMed]
- Gillin, J.C.; Smith, T.L.; Irwin, M.; Kripke, D.F.; Schuckit, M. EEG Sleep Studies in “Pure” Primary Alcoholism during Subacute Withdrawal: Relationships to Normal Controls, Age, and Other Clinical Variables. Biol. Psychiatry 1990, 27, 477–488. [Google Scholar] [CrossRef] [PubMed]
- Massimini, M.; Huber, R.; Ferrarelli, F.; Hill, S.; Tononi, G. The Sleep Slow Oscillation as a Traveling Wave. J. Neurosci. 2004, 24, 6862–6870. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Drummond, S.P.A.; Gillin, J.C.; Smith, T.L.; DeModena, A. The Sleep of Abstinent Pure Primary Alcoholic Patients: Natural Course and Relationship to Relapse. Alcohol. Clin. Exp. Res. 1998, 22, 1796–1802. [Google Scholar] [CrossRef] [PubMed]
- Williams, H.L.; Rundell, O.H. Altered Sleep Physiology in Chronic Alcoholics: Reversal with Abstinence. Alcohol. Clin. Exp. Res. 1981, 5, 318–325. [Google Scholar] [CrossRef] [PubMed]
- D’Rozario, A.L.; Chapman, J.L.; Phillips, C.L.; Palmer, J.R.; Hoyos, C.M.; Mowszowski, L.; Duffy, S.L.; Marshall, N.S.; Benca, R.; Mander, B.; et al. Objective Measurement of Sleep in Mild Cognitive Impairment: A Systematic Review and Meta-Analysis. Sleep Med. Rev. 2020, 52, 101308. [Google Scholar] [CrossRef]
- Petit, D.; Gagnon, J.F.; Fantini, M.L.; Ferini-Strambi, L.; Montplaisir, J. Sleep and Quantitative EEG in Neurodegenerative Disorders. J. Psychosom. Res. 2004, 56, 487–496. [Google Scholar] [CrossRef]
- Song, Y.; Blackwell, T.; Yaffe, K.; Ancoli-Israel, S.; Redline, S.; Stone, K.L. Relationships between Sleep Stages and Changes in Cognitive Function in Older Men: The MrOS Sleep Study. Sleep 2015, 38, 411–421. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blackwell, T.; Yaffe, K.; Laffan, A.; Ancoli-Israel, S.; Redline, S.; Ensrud, K.E.; Song, Y.; Stone, K.L.; Osteoporotic Fractures in Men (MrOS) Study Group. Associations of Objectively and Subjectively Measured Sleep Quality with Subsequent Cognitive Decline in Older Community-Dwelling Men: The MrOS Sleep Study. Sleep 2014, 37, 655–663. [Google Scholar] [CrossRef]
- Pase, M.P.; Himali, J.J.; Grima, N.A.; Beiser, A.S.; Satizabal, C.L.; Aparicio, H.J.; Thomas, R.J.; Gottlieb, D.J.; Auerbach, S.H.; Seshadri, S. Sleep Architecture and the Risk of Incident Dementia in the Community. Neurology 2017, 89, 1244–1250. [Google Scholar] [CrossRef]
- Crespi, F.; Jouvet, M. Sleep and Indolamine Alterations Induced by Thiamine Deficiency. Brain Res. 1982, 248, 275–283. [Google Scholar] [CrossRef]
- Dhir, S.; Tarasenko, M.; Napoli, E.; Giulivi, C. Neurological, Psychiatric, and Biochemical Aspects of Thiamine Deficiency in Children and Adults. Front. Psychiatry 2019, 10, 207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scammell, T.E.; Arrigoni, E.; Lipton, J.O. Neural Circuitry of Wakefulness and Sleep. Neuron 2017, 93, 747–765. [Google Scholar] [CrossRef] [Green Version]
- Schliebs, R.; Arendt, T. The Cholinergic System in Aging and Neuronal Degeneration. Behav. Brain Res. 2011, 221, 555–563. [Google Scholar] [CrossRef]
- Blake, M.G.; Boccia, M.M. Basal Forebrain Cholinergic System and Memory. Curr. Top. Behav. Neurosci. 2018, 37, 253–273. [Google Scholar] [CrossRef] [PubMed]
- Zhao, N.; Zhong, C.; Wang, Y.; Zhao, Y.; Gong, N.; Zhou, G.; Xu, T.; Hong, Z. Impaired Hippocampal Neurogenesis Is Involved in Cognitive Dysfunction Induced by Thiamine Deficiency at Early Pre-Pathological Lesion Stage. Neurobiol. Dis. 2008, 29, 176–185. [Google Scholar] [CrossRef] [PubMed]
- Nunes, P.T.; Kipp, B.T.; Reitz, N.L.; Savage, L.M. Aging with Alcohol-Related Brain Damage: Critical Brain Circuits Associated with Cognitive Dysfunction. In International Review of Neurobiology; Academic Press Inc.: Cambridge, MA, USA, 2019; Volume 148, pp. 101–168. ISBN 9780128175309. [Google Scholar]
- De Mendonça, F.M.R.; de Mendonça, G.P.R.R.; Souza, L.C.; Galvão, L.P.; Paiva, H.S.; de Azevedo Marques Périco, C.; Torales, J.; Ventriglio, A.; Maurício Castaldelli-Maia, J.; Sousa Martins Silva, A. Benzodiazepines and Sleep Architecture: A Systematic Review. CNS Neurol. Disord. Drug Targets 2021, 22, 172–179. [Google Scholar] [CrossRef]
- Currie, S.R.; Clark, S.; Rimac, S.; Malhotra, S. Comprehensive Assessment of Insomnia in Recovering Alcoholics Using Daily Sleep Diaries and Ambulatory Monitoring. Alcohol. Clin. Exp. Res. 2003, 27, 1262–1269. [Google Scholar] [CrossRef] [PubMed]
- Wamsley, E.J.; Tucker, M.A.; Shinn, A.K.; Ono, K.E.; McKinley, S.K.; Ely, A.V.; Goff, D.C.; Stickgold, R.; Manoach, D.S. Reduced Sleep Spindles and Spindle Coherence in Schizophrenia: Mechanisms of Impaired Memory Consolidation? Biol. Psychiatry 2012, 71, 154–161. [Google Scholar] [CrossRef] [Green Version]
- Pitel, A.-L.; Chételat, G.; Le Berre, A.-P.; Desgranges, B.; Eustache, F.; Beaunieux, H. Macrostructural Abnormalities in Korsakoff Syndrome Compared with Uncomplicated Alcoholism. Neurology 2012, 78, 1330–1333. [Google Scholar] [CrossRef] [Green Version]
- Pitel, A.L.; Aupée, A.M.; Chételat, G.; Mézenge, F.; Beaunieux, H.; de la Sayette, V.; Viader, F.; Baron, J.C.; Eustache, F.; Desranges, B. Morphological and Glucose Metabolism Abnormalities in Alcoholic Korsakoff’s Syndrome: Group Comparisons and Individual Analyses. PLoS ONE 2009, 4, e7748. [Google Scholar] [CrossRef] [Green Version]
- Loprinzi, P.D.; Frith, E. The Role of Sex in Memory Function: Considerations and Recommendations in the Context of Exercise. J. Clin. Med. 2018, 7, 132. [Google Scholar] [CrossRef] [Green Version]
- Nixon, S.J. Cognitive Deficits in Alcoholic Women. Alcohol. Clin. Exp. Res. 1994, 1, 371–377. [Google Scholar] [CrossRef]
- El Haj, M.; Kessels, R.P.C.; Nandrino, J.L. Sex Differences in Korsakoff’s Syndrome for Inhibition but Not for Episodic Memory or Flexibility. Am. J. Addict. 2020, 29, 129–133. [Google Scholar] [CrossRef] [PubMed]
- Inkelis, S.M.; Hasler, B.P.; Baker, F.C. Sleep and Alcohol Use in Women. Alcohol Res. Curr. Rev. 2019, 40, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Brower, K.J. Alcohol’s Effects on Sleep in Alcoholics. Alcohol Res. Health 2001, 25, 110–125. [Google Scholar] [PubMed]
- Colrain, I.M.; Crowley, K.E.; Nicholas, C.L.; Padilla, M.; Baker, F.C. The Impact of Alcoholism on Sleep Evoked Δ Frequency Responses. Biol. Psychiatry 2009, 66, 177–184. [Google Scholar] [CrossRef] [PubMed] [Green Version]



| HC N = 15 | AUD N = 22 | KS N = 7 | Statistics a | Group Comparisons | |
|---|---|---|---|---|---|
| Demographic data | |||||
| Age (years) | 48.3 ± 11.3 | 47.6 ± 9.7 | 56.1 ± 4 | H(2, N = 44) = 5.23, p = 0.07 | NS |
| Education (years) | 11.8 ± 0.6 | 11.8 ± 2.5 | 10.4 ± 1.1 | H(2, N = 44) = 3.78, p = 0.15 | NS |
| Sex ratio (W/M) | 5/10 | 0/22 | 7/0 | χ2 = 27.2, p < 0.001 | (HC = AUD) ≠ KS |
| Body Mass Index (kg/m2) | 24.3 ± 4 | 23.2 ± 2.7 | 26 ± 6.3 | H(2, N = 43) = 1.63, p = 0.44 | NS |
| STAI-A | 25.8 ± 4.9 | 32.3 ± 10.1 | 30.7 ± 12.4 | H(2, N = 43) = 5.05, p = 0.08 | HC < AUD; HC = KS; AUD = KS |
| STAI-B | 33.3 ± 7.7 | 47 ± 28.5 | 40.5 ± 10.9 | H(2, N = 43) = 12.83, p = 0.002 | NS |
| BDI | 2.6 ± 2.3 | 13.4 ± 9.9 | 8.9 ± 6.4 | H(2, N = 41) = 15.23, p < 0.001 | HC < AUD; HC = KS; AUD = KS |
| Alcohol-related variables | |||||
| AUDIT | 2 ± 1.1 | 28.5 ± 5 | NA | U = 0, p < 0.001 | HC < AUD |
| Alcohol use disorder severity (number of DSM-5 criteria) | / | 9.04 ± 1.43 | NA | / | |
| Duration of alcohol use disorder (years) | / | 25.63 ± 11.27 | NA | / | |
| Daily alcohol consumption before entry (units/day †) | / | 18.86 ± 8.12 | NA | / | |
| Number of previous alcohol withdrawal episodes | / | 1.95 ± 1.29 | NA | / | |
| Abstinence (number of days before inclusion) | / | 10.81 ± 3.80 | NA | / | |
| Cognitive functions (z-score) | |||||
| Processing speed | 0 ± 0.8 | −1.3 ± 1.5 | −1.7 ± 1.4 | H(2, N = 44) = 11.95, p = 0.002 | HC > (AUD = KS) |
| Short-term memory | 0 ± 1 | −0.5 ± 1 | −0.8 ± 0.8 | H(2, N = 44) = 3.89, p = 0.14 | NS |
| Executive functions | 0 ± 0.8 | −1 ± 1.2 | −1.4 ± 0.9 | H(2, N = 44) = 13.93, p < 0.001 | HC > (AUD = KS) |
| Episodic memory | 0 ± 1 | −1.5 ± 1.3 | −4.7 ± 1.8 | H(2, N = 43) = 22, p < 0.0001 | HC > AUD > KS |
| Sleep architecture | |||||
| Sleep onset latency (min) | 31.7 ± 22.5 | 20 ± 15.4 | 11.3 ± 12.5 | H(2, N = 44) = 5.11, p = 0.07 | NS |
| Sleep efficiency % | 82.3 ± 8.7 | 84.2 ± 8.7 | 85.1 ± 6 | H(2, N = 44) = 0.57, p = 0.75 | NS |
| Total sleep time (min) | 387 ± 59.7 | 376 ± 65.7 | 465 ± 40.6 | H(2, N = 44) = 9.78, p = 0.008 | (HC = AUD) < KS |
| WASO (min) | 51.9 ± 37.3 | 52.3 ± 39.5 | 69.9 ± 37.4 | H(2, N = 44) = 1.77, p = 0.41 | NS |
| Stage shifts to N1-sleep index (nb/h) | 1.61 ± 2.01 | 4.73 ± 2.2 | 5.68 ± 2.52 | H(2, N = 44) = 6.26, p = 0.01 | HC < (AUD = KS) |
| Apnea-Hypopnea Index (AHI, nb/h) | 9.4 ± 4.3 | 26.2 ± 14.9 | 29.5 ± 21.6 | H(2, N = 44) = 15.80, p < 0.001 | HC < (AUD = KS) |
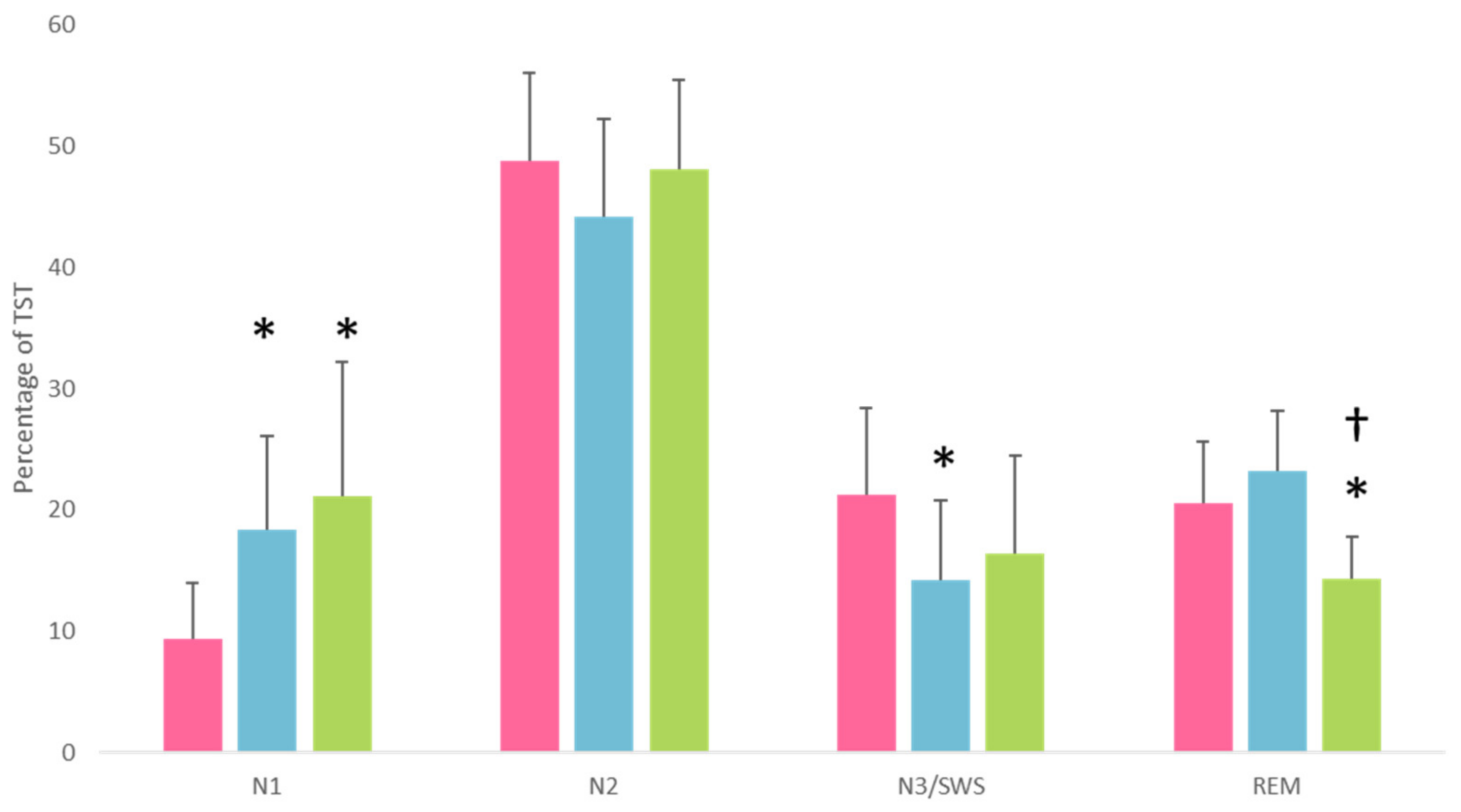
| N1 sleep (% of total sleep time) | 9.4 ± 4.5 | 18.4 ± 7.72 | 21.1 ± 11 | H(2, N = 44) = 16.36, p < 0.001 | HC < (AUD = KS) ‡ |
| N2 sleep (% of total sleep time) | 48.8 ± 7.3 | 44.2 ± 8.1 | 48.1 ± 7.4 | H(2, N = 44) = 3.52, p = 0.17 | NS |
| N3 sleep (% of total sleep time) | 21.2 ± 7.2 | 14.3 ± 6.6 | 16.3 ± 8.1 | H(2, N = 44) = 6.86, p = 0.03 | HC > AUD; HC = KS; AUD = KS ‡ |
| REM sleep (% of total sleep time) | 20.6 ± 5 | 23.2 ± 4.9 | 14.4 ± 3.4 | H(2, N = 44) = 12.51, p = 0.002 | (HC = AUD) > KS |
| KS | Gender, Age | Number of Years in the Nursing Home | Major Medication (Daily Dose) |
|---|---|---|---|
| 1 | W, 59 | >10 years | / |
| 2 | W, 51 | >10 years | Zopiclone (7.5 mg/day), Alprazolam (1.5 mg/day) |
| 3 | W, 52 | >10 years | Hydroxyzine (150 mg/day), Lorazepam (3 mg/day), Duloxetine (60 mg/day) |
| 4 | W, 53 | >10 years | Clonazepam (0.9 mg/day) |
| 5 | W, 61 | >10 years | Venlafaxine (150 mg/day), Lorazepam (1 mg/day) |
| 6 | W, 58 | >10 years | / |
| 7 | W, 52 | 18 months | / |
| HC | AUD | KS | Statistics a | Group Comparisons | |
|---|---|---|---|---|---|
| ESS total score | 4.5 ± 2.8 | 4.0 ± 2.9 | 5.3 ± 3.4 | H(2, N = 44) = 0.14, p = 0.93 | NS |
| PSQI total score | 2.3 ± 1.4 | 8.1 ± 2.9 | 4.6 ± 2.1 | H(2, N = 42) = 26.6, p < 0.001 | HC < KS < AUD |
| Component 1: subjective sleep quality | 0.3 ± 0.5 | 1.3 ± 0.7 | 0.6 ± 0.5 | H(2, N = 42) = 17.85, p < 0.001 | HC = KS < AUD |
| Component 2: sleep latency | 0.5 ± 0.5 | 1.8 ± 1.1 | 1.1 ± 1 | H(2, N = 42) = 11.47, p = 0.033 | HC < AUD; HC = KS; AUD = KS |
| Component 3: sleep duration | 0.3 ± 0.4 | 1.3 ± 0.9 | 0.1 ± 0.4 | H(2, N = 42) = 17.21, p < 0.001 | HC = KS < AUD |
| Component 4: habitual sleep efficiency | 0.1 ± 0.3 | 1.2 ± 1 | 0.4 ± 0.8 | H(2, N = 44) = 12.45, p = 0.002 | HC < AUD; HC = KS; AUD = KS |
| Component 5: sleep disturbances | 0.7 ± 0.5 | 0.9 ± 0.4 | 0.9 ± 0.4 | H(2, N = 44) = 3.59, p = 0.16 | NS |
| Component 6: use of sleeping medication | 0 ± 0 | 0.4 ± 1.1 | 0.8 ± 1.5 | H(2, N = 44) = 3.97, p = 0.13 | NS |
| Component 7: daytime dysfunction | 0.1 ± 0.3 | 1 ± 0.4 | 0.6 ± 1.1 | H(2, N = 42) = 10.17, p = 0.006 | HC < AUD; HC = KS; AUD = KS |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Laniepce, A.; Segobin, S.; André, C.; Bertran, F.; Boudehent, C.; Lahbairi, N.; Maillard, A.; Mary, A.; Urso, L.; Vabret, F.; et al. Distinct Sleep Alterations in Alcohol Use Disorder Patients with and without Korsakoff’s Syndrome: Relationship with Episodic Memory. J. Clin. Med. 2023, 12, 2440. https://doi.org/10.3390/jcm12062440
Laniepce A, Segobin S, André C, Bertran F, Boudehent C, Lahbairi N, Maillard A, Mary A, Urso L, Vabret F, et al. Distinct Sleep Alterations in Alcohol Use Disorder Patients with and without Korsakoff’s Syndrome: Relationship with Episodic Memory. Journal of Clinical Medicine. 2023; 12(6):2440. https://doi.org/10.3390/jcm12062440
Chicago/Turabian StyleLaniepce, Alice, Shailendra Segobin, Claire André, Françoise Bertran, Céline Boudehent, Najlaa Lahbairi, Angéline Maillard, Alison Mary, Laurent Urso, François Vabret, and et al. 2023. "Distinct Sleep Alterations in Alcohol Use Disorder Patients with and without Korsakoff’s Syndrome: Relationship with Episodic Memory" Journal of Clinical Medicine 12, no. 6: 2440. https://doi.org/10.3390/jcm12062440