
Management of Pelvic Fracture Urethral Injury: Is Supracrural Urethral Rerouting (Step 4) Becoming Anecdotical or Does It Remain in Force?

 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Preoperative Evaluation
2.3. Clinical Outcomes
2.4. Statistical Tests
3. Results
3.1. Baseline Characteristics
3.2. Urethroplasty Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Latini, J.M.; McAninch, J.W.; Brandes, S.B.; Chung, J.Y.; Rosenstein, D. SIU/ICUD Consultation On Urethral Strictures: Epidemiology, etiology, anatomy, and nomenclature of urethral stenoses, strictures, and pelvic fracture urethral disruption injuries. Urology 2014, 83, S1–S7. [Google Scholar] [CrossRef] [PubMed]
- Kulkarni, S.B.; Joshi, P.; Ramírez Pérez, E.A. Surgical Reconstruction of Pelvic Fracture Urethral Injury. In Textbook of Male Genitourethral Reconstruction; Martins, F.E., Kulkarni, S.B., Köhler, T.S., Eds.; Springer International Publishing: Cham, Switzerland, 2020; pp. 253–265. [Google Scholar]
- Andrich, D.E.; Mundy, A.R. The nature of urethral injury in cases of pelvic fracture urethral trauma. J. Urol. 2001, 165, 1492–1495. [Google Scholar] [CrossRef] [PubMed]
- Mouraviev, V.B.; Santucci, R.A. Cadaveric anatomy of pelvic fracture urethral distraction injury: Most injuries are distal to the external urinary sphincter. J. Urol. 2005, 173, 869–872. [Google Scholar] [CrossRef] [PubMed]
- Sreeranga, Y.L.; Joshi, P.M.; Bandini, M.; Kulkarni, S.B. Comprehensive analysis of paediatric pelvic fracture urethral injury: A reconstructive centre experience. BJU Int. 2022, 130, 114–125. [Google Scholar] [CrossRef] [PubMed]
- Webster, G.D.; Ramon, J. Repair of pelvic fracture posterior urethral defects using an elaborated perineal approach: Experience with 74 cases. J. Urol. 1991, 145, 744–748. [Google Scholar] [CrossRef] [PubMed]
- Webster, G.D.; Goldwasser, B. Perineal transpubic repair: A technique for treating post-traumatic prostatomembranous urethral strictures. J. Urol. 1986, 135, 278–279. [Google Scholar] [CrossRef]
- Webster, G.D.; Peterson, A.C. Simple perineal and elaborated perineal posterior urethroplasty. Arab. J. Urol. 2015, 13, 17–23. [Google Scholar] [CrossRef]
- Kulkarni, S.B.; Bandini, M.; Patil, A.; Bhadranavar, S.; Sharma, V.; Bafna, S.; Yatam, S.L.; Barbagli, G.; Montorsi, F.; Joshi, P.M. The Right Instrument for the Right Purpose: Spreading the Use of Small Caliber Ureteroscope for the Inspection of the Male and Female Urethra. Société Int. D’urologie J. 2021, 2, 259–263. [Google Scholar] [CrossRef]
- Joshi, P.M.; Desai, D.J.; Shah, D.; Joshi, D.P.; Kulkarni, S.B. Magnetic resonance imaging procedure for pelvic fracture urethral injuries and recto urethral fistulas: A simplified protocol. Turk. J. Urol. 2021, 47, 35–42. [Google Scholar] [CrossRef]
- Joshi, P.; Bandini, M.; Montorsi, F.; Kulkarni, S.B. Challenging the dogma of 6 steps for anastomotic urethroplasty in posterior urethral stricture: Introducing step 3a. World J. Urol. 2022, 40, 1277–1278. [Google Scholar] [CrossRef]
- Jackson, M.J.; Sciberras, J.; Mangera, A.; Brett, A.; Watkin, N.; N'Dow, J.M.; Chapple, C.R.; Andrich, D.E.; Pickard, R.S.; Mundy, A.R. Defining a patient-reported outcome measure for urethral stricture surgery. Eur. Urol. 2011, 60, 60–68. [Google Scholar] [CrossRef]
- Rosen, R.C.; Riley, A.; Wagner, G.; Osterloh, I.H.; Kirkpatrick, J.; Mishra, A. The international index of erectile function (IIEF): A multidimensional scale for assessment of erectile dysfunction. Urology 1997, 49, 822–830. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kulkarni, S.B.; Barbagli, G.; Kulkarni, J.S.; Romano, G.; Lazzeri, M. Posterior urethral stricture after pelvic fracture urethral distraction defects in developing and developed countries, and choice of surgical technique. J. Urol. 2010, 183, 1049–1054. [Google Scholar] [CrossRef] [PubMed]
- Barbagli, G. History and evolution of transpubic urethroplasty: A lesson for young urologists in training. Eur. Urol. 2007, 52, 1290–1292. [Google Scholar] [CrossRef] [PubMed]
- Cooperberg, M.R.; McAninch, J.W.; Alsikafi, N.F.; Elliott, S.P. Urethral reconstruction for traumatic posterior urethral disruption: Outcomes of a 25-year experience. J. Urol. 2007, 178, 2006–2010, discussion 2010. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koraitim, M.M. Predictors of surgical approach to repair pelvic fracture urethral distraction defects. J. Urol. 2009, 182, 1435–1439. [Google Scholar] [CrossRef] [PubMed]
- Flynn, B.J.; Delvecchio, F.C.; Webster, G.D. Perineal repair of pelvic fracture urethral distraction defects: Experience in 120 patients during the last 10 years. J. Urol. 2003, 170, 1877–1880. [Google Scholar] [CrossRef]
- Kizer, W.S.; Armenakas, N.A.; Brandes, S.B.; Cavalcanti, A.G.; Santucci, R.A.; Morey, A.F. Simplified reconstruction of posterior urethral disruption defects: Limited role of supracrural rerouting. J. Urol. 2007, 177, 1378–1381, discussion 1381–1372. [Google Scholar] [CrossRef] [Green Version]
- Hosseini, S.J.; Rezaei, A.; Mohammadhosseini, M.; Rezaei, I.; Javanmard, B. Supracrural rerouting as a technique for resolution of posterior urethral disruption defects. Urol. J. 2009, 6, 204–207. [Google Scholar]
- Singh, S.K.; Pawar, D.S.; Khandelwal, A.K.; Jagmohan. Transperineal bulboprostatic anastomotic repair of pelvic fracture urethral distraction defect and role of ancillary maneuver: A retrospective study in 172 patients. Urol. Ann. 2010, 2, 53–57. [Google Scholar] [CrossRef]
- Johnsen, N.V.; Moses, R.A.; Elliott, S.P.; Vanni, A.J.; Baradaran, N.; Greear, G.; Smith, T.G., 3rd; Granieri, M.A.; Alsikafi, N.F.; Erickson, B.A.; et al. Multicenter analysis of posterior urethroplasty complexity and outcomes following pelvic fracture urethral injury. World J. Urol. 2020, 38, 1073–1079. [Google Scholar] [CrossRef] [Green Version]
- Joshi, P.M.; Bandini, M.; Yepes, C.; Bafna, S.; Bhadranavar, S.; Sharma, V.; Cirulli, G.O.; Kulkarni, S.B. Flaps for bulbar urethral ischemic necrosis in pelvic fracture urethral injury. Plast. Aesthetic Res. 2022, 9, 22. [Google Scholar] [CrossRef]
- Guan, Y.; Wendong, S.; Zhao, S.; Liu, T.; Liu, Y.; Zhang, X.; Yuan, M. The vascular and neurogenic factors associated with erectile dysfunction in patients after pelvic fractures. Int. Braz. J. Urol. 2015, 41, 959–966. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joshi, P.M.; Batra, V.; Kulkarni, S.B. Controversies in the management of pelvic fracture urethral distraction defects. Turk. J. Urol. 2019, 45, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Clavien, P.A.; Barkun, J.; de Oliveira, M.L.; Vauthey, J.N.; Dindo, D.; Schulick, R.D.; de Santibañes, E.; Pekolj, J.; Slankamenac, K.; Bassi, C.; et al. The Clavien-Dindo classification of surgical complications: Five-year experience. Ann. Surg. 2009, 250, 187–196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andrich, D.E.; O’Malley, K.J.; Summerton, D.J.; Greenwell, T.J.; Mundy, A.R. The type of urethroplasty for a pelvic fracture urethral distraction defect cannot be predicted preoperatively. J. Urol. 2003, 170, 464–467. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable | Overall |
|---|---|
| Urethroplasty | |
| Primary, n (%) | 346 (47) |
| Redo, n (%) | 391 (53) |
| Age, years, median (IQR) | 28 (7–72) |
| Stricture etiology, n (%) | |
| Pelvic blunt trauma | 737 (100) |
| Defect size, cm, median (IQR) | |
| Primary | 3 (1–6) |
| Redo | 6 (1–12) |
| Outcome | |
| Success, n (%) | 577 (78.2) |
| Recurrence, n (%) | 160 (21.8) |
| Site of injury, n (%) | |
| Posterior urethra | 737 (100) |
| Initial Management, n (%) | |
| Suprapubic catheter | 700 (95) |
| Realignment | 37 (5) |
| Surgical Procedure | No. of Patients | Success Rate |
|---|---|---|
| Circumferential urethral mobilization | 140 (18.8%) | 104 (74.2%) |
| Corporeal body separation | 130 (17.6%) | 118 (91%) |
| Inferior wedge pubectomy | 345 (46.8%) | 257 (74.4%) |
| Substeps | 34 (3a), 311 (3b) | |
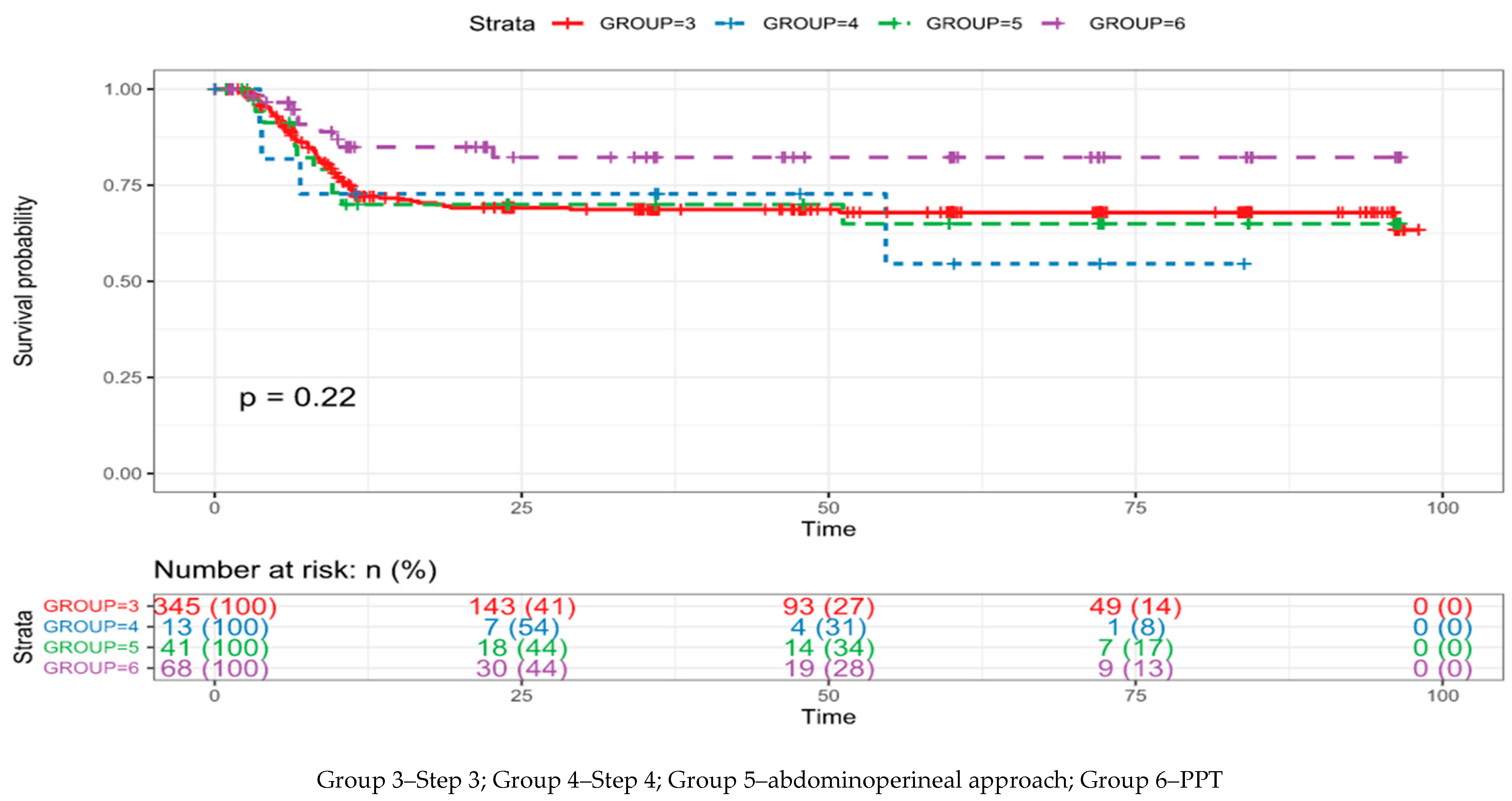
| Supracrural urethral rerouting | 13 (1.8%) | 9 (69.2%) |
| Abdominoperineal approach | 41 (5.6%) | 30 (74.4%) |
| Pedicled preputial tube | 68 (9.2%) | 59 (86.4%) |
| Variable | Overall |
|---|---|
| Median age (range) | 19 (9–40) |
| Stenosis etiology Pelvic trauma | 13 (100%) |
| Primary cases Redo cases | 2 (15.4%) 11 (84.6%) |
| Erectile dysfunction | 6 (46.1%) |
| Success rate Recurrence Final success rate | 9 (69.2%) 4 (30.8%) 11 (84.6%) |
| Authors and Year of Publication | Patients (n) | Supracrural Urethral Rerouting (Step 4) (n) | Success Rate (%) |
|---|---|---|---|
| Webster et al. [6], 1991 | 74 | 11 | 87 |
| Flynn et al. [18], 2003 | 120 | 46 | - |
| Kizer et al. [19], 2007 | 142 | 4 | 25 |
| Hosseini et al. [20], 2009 | 200 | 11 | 18.2 |
| Singh et al. [21], 2010 | 172 | 3 | 66.6 |
| Kulkarni et al. [14], 2010 | 255 | 4 | 100 |
| Johnsen et al. [22], 2019 | 122 | 2 | 100 |
| Joshi et al. [23], 2023 | 737 | 13 | 84.6 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yepes, C.; Oszczudlowski, M.; Bandini, M.; Joshi, P.M.; Alrefaey, A.; Bhadranavar, S.; Martins, F.E.; Kulkarni, S.B. Management of Pelvic Fracture Urethral Injury: Is Supracrural Urethral Rerouting (Step 4) Becoming Anecdotical or Does It Remain in Force? J. Clin. Med. 2023, 12, 2427. https://doi.org/10.3390/jcm12062427
Yepes C, Oszczudlowski M, Bandini M, Joshi PM, Alrefaey A, Bhadranavar S, Martins FE, Kulkarni SB. Management of Pelvic Fracture Urethral Injury: Is Supracrural Urethral Rerouting (Step 4) Becoming Anecdotical or Does It Remain in Force? Journal of Clinical Medicine. 2023; 12(6):2427. https://doi.org/10.3390/jcm12062427
Chicago/Turabian StyleYepes, Christian, Maciej Oszczudlowski, Marco Bandini, Pankaj M. Joshi, Ahmed Alrefaey, Shreyas Bhadranavar, Francisco E. Martins, and Sanjay B. Kulkarni. 2023. "Management of Pelvic Fracture Urethral Injury: Is Supracrural Urethral Rerouting (Step 4) Becoming Anecdotical or Does It Remain in Force?" Journal of Clinical Medicine 12, no. 6: 2427. https://doi.org/10.3390/jcm12062427