
Remineralization Potential of Three Restorative Glass Ionomer Cements: An In Vitro Study

Abstract
:1. Introduction
2. Materials and Methods
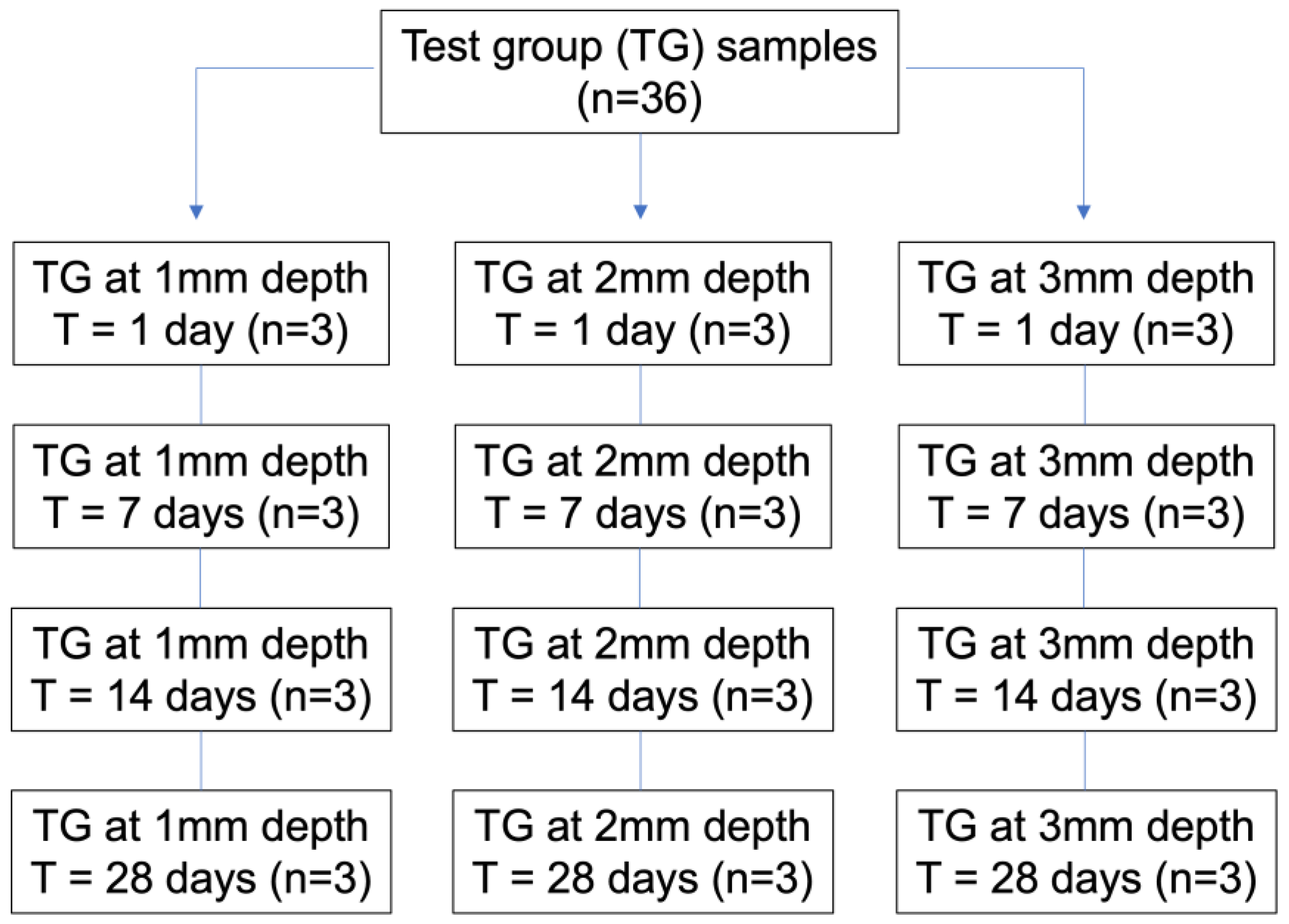
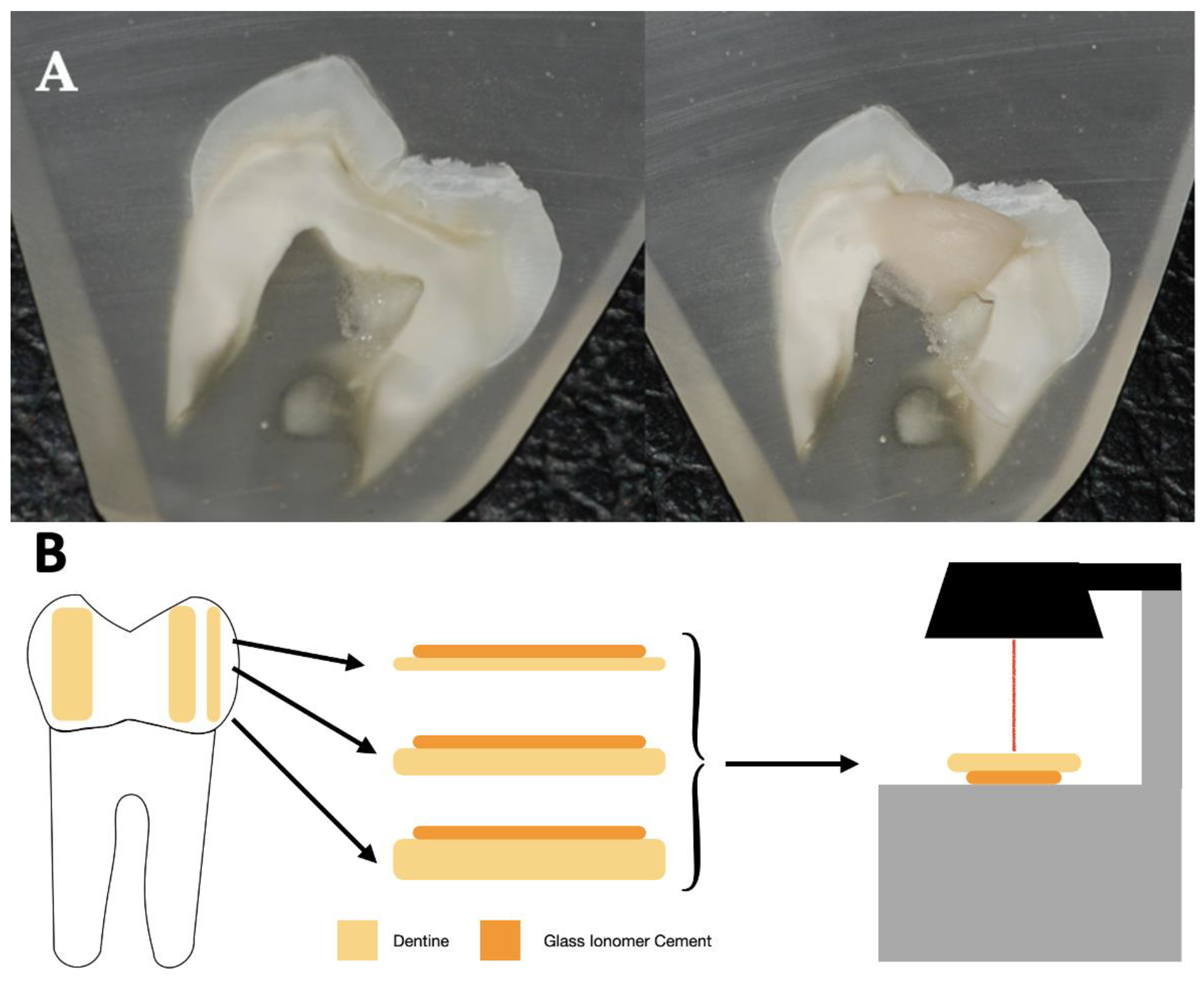
2.1. Sample Preparation
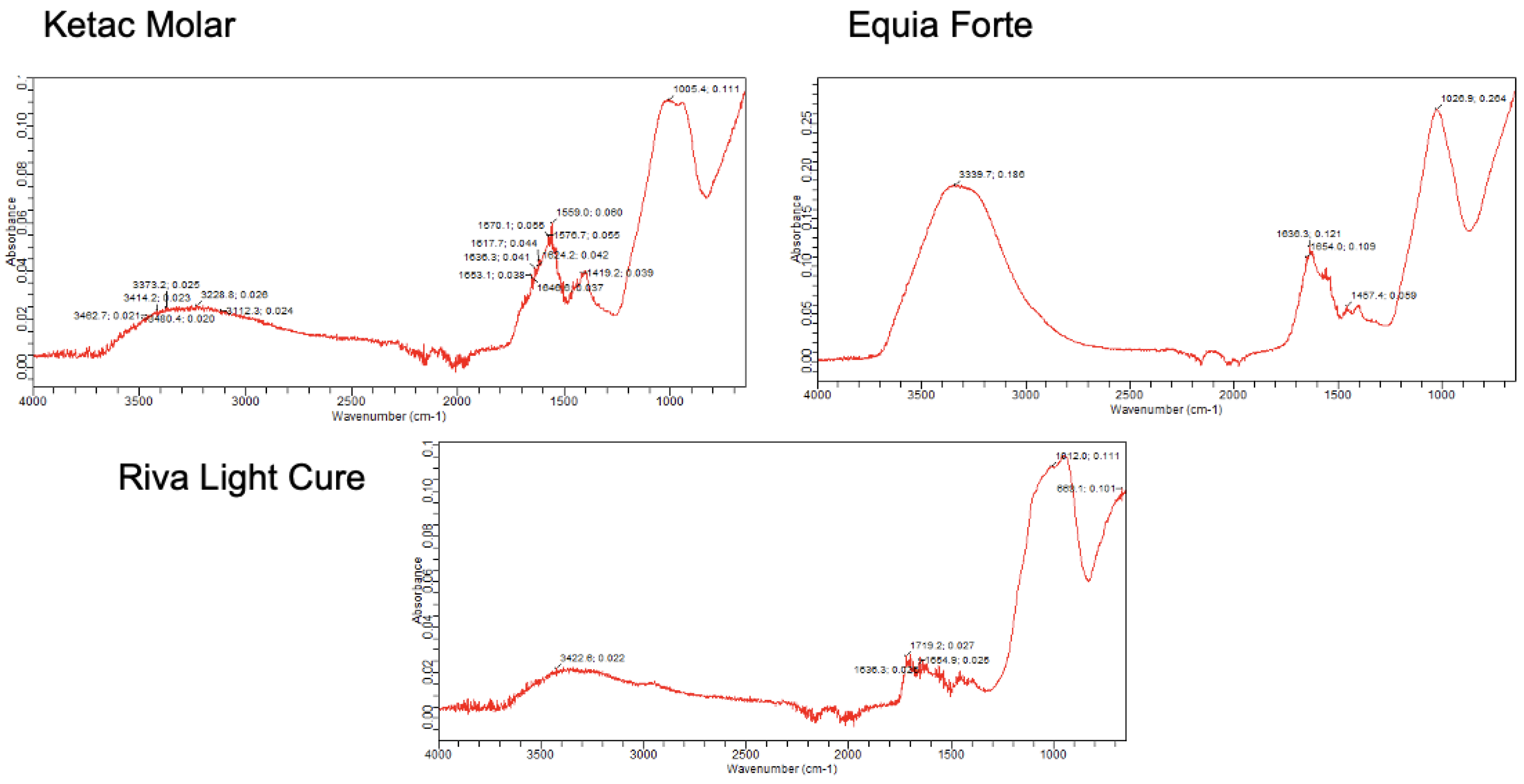
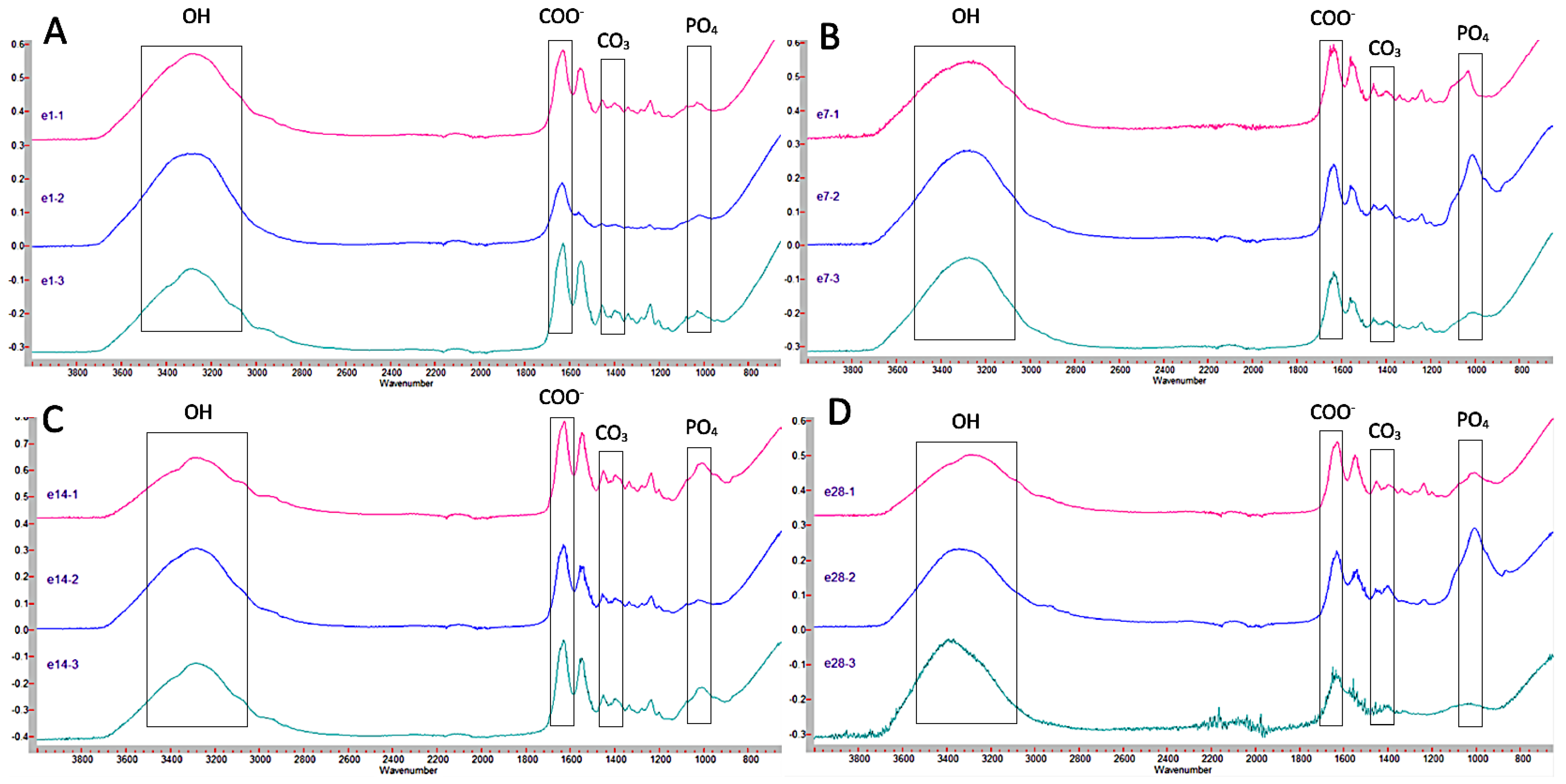
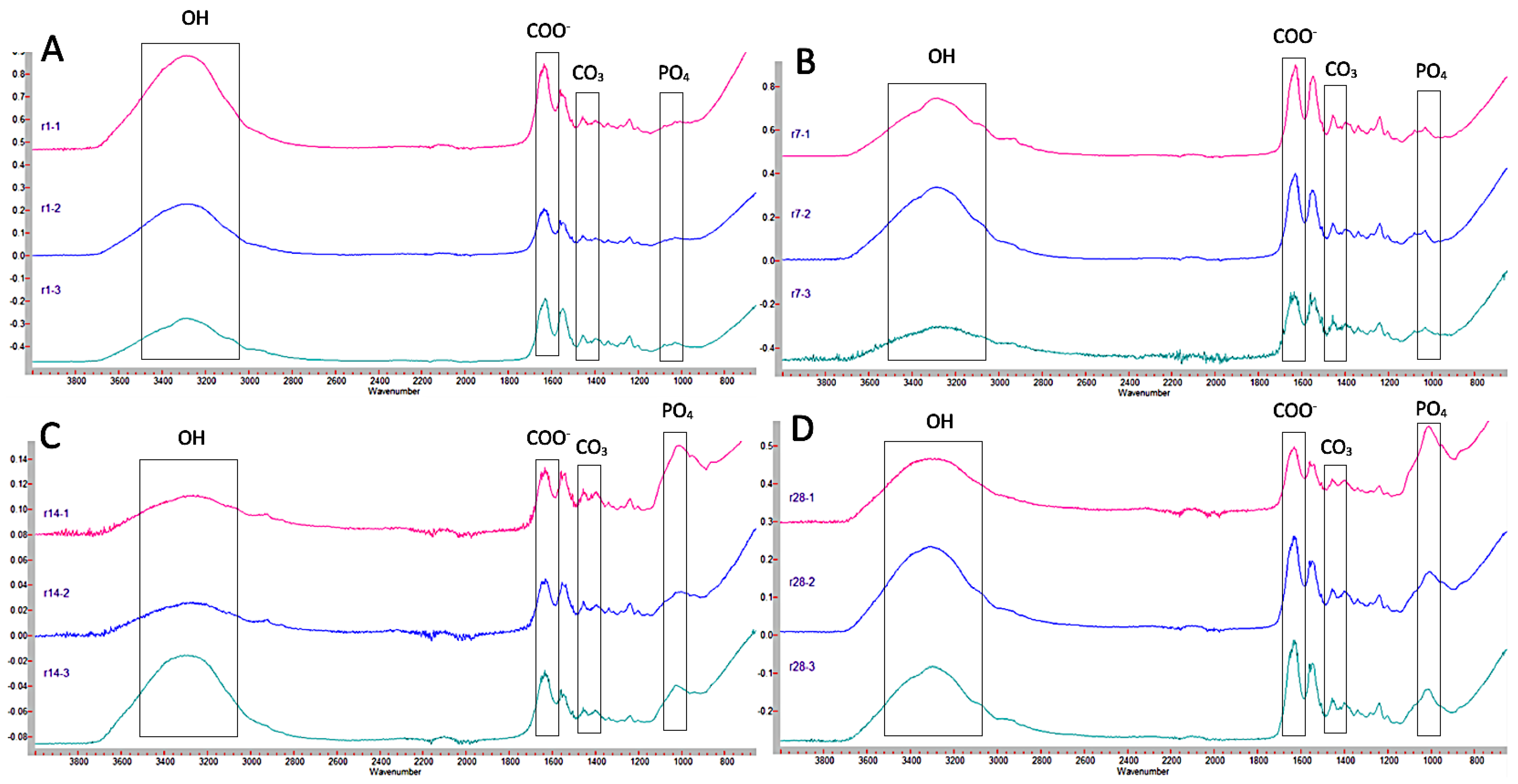
2.2. Fourier Transform Infrared Spectrometry (FTIR)
- -
- 3000–3700 cm−1: Corresponding with OH group.
- -
- 1636 cm−1: Corresponding with COO− group.
- -
- 1021 cm−1: Corresponding with PO4 groups.
- -
- 820 and 1420 cm−1: corresponding with CO3 group.
- -
- 700 cm−1: Corresponding with P2O7 group.
- -
- The joint presence of PO4 and CO3 together indicates the presence of carbonate hydroxyapatite.
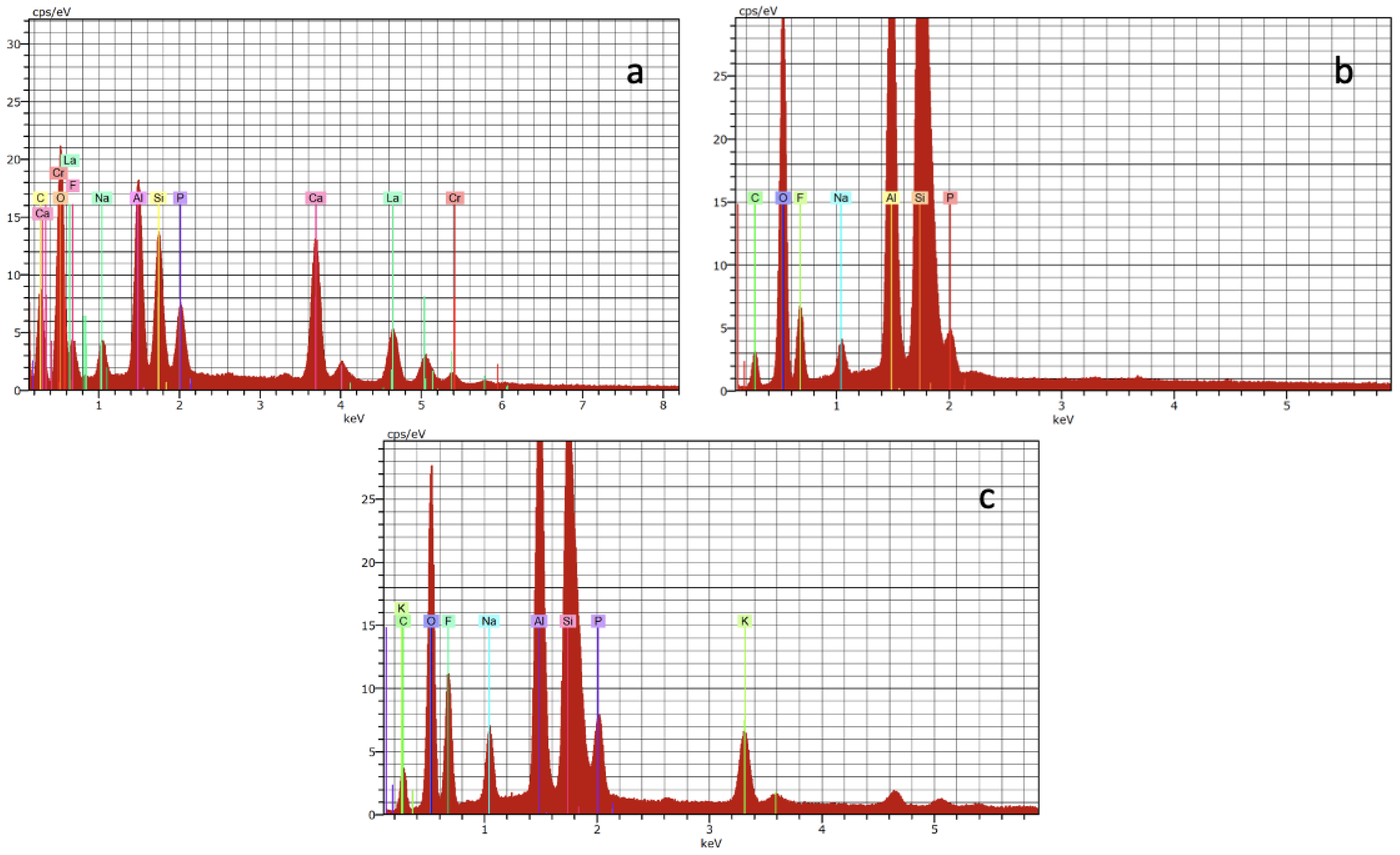
2.3. Energy Dispersive Spectroscopy (EDX)
2.4. Statistical Analysis
3. Results
3.1. Fourier Transform Infrared Spectrometry (FTIR)
3.2. Energy Dispersive Spectroscopy (EDX)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bertassoni, L.E.; Habelitz, S.; Kinney, J.H.; Marshall, S.J.; Marshall, G.W.J. Biomechanical Perspective on the Remineralization of Dentin. Caries Res. 2009, 43, 70–77. [Google Scholar] [CrossRef] [PubMed]
- Abou Neel, E.A.; Aljabo, A.; Strange, A.; Ibrahim, S.; Coathup, M.; Young, A.M.; Bozec, L.; Mudera, V. Demineralization-Remineralization Dynamics in Teeth and Bone. Int. J. Nanomed. 2016, 11, 4743–4763. [Google Scholar] [CrossRef] [PubMed]
- James, S.L.; Abate, D.; Abate, K.H.; Abay, S.M.; Abbafati, C.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F.; Abdela, J.; Abdelalim, A.; et al. Global, Regional, and National Incidence, Prevalence, and Years Lived with Disability for 354 Diseases and Injuries for 195 Countries and Territories, 1990–2017: A Systematic Analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1789–1858. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fusayama, T.; Okuse, K.; Hosoda, H. Relationship between Hardness, Discoloration, and Microbial Invasion in Carious Dentin. J. Dent. Res. 1966, 45, 1033–1046. [Google Scholar] [CrossRef]
- Barros, M.M.A.F.; de Queiroz Rodrigues, M.I.; Muniz, F.W.M.G.; Rodrigues, L.K.A. Selective, Stepwise, or Nonselective Removal of Carious Tissue: Which Technique Offers Lower Risk for the Treatment of Dental Caries in Permanent Teeth? A Systematic Review and Meta-Analysis. Clin. Oral. Investig. 2020, 24, 521–532. [Google Scholar] [CrossRef]
- Innes, N.P.T.; Frencken, J.E.; Bjørndal, L.; Maltz, M.; Manton, D.J.; Ricketts, D.; van Landuyt, K.; Banerjee, A.; Campus, G.; Doméjean, S.; et al. Managing Carious Lesions: Consensus Recommendations on Terminology. Adv. Dent. Res. 2016, 28, 49–57. [Google Scholar] [CrossRef] [Green Version]
- Dai, L.; Liu, Y.; Salameh, Z.; Khan, S.; Mao, J.; Pashley, D.H.; Tay, F.R. Can Caries-Affected Dentin Be Completely Remineralized by Guided Tissue Remineralization? Dent. Hypotheses 2011, 2, 74–82. [Google Scholar] [CrossRef]
- Gao, W.; Smales, R.J.; Yip, H.K. Demineralisation and Remineralisation of Dentine Caries, and the Role of Glass-Ionomer Cements. Int. Dent. J. 2000, 50, 51–56. [Google Scholar] [CrossRef]
- Sidhu, S.K.; Nicholson, J.W. A Review of Glass-Ionomer Cements for Clinical Dentistry. J. Funct. Biomater. 2016, 7, 16. [Google Scholar] [CrossRef]
- Nicholson, J.W.; Brookman, P.J.; Lacy, O.M.; Wilson, A.D. Fourier Transform Infrared Spectroscopic Study of the Role of Tartaric Acid in Glass-Ionomer Dental Cements. J. Dent. Res. 1988, 67, 1451–1454. [Google Scholar] [CrossRef]
- Berzins, D.W.; Abey, S.; Costache, M.C.; Wilkie, C.A.; Roberts, H.W. Resin-Modified Glass-Ionomer Setting Reaction Competition. J. Dent. Res. 2010, 89, 82–86. [Google Scholar] [CrossRef] [PubMed]
- He, L.; Hao, Y.; Zhen, L.; Liu, H.; Shao, M.; Xu, X.; Liang, K.; Gao, Y.; Yuan, H.; Li, J.; et al. Biomineralization of Dentin. J. Struct. Biol. 2019, 207, 115–122. [Google Scholar] [CrossRef] [PubMed]
- Kong, W.; Du, Q.; Qu, Y.; Shao, C.; Chen, C.; Sun, J.; Mao, C.; Tang, R.; Gu, X. Tannic Acid Induces Dentin Biomineralization by Crosslinking and Surface Modification. RSC Adv. 2022, 12, 3454–3464. [Google Scholar] [CrossRef]
- Jang, J.-H.; Lee, M.G.; Ferracane, J.L.; Davis, H.; Bae, H.E.; Choi, D.; Kim, D.-S. Effect of Bioactive Glass-Containing Resin Composite on Dentin Remineralization. J. Dent. 2018, 75, 58–64. [Google Scholar] [CrossRef] [PubMed]
- Kranz, S.; Heyder, M.; Mueller, S.; Guellmar, A.; Krafft, C.; Nietzsche, S.; Tschirpke, C.; Herold, V.; Sigusch, B.; Reise, M. Remineralization of Artificially Demineralized Human Enamel and Dentin Samples by Zinc-Carbonate Hydroxyapatite Nanocrystals. Materials 2022, 15, 7173. [Google Scholar] [CrossRef] [PubMed]
- Sobh, E.G.; Hamama, H.H.; Palamara, J.; Mahmoud, S.H.; Burrow, M.F. Effect of CPP-ACP Modified-GIC on Prevention of Demineralization in Comparison to Other Fluoride-Containing Restorative Materials. Aust. Dent. J. 2022, 67, 220–229. [Google Scholar] [CrossRef]
- Gandolfi, M.G.; Taddei, P.; Siboni, F.; Modena, E.; De Stefano, E.D.; Prati, C. Biomimetic remineralization of human dentin using promising innovative calcium-silicate hybrid “smart” materials. Dent. Mater. 2011, 27, 1055–1069. [Google Scholar] [CrossRef]
- Sajini, S.I.; Alshawi, B.A.; Alharbi, L.M. Assessment of remineralisation potentials of bioactive dental composite using an in-vitro demineralised dentine model. J. Taibah Univ. Sci. 2022, 17, 640–647. [Google Scholar] [CrossRef] [PubMed]
- Liang, K.; Xiao, S.; Shi, W.; Li, J.; Yang, X.; Gao, Y.; Gou, Y.; Hao, L.; He, L.; Cheng, L.; et al. 8DSS-promoted remineralization of demineralized dentin in vitro. J. Mater. Chem. B 2015, 3, 6763–6772. [Google Scholar] [CrossRef]
- Schwendicke, F. Contemporary Concepts in Carious Tissue Removal: A Review. J. Esthet. Restor. Dent. 2017, 29, 403–408. [Google Scholar] [CrossRef]
- de Oliveira Roma, F.R.V.; de Oliveira, T.J.L.; Bauer, J.; Firoozmand, L.M. Resin-Modified Glass Ionomer Enriched with BIOGLASS: Ion-Release, Bioactivity and Antibacterial Effect. J. Biomed. Mater. Res. B. Appl. Biomater. 2023, 111, 903–911. [Google Scholar] [CrossRef] [PubMed]
- Valizadeh, S.; Kamangar, S.S.H.; Nekoofar, M.H.; Behroozibakhsh, M.; Shahidi, Z. Comparison of Dentin Caries Remineralization with Four Bioactive Cements. Eur. J. Prosthodont. Restor. Dent. 2022, 30, 223–229. [Google Scholar] [CrossRef] [PubMed]
- Daneshpoor, N.; Pishevar, L. Comparative Evaluation of Bioactive Cements on Biomimetic Remineralization of Dentin. J. Clin. Exp. Dent. 2020, 12, e291–e299. [Google Scholar] [CrossRef]
- Simila, H.O.; Karpukhina, N.; Hill, R.G. Bioactivity and Fluoride Release of Strontium and Fluoride Modified Biodentine. Dent. Mater. 2018, 34, e1–e7. [Google Scholar] [CrossRef]
- Correa, D.; Almirall, A.; García-Carrodeguas, R.; dos Santos, L.; de Aza, A.H.; Parra, J.; Ángel Delgado, J. β-Dicalcium Silicate-Based Cement: Synthesis, Characterization and in Vitro Bioactivity and Biocompatibility Studies. J. Biomed. Mater. Res. A 2014, 102, 3693–3703. [Google Scholar] [CrossRef] [PubMed]
- Chen, B.; Haapasalo, M.; Mobuchon, C.; Li, X.; Ma, J.; Shen, Y. Cytotoxicity and the Effect of Temperature on Physical Properties and Chemical Composition of a New Calcium Silicate-Based Root Canal Sealer. J. Endod. 2020, 46, 531–538. [Google Scholar] [CrossRef] [PubMed]
- Camilleri, J. Sealers and Warm Gutta-Percha Obturation Techniques. J. Endod. 2015, 41, 72–78. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Z.; Ge, X.; Bian, M.; Xu, T.; Li, N.; Lu, J.; Yu, J. Remineralization of Dentin Slices Using Casein Phosphopeptide-Amorphous Calcium Phosphate Combined with Sodium Tripolyphosphate. Biomed. Eng. Online 2020, 19, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Song, F.V.; Yang, B.; Di Tommaso, D.; Donnan, R.S.; Chass, G.A.; Yada, R.Y.; Farrare, D.H.; Tian, K.V. Resolving nanoscopic structuring and interfacial THz dynamics in setting cements. Mater. Adv. 2022, 3, 4982–4990. [Google Scholar] [CrossRef]
- Kun, V.T.; Chass, G.A.; Di Tommaso, D. Simulations reveal the role of composition into the atomic-level flexibility of bioactive glass cements. Phys. Chem. Chem. Phys. 2016, 18, 837. [Google Scholar]
- Thuy, T.T.; Nakagaki, H.; Kato, K.; Hung, P.A.; Inukai, J.; Tsuboi, S.; Nakagaki, H.; Hirose, M.N.; Igarashi, S.; Robinson, C. Effect of Strontium in Combination with Fluoride on Enamel Remineralization in Vitro. Arch. Oral. Biol. 2008, 53, 1017–1022. [Google Scholar] [CrossRef] [PubMed]
- Dai, L.L.; Mei, M.L.; Chu, C.H.; Lo, E.C.M. Remineralizing Effect of a New Strontium-Doped Bioactive Glass and Fluoride on Demineralized Enamel and Dentine. J. Dent. 2021, 108, 103633. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.Z.; Cao, Y.; Liu, W.; Chu, C.H.; Li, Q.L. Polydopamine-induced tooth remineralization. ACS Appl. Mater. Interfaces 2012, 4, 6901–6910. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Material | Composition | Manufacturer | Batch N° |
|---|---|---|---|
| Ketac Molar Aplicap (KM) | Liquid: water, copolymer, polyacrylic acid, maleic and tartaric acid Powder: aluminum-calcium-lanthanum fluorosilicate glass | 3M ESPE® Seefeld, Germany | 56420 |
| Equia Forte HT (EF) | Liquid: polycarboxylic acid, water Powder: strontium fluoro aluminum silicate glass, iron oxide | GC Corp®, Tokio, Japan | 901584 |
| Riva Light Cure HV (RL) | Liquid: polyacrylic acid, tartaric acid, HEMA Powder: bioactive glass (Ionglass™), contains fluoride and strontium ions. | SDI® Victoria, Australia | 873003 |
| 1 Day | 7 Days | 14 Days | 28 Days | |
|---|---|---|---|---|
| KM 1 mm | 2.23 ± 0.6 | 2.46 ± 0.7 | 2.84 ± 0.9 | 1.85 ± 0.8 |
| KM 2 mm | 1.52 ± 0.3 | 1.24 ± 0.2 | 1.93 ± 0.4 | 1.76 ± 0.5 |
| KM 3 mm | 1.17 ± 0.1 | 1.94 ± 0.4 | 2.12 ± 0.5 | 1.65 ± 0.6 |
| EF 1 mm | 1.09 ± 0.2 | 2.01 ± 0.7 | 1.01 ± 0.1 | 1.74 ± 0.5 |
| EF 2 mm | 2.21 ± 0.9 | 2.37 ± 0.8 | 2.12 ± 0.3 | 1.94 ± 0.2 |
| EF 3 mm | 1.91 ± 0.7 | 2.16 ± 0.6 | 1.72 ± 0.2 | 1.11 ± 0.4 |
| RL 1 mm | 1.98 ± 0.6 | 1.34 ± 0.5 | 1.83 ± 0.4 | 2.01 ± 0.5 |
| RL 2 mm | 1.65 ± 0.5 | 2.44 ± 0.7 | 1.69 ± 0.5 | 1.94 ± 0.6 |
| RL 3 mm | 2.09 ± 0.6 | 1.94 ± 0.3 | 1.72 ± 0.3 | 1.11 ± 0.2 |
| 1 Day | 7 Days | 14 Days | 28 Days | |
|---|---|---|---|---|
| KM 1 mm | 34.10 | 40.15 | 48.18 | 20.54 a |
| KM 2 mm | 3.50 | −18.33 | 23.88 | 16.70 a |
| KM 3 mm | −25.16 | 24.09 | 30.65 | 10.69 |
| EF 1 mm | −35.05 | 26.89 | −45.48 | 15.58 |
| EF 2 mm | 33.52 | 38.00 | 30.65 | 24.41 |
| EF 3 mm | 22.89 | 31.90 | 14.59 | −32.68 |
| RL 1 mm | 25.63 a | −9.59 | 19.49 | 26.91 a |
| RL 2 mm | 10.94 | 39.82 | 12.90 a | 24.41 a |
| RL 3 mm | 29.80 a | 24.09 | 14.59 a | −32.68 |
| 1 Day | 7 Days | 14 Days | 28 Days | |
|---|---|---|---|---|
| KM 1 mm | 37.24 | 43.00 | 50.64 | 24.33 a |
| KM 2 mm | 8.10 | −12.69 | 27.51 | 20.66 a |
| KM 3 mm | −19.20 | 27.70 | 33.96 | 14.94 |
| EF 1 mm | −28.62 | 30.37 a | −38.55 | 19.60 |
| EF 2 mm | 36.68 | 40.96 | 33.95 | 28.01 |
| EF 3 mm | 26.56 | 35.14 a | 18.66 | −26.36 |
| RL 1 mm | 29.18 | −4.37 | 23.32 | 30.40 a |
| RL 2 mm | 15.18 | 42.68 | 17.05 a | 28.01 a |
| RL 3 mm | 33.14 | 27.70 | 18.66 a | −26.36 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ghilotti, J.; Fernández, I.; Sanz, J.L.; Melo, M.; Llena, C. Remineralization Potential of Three Restorative Glass Ionomer Cements: An In Vitro Study. J. Clin. Med. 2023, 12, 2434. https://doi.org/10.3390/jcm12062434
Ghilotti J, Fernández I, Sanz JL, Melo M, Llena C. Remineralization Potential of Three Restorative Glass Ionomer Cements: An In Vitro Study. Journal of Clinical Medicine. 2023; 12(6):2434. https://doi.org/10.3390/jcm12062434
Chicago/Turabian StyleGhilotti, James, Icíar Fernández, José Luis Sanz, María Melo, and Carmen Llena. 2023. "Remineralization Potential of Three Restorative Glass Ionomer Cements: An In Vitro Study" Journal of Clinical Medicine 12, no. 6: 2434. https://doi.org/10.3390/jcm12062434