
Up to a 15-Year Survival Rate and Marginal Bone Resorption of 1780 Implants with or without Microthreads: A Multi Center Retrospective Study

Abstract
:1. Introduction
2. Materials and Methods
3. Results
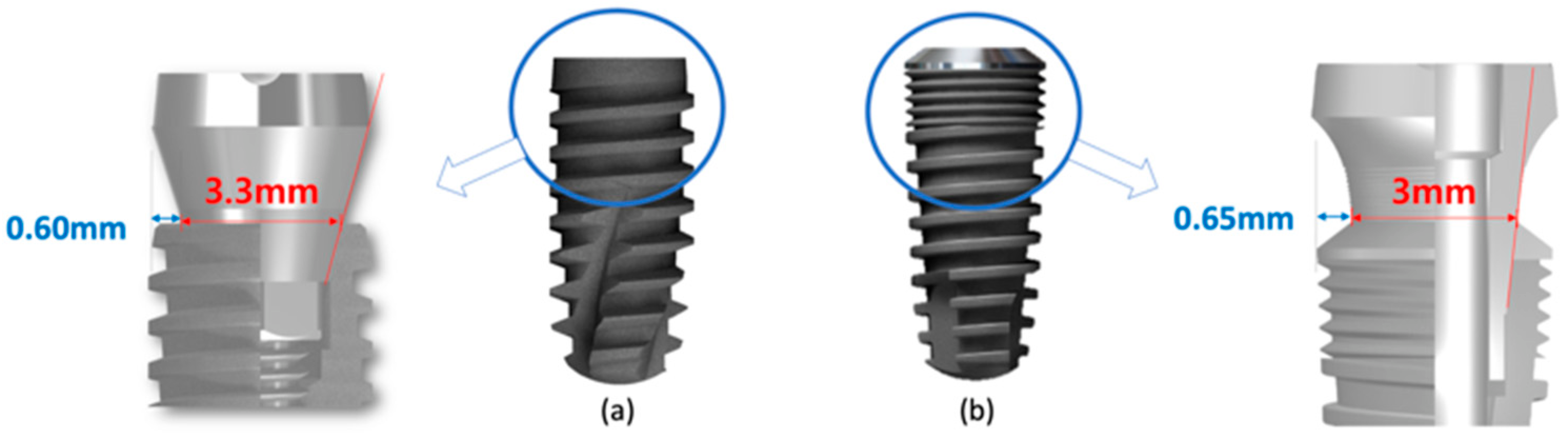
3.1. Description of the Implant and Patient Cohort
3.2. Survival Rate
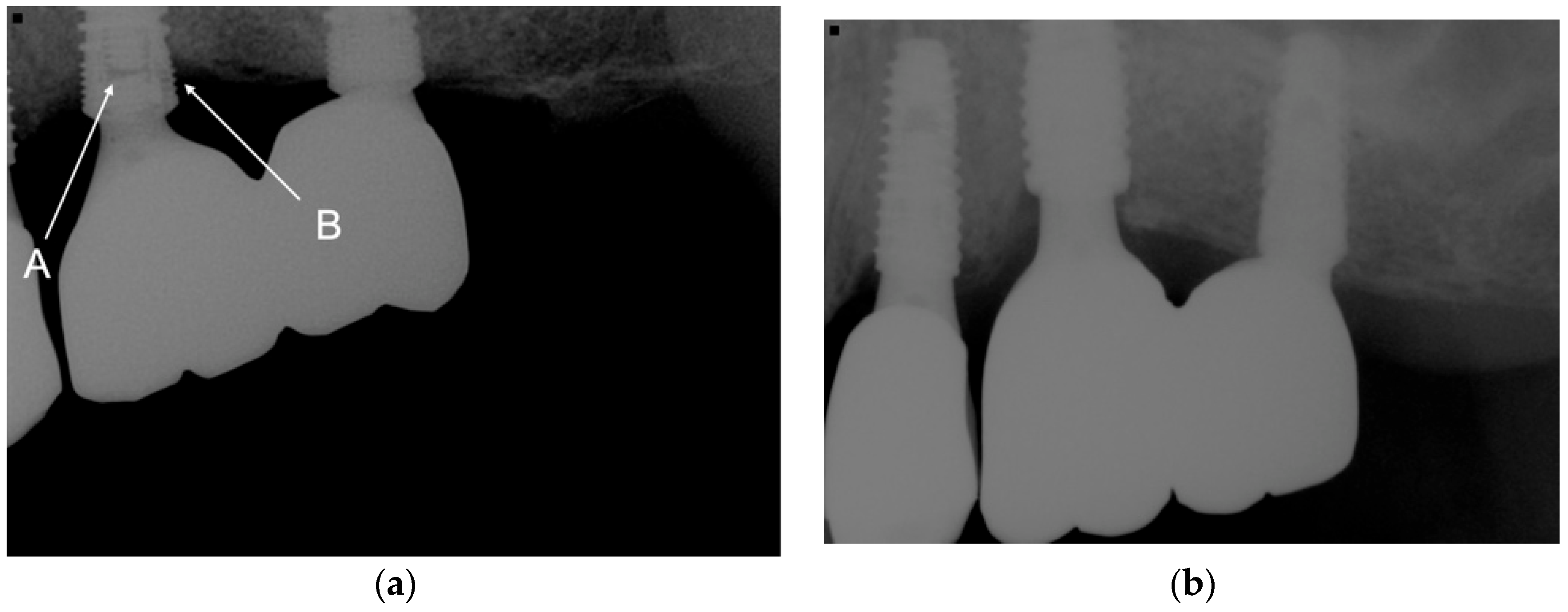
3.3. Bone Level Comparison
3.4. Incidence of Peri-Implantitis
4. Discussion
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Buser, D.; Buser, D.; Mericske-Stern, R.; Bernard, J.P.; Behneke, A.; Behneke, N.; Hirt, H.P.; Belser, U.C.; Lang, N.P. Long-term evaluation of non-submerged ITI implants. Part 1: 8-year life table analsysis of a prospective multi-center study with 2359 implants. Clin. Oral Implant. Res. 1997, 8, 161–172. [Google Scholar] [CrossRef]
- Gracis, S.; Michalakis, K.; Vigolo, P.; Vult von Steyern, P.; Zwahlen, M.; Sailer, I. Internal vs. external connections for abutments/reconstructions: A systematic review. Clin. Oral Implant. Res. 2012, 23 (Suppl. 6), 202–216. [Google Scholar] [CrossRef] [PubMed]
- French, D.; Ofec, R.; Levin, L. Long term clinical performance of 10871 dental implants with up to 22 years of follow-up: A cohort study in 4247 patients. Clin. Implant Dent. Relat. Res. 2021, 23, 289–297. [Google Scholar] [CrossRef] [PubMed]
- Tallarico, M.; Lumbau, A.M.I.; Meloni, S.M.; Ieria, I.; Park, C.J.; Zadrożny, L.; Xhanari, E.; Pisano, M. Five-year prospective study on implant failure and marginal bone remodeling expected using bone level implants with sandblasted/acid-etched surface and conical connection. Eur. J. Dent. 2022, 16, 787–795. [Google Scholar] [CrossRef] [PubMed]
- Atieh, M.A.; Ibrahim, H.M.; Atieh, A.H. Platform switching for marginal bone preservation around dental implants: A systematic review and meta-analysis. J. Periodontol. 2010, 81, 1350–1366. [Google Scholar] [CrossRef]
- Papaspyridakos, P.; Chen, C.J.; Singh, M.; Weber, H.P.; Gallucci, G.O. Success criteria in implant dentistry: A systematic review. J. Dent. Res. 2012, 91, 242–248. [Google Scholar] [CrossRef]
- Cooper, L.F.; Tarnow, D.; Froum, S.; Moriarty, J.; De Kok, I.J. Comparison of marginal bone changes with internal conus and external hexagon design implant systems: A prospective, randomized study. Int. J. Periodontics Restorative Dent. 2016, 36, 631–642. [Google Scholar] [CrossRef]
- Derks, J.; Schaller, D.; Håkansson, J.; Wennström, J.L.; Tomasi, C.; Berglundh, T. Peri-implantitis—Onset and pattern of progression. J. Clin. Periodontol. 2016, 43, 383–838. [Google Scholar] [CrossRef]
- Hansson, S. The implant neck: Smooth or provided with retention elements. A biomechanical approach. Clin. Oral Implants Res. 1999, 10, 394–405. [Google Scholar] [CrossRef]
- Bratu, E.A.; Tandlich, M.; Shapira, L. A rough surface implant neck with microthreads reduces the amount of marginal bone loss: A prospective clinical study. Clin. Oral Implants Res. 2009, 20, 827–832. [Google Scholar] [CrossRef]
- Lee, D.W.; Choi, Y.S.; Park, K.H.; Kim, C.S.; Moon, I.S. Effect of microthread on the maintenance of marginal bone level: A 3-year prospective study. Clin. Oral Implants Res. 2007, 18, 465–470. [Google Scholar] [CrossRef]
- Carossa, M.; Alovisi, M.; Crupi, A.; Ambrogio, G.; Pera, F. Full-Arch Rehabilitation Using Trans-Mucosal Tissue-Level Implants with and without Implant-Abutment Units: A Case Report. Dent. J. 2022, 10, 116. [Google Scholar] [CrossRef]
- Menini, M.; Pesce, P.; Delucchi, F.; Ambrogio, G.; Canepa, C.; Carossa, M.; Pera, F. One-stage versus two-stage technique using two splinted extra-short implants: A multicentric split-mouth study with a one-year follow-up. Clin. Implant. Dent. Relat. Res. 2002, 24, 602–610. [Google Scholar] [CrossRef]
- Lazzara, R.J.; Porter, S.S. Platform switching: A new concept in implant dentistry for controlling postrestorative crestal bone levels. Int. J. Periodontics Restorative Dent. 2006, 26, 9–17. [Google Scholar]
- Mishra, S.K.; Gaddale, R.; Sonnahalli, N.K.; Chowdhary, R. Platform-switching concept in dental implants: A systematic review and meta-analysis of randomized controlled trials with a minimum follow-up of 3 years. Int. J. Oral Maxillofac. Implant. 2021, 36, e97–e109. [Google Scholar] [CrossRef]
- Schrotenboer, J.; Tsao, Y.P.; Kinariwala, V.; Wang, H.L. Effect of microthreads and platform switching on crestal bone stress levels: A finite element analysis. J. Periodontol. 2008, 79, 2166–2172. [Google Scholar] [CrossRef] [Green Version]
- Shin, Y.K.; Han, C.H.; Heo, S.J.; Kim, S.; Chun, H.J. Radiographic evaluation of marginal bone level around implants with different neck designs after 1 year. Int. J. Oral Maxillofac. Implant. 2006, 21, 789–794. [Google Scholar]
- Van de Velde, T.; Collaert, B.; Sennerby, L.; De Bruyn, H. Effect of implant design on preservation of marginal bone in the mandible. Clin. Implant Dent. Relat. Res. 2010, 12, 134–141. [Google Scholar] [CrossRef]
- Cha, H.S.; Kim, Y.S.; Jeon, J.H.; Lee, J.H. Cumulative survival rate and complication rates of single-tooth implant; focused on the coronal fracture of fixture in the internal connection implant. J. Oral Rehabil. 2013, 40, 595–602. [Google Scholar] [CrossRef]
- Wang, K.; Geng, J.; Jones, D.; Xu, W. Comparison of the fracture resistance of dental implants with different abutment taper angles. Mater. Sci. Eng. C Mater. Biol. Appl. 2016, 63, 164–171. [Google Scholar] [CrossRef] [Green Version]
- Jin, X.; Guan, Y.; Ren, J.; Zhao, Y.; Wang, X.; He, F. A retrospective study of 12,538 internal conical connection implants focused on the long-term integrity of implant-abutment complexes. Clin. Oral Implants Res. 2022, 33, 377–390. [Google Scholar] [CrossRef] [PubMed]
- Manzoor, B.; Suleiman, M.; Palmer, R.M. The effects of simulated bone loss on the implant-abutment assembly and likelihood of fracture: An in vitro study. Int. J. Oral Maxillofac. Implant. 2013, 28, 729–738. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, J.H.; Kim, Y.T.; Jeong, S.N.; Kim, N.H.; Lee, D.W. Incidence and pattern of implant fractures: A long-term follow-up multicenter study. Clin. Implant Dent. Relat. Res. 2018, 20, 463–469. [Google Scholar] [CrossRef] [PubMed]
- Yi, Y.; Heo, S.J.; Koak, J.Y.; Kim, S.K. Mechanical complications of implant-supported restorations with internal conical connection implants: A 14-year retrospective study. J. Prosthet. Dent. 2021, in press. [Google Scholar] [CrossRef]
- Chrcanovic, B.R.; Kisch, J.; Larsson, C. Retrospective clinical evaluation of implant-supported single crowns: Mean follow-up of 15 years. Clin. Oral Implants Res. 2019, 30, 691–701. [Google Scholar] [CrossRef]
- Wennström, J.; Zurdo, J.; Karlsson, S.; Ekestubbe, A.; Gröndahl, K.; Lindhe, J. Bone level change at implant-supported fixed partial dentures with and without cantilever extension after 5 years in function. J. Clin. Periodontol. 2004, 31, 1077–1083. [Google Scholar] [CrossRef]
- Hälg, G.A.; Schmid, J.; Hämmerle, C.H. Bone level changes at implants supporting crowns or fixed partial dentures with or without cantilevers. Clin. Oral Implants Res. 2008, 19, 983–990. [Google Scholar] [CrossRef]
- Zurdo, J.; Romão, C.; Wennström, J.L. Survival and complication rates of implant-supported fixed partial dentures with cantilevers: A systematic review. Clin. Oral Implants Res. 2009, 20 (Suppl. 4), 59–66. [Google Scholar] [CrossRef]
- Maló, P.; de Araujo Nobre, M.; Lopes, A. The prognosis of partial implant-supported fixed dental prostheses with cantilevers. A 5-year retrospective cohort study. Eur. J. Oral Implantol. 2013, 6, 51–59. [Google Scholar]
- Aglietta, M.; Siciliano, V.I.; Zwahlen, M.; Brägger, U.; Pjetursson, B.E.; Lang, N.P.; Salvi, G.E. A systematic review of the survival and complication rates of implant supported fixed dental prostheses with cantilever extensions after an observation period of at least 5 years. Clin. Oral Implants Res. 2009, 20, 441–451. [Google Scholar] [CrossRef]
- Chrcanovic, B.R.; Kisch, J.; Albrektsson, T.; Wennerberg, A. Factors influencing the fracture of dental implants. Clin. Implant Dent. Relat. Res. 2018, 20, 58–67. [Google Scholar] [CrossRef]
- Schwarz, F.; Derks, J.; Monje, A.; Wang, H.L. Peri-implantitis. J. Clin. Periodontol. 2018, 45 (Suppl. 20), S246–S266. [Google Scholar] [CrossRef] [Green Version]
- Ravidà, A.; Tattan, M.; Askar, H.; Barootchi, S.; Tavelli, L.; Wang, H.L. Comparison of three different types of implant-supported fixed dental prostheses: A long-term retrospective study of clinical outcomes and cost-effectiveness. Clin. Oral Implants Res. 2019, 30, 295–305. [Google Scholar] [CrossRef]
- Yi, Y.; Koo, K.T.; Schwarz, F.; Ben Amara, H.; Heo, S.J. Association of prosthetic features and peri-implantitis: A cross-sectional study. J. Clin. Periodontol. 2020, 47, 392–403. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | N | |
|---|---|---|
| Implant types | IT | 1379 |
| IU | 401 | |
| Sex | Male | 799 |
| Female | 981 | |
| Diameter | <4 mm | 98 |
| 4–5 mm | 1444 | |
| >5 mm | 239 | |
| Length | <8.5 mm | 63 |
| 8.5~10 mm | 1591 | |
| >10 mm | 126 | |
| Prosthesis type | Single | 472 |
| Consecutive | 1032 | |
| Bridge | 276 | |
| Maxilla | Anterior | 193 |
| Posterior | 738 | |
| Mandible | Anterior | 38 |
| Posterior | 793 | |
| Time of Failure | Patient | Age | Sex | Position | Implant Type | Diameter | Length | Prosthesis Type | Cause of Failure |
|---|---|---|---|---|---|---|---|---|---|
| BDP | 1 | 75 | M | I27 | IT | 4.3 | 10 | - | Graft infection |
| BDP | 2 | 59 | F | I36 | IT | 4.3 | 10 | - | Graft infection |
| BDP | 3 | 71 | M | I37 | IU | 5 | 8.5 | - | Failure of osseointegration |
| BDP | 4 | 55 | F | I22 | IT | 4.3 | 11.5 | - | Failure of osseointegration |
| BDP | 5 | 56 | M | I14 | IT | 4.3 | 13 | - | Failure of osseointegration |
| <1 year | 1 | 75 | M | I26 | IT | 4.3 | 11.5 | Consecutive | Failure of osseointegration |
| <1 year | 6 | 54 | F | I27 | IT | 4.3 | 10 | Consecutive | Failure of osseointegration |
| <1 year | 7 | 72 | F | I46 | IT | 4.3 | 8.5 | Single (most distal) | Failure of osseointegration |
| 1 year | 8 | 50 | F | I47 | IU | 4.5 | 10 | Single (most distal) | Failure of osseointegration |
| 2 years | 9 | 66 | M | I26 | IU | 4.5 | 10 | Consecutive (most distal) | Failure of osseointegration |
| 3 years | 10 | 37 | IT | 4.3 | 10 | Single (most distal) | Peri-implantitis | ||
| 5 years | 11 | 62 | M | I26 | IT | 4.3 | 10 | Consecutive | Abutment neck fracture and implant fracture |
| 5 years | 12 | 66 | M | I36 | IT | 4.3 | 10 | Consecutive (cantilever) | Remained fractured fragment, implant buried |
| 8 years | 13 | 59 | M | I46 | IT | 4.3 | 10 | Single (most distal) | Abutment screw fracture and implant fracture |
| 7 years | 14 | 69 | F | I36 | IT | 4.3 | 10 | Consecutive | Implant fracture and peri-implantitis |
| 7 years | 15 | 29 | F | I47 | IT | 4.3 | 8.5 | Single (most distal) | Abutment neck fracture and implant fracture |
| 9 years | 16 | 60 | F | 16 | IT | 4.3 | 11.5 | Consecutive | Peri-implantitis |
| 9 years | 14 | 71 | F | I45 | IT | 4.3 | 10 | FPD (mesial implant) | Implant fracture and peri-implantitis |
| 11 years | 17 | 60 | F | I16 | IT | 4.3 | 11.5 | Consecutive | Peri-implantitis |
| 14 years | 18 | 52 | F | I14 | IT | 4.3 | 10 | Consecutive | Peri-implantitis |
| Mean (Standard Deviation) of Mesial Marginal Bone Loss | Mean (Standard Deviation) of Distal Marginal Bone Loss | |||||||
|---|---|---|---|---|---|---|---|---|
| 1 Year | 2 Years | 4 Years | 6+ Years | 1 Year | 2 Years | 4 Years | 6+ Years | |
| IT | 0.06 (0.2) | 0.10 (0.27) | 0.18 (0.45) | 0.29 (0.6) | 0.08 (0.24) | 0.12 (0.30) | 0.18 (0.45) | 0.23 (0.55) |
| IU | 0.04 (0.12) | −0.07 (0.19) | 0.09 (0.20) | 0 (0.0) | 0.05 (0.15) | 0.07 (0.20) | 0.08 (0.18) | 0 (0.0) |
| p > 0.05 | ||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oh, J.-H.; Pyo, S.-W.; Chang, J.-S.; Kim, S. Up to a 15-Year Survival Rate and Marginal Bone Resorption of 1780 Implants with or without Microthreads: A Multi Center Retrospective Study. J. Clin. Med. 2023, 12, 2425. https://doi.org/10.3390/jcm12062425
Oh J-H, Pyo S-W, Chang J-S, Kim S. Up to a 15-Year Survival Rate and Marginal Bone Resorption of 1780 Implants with or without Microthreads: A Multi Center Retrospective Study. Journal of Clinical Medicine. 2023; 12(6):2425. https://doi.org/10.3390/jcm12062425
Chicago/Turabian StyleOh, Ji-Hwan, Se-Wook Pyo, Jae-Seung Chang, and Sunjai Kim. 2023. "Up to a 15-Year Survival Rate and Marginal Bone Resorption of 1780 Implants with or without Microthreads: A Multi Center Retrospective Study" Journal of Clinical Medicine 12, no. 6: 2425. https://doi.org/10.3390/jcm12062425