
Impact of Sociodemographic, Premorbid, and Injury-Related Factors on Patient-Reported Outcome Trajectories after Traumatic Brain Injury (TBI)
 , , , , , , ,
, , , , , , ,  and
and
Abstract
:1. Introduction
- Identifying classes related to trajectories of improving or decreasing patient-reported TBI-specific and generic HRQoL and psychosocial and post-concussion symptom burden from three to twelve months after a TBI.
- Examining sociodemographic, premorbid, and injury-related factors associated with these recuperation classes of PROs.
2. Materials and Methods
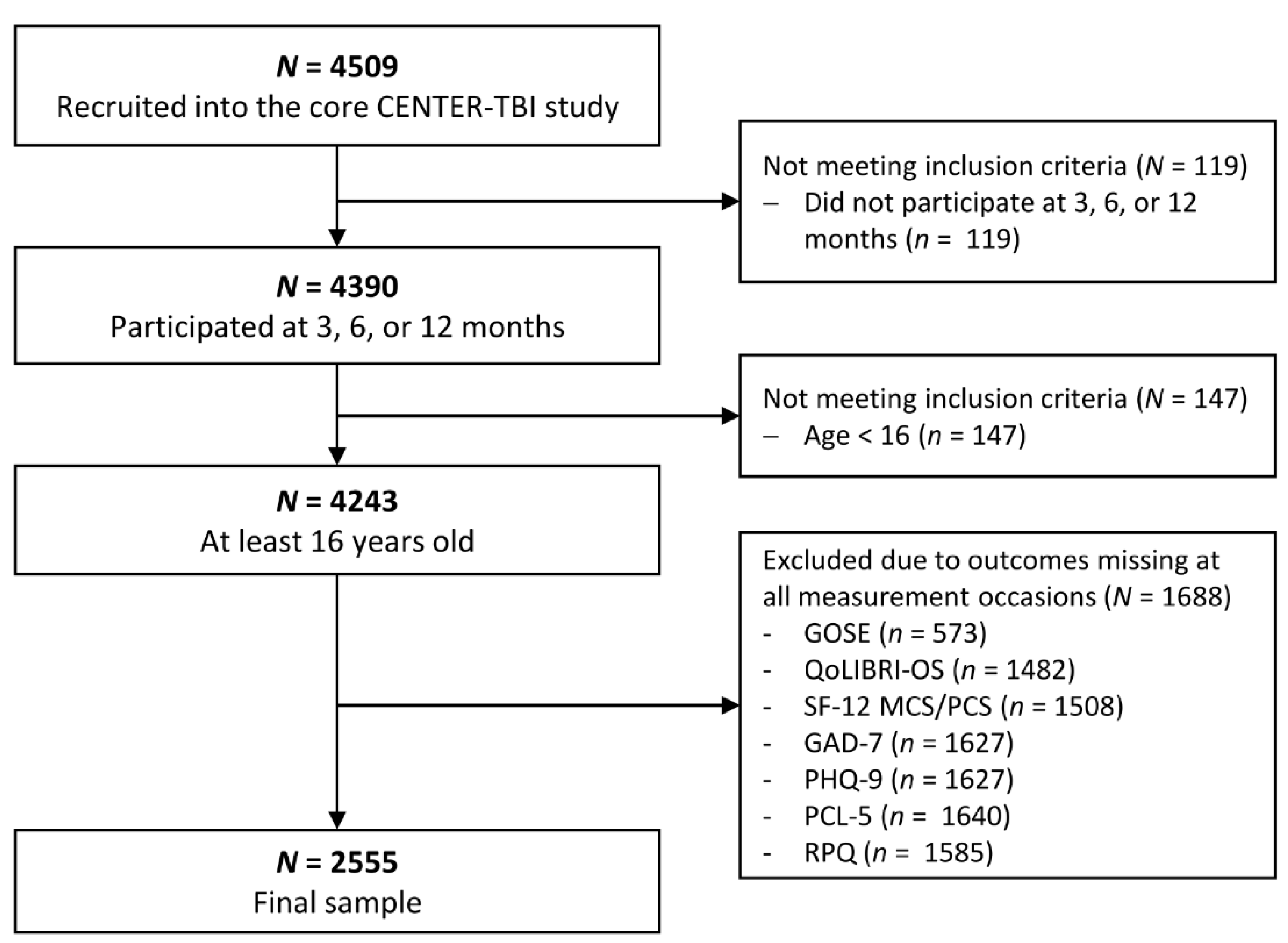
2.1. Study Sample
2.2. Ethical Approval
2.3. Sociodemographic, Premorbid and Injury-Related Characteristics
2.4. Patient-Reported Outcome Measures
2.5. Data Analyses
2.5.1. Multivariate Latent Class Mixed Models (MLCMM)
2.5.2. Multinomial Logistic Regressions (MLR)
3. Results
3.1. Sample Characteristics
3.1.1. Sociodemographic Information
3.1.2. Premorbid and Injury-Related Information
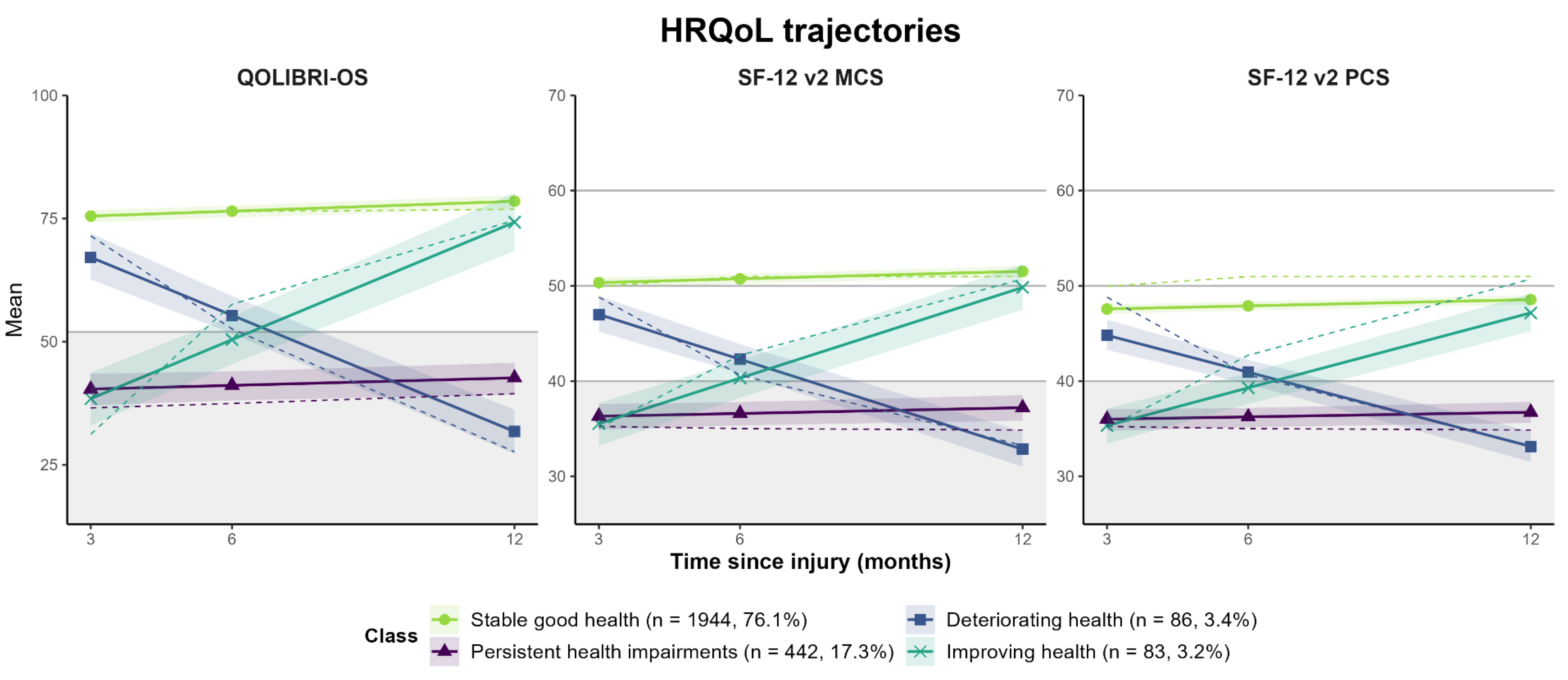
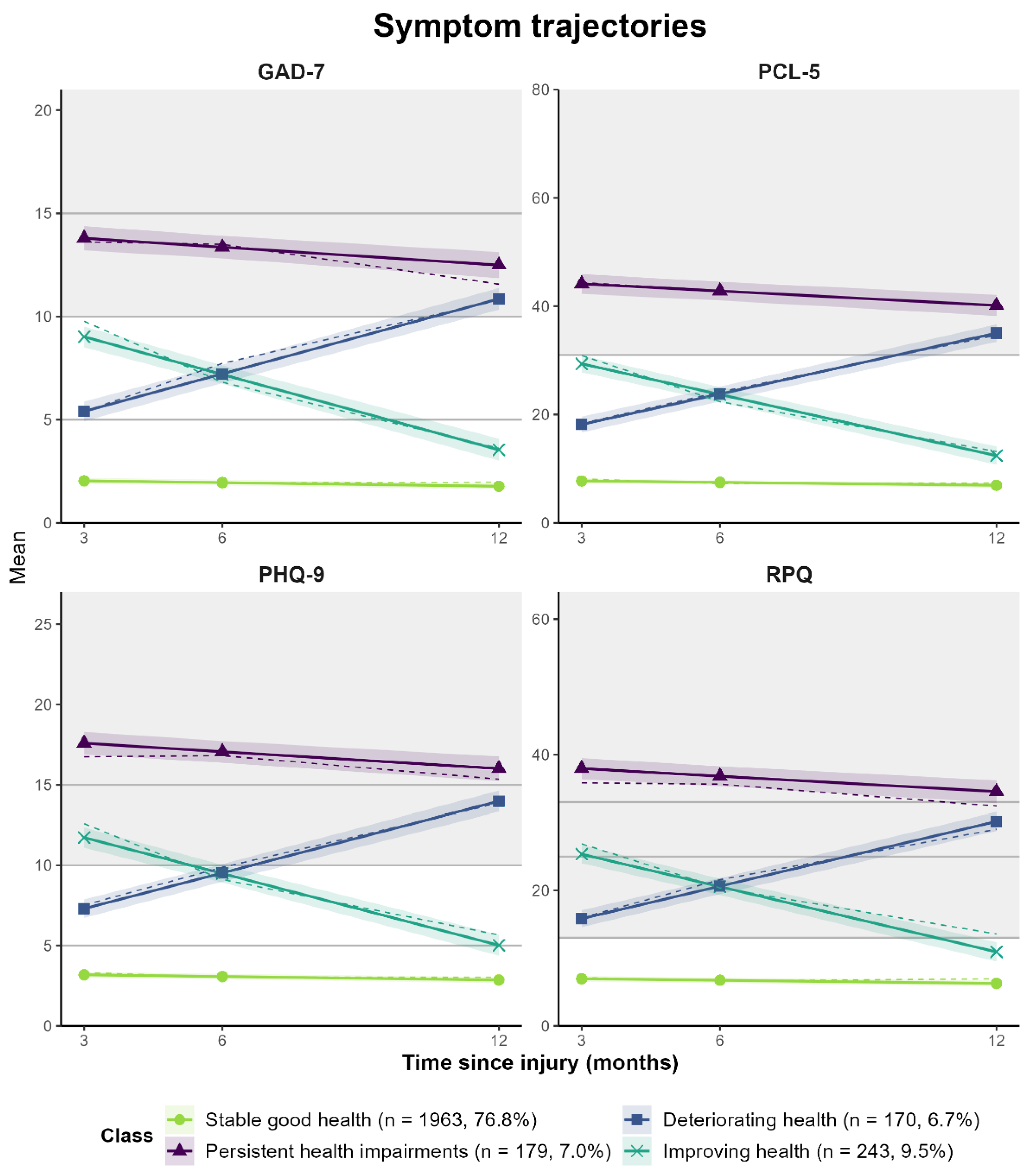
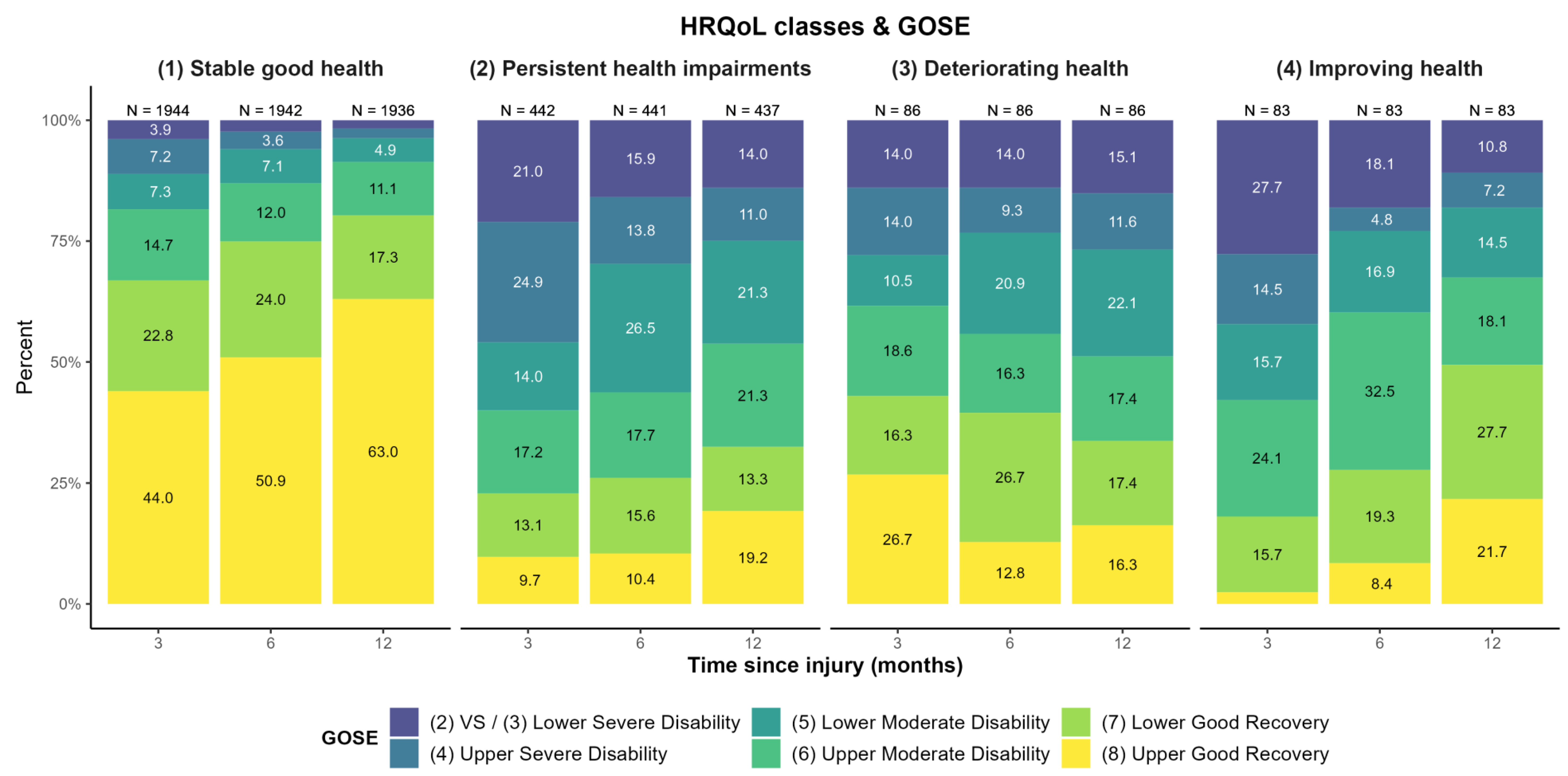
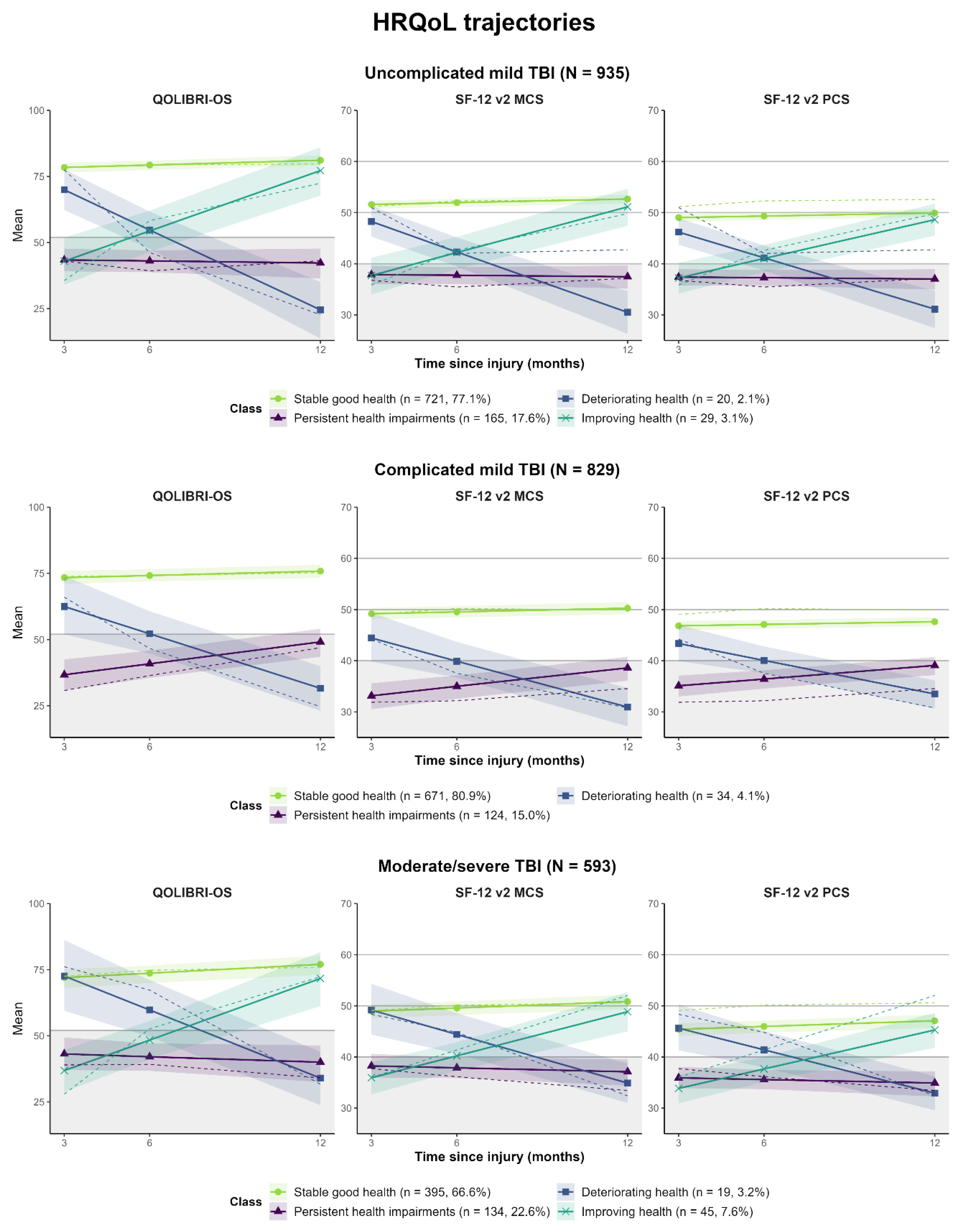
3.2. Classes of Outcome Trajectories
3.3. Association of Sociodemographic, Premorbid, and Injury-Related Factors with Trajectory Classes
3.3.1. Results of Univariate Comparisons between Trajectory Classes
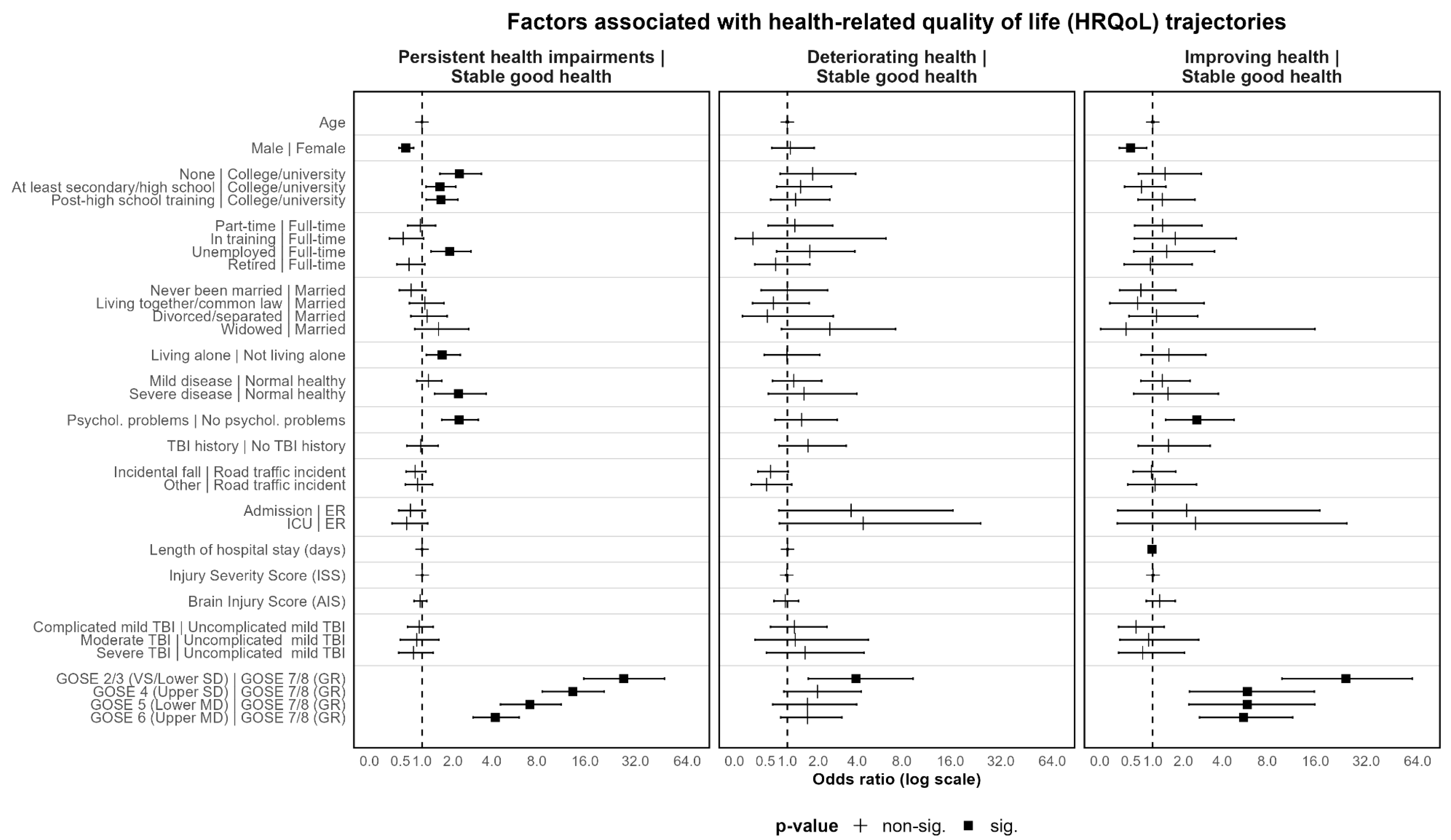
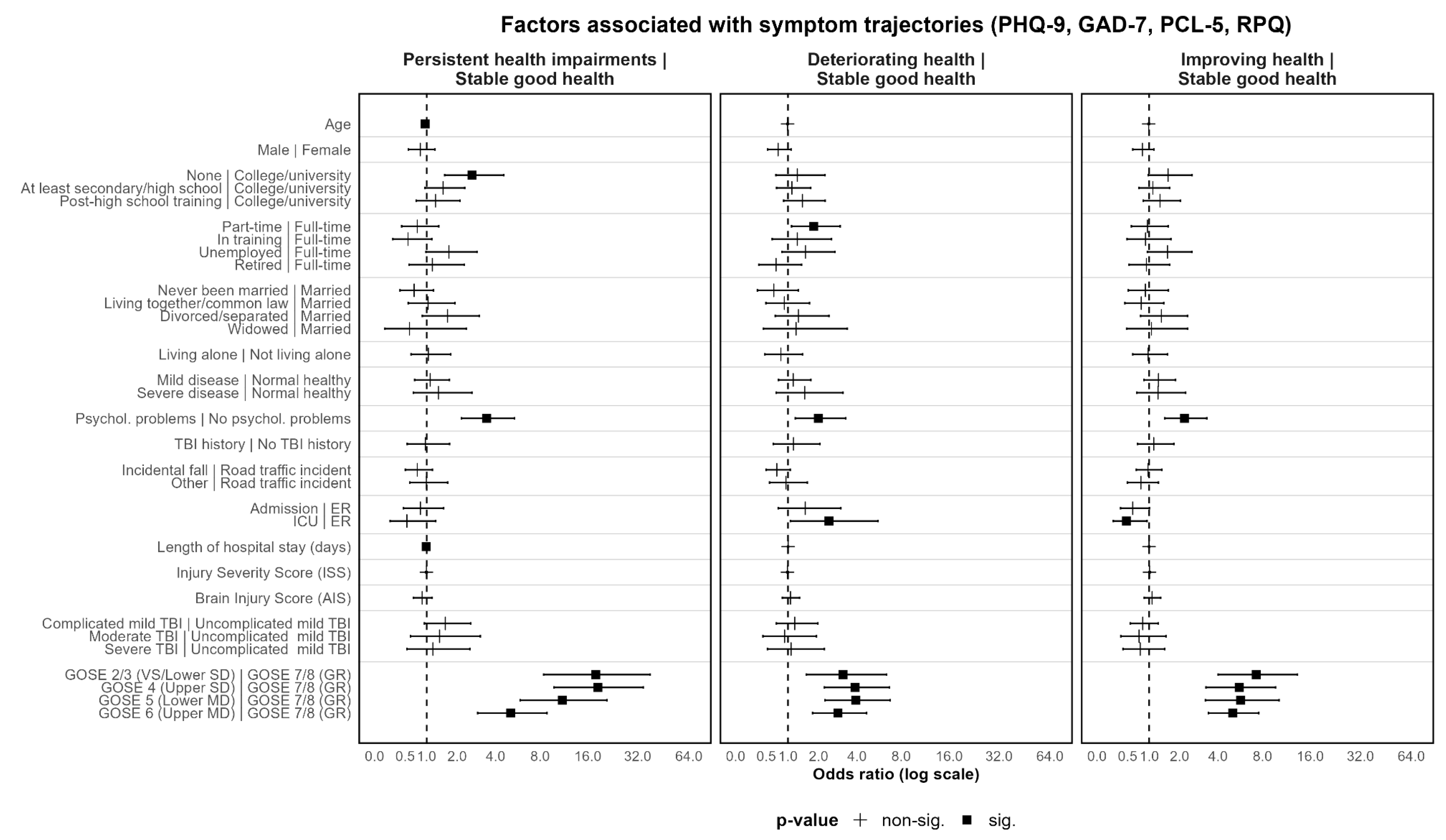
3.3.2. Results of Multinomial Logistic Regression Analyses
4. Discussion
4.1. Classes of Patient-Reported Outcome Trajectories
4.2. Unfavorable/Non-Stable Trajectory Classes, Associated Patient Characteristics, and Clinical Implications
4.2.1. Persistent Health Impairments
4.2.2. Deteriorating Health Status
4.2.3. Improving Health Status
4.3. Strengths & Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Descriptive Statistics for Included and Excluded Participants

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Included (n = 2555) | Excluded (n = 1954) | p-Value |
|---|---|---|---|
| Age (in years) | 0.428 | ||
| M (SD) | 48.86 (19.49) | 49.1 (23.4) | |
| Sex | 0.005 | ||
| Male | 1669 (65.3%) | 1354 (69.3%) | |
| Education level | <0.001 | ||
| None/primary school | 327 (14.4%) | 314 (24.3%) | |
| At least secondary/high school | 852 (37.5%) | 527 (40.8%) | |
| Post-high school training | 469 (20.6%) | 227 (17.6%) | |
| College/University | 626 (27.5%) | 224 (17.3%) | |
| Employment status | <0.001 | ||
| Full-time employed | 1072 (44.7%) | 513 (32.4%) | |
| Part-time employed | 269 (11.2%) | 122 (7.70%) | |
| In training | 241 (10.1%) | 245 (15.5%) | |
| Unemployed | 216 (9.0%) | 190 (12.0%) | |
| Retired | 598 (25.0%) | 514 (32.4%) | |
| Marital status | <0.001 | ||
| Never been married | 756 (31.3%) | 603 (36.8%) | |
| Married | 1073 (44.5%) | 663 (40.5%) | |
| Living together/common law | 221 (9.2%) | 113 (6.9%) | |
| Divorced/separated | 229 (9.5%) | 126 (7.7%) | |
| Widowed | 134 (5.6%) | 132 (8.1%) | |
| Living alone | >0.99 | ||
| Yes | 526 (20.6%) | 400 (20.6%) |
| Characteristic | Included (n = 2555) | Excluded (n = 1954) | p-Value |
|---|---|---|---|
| Physical health Status (ASA) | <0.001 | ||
| Normal healthy | 1510 (59.8%) | 991 (53.6%) | |
| Mild disease | 805 (31.9%) | 605 (32.7%) | |
| Severe disease | 209 (8.3%) | 253 (13.7%) | |
| Psychological problems | <0.001 | ||
| Yes | 304 (12.1%) | 297 (16.2%) | |
| TBI history | 0.176 | ||
| Yes | 249 (10.2%) | 153 (8.90%) | |
| Developmental problems | 0.143 | ||
| Yes | 26 (1.0%) | 29 (1.59%) | |
| Cause of injury | <0.001 | ||
| Road traffic incident | 1026 (41.0%) | 656 (34.8%) | |
| Incidental fall | 1113 (44.5%) | 911 (48.3%) | |
| Other | 363 (14.5%) | 319 (16.9%) | |
| Clinical care pathways | <0.001 | ||
| ER | 530 (20.7%) | 318 (16.3%) | |
| Admission | 974 (38.1%) | 549 (28.1%) | |
| ICU | 1051 (41.1%) | 1087 (55.6%) | |
| Length of hospital stay (days) | 0.040 | ||
| M (SD) | 11.44 (18.86) | 13.4 (23.7) | |
| Injury Severity Score (ISS) | <0.001 | ||
| M (SD) | 18.62 (14.90) | 24.1 (18.8) | |
| Brain Injury Score (AIS) | <0.001 | ||
| M (SD) | 2.99 (1.35) | 3.50 (1.51) | |
| TBI Severity Classification | <0.001 | ||
| Uncomplicated mild | 935 (39.7%) | 566 (32.1%) | |
| Complicated mild | 829 (35.2%) | 414 (23.5%) | |
| Moderate | 183 (7.8%) | 206 (11.7%) | |
| Severe | 410 (17.4%) | 576 (32.7%) | |
| GOSE | <0.001 | ||
| (1) Dead | 0 (0.00%) | 429 (34.8%) | |
| (2) VS/(3) Lower SD | 204 (7.98%) | 221 (17.9%) | |
| (4) Upper SD | 274 (10.7%) | 66 (5.4%) | |
| (5) Lower MD | 226 (8.85%) | 43 (3.5%) | |
| (6) Upper MD | 398 (15.6%) | 85 (6.9%) | |
| (7) Lower GR | 529 (20.7%) | 125 (10.1%) | |
| (8) Upper GR | 924 (36.2%) | 263 (21.3%) |
Appendix B. Multivariate Latent Class Growth Analysis Results
| Model | NC | NPM | LogLik | AIC | BIC | SABIC | Class (%) | LMR (p) | Entr. | PP Min | PP Max | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | |||||||||||
| (1) Random intercept, fixed slope | 1 | 10 | −65,860.31 | 131,740.61 | 131,799.07 | 131,767.30 | 100.0 | 1.00 | 0.00 | 0.00 | |||||
| 2 | 13 | −65,751.21 | 131,528.42 | 131,604.41 | 131,563.11 | 96.5 | 3.5 | <0.001 | 0.80 | 0.79 | 0.96 | ||||
| 3 | 16 | −65,652.25 | 131,336.51 | 131,430.04 | 131,379.20 | 76.6 | 5.6 | 17.8 | <0.001 | 0.68 | 0.74 | 0.89 | |||
| 4 | 19 | −65,600.54 | 131,239.08 | 131,350.15 | 131,289.78 | 3.2 | 3.4 | 17.3 | 76.1 | <0.001 | 0.71 | 0.70 | 0.89 | ||
| 5 | 22 | −65,652.25 | 131,348.51 | 131,477.11 | 131,407.21 | 6.5 | 0.0 | 0.0 | 71.6 | 21.9 | >0.999 | 0.37 | 0.00 | 0.72 | |
| (2) Random intercept, random slope, | 1 | 12 | −65,796.38 | 131,616.76 | 131,686.91 | 131,648.79 | 100.0 | 1.00 | 0.00 | 0.00 | |||||
| 2 | 15 | −65,693.04 | 131,416.07 | 131,503.76 | 131,456.10 | 80.2 | 19.8 | <0.001 | 0.66 | 0.81 | 0.91 | ||||
| 3 | 18 | −65,641.63 | 131,319.26 | 131,424.48 | 131,367.29 | 19.6 | 76.5 | 3.9 | <0.001 | 0.70 | 0.74 | 0.91 | |||
| 4 | Model did not converge | ||||||||||||||
| (3) Random intercept, fixed slope, different variances | 1 | 10 | −65,860.31 | 131,740.61 | 131,799.07 | 131,767.30 | 100.0 | 1.00 | 0.00 | 0.00 | |||||
| 2 | 14 | −65,751.15 | 131,530.30 | 131,612.14 | 131,567.66 | 3.1 | 96.9 | <0.001 | 0.82 | 0.81 | 0.96 | ||||
| 3 | 18 | −65,627.70 | 131,291.41 | 131,396.63 | 131,339.44 | 5.0 | 54.4 | 40.5 | <0.001 | 0.53 | 0.78 | 0.79 | |||
| 4 | 22 | −65,579.01 | 131,202.02 | 131,330.62 | 131,260.72 | 3.4 | 52.7 | 41.1 | 2.8 | <0.001 | 0.57 | 0.74 | 0.79 | ||
| 5 | Model did not converge | ||||||||||||||
| (4) Random intercept, random slope, different variances | 1 | 12 | −65,796.38 | 131,616.76 | 131,686.91 | 131,648.79 | 100.0 | 1.00 | 0.00 | 0.00 | |||||
| 2 | 16 | −65,637.08 | 131,306.17 | 131,399.70 | 131,348.87 | 48.5 | 51.5 | <0.001 | 0.47 | 0.76 | 0.89 | ||||
| 3 | 20 | −65,565.36 | 131,170.72 | 131,287.64 | 131,224.10 | 38.2 | 21.3 | 40.5 | <0.001 | 0.58 | 0.69 | 0.89 | |||
| 4 | Model did not converge | ||||||||||||||
| Model | NC | NPM | LogLik | AIC | BIC | SABIC | Class (%) | LMR (p) | Entr. | PP Min | PP Max | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | |||||||||||
| (1) Random intercept, fixed slope | 1 | 13 | −68,155.52 | 136,337.04 | 136,413.04 | 136,371.73 | 100.0 | 1.00 | 0.00 | 0.00 | |||||
| 2 | 16 | −67,662.29 | 135,356.59 | 135,450.12 | 135,399.29 | 90.9 | 9.1 | <0.001 | 0.85 | 0.86 | 0.96 | ||||
| 3 | 19 | −67,196.45 | 134,430.89 | 134,541.96 | 134,481.60 | 7.8 | 11.6 | 80.6 | <0.001 | 0.85 | 0.83 | 0.95 | |||
| 4 | 22 | −67,009.75 | 134,063.50 | 134,192.11 | 134,122.21 | 9.5 | 7.0 | 76.8 | 6.7 | <0.001 | 0.85 | 0.74 | 0.94 | ||
| 5 | 25 | −67,009.75 | 134,069.50 | 134,215.64 | 134,136.21 | 9.6 | 76.7 | 6.7 | 7.0 | 0.0 | >0.999 | 0.78 | 0.00 | 0.90 | |
| (2) Random intercept, random slope | 1 | 15 | −67,671.29 | 135,372.58 | 135,460.26 | 135,412.60 | 100.0 | 1.00 | 0.00 | 0.00 | |||||
| 2 | 18 | −67,290.22 | 134,616.44 | 134,721.67 | 134,664.48 | 84.9 | 15.1 | <0.001 | 0.88 | 0.89 | 0.97 | ||||
| 3 | 21 | −67,290.22 | 134,622.44 | 134,745.20 | 134,678.48 | 15.7 | 84.3 | 0.0 | >0.999 | 0.46 | 0.00 | 0.88 | |||
| (3) Random intercept, fixed slope, different variances | 1 | 13 | −68,155.52 | 136,337.04 | 136,413.04 | 136,371.73 | 100.0 | 1.00 | 0.00 | 0.00 | |||||
| 2 | 17 | −67,596.70 | 135,227.40 | 135,326.78 | 135,272.76 | 11.3 | 88.7 | <0.001 | 0.79 | 0.87 | 0.95 | ||||
| 3 | 21 | −66,944.93 | 133,931.86 | 134,054.62 | 133,987.90 | 10.9 | 65.5 | 23.6 | <0.001 | 0.71 | 0.82 | 0.90 | |||
| 4 | 25 | −66,730.05 | 133,510.09 | 133,656.24 | 133,576.81 | 33.3 | 42.9 | 8.7 | 15.1 | <0.001 | 0.64 | 0.76 | 0.85 | ||
| 5 | 29 | −66,639.54 | 133,337.08 | 133,506.61 | 133,414.47 | 8.9 | 33.0 | 5.1 | 41.6 | 11.3 | <0.001 | 0.66 | 0.72 | 0.84 | |
| 6 | Model did not converge | ||||||||||||||
| (4) Random intercept, random slope, different variances | 1 | 15 | −67,671.29 | 135,372.58 | 135,460.26 | 135,412.60 | 100.0 | 1.00 | 0.00 | 0.00 | |||||
| 2 | 19 | −66,770.92 | 133,579.84 | 133,690.91 | 133,630.54 | 55.6 | 44.4 | <0.001 | 0.67 | 0.88 | 0.94 | ||||
| 3 | 23 | −66,520.72 | 133,087.44 | 133,221.90 | 133,148.82 | 33.6 | 42.8 | 23.6 | <0.001 | 0.66 | 0.78 | 0.91 | |||
| 4 | Model did not converge | ||||||||||||||
Appendix C. Robustness Checks: Analyses of Trajectory Classes for Subgroups with Different TBI Severity ((1) Uncomplicated Mild, (2) Complicated Mild and (3) Moderate/Severe)
| Model | NC | NPM | LogLik | AIC | BIC | SABIC | Class (%) | LMR (p) | Entr. | PP Min | PP Max | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | |||||||||||
| (1) Random intercept, fixed slope | 1 | 10 | −21,946.06 | 43,912.13 | 43,960.53 | 43,928.77 | 100.0 | 1.00 | 0.00 | 0.00 | |||||
| 2 | 13 | −21,902.23 | 43,830.45 | 43,893.38 | 43,852.09 | 92.1 | 7.9 | <0.001 | 0.76 | 0.77 | 0.95 | ||||
| 3 | 16 | −21,864.55 | 43,761.10 | 43,838.55 | 43,787.74 | 3.0 | 75.4 | 21.6 | <0.001 | 0.72 | 0.77 | 0.92 | |||
| 4 | 19 | −21,839.53 | 43,717.05 | 43,809.02 | 43,748.68 | 17.6 | 77.1 | 2.1 | 3.1 | <0.001 | 0.74 | 0.71 | 0.91 | ||
| 5 | 22 | −21,839.53 | 43,723.05 | 43,829.54 | 43,759.67 | 19.0 | 2.2 | 75.4 | 3.3 | 0.0 | >0.999 | 0.60 | 0.69 | 0.82 | |
| (2) Random intercept, random slope, | 1 | 12 | −21,920.71 | 43,865.41 | 43,923.50 | 43,885.39 | 100.0 | 1.00 | 0.00 | 0.00 | |||||
| 2 | 15 | −21,874.30 | 43,778.59 | 43,851.20 | 43,803.56 | 80.3 | 19.7 | <0.001 | 0.70 | 0.83 | 0.94 | ||||
| 3 | 18 | −21,855.03 | 43,746.06 | 43,833.19 | 43,776.02 | 2.0 | 19.1 | 78.8 | <0.001 | 0.75 | 0.79 | 0.93 | |||
| 4 | 21 | −21,855.03 | 43,752.06 | 43,853.71 | 43,787.02 | 2.2 | 75.8 | 0.0 | 21.9 | >0.999 | 0.43 | 0.53 | 0.75 | ||
| (3) Random intercept, fixed slope, different variances | 1 | 10 | −21,946.06 | 43,912.13 | 43,960.53 | 43,928.77 | 100.0 | 1.00 | 0.00 | 0.00 | |||||
| 2 | 14 | −21,900.68 | 43,829.37 | 43,897.14 | 43,852.67 | 92.5 | 7.5 | <0.001 | 0.72 | 0.77 | 0.94 | ||||
| 3 | 18 | −21,849.90 | 43,735.81 | 43,822.94 | 43,765.77 | 3.2 | 57.1 | 39.7 | <0.001 | 0.55 | 0.79 | 0.82 | |||
| 4 | 22 | −21,829.14 | 43,702.28 | 43,808.78 | 43,738.91 | 33.4 | 2.4 | 61.2 | 3.1 | <0.001 | 0.60 | 0.71 | 0.82 | ||
| 5 | 26 | −21,808.49 | 43,668.98 | 43,794.84 | 43,712.26 | 43.1 | 2.5 | 22.7 | 3.0 | 28.8 | <0.001 | 0.60 | 0.70 | 0.81 | |
| 6 | Model did not converge | ||||||||||||||
| (4) Random intercept, random slope, different variances | 1 | 12 | −21,920.71 | 43,865.41 | 43,923.50 | 43,885.39 | 100.0 | 1.00 | 0.00 | 0.00 | |||||
| 2 | 16 | −21,848.86 | 43,729.72 | 43,807.17 | 43,756.36 | 44.2 | 55.8 | <0.001 | 0.47 | 0.79 | 0.90 | ||||
| 3 | 20 | −21,813.66 | 43,667.32 | 43,764.13 | 43,700.61 | 36.9 | 25.3 | 37.8 | <0.001 | 0.61 | 0.72 | 0.90 | |||
| 4 | 24 | −21,799.13 | 43,646.27 | 43,762.44 | 43,686.22 | 37.2 | 25.0 | 11.2 | 26.5 | <0.001 | 0.61 | 0.68 | 0.88 | ||
| 5 | Model did not converge | ||||||||||||||
| Model | NC | NPM | LogLik | AIC | BIC | SABIC | Class (%) | LMR (p) | Entr. | PP Min | PP Max | |||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | |||||||||||
| (1) Random intercept, fixed slope | 1 | 10 | −22,678.04 | 45,376.09 | 45,423.29 | 45,391.53 | 100.0 | 1.00 | 0.00 | 0.00 | ||||
| 2 | 13 | −22,650.23 | 45,326.47 | 45,387.83 | 45,346.55 | 97.0 | 3.0 | <0.001 | 0.87 | 0.79 | 0.98 | |||
| 3 | 16 | −22,617.02 | 45,266.04 | 45,341.56 | 45,290.75 | 80.9 | 4.1 | 15.0 | <0.001 | 0.73 | 0.77 | 0.91 | ||
| 4 | 19 | −22,617.02 | 45,272.04 | 45,361.72 | 45,301.38 | 0.0 | 80.1 | 4.1 | 15.8 | >0.999 | 0.54 | 0.75 | 0.77 | |
| (2) Random intercept, random slope, | 1 | 12 | −22,671.25 | 45,366.50 | 45,423.14 | 45,385.03 | 100.0 | 1.00 | 0.00 | 0.00 | ||||
| 2 | 15 | −22,638.70 | 45,307.41 | 45,378.21 | 45,330.58 | 84.4 | 15.6 | <0.001 | 0.68 | 0.83 | 0.92 | |||
| 3 | 18 | −22,616.95 | 45,269.89 | 45,354.86 | 45,297.69 | 15.1 | 4.2 | 80.7 | <0.001 | 0.73 | 0.76 | 0.91 | ||
| 4 | 21 | −22,616.95 | 45,275.89 | 45,375.02 | 45,308.33 | 18.5 | 0.0 | 76.7 | 4.8 | >0.999 | 0.40 | 0.50 | 0.73 | |
| (3) Random intercept, fixed slope, different variances | 1 | 10 | −22,678.04 | 45,376.09 | 45,423.29 | 45,391.53 | 100.0 | 1.00 | 0.00 | 0.00 | ||||
| 2 | 14 | −22,649.69 | 45,327.37 | 45,393.46 | 45,349.00 | 49.5 | 50.5 | <0.001 | 0.38 | 0.75 | 0.84 | |||
| 3 | 18 | −22,613.70 | 45,263.40 | 45,348.37 | 45,291.21 | 4.7 | 66.9 | 28.3 | <0.001 | 0.59 | 0.76 | 0.84 | ||
| 4 | Model did not converge | |||||||||||||
| (4) Random intercept, random slope, different variances | 1 | 12 | −22,671.25 | 45,366.50 | 45,423.14 | 45,385.03 | 100.0 | 1.00 | 0.00 | 0.00 | ||||
| 2 | 16 | −22,630.12 | 45,292.25 | 45,367.77 | 45,316.96 | 48.9 | 51.1 | <0.001 | 0.42 | 0.77 | 0.86 | |||
| 3 | 20 | −22,612.43 | 45,264.85 | 45,359.26 | 45,295.75 | 3.6 | 59.1 | 37.3 | <0.001 | 0.54 | 0.76 | 0.80 | ||
| 4 | 24 | −22,600.68 | 45,249.35 | 45,362.64 | 45,286.42 | 49.3 | 16.4 | 3.0 | 31.2 | <0.001 | 0.57 | 0.72 | 0.81 | |
| 5 | Model did not converge | |||||||||||||
| Model | NC | NPM | LogLik | AIC | BIC | SABIC | Class (%) | LMR (p) | Entr. | PP Min | PP Max | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | |||||||||||
| (1) Random intercept, fixed slope | 1 | 10 | −16,150.86 | 32,321.72 | 32,365.58 | 32,333.83 | 100.0 | 1.00 | 0.00 | 0.00 | |||||
| 2 | 13 | −16,124.21 | 32,274.42 | 32,331.43 | 32,290.16 | 6.4 | 93.6 | <0.001 | 0.69 | 0.78 | 0.93 | ||||
| 3 | 16 | −16,110.17 | 32,252.35 | 32,322.51 | 32,271.72 | 7.8 | 86.5 | 5.7 | <0.001 | 0.68 | 0.72 | 0.88 | |||
| 4 | 19 | −16,097.75 | 32,233.50 | 32,316.82 | 32,256.50 | 22.6 | 66.6 | 7.6 | 3.2 | <0.001 | 0.63 | 0.69 | 0.85 | ||
| 5 | 22 | −16,097.75 | 32,239.50 | 32,335.97 | 32,266.13 | 28.7 | 3.9 | 58.5 | 0.0 | 8.9 | >0.999 | 0.42 | 0.48 | 0.65 | |
| (2) Random intercept, random slope, | 1 | 12 | −16,129.65 | 32,283.30 | 32,335.93 | 32,297.83 | 100.0 | 1.00 | 0.00 | 0.00 | |||||
| 2 | 15 | −16,112.44 | 32,254.89 | 32,320.66 | 32,273.04 | 79.3 | 20.7 | <0.001 | 0.59 | 0.81 | 0.89 | ||||
| 3 | 18 | −16,101.96 | 32,239.93 | 32,318.86 | 32,261.72 | 39.3 | 53.0 | 7.8 | <0.001 | 0.63 | 0.76 | 0.87 | |||
| 4 | 21 | −16,101.96 | 32,245.93 | 32,338.02 | 32,271.35 | 44.5 | 0.0 | 7.8 | 47.7 | >0.999 | 0.45 | 0.52 | 0.87 | ||
| (3) Random intercept, fixed slope, different variances | 1 | 10 | −16,150.86 | 32,321.72 | 32,365.58 | 32,333.83 | 100.0 | 1.00 | 0.00 | 0.00 | |||||
| 2 | 14 | −16,123.77 | 32,275.54 | 32,336.94 | 32,292.49 | 6.2 | 93.8 | <0.001 | 0.72 | 0.77 | 0.94 | ||||
| 3 | 18 | −16,107.20 | 32,250.40 | 32,329.33 | 32,272.19 | 14.8 | 48.2 | 36.9 | <0.001 | 0.45 | 0.72 | 0.77 | |||
| 4 | 22 | −16,095.27 | 32,234.55 | 32,331.02 | 32,261.18 | 48.9 | 41.1 | 3.9 | 6.1 | <0.001 | 0.54 | 0.72 | 0.76 | ||
| 5 | Model did not converge | ||||||||||||||
| (4) Random intercept, random slope, different variances | 1 | 12 | −16,129.65 | 32,283.30 | 32,335.93 | 32,297.83 | 100.0 | 1.00 | 0.00 | 0.00 | |||||
| 2 | 16 | −16,105.28 | 32,242.57 | 32,312.73 | 32,261.94 | 71.2 | 28.8 | <0.001 | 0.57 | 0.73 | 0.91 | ||||
| 3 | 20 | −16,090.06 | 32,220.12 | 32,307.82 | 32,244.33 | 34.4 | 18.4 | 47.2 | <0.001 | 0.57 | 0.66 | 0.89 | |||
| 4 | 24 | −16,086.19 | 32,220.38 | 32,325.63 | 32,249.44 | 35.9 | 37.4 | 18.7 | 7.9 | 0.118 | 0.68 | 0.78 | 0.84 | ||
| Model | NC | NPM | LogLik | AIC | BIC | SABIC | Class (%) | LMR (p) | Entr. | PP Min | PP Max | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | |||||||||||
| (1) Random intercept, fixed slope | 1 | 13 | −22,525.18 | 45,076.37 | 45,139.30 | 45,098.01 | 100.0 | 1.00 | 0.00 | 0.00 | ||||||
| 2 | 16 | −22,367.14 | 44,766.28 | 44,843.73 | 44,792.91 | 90.7 | 9.3 | <0.001 | 0.90 | 0.87 | 0.98 | |||||
| 3 | 19 | −22,215.31 | 44,468.61 | 44,560.58 | 44,500.24 | 5.1 | 83.6 | 11.2 | <0.001 | 0.88 | 0.83 | 0.97 | ||||
| 4 | 22 | −22,152.65 | 44,349.30 | 44,455.79 | 44,385.92 | 16.1 | 4.5 | 4.9 | 74.4 | <0.001 | 0.87 | 0.80 | 0.96 | |||
| 5 | 25 | −22,152.65 | 44,355.30 | 44,476.31 | 44,396.92 | 16.1 | 4.9 | 0.0 | 74.4 | 4.5 | >0.999 | 0.84 | 0.80 | 0.94 | ||
| (2) Random intercept, random slope, | 1 | 15 | −22,416.08 | 44,862.16 | 44,934.76 | 44,887.13 | 100.0 | 1.00 | 0.00 | 0.00 | ||||||
| 2 | 18 | −22,265.59 | 44,567.18 | 44,654.31 | 44,597.14 | 87.8 | 12.2 | <0.001 | 0.89 | 0.91 | 0.98 | |||||
| 3 | 21 | −22,191.35 | 44,424.71 | 44,526.36 | 44,459.67 | 18.7 | 3.2 | 78.1 | <0.001 | 0.92 | 0.91 | 0.98 | ||||
| 4 | 24 | −22,265.59 | 44,579.18 | 44,695.36 | 44,619.13 | 0.0 | 0.0 | 85.8 | 14.2 | >0.999 | 0.32 | 0.46 | 0.83 | |||
| (3) Random intercept, fixed slope, different variances | 1 | 13 | −22,525.18 | 45,076.37 | 45,139.30 | 45,098.01 | 100.0 | 1.00 | 0.00 | 0.00 | ||||||
| 2 | 17 | −22,239.49 | 44,512.98 | 44,595.27 | 44,541.28 | 56.9 | 43.1 | <0.001 | 0.65 | 0.87 | 0.96 | |||||
| 3 | 21 | −22,071.70 | 44,185.41 | 44,287.06 | 44,220.36 | 56.1 | 7.6 | 36.3 | <0.001 | 0.72 | 0.85 | 0.90 | ||||
| 4 | 25 | −21,999.57 | 44,049.13 | 44,170.15 | 44,090.75 | 33.6 | 7.0 | 50.5 | 9.0 | <0.001 | 0.69 | 0.76 | 0.87 | |||
| 5 | 29 | −21,960.61 | 43,979.23 | 44,119.60 | 44,027.50 | 17.5 | 23.2 | 7.5 | 48.8 | 3.0 | <0.001 | 0.68 | 0.69 | 0.88 | ||
| 6 | 33 | −21,933.83 | 43,933.67 | 44,093.41 | 43,988.60 | 24.9 | 7.1 | 14.8 | 49.0 | 1.6 | 2.7 | <0.001 | 0.71 | 0.70 | 0.90 | |
| (4) Random intercept, random slope, different variances | 1 | 15 | −22,416.08 | 44,862.16 | 44,934.76 | 44,887.13 | 100.0 | 1.00 | 0.00 | 0.00 | ||||||
| 2 | 19 | −22,017.10 | 44,072.20 | 44,164.17 | 44,103.83 | 54.5 | 45.5 | <0.001 | 0.72 | 0.91 | 0.95 | |||||
| 3 | 23 | −21,928.60 | 43,903.21 | 44,014.54 | 43,941.50 | 49.6 | 23.3 | 27.1 | <0.001 | 0.71 | 0.77 | 0.93 | ||||
| 4 | Model did not converge | |||||||||||||||
| Model | NC | NPM | LogLik | AIC | BIC | SABIC | Class (%) | LMR (p) | Entr. | PP Min | PP Max | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | |||||||||||
| (1) Random intercept, fixed slope | 1 | 13 | −23,554.78 | 47,135.57 | 47,196.93 | 47,155.65 | 100.0 | 1.00 | 0.00 | 0.00 | ||||||
| 2 | 16 | −23,411.19 | 46,854.39 | 46,929.91 | 46,879.10 | 8.9 | 91.1 | <0.001 | 0.88 | 0.89 | 0.97 | |||||
| 3 | 19 | −23,251.66 | 46,541.32 | 46,631.00 | 46,570.67 | 79.7 | 12.2 | 8.1 | <0.001 | 0.87 | 0.85 | 0.97 | ||||
| 4 | 22 | −23,197.04 | 46,438.09 | 46,541.93 | 46,472.07 | 6.5 | 9.8 | 7.7 | 76.0 | <0.001 | 0.86 | 0.78 | 0.96 | |||
| 5 | 25 | −23,197.04 | 46,444.09 | 46,562.09 | 46,482.70 | 6.9 | 7.7 | 75.2 | 10.3 | 0.0 | >0.999 | 0.58 | 0.62 | 0.87 | ||
| (2) Random intercept, random slope | 1 | 15 | −23,428.64 | 46,887.29 | 46,958.09 | 46,910.46 | 100.0 | 1.00 | 0.00 | 0.00 | ||||||
| 2 | 18 | −23,296.27 | 46,628.55 | 46,713.51 | 46,656.35 | 83.0 | 17.0 | <0.001 | 0.88 | 0.91 | 0.98 | |||||
| 3 | 21 | −23,296.27 | 46,634.55 | 46,733.67 | 46,666.98 | 0.0 | 83.0 | 17.0 | >0.999 | 0.89 | 0.91 | 0.97 | ||||
| (3) Random intercept, fixed slope, different variances | 1 | 13 | −23,554.78 | 47,135.57 | 47,196.93 | 47,155.65 | 100.0 | 1.00 | 0.00 | 0.00 | ||||||
| 2 | 17 | −23,368.42 | 46,770.84 | 46,851.08 | 46,797.10 | 66.0 | 34.0 | <0.001 | 0.59 | 0.87 | 0.93 | |||||
| 3 | 21 | −23,175.18 | 46,392.36 | 46,491.48 | 46,424.79 | 11.3 | 69.0 | 19.7 | <0.001 | 0.75 | 0.83 | 0.92 | ||||
| 4 | 25 | −23,109.07 | 46,268.14 | 46,386.14 | 46,306.75 | 36.2 | 14.8 | 38.0 | 11.0 | <0.001 | 0.67 | 0.78 | 0.86 | |||
| 5 | 29 | −23,089.27 | 46236.53 | 46,373.42 | 46,281.32 | 27.5 | 5.5 | 39.6 | 15.0 | 12.4 | <0.001 | 0.66 | 0.67 | 0.87 | ||
| 6 | 33 | −23,070.54 | 46,207.08 | 46,362.84 | 46,258.05 | 27.1 | 4.7 | 14.1 | 3.3 | 39.8 | 11.0 | <0.001 | 0.68 | 0.66 | 0.88 | |
| (4) Random intercept, random slope, different variances | 1 | 15 | −23,428.64 | 46,887.29 | 46,958.09 | 46,910.46 | 100.0 | 1.00 | 0.00 | 0.00 | ||||||
| 2 | 19 | −23,144.47 | 46,326.94 | 46,416.62 | 46,356.29 | 61.5 | 38.5 | <0.001 | 0.65 | 0.89 | 0.93 | |||||
| 3 | Model did not converge | |||||||||||||||
| Model | NC | NPM | LogLik | AIC | BIC | SABIC | Class (%) | LMR (p) | Entr. | PP Min | PP Max | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | |||||||||||
| (1) Random intercept, fixed slope | 1 | 13 | −16,786.95 | 33,599.90 | 33,656.90 | 33,615.63 | 100.0 | 1.00 | 0.00 | 0.00 | ||||||
| 2 | 16 | −16,623.86 | 33,279.72 | 33,349.89 | 33,299.09 | 86.7 | 13.3 | <0.001 | 0.74 | 0.87 | 0.94 | |||||
| 3 | 19 | −16,514.80 | 33,067.60 | 33,150.92 | 33,090.60 | 12.1 | 75.0 | 12.8 | <0.001 | 0.79 | 0.83 | 0.93 | ||||
| 4 | 22 | −16,473.81 | 32,991.63 | 33,088.10 | 33,018.26 | 11.5 | 6.2 | 72.7 | 9.6 | <0.001 | 0.80 | 0.79 | 0.92 | |||
| 5 | 25 | −16,455.19 | 32,960.38 | 33,070.01 | 32,990.65 | 14.8 | 6.7 | 62.9 | 3.4 | 12.1 | <0.001 | 0.78 | 0.78 | 0.89 | ||
| 6 | 28 | −16,455.19 | 32,966.38 | 33,089.17 | 33,000.28 | 15.9 | 0.0 | 57.3 | 16.7 | 6.7 | 3.4 | 1.000 | 0.58 | 0.47 | 0.87 | |
| (2) Random intercept, random slope | 1 | 15 | −16,599.62 | 33,229.23 | 33,295.01 | 33,247.39 | 100.0 | 1.00 | 0.00 | 0.00 | ||||||
| 2 | 18 | −16,530.04 | 33,096.07 | 33,175.01 | 33,117.86 | 15.7 | 84.3 | <0.001 | 0.85 | 0.87 | 0.97 | |||||
| 3 | 21 | −16,530.04 | 33,102.08 | 33,194.16 | 33,127.50 | 0.0 | 17.9 | 82.1 | 1.000 | 0.40 | 0.60 | 0.82 | ||||
| (3) Random intercept, fixed slope, different variances | 1 | 13 | −16,786.95 | 33,599.90 | 33,656.90 | 33,615.63 | 100.0 | 1.00 | 0.00 | 0.00 | ||||||
| 2 | 17 | −16,621.38 | 33,276.77 | 33,351.32 | 33,297.35 | 14.7 | 85.3 | <0.001 | 0.74 | 0.87 | 0.94 | |||||
| 3 | 21 | −16,469.16 | 32,980.31 | 33,072.40 | 33,005.73 | 16.4 | 63.4 | 20.2 | <0.001 | 0.72 | 0.84 | 0.89 | ||||
| 4 | 25 | −16,434.10 | 32,918.20 | 33,027.83 | 32,948.47 | 31.7 | 37.4 | 12.5 | 18.4 | <0.001 | 0.62 | 0.74 | 0.85 | |||
| 5 | 29 | −16,413.02 | 32,884.03 | 33,011.20 | 32,919.14 | 31.7 | 14.5 | 35.6 | 8.9 | 9.3 | <0.001 | 0.63 | 0.73 | 0.79 | ||
| 6 | 33 | −16,375.99 | 32,817.98 | 32,962.69 | 32,857.92 | 21.6 | 37.1 | 6.9 | 15.3 | 1.9 | 17.2 | <0.001 | 0.66 | 0.62 | 0.89 | |
| (4) Random intercept, random slope, different variances | 1 | 15 | −16,599.62 | 33,229.23 | 33,295.01 | 33,247.39 | 100.0 | 1.00 | 0.00 | 0.00 | ||||||
| 2 | 19 | −16,430.22 | 32,898.45 | 32,981.77 | 32,921.45 | 48.9 | 51.1 | <0.001 | 0.65 | 0.86 | 0.95 | |||||
| 3 | 23 | −16,375.14 | 32,796.27 | 32,897.13 | 32,824.11 | 25.5 | 36.1 | 38.4 | <0.001 | 0.64 | 0.79 | 0.91 | ||||
| 4 | 27 | −16,357.49 | 32,768.98 | 32,887.38 | 32,801.67 | 39.0 | 1.0 | 36.1 | 23.9 | <0.001 | 0.73 | 0.81 | 0.92 | |||
| 5 | 31 | −16,353.25 | 32,768.51 | 32,904.45 | 32,806.03 | 35.6 | 3.2 | 1.0 | 36.4 | 23.8 | 0.090 | 0.72 | 0.61 | 0.93 | ||


Appendix D. Association of HRQoL and Symptom Classes

Appendix E. Comparison of Trajectory Classes
| Characteristic | (A) Stable Good Health Status (n = 1944) 1 | (B) Persistent Health Impairments (n = 442) 1 | (C) Deteriorating Health Status (n = 86) 1 | (D) Improving Health Status (n = 83) 1 | p-Value 2 |
|---|---|---|---|---|---|
| Age (in years) | ns | ns | ns | ns | 0.069 |
| M (SD) | 48.24 (19.70) | 51.19 (18.44) | 49.40 (19.76) | 50.41 (19.07) | |
| Sex | B | A | ns | ns | <0.001 |
| Male | 1318 (67.8%) | 246 (55.7%) | 60 (69.8%) | 45 (54.2%) | |
| Education level | B | A | ns | ns | <0.001 |
| None/primary school | 211 (12.2%) | 88 (22.3%) | 14 (18.2%) | 14 (18.7%) | |
| At least secondary/high school | 649 (37.6%) | 151 (38.3%) | 31 (40.3%) | 21 (28.0%) | |
| Post-high school training | 353 (20.4%) | 81 (20.6%) | 16 (20.8%) | 19 (25.3%) | |
| College/University | 515 (29.8%) | 74 (18.8%) | 16 (20.8%) | 21 (28.0%) | |
| Employment status | B | A | ns | ns | <0.001 |
| Full-time employed | 835 (45.6%) | 170 (41.9%) | 35 (43.8%) | 32 (40.5%) | |
| Part-time employed | 201 (11.0%) | 46 (11.3%) | 11 (13.8%) | 11 (13.9%) | |
| In training | 210 (11.5%) | 19 (4.7%) | 4 (5.0%) | 8 (10.1%) | |
| Unemployed | 126 (6.9%) | 70 (17.2%) | 11 (13.8%) | 9 (11.4%) | |
| Retired | 459 (25.1%) | 101 (24.9%) | 19 (23.8%) | 19 (24.1%) | |
| Marital status | B | A | ns | ns | <0.001 |
| Never been married | 597 (32.4%) | 111 (26.9%) | 25 (31.6%) | 23 (28.7%) | |
| Married | 830 (45.1%) | 169 (41.0%) | 36 (45.6%) | 38 (47.5%) | |
| Living together/common law | 172 (9.3%) | 38 (9.2%) | 5 (6.3%) | 6 (7.5%) | |
| Divorced/separated | 159 (8.6%) | 55 (13.3%) | 5 (6.3%) | 10 (12.5%) | |
| Widowed | 84 (4.6%) | 39 (9.5%) | 8 (10.1%) | 3 (3.8%) | |
| Living alone | B | A | ns | ns | 0.015 |
| Yes | 374 (19.3%) | 115 (26.1%) | 18 (20.9%) | 19 (22.9%) |
| Characteristic | (A) Stable Good Health Status (n = 1944) 1 | (B) Persistent Health Impairments (n = 442) 1 | (C) Deteriorating Health Status (n = 86) 1 | (D) Improving Health Status (n = 83) 1 | p-Value 2 |
|---|---|---|---|---|---|
| Physical health Status (ASA) | B | A | ns | ns | <0.001 |
| Normal healthy | 1209 (62.9%) | 212 (48.6%) | 47 (56.0%) | 42 (51.2%) | |
| Mild disease | 583 (30.3%) | 161 (36.9%) | 29 (34.5%) | 32 (39.0%) | |
| Severe disease | 130 (6.8%) | 63 (14.4%) | 8 (9.5%) | 8 (9.8%) | |
| Psychological problems | B, D | A | ns | A | <0.001 |
| Yes | 171 (8.9%) | 102 (23.4%) | 12 (14.3%) | 19 (22.9%) | |
| TBI history | ns | ns | ns | ns | 0.645 |
| Yes | 188 (10.1%) | 40 (9.5%) | 11 (13.3%) | 10 (12.8%) | |
| Developmental problems | ns | ns | ns | ns | 0.413 |
| Yes | 19 (1.0%) | 5 (1.2%) | 0 (0.0%) | 2 (2.4%) | |
| Cause of injury | ns | ns | ns | ns | 0.065 |
| Road traffic incident | 747 (39.2%) | 200 (46.1%) | 43 (51.8%) | 36 (45.0%) | |
| Incidental fall | 873 (45.8%) | 175 (40.3%) | 31 (37.3%) | 34 (42.5%) | |
| Other | 285 (15.0%) | 59 (13.6%) | 9 (10.8%) | 10 (12.5%) | |
| Clinical care pathways | B, C, D | A, D | A | A, B | <0.001 |
| ER | 445 (22.9%) | 74 (16.7%) | 6 (7.0%) | 5 (6.0%) | |
| Admission | 780 (40.1%) | 138 (31.2%) | 33 (38.4%) | 23 (27.7%) | |
| ICU | 719 (37.0%) | 230 (52.0%) | 47 (54.7%) | 55 (66.3%) | |
| Length of hospital stay (days) | B, C, D | A | A | A | <0.001 |
| M (SD) | 9.74 (17.34) | 16.81 (23.06) | 16.84 (22.05) | 16.95 (17.33) | |
| Injury Severity Score (ISS) | B, C, D | A, D | A, D | A, B, C | <0.001 |
| M (SD) | 17.23 (14.00) | 22.60 (17.21) | 21.81 (15.57) | 26.77 (14.95) | |
| Brain Injury Score (AIS) | B, C, D | A, D | A, D | A, B, C | <0.001 |
| M (SD) | 2.88 (1.32) | 3.26 (1.37) | 3.34 (1.27) | 3.75 (1.33) | |
| TBI severity | B, C, D | A | A | A | <0.001 |
| Uncomplicated mild | 764 (42.7%) | 130 (31.9%) | 21 (26.6%) | 20 (25.3%) | |
| Complicated mild | 635 (35.5%) | 142 (34.8%) | 30 (38.0%) | 22 (27.8%) | |
| Moderate | 127 (7.1%) | 38 (9.3%) | 7 (8.9%) | 11 (13.9%) | |
| Severe | 265 (14.8%) | 98 (24.0%) | 21 (26.6%) | 26 (32.9%) | |
| GOSE | B, C, D | A, C, D | A, B, D | A, B, C | <0.001 |
| (2) VS/(3) Lower SD | 76 (3.9%) | 93 (21.0%) | 12 (14.0%) | 23 (27.7%) | |
| (4) Upper SD | 140 (7.2%) | 110 (24.9%) | 12 (14.0%) | 12 (14.5%) | |
| (5) Lower MD | 142 (7.3%) | 62 (14.0%) | 9 (10.5%) | 13 (15.7%) | |
| (6) Upper MD | 286 (14.7%) | 76 (17.2%) | 16 (18.6%) | 20 (24.1%) | |
| (7) Lower GR | 444 (22.8%) | 58 (13.1%) | 14 (16.3%) | 13 (15.7%) | |
| (8) Upper GR | 856 (44.0%) | 43 (9.7%) | 23 (26.7%) | 2 (2.4%) |
| Characteristic | (A) Stable Good Health Status (n = 1963) 1 | (B) Persistent Health Impairments (n = 179) 1 | (C) Deteriorating Health Status (n = 170) 1 | (D) Improving Health Status (n = 243) 1 | p-Value 2 |
|---|---|---|---|---|---|
| Age (in years) | B | A | ns | ns | <0.001 |
| M (SD) | 49.59 (19.89) | 44.20 (17.71) | 46.86 (17.62) | 47.76 (18.18) | |
| Sex | ns | ns | ns | ns | 0.139 |
| Male | 1306 (66.5%) | 109 (60.9%) | 104 (61.2%) | 150 (61.7%) | |
| Education level | B | A | ns | ns | 0.004 |
| None/primary school | 231 (13.2%) | 36 (22.6%) | 20 (13.2%) | 40 (18.2%) | |
| At least secondary/high school | 651 (37.3%) | 66 (41.5%) | 58 (38.4%) | 77 (35.0%) | |
| Post-high school training | 354 (20.3%) | 26 (16.4%) | 39 (25.8%) | 50 (22.7%) | |
| College/University | 508 (29.1%) | 31 (19.5%) | 34 (22.5%) | 53 (24.1%) | |
| Employment status | B, C, D | A | A | A | <0.001 |
| Full-time employed | 822 (44.5%) | 74 (46.0%) | 69 (44.2%) | 107 (46.3%) | |
| Part-time employed | 200 (10.8%) | 15 (9.3%) | 29 (18.6%) | 25 (10.8%) | |
| In training | 192 (10.4%) | 14 (8.7%) | 16 (10.3%) | 19 (8.2%) | |
| Unemployed | 134 (7.3%) | 31 (19.3%) | 19 (12.2%) | 32 (13.9%) | |
| Retired | 500 (27.1%) | 27 (16.8%) | 23 (14.7%) | 48 (20.8%) | |
| Marital status | ns | ns | ns | ns | 0.082 |
| Never been married | 576 (31.1%) | 59 (35.1%) | 46 (28.9%) | 75 (32.1%) | |
| Married | 846 (45.7%) | 60 (35.7%) | 69 (43.4%) | 98 (41.9%) | |
| Living together/common law | 167 (9.0%) | 18 (10.7%) | 17 (10.7%) | 19 (8.1%) | |
| Divorced/separated | 155 (8.4%) | 25 (14.9%) | 20 (12.6%) | 29 (12.4%) | |
| Widowed | 108 (5.8%) | 6 (3.6%) | 7 (4.4%) | 13 (5.6%) | |
| Living alone | ns | ns | ns | ns | 0.783 |
| Yes | 406 (20.7%) | 38 (21.3%) | 30 (17.6%) | 52 (21.4%) |
| Characteristic | (A) Stable Good Health Status (n = 1963) 1 | (B) Persistent Health Impairments (n = 179) 1 | (C) Deteriorating Health Status (n = 170) 1 | (D) Improving Health Status (n = 243) 1 | p-Value 2 |
|---|---|---|---|---|---|
| Physical health Status (ASA) | ns | ns | ns | ns | 0.482 |
| Normal healthy | 1183 (60.9%) | 101 (57.4%) | 96 (57.5%) | 130 (54.2%) | |
| Mild disease | 605 (31.2%) | 58 (33.0%) | 55 (32.9%) | 87 (36.2%) | |
| Severe disease | 153 (7.9%) | 17 (9.7%) | 16 (9.6%) | 23 (9.6%) | |
| Psychological problems | B, C, D | A | A | A | <0.001 |
| Yes | 173 (8.9%) | 48 (27.1%) | 33 (19.9%) | 50 (21.0%) | |
| TBI history | ns | ns | ns | ns | 0.895 |
| Yes | 187 (10.0%) | 19 (10.9%) | 17 (10.6%) | 26 (11.4%) | |
| Developmental problems | ns | ns | ns | ns | 0.157 |
| Yes | 20 (1.0%) | 1 (0.6%) | 0 (0.0%) | 5 (2.1%) | |
| Cause of injury | ns | ns | ns | ns | 0.001 |
| Road traffic incident | 750 (38.9%) | 85 (48.9%) | 80 (48.8%) | 111 (46.6%) | |
| Incidental fall | 898 (46.6%) | 57 (32.8%) | 59 (36.0%) | 99 (41.6%) | |
| Other | 278 (14.4%) | 32 (18.4%) | 25 (15.2%) | 28 (11.8%) | |
| Clinical care pathways | C, D | C | A, B, D | A, C | <0.001 |
| ER | 437 (22.3%) | 32 (17.9%) | 14 (8.2%) | 47 (19.3%) | |
| Admission | 785 (40.0%) | 68 (38.0%) | 47 (27.6%) | 74 (30.5%) | |
| ICU | 741 (37.7%) | 79 (44.1%) | 109 (64.1%) | 122 (50.2%) | |
| Length of hospital stay (days) | B, C, D | A, C | A, B, D | A, C | <0.001 |
| M (SD) | 10.24 (18.46) | 12.49 (16.39) | 19.10 (22.83) | 15.02 (19.10) | |
| Injury Severity Score (ISS) | C, D | C | A, B | A | <0.001 |
| M (SD) | 17.56 (14.26) | 19.86 (15.17) | 23.72 (15.70) | 22.78 (17.55) | |
| Brain Injury Score (AIS) | C, D | C | A, B | A | <0.001 |
| M (SD) | 2.89 (1.34) | 3.09 (1.32) | 3.56 (1.22) | 3.26 (1.39) | |
| TBI Severity Classification | C, D | ns | A | A | <0.001 |
| Uncomplicated mild | 763 (42.4%) | 51 (31.1%) | 38 (23.2%) | 83 (36.2%) | |
| Complicated mild | 631 (35.1%) | 65 (39.6%) | 62 (37.8%) | 71 (31.0%) | |
| Moderate | 132 (7.3%) | 16 (9.8%) | 16 (9.8%) | 19 (8.3%) | |
| Severe | 274 (15.2%) | 32 (19.5%) | 48 (29.3%) | 56 (24.5%) | |
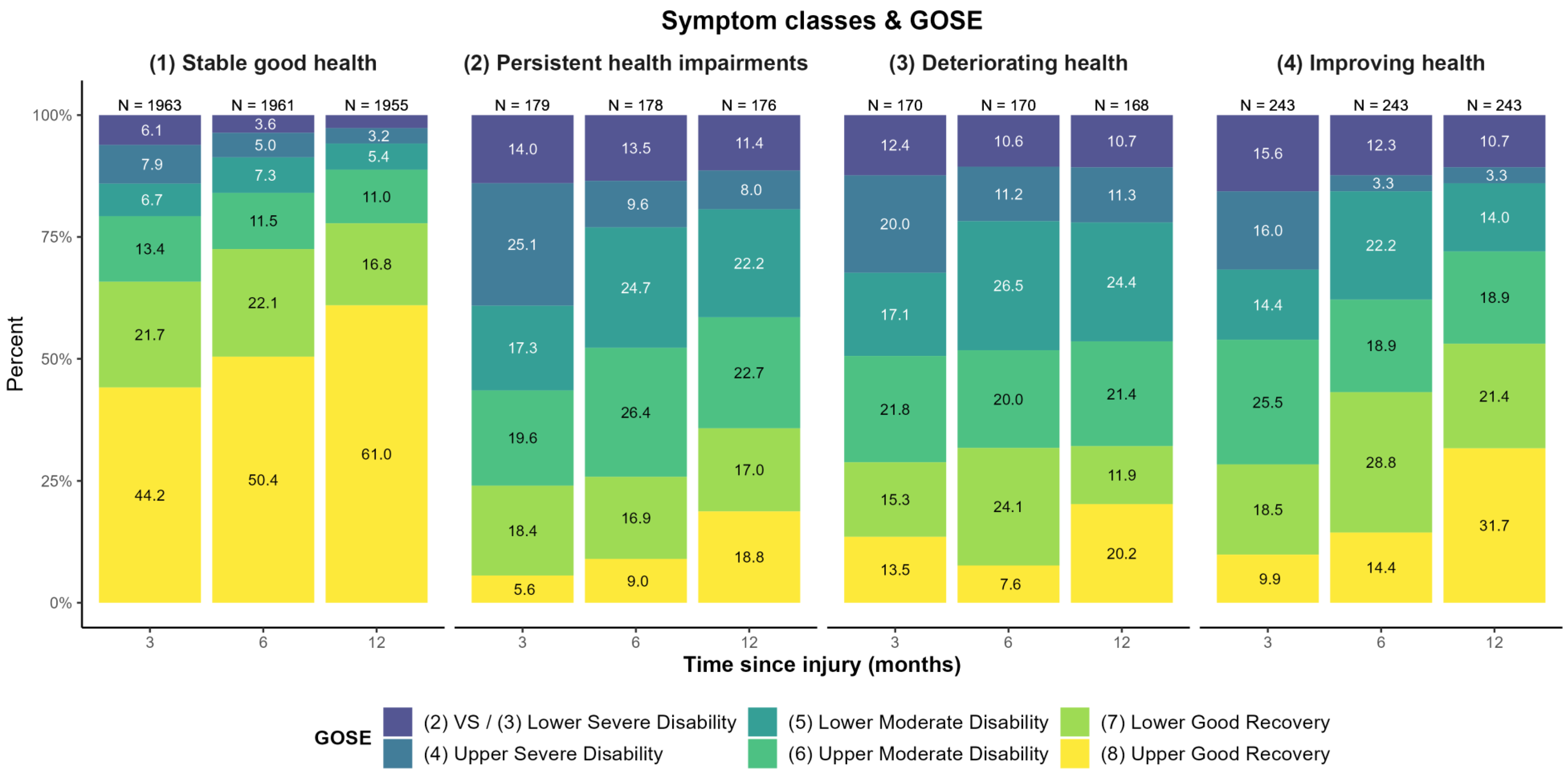
| GOSE | B, C, D | A | A | A | <0.001 |
| (2) VS/(3) Lower SD | 120 (6.1%) | 25 (14.0%) | 21 (12.4%) | 38 (15.6%) | |
| (4) Upper SD | 156 (7.9%) | 45 (25.1%) | 34 (20.0%) | 39 (16.0%) | |
| (5) Lower MD | 131 (6.7%) | 31 (17.3%) | 29 (17.1%) | 35 (14.4%) | |
| (6) Upper MD | 264 (13.4%) | 35 (19.6%) | 37 (21.8%) | 62 (25.5%) | |
| (7) Lower GR | 425 (21.7%) | 33 (18.4%) | 26 (15.3%) | 45 (18.5%) | |
| (8) Upper GR | 867 (44.2%) | 10 (5.6%) | 23 (13.5%) | 24 (9.9%) |
References
- McKinlay, A.; Grace, R.C.; Horwood, L.J.; Fergusson, D.M.; Ridder, E.M.; MacFarlane, M.R. Prevalence of Traumatic Brain Injury among Children, Adolescents and Young Adults: Prospective Evidence from a Birth Cohort. Brain Inj. 2008, 22, 175–181. [Google Scholar] [CrossRef] [PubMed]
- Hukkelhoven, C.W.P.M.; Steyerberg, E.W.; Rampen, A.J.J.; Farace, E.; Habbema, J.D.F.; Marshall, L.F.; Murray, G.D.; Maas, A.I.R. Patient Age and Outcome Following Severe Traumatic Brain Injury: An Analysis of 5600 Patients. J. Neurosurg. 2003, 99, 666–673. [Google Scholar] [CrossRef] [PubMed]
- Flaada, J.T.; Leibson, C.L.; Mandrekar, J.N.; Diehl, N.; Perkins, P.K.; Brown, A.W.; Malec, J.F. Relative Risk of Mortality after Traumatic Brain Injury: A Population-Based Study of The Role of Age And Injury Severity. J. Neurotrauma 2007, 24, 435–445. [Google Scholar] [CrossRef]
- Thompson, H.J.; McCormick, W.C.; Kagan, S.H. Traumatic Brain Injury in Older Adults: Epidemiology, Outcomes, and Future Implications: Traumatic Brain Injury and Older Adults. J. Am. Geriatr. Soc. 2006, 54, 1590–1595. [Google Scholar] [CrossRef] [PubMed]
- Dawson, D.R.; Schwartz, M.L.; Winocur, G.; Stuss, D.T. Return to Productivity Following Traumatic Brain Injury: Cognitive, Psychological, Physical, Spiritual, and Environmental Correlates. Disabil. Rehabil. 2007, 29, 301–313. [Google Scholar] [CrossRef]
- Ponsford, J.; Schönberger, M. Family Functioning and Emotional State Two and Five Years after Traumatic Brain Injury. J. Int. Neuropsychol. Soc. 2010, 16, 306–317. [Google Scholar] [CrossRef] [PubMed]
- Ponsford, J.L.; Downing, M.G.; Olver, J.; Ponsford, M.; Acher, R.; Carty, M.; Spitz, G. Longitudinal Follow-Up of Patients with Traumatic Brain Injury: Outcome at Two, Five, and Ten Years Post-Injury. J. Neurotrauma 2014, 31, 64–77. [Google Scholar] [CrossRef] [PubMed]
- Haagsma, J.A.; Graetz, N.; Bolliger, I.; Naghavi, M.; Higashi, H.; Mullany, E.C.; Abera, S.F.; Abraham, J.P.; Adofo, K.; Alsharif, U.; et al. The Global Burden of Injury: Incidence, Mortality, Disability-Adjusted Life Years and Time Trends from the Global Burden of Disease Study 2013. Inj. Prev. 2016, 22, 3–18. [Google Scholar] [CrossRef] [Green Version]
- Olesen, J.; Gustavsson, A.; Svensson, M.; Wittchen, H.-U.; Jönsson, B.; on behalf of the CDBE2010 Study Group; European Brain Council. The Economic Cost of Brain Disorders in Europe: Economic Cost of Brain Disorders in Europe. Eur. J. Neurol. 2012, 19, 155–162. [Google Scholar] [CrossRef]
- Maas, A.I.R.; Menon, D.K.; Adelson, P.D.; Andelic, N.; Bell, M.J.; Belli, A.; Bragge, P.; Brazinova, A.; Büki, A.; Chesnut, R.M.; et al. Traumatic Brain Injury: Integrated Approaches to Improve Prevention, Clinical Care, and Research. Lancet Neurol. 2017, 16, 987–1048. [Google Scholar] [CrossRef] [Green Version]
- van der Naalt, J.; Timmerman, M.E.; de Koning, M.E.; van der Horn, H.J.; Scheenen, M.E.; Jacobs, B.; Hageman, G.; Yilmaz, T.; Roks, G.; Spikman, J.M. Early Predictors of Outcome after Mild Traumatic Brain Injury (UPFRONT): An Observational Cohort Study. Lancet Neurol. 2017, 16, 532–540. [Google Scholar] [CrossRef] [PubMed]
- Perry, D.C.; Sturm, V.E.; Peterson, M.J.; Pieper, C.F.; Bullock, T.; Boeve, B.F.; Miller, B.L.; Guskiewicz, K.M.; Berger, M.S.; Kramer, J.H.; et al. Association of Traumatic Brain Injury with Subsequent Neurological and Psychiatric Disease: A Meta-Analysis. J. Neurosurg. 2016, 124, 511–526. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dikmen, S.; Machamer, J.; Temkin, N. Mild Traumatic Brain Injury: Longitudinal Study of Cognition, Functional Status, and Post-Traumatic Symptoms. J. Neurotrauma 2017, 34, 1524–1530. [Google Scholar] [CrossRef] [Green Version]
- Sigurdardottir, S.; Andelic, N.; Roe, C.; Schanke, A.-K. Cognitive Recovery and Predictors of Functional Outcome 1 Year after Traumatic Brain Injury. J. Int. Neuropsychol. Soc. 2009, 15, 740–750. [Google Scholar] [CrossRef]
- Corrigan, J.D.; Hammond, F.M. Traumatic Brain Injury as a Chronic Health Condition. Arch. Phys. Med. Rehabil. 2013, 94, 1199–1201. [Google Scholar] [CrossRef] [PubMed]
- Corrigan, J.D.; Cuthbert, J.P.; Harrison-Felix, C.; Whiteneck, G.G.; Bell, J.M.; Miller, A.C.; Coronado, V.G.; Pretz, C.R. US Population Estimates of Health and Social Outcomes 5 Years After Rehabilitation for Traumatic Brain Injury. J. Head Trauma Rehabil. 2014, 29, E1–E9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Satz, P.; Forney, D.L.; Zaucha, K.; Asarnow, R.R.; Light, R.; McCleary, C.; Levin, H.; Kelly, D.; Bergsneider, M.; Hovda, D.; et al. Depression, Cognition, and Functional Correlates of Recovery Outcome after Traumatic Brain Injury. Brain Inj. 1998, 12, 537–553. [Google Scholar] [CrossRef]
- Hawthorne, G.; Gruen, R.; Kaye, A.H. Traumatic Brain Injury and Long-Term Quality of Life: Findings from an Australian Study. J. Neurotrauma 2009, 26, 1623–1633. [Google Scholar] [CrossRef]
- Pagulayan, K.F.; Temkin, N.R.; Machamer, J.; Dikmen, S.S. A Longitudinal Study of Health-Related Quality of Life After Traumatic Brain Injury. Arch. Phys. Med. Rehabil. 2006, 87, 611–618. [Google Scholar] [CrossRef]
- Soberg, H.; Roe, C.; Anke, A.; Arango-Lasprilla, J.; Skandsen, T.; Sveen, U.; Steinbüchel, N.; Andelic, N. Health-Related Quality of Life 12 Months after Severe Traumatic Brain Injury: A Prospective Nationwide Cohort Study. J. Rehabil. Med. 2013, 45, 785–791. [Google Scholar] [CrossRef] [Green Version]
- Jeon, I.-C.; Kim, O.-L.; Kim, M.-S.; Kim, S.-H.; Chang, C.-H.; Bai, D.-S. The Effect of Premorbid Demographic Factors on the Recovery of Neurocognitive Function in Traumatic Brain Injury Patients. J. Korean Neurosurg. Soc. 2008, 44, 295. [Google Scholar] [CrossRef] [PubMed]
- Mushkudiani, N.A.; Engel, D.C.; Steyerberg, E.W.; Butcher, I.; Lu, J.; Marmarou, A.; Slieker, F.; McHugh, G.S.; Murray, G.D.; Maas, A.I.R. Prognostic Value of Demographic Characteristics in Traumatic Brain Injury: Results from The IMPACT Study. J. Neurotrauma 2007, 24, 259–269. [Google Scholar] [CrossRef] [PubMed]
- Arango-Lasprilla, J.C.; Rosenthal, M.; DeLuca, J.; Cifu, D.X.; Hanks, R.; Komaroff, E. Functional Outcomes From Inpatient Rehabilitation After Traumatic Brain Injury: How Do Hispanics Fare? Arch. Phys. Med. Rehabil. 2007, 88, 11–18. [Google Scholar] [CrossRef] [PubMed]
- Arango-Lasprilla, J.C.; Rosenthal, M.; Deluca, J.; Komaroff, E.; Sherer, M.; Cifu, D.; Hanks, R. Traumatic Brain Injury and Functional Outcomes: Does Minority Status Matter? Brain Inj. 2007, 21, 701–708. [Google Scholar] [CrossRef] [PubMed]
- Polinder, S.; Cnossen, M.C.; Real, R.G.L.; Covic, A.; Gorbunova, A.; Voormolen, D.C.; Master, C.L.; Haagsma, J.A.; Diaz-Arrastia, R.; von Steinbuechel, N. A Multidimensional Approach to Post-Concussion Symptoms in Mild Traumatic Brain Injury. Front. Neurol. 2018, 9, 1113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wagner, A.K.; Sasser, H.C.; Hammond, F.M.; Wiercisiewski, D.; Alexander, J. Intentional Traumatic Brain Injury: Epidemiology, Risk Factors, and Associations with Injury Severity and Mortality. J. Trauma Inj. Infect. Crit. Care 2000, 49, 404–410. [Google Scholar] [CrossRef] [PubMed]
- Dillahunt-Aspillaga, C.; Nakase-Richardson, R.; Hart, T.; Powell-Cope, G.; Dreer, L.E.; Eapen, B.C.; Barnett, S.D.; Mellick, D.; Haskin, A.; Silva, M.A. Predictors of Employment Outcomes in Veterans With Traumatic Brain Injury: A VA Traumatic Brain Injury Model Systems Study. J. Head Trauma Rehabil. 2017, 32, 271–282. [Google Scholar] [CrossRef]
- Schreiber, M.A. Determinants of Mortality in Patients With Severe Blunt Head Injury. Arch. Surg. 2002, 137, 285. [Google Scholar] [CrossRef]
- Signorini, D.F.; Andrews, P.J.D.; Jones, P.A.; Wardlaw, J.M.; Miller, J.D. Adding Insult to Injury: The Prognostic Value of Early Secondary Insults for Survival after Traumatic Brain Injury. J. Neurol. Neurosurg. Psychiatry 1999, 66, 26–31. [Google Scholar] [CrossRef]
- Ketchum, J.M.; Almaz Getachew, M.; Krch, D.; Baños, J.H.; Kolakowsky-Hayner, S.A.; Lequerica, A.; Jamison, L.; Arango-Lasprilla, J.C. Early Predictors of Employment Outcomes 1 Year Post Traumatic Brain Injury in a Population of Hispanic Individuals. NeuroRehabilitation 2012, 30, 13–22. [Google Scholar] [CrossRef]
- Nakase-Richardson, R.; Sherer, M.; Seel, R.T.; Hart, T.; Hanks, R.; Arango-Lasprilla, J.C.; Yablon, S.A.; Sander, A.M.; Barnett, S.D.; Walker, W.C.; et al. Utility of Post-Traumatic Amnesia in Predicting 1-Year Productivity Following Traumatic Brain Injury: Comparison of the Russell and Mississippi PTA Classification Intervals. J. Neurol. Neurosurg. Psychiatry 2011, 82, 494–499. [Google Scholar] [CrossRef] [PubMed]
- Levin, H.S. Prediction of Recovery from Traumatic Brain Injury. J. Neurotrauma 1995, 12, 913–922. [Google Scholar] [CrossRef]
- Hellawell, D.J.; Taylor, R.; Pentland, B. Cognitive and Psychosocial Outcome Following Moderate or Severe Traumatic Brain Injury. Brain Inj. 1999, 13, 489–504. [Google Scholar] [CrossRef]
- Forslund, M.V.; Arango-Lasprilla, J.C.; Roe, C.; Perrin, P.B.; Sigurdardottir, S.; Andelic, N. Multi-Level Modelling of Employment Probability Trajectories and Employment Stability at 1, 2 and 5 Years after Traumatic Brain Injury. Brain Inj. 2014, 28, 980–986. [Google Scholar] [CrossRef] [PubMed]
- Cattelani, R.; Tanzi, F.; Lombardi, F.; Mazzucchi, A. Competitive Re-Employment after Severe Traumatic Brain Injury: Clinical, Cognitive and Behavioural Predictive Variables. Brain Inj. 2002, 16, 51–64. [Google Scholar] [CrossRef] [PubMed]
- Corrigan, J.D.; Horn, S.D.; Barrett, R.S.; Smout, R.J.; Bogner, J.; Hammond, F.M.; Brandstater, M.E.; Majercik, S. Effects of Patient Preinjury and Injury Characteristics on Acute Rehabilitation Outcomes for Traumatic Brain Injury. Arch. Phys. Med. Rehabil. 2015, 96, S209–S221. [Google Scholar] [CrossRef] [Green Version]
- Cowen, T.D.; Meythaler, J.M.; DeVivo, M.J.; Ivie, C.S.; Lebow, J.; Novack, T.A. Influence of Early Variables in Traumatic Brain Injury on Functional Independence Measure Scores and Rehabilitation Length of Stay and Charges. Arch. Phys. Med. Rehabil. 1995, 76, 797–803. [Google Scholar] [CrossRef]
- Einarsen, C.E.; van der Naalt, J.; Jacobs, B.; Follestad, T.; Moen, K.G.; Vik, A.; Håberg, A.K.; Skandsen, T. Moderate Traumatic Brain Injury: Clinical Characteristics and a Prognostic Model of 12-Month Outcome. World Neurosurg. 2018, 114, e1199–e1210. [Google Scholar] [CrossRef]
- Bonow, R.H.; Barber, J.; Temkin, N.R.; Videtta, W.; Rondina, C.; Petroni, G.; Lujan, S.; Alanis, V.; La Fuente, G.; Lavadenz, A.; et al. The Outcome of Severe Traumatic Brain Injury in Latin America. World Neurosurg. 2018, 111, e82–e90. [Google Scholar] [CrossRef]
- Novack, T.A.; Bush, B.A.; Meythaler, J.M.; Canupp, K. Outcome after Traumatic Brain Injury: Pathway Analysis of Contributions from Premorbid, Injury Severity, and Recovery Variables. Arch. Phys. Med. Rehabil. 2001, 82, 300–305. [Google Scholar] [CrossRef]
- MacMillan, P.J.; Hart, R.P.; Martelli, M.F.; Zasler, N.D. Pre-Injury Status and Adaptation Following Traumatic Brain Injury. Brain Inj. 2002, 16, 41–49. [Google Scholar] [CrossRef] [PubMed]
- Fraser, E.E.; Downing, M.G.; Biernacki, K.; McKenzie, D.P.; Ponsford, J.L. Cognitive Reserve and Age Predict Cognitive Recovery after Mild to Severe Traumatic Brain Injury. J. Neurotrauma 2019, 36, 2753–2761. [Google Scholar] [CrossRef]
- Hart, T.; Brenner, L.; Clark, A.N.; Bogner, J.A.; Novack, T.A.; Chervoneva, I.; Nakase-Richardson, R.; Arango-Lasprilla, J.C. Major and Minor Depression After Traumatic Brain Injury. Arch. Phys. Med. Rehabil. 2011, 92, 1211–1219. [Google Scholar] [CrossRef] [PubMed]
- McCauley, S.R.; Wilde, E.A.; Miller, E.R.; Frisby, M.L.; Garza, H.M.; Varghese, R.; Levin, H.S.; Robertson, C.S.; McCarthy, J.J. Preinjury Resilience and Mood as Predictors of Early Outcome Following Mild Traumatic Brain Injury. J. Neurotrauma 2013, 30, 642–652. [Google Scholar] [CrossRef] [PubMed]
- Willer, B.; Leddy, J.J. Management of Concussion and Post-Concussion Syndrome. Curr. Treat. Options Neurol. 2006, 8, 415–426. [Google Scholar] [CrossRef]
- Goreth, M.B.; Palokas, M. Association between Premorbid Neuropsychological Conditions and Pediatric Mild Traumatic Brain Injury/Concussion Recovery Time and Symptom Severity: A Systematic Review. JBI Database Syst. Rev. Implement. Rep. 2019, 17, 1464–1493. [Google Scholar] [CrossRef]
- Arango-Lasprilla, J.; Zeldovich, M.; Olabarrieta-Landa, L.; Forslund, M.; Núñez-Fernández, S.; von Steinbuechel, N.; Howe, E.; Røe, C.; Andelic, N.; CENTER-TBI Participants and Investigators. Early Predictors of Employment Status One Year Post Injury in Individuals with Traumatic Brain Injury in Europe. J. Clin. Med. 2020, 9, 2007. [Google Scholar] [CrossRef] [PubMed]
- Connelly, J.B.; Chell, S.; Tennant, A.; Rigby, A.S.; Airey, C.M. Modelling 5-Year Functional Outcome in a Major Traumatic Injury Survivor Cohort. Disabil. Rehabil. 2006, 28, 629–636. [Google Scholar] [CrossRef]
- Katz, D.I.; Polyak, M.; Coughlan, D.; Nichols, M.; Roche, A. Natural History of Recovery from Brain Injury after Prolonged Disorders of Consciousness: Outcome of Patients Admitted to Inpatient Rehabilitation with 1–4 Year Follow-Up. Prog Brain Res. 2009, 177, 73–88. [Google Scholar] [CrossRef]
- Blackerby, W.F. Intensity of Rehabilitation and Length of Stay. Brain Inj. 1990, 4, 167–173. [Google Scholar] [CrossRef] [PubMed]
- Zarshenas, S.; Colantonio, A.; Horn, S.D.; Jaglal, S.; Cullen, N. Cognitive and Motor Recovery and Predictors of Long-Term Outcome in Patients With Traumatic Brain Injury. Arch. Phys. Med. Rehabil. 2019, 100, 1274–1282. [Google Scholar] [CrossRef] [PubMed]
- Howrey, B.T.; Graham, J.E.; Pappadis, M.R.; Granger, C.V.; Ottenbacher, K.J. Trajectories of Functional Change After Inpatient Rehabilitation for Traumatic Brain Injury. Arch. Phys. Med. Rehabil. 2017, 98, 1606–1613. [Google Scholar] [CrossRef] [PubMed]
- Røe, C.; Tverdal, C.; Howe, E.I.; Tenovuo, O.; Azouvi, P.; Andelic, N. Randomized Controlled Trials of Rehabilitation Services in the Post-Acute Phase of Moderate and Severe Traumatic Brain Injury—A Systematic Review. Front. Neurol. 2019, 10, 557. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Testa, J.A.; Malec, J.F.; Moessner, A.M.; Brown, A.W. Outcome After Traumatic Brain Injury: Effects of Aging on Recovery. Arch. Phys. Med. Rehabil. 2005, 86, 1815–1823. [Google Scholar] [CrossRef]
- Susman, M.; DiRusso, S.M.; Sullivan, T.; Risucci, D.; Nealon, P.; Cuff, S.; Haider, A.; Benzil, D. Traumatic Brain Injury in the Elderly: Increased Mortality and Worse Functional Outcome At Discharge Despite Lower Injury Severity. J. Trauma Inj. Infect. Crit. Care 2002, 53, 219–224. [Google Scholar] [CrossRef]
- Farace, E.; Alves, W.M. Do Women Fare Worse: A Metaanalysis of Gender Differences in Traumatic Brain Injury Outcome. J. Neurosurg. 2000, 93, 539–545. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bruns, J.; Hauser, W.A. The Epidemiology of Traumatic Brain Injury: A Review: Epidemiology of Traumatic Brain Injury. Epilepsia 2003, 44, 2–10. [Google Scholar] [CrossRef]
- Mikolic, A.; van Klaveren, D.; Oude Groeniger, J.; Wiegers, E.; Lingsma, H.F.; Zeldovich, M.; von Steinbuechel, N.; Maas, A.; Roeters van Lennep, J.E.; Polinder, S. Differences between Men and Women in Treatment and Outcome Following Traumatic Brain Injury. J. Neurotrauma 2020, 38, 235–251. [Google Scholar] [CrossRef] [PubMed]
- Lingsma, H.F.; Cnossen, M.C. Identification of Patients at Risk for Poor Outcome after MTBI. Lancet Neurol. 2017, 16, 494–495. [Google Scholar] [CrossRef]
- Karzmark, P.; Hall, K.; Englander, J. Late-Onset Post-Concussion Symptoms after Mild Brain Injury: The Role of Premorbid, Injury-Related, Environmental, and Personality Factors. Brain Inj. 1995, 9, 21–26. [Google Scholar] [CrossRef]
- Peeters, W.; van den Brande, R.; Polinder, S.; Brazinova, A.; Steyerberg, E.W.; Lingsma, H.F.; Maas, A.I.R. Epidemiology of Traumatic Brain Injury in Europe. Acta Neurochir. 2015, 157, 1683–1696. [Google Scholar] [CrossRef] [Green Version]
- Lenell, S.; Nyholm, L.; Lewén, A.; Enblad, P. Clinical Outcome and Prognostic Factors in Elderly Traumatic Brain Injury Patients Receiving Neurointensive Care. Acta Neurochir. 2019, 161, 1243–1254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kraus, J.F.; Peek-Asa, C.; McArthur, D. The Independent Effect of Gender on Outcomes Following Traumatic Brain Injury: A Preliminary Investigation. Neurosurg. Focus 2000, 8, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Slewa-Younan, S.; Baguley, I.J.; Heriseanu, R.; Cameron, I.D.; Pitsiavas, V.; Mudaliar, Y.; Nayyar, V. Do Men and Women Differ in Their Course Following Traumatic Brain Injury? A Preliminary Prospective Investigation of Early Outcome. Brain Inj. 2008, 22, 183–191. [Google Scholar] [CrossRef]
- Groswasser, Z.; Cohen, M.; Keren, O. Female TBI Patients Recover Better than Males. Brain Inj. 1998, 12, 805–808. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, R.E.; Livingston, L.; Marwitz, J.H.; Gueck, S.; Kreutzer, J.S.; Sander, A.M. Complicated Mild Traumatic Brain Injury on the Inpatient Rehabilitation Unit: A Multicenter Analysis. J. Head Trauma Rehabil. 2006, 21, 260–271. [Google Scholar] [CrossRef]
- Ratcliff, J.J.; Greenspan, A.I.; Goldstein, F.C.; Stringer, A.Y.; Bushnik, T.; Hammond, F.M.; Novack, T.A.; Whyte, J.; Wright, D.W. Gender and Traumatic Brain Injury: Do the Sexes Fare Differently? Brain Inj. 2007, 21, 1023–1030. [Google Scholar] [CrossRef]
- Bombardier, C.H.; Hoekstra, T.; Dikmen, S.; Fann, J.R. Depression Trajectories during the First Year after Traumatic Brain Injury. J. Neurotrauma 2016, 33, 2115–2124. [Google Scholar] [CrossRef]
- Stulemeijer, M.; van der Werf, S.; Borm, G.F.; Vos, P.E. Early Prediction of Favourable Recovery 6 Months after Mild Traumatic Brain Injury. J. Neurol. Neurosurg. Psychiatry 2008, 79, 936–942. [Google Scholar] [CrossRef]
- Walker, W.C.; Stromberg, K.A.; Marwitz, J.H.; Sima, A.P.; Agyemang, A.A.; Graham, K.M.; Harrison-Felix, C.; Hoffman, J.M.; Brown, A.W.; Kreutzer, J.S.; et al. Predicting Long-Term Global Outcome after Traumatic Brain Injury: Development of a Practical Prognostic Tool Using the Traumatic Brain Injury Model Systems National Database. J. Neurotrauma 2018, 35, 1587–1595. [Google Scholar] [CrossRef] [Green Version]
- Brett, B.L.; Kramer, M.D.; Whyte, J.; McCrea, M.A.; Stein, M.B.; Giacino, J.T.; Sherer, M.; Markowitz, A.J.; Manley, G.T.; Nelson, L.D.; et al. Latent Profile Analysis of Neuropsychiatric Symptoms and Cognitive Function of Adults 2 Weeks After Traumatic Brain Injury: Findings From the TRACK-TBI Study. JAMA Netw. Open 2021, 4, e213467. [Google Scholar] [CrossRef]
- Stocchetti, N.; Zanier, E.R. Chronic Impact of Traumatic Brain Injury on Outcome and Quality of Life: A Narrative Review. Crit. Care 2016, 20, 148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sigurdardottir, S.; Andelic, N.; Roe, C.; Schanke, A.K. Identifying Longitudinal Trajectories of Emotional Distress Symptoms 5 Years after Traumatic Brain Injury. Brain Inj. 2014, 28, 1542–1550. [Google Scholar] [CrossRef]
- Teymoori, A.; Real, R.; Gorbunova, A.; Haghish, E.F.; Andelic, N.; Wilson, L.; Asendorf, T.; Menon, D.; von Steinbüchel, N. Measurement Invariance of Assessments of Depression (PHQ-9) and Anxiety (GAD-7) across Sex, Strata and Linguistic Backgrounds in a European-Wide Sample of Patients after Traumatic Brain Injury. J. Affect. Disord. 2020, 262, 278–285. [Google Scholar] [CrossRef] [PubMed]
- Wang, B.; Zeldovich, M.; Rauen, K.; Wu, Y.-J.; Covic, A.; Muller, I.; Haagsma, J.A.; Polinder, S.; Menon, D.; Asendorf, T.; et al. Longitudinal Analyses of the Reciprocity of Depression and Anxiety after Traumatic Brain Injury and Its Clinical Implications. J. Clin. Med. 2021, 10, 5597. [Google Scholar] [CrossRef]
- Andelic, N.; Hammergren, N.; Bautz-Holter, E.; Sveen, U.; Brunborg, C.; Røe, C. Functional Outcome and Health-Related Quality of Life 10 Years after Moderate-to-Severe Traumatic Brain Injury. Acta Neurol. Scand. 2009, 120, 16–23. [Google Scholar] [CrossRef] [PubMed]
- Dijkers, M.P. Quality of Life after Traumatic Brain Injury: A Review of Research Approaches and Findings. Arch. Phys. Med. Rehabil. 2004, 85, 21–35. [Google Scholar] [CrossRef]
- Maas, A.I.R.; Menon, D.K.; Steyerberg, E.W.; Citerio, G.; Lecky, F.; Manley, G.T.; Hill, S.; Legrand, V.; Sorgner, A. Collaborative European NeuroTrauma Effectiveness Research in Traumatic Brain Injury (CENTER-TBI): A Prospective Longitudinal Observational Study. Neurosurgery 2015, 76, 67–80. [Google Scholar] [CrossRef] [Green Version]
- Steyerberg, E.W.; Wiegers, E.; Sewalt, C.; Buki, A.; Citerio, G.; De Keyser, V.; Ercole, A.; Kunzmann, K.; Lanyon, L.; Lecky, F.; et al. Case-Mix, Care Pathways, and Outcomes in Patients with Traumatic Brain Injury in CENTER-TBI: A European Prospective, Multicentre, Longitudinal, Cohort Study. Lancet Neurol. 2019, 18, 923–934. [Google Scholar] [CrossRef]
- Mayhew, D.; Mendonca, V.; Murthy, B.V.S. A Review of ASA Physical Status—Historical Perspectives and Modern Developments. Anaesthesia 2019, 74, 373–379. [Google Scholar] [CrossRef] [Green Version]
- Wilson, J.T.L.; Pettigrew, L.E.L.; Teasdale, G. Structured Interviews for the Glasgow Outcome Scale and the Extended Glasgow Outcome Scale: Guidelines for Their Use. J. Neurotrauma 1998, 15, 573–585. [Google Scholar] [CrossRef] [PubMed]
- Wilson, L.; Edwards, P.; Fiddes, H.; Stewart, E.; Teasdale, G.M. Reliability of Postal Questionnaires for the Glasgow Outcome Scale. J. Neurotrauma 2002, 19, 999–1005. [Google Scholar] [CrossRef] [PubMed]
- Kunzmann, K.; Wernisch, L.; Richardson, S.; Steyerberg, E.W.; Lingsma, H.; Ercole, A.; Maas, A.I.R.; Menon, D.; Wilson, L. Imputation of Ordinal Outcomes: A Comparison of Approaches in Traumatic Brain Injury. J. Neurotrauma 2021, 38, 455–463. [Google Scholar] [CrossRef] [PubMed]
- Teasdale, G.; Jennett, B. Assessment of Coma and Impaired Consciousness. A Practical Scale. Lancet Lond. Engl. 1974, 2, 81–84. [Google Scholar] [CrossRef]
- Gennarelli, T.A.; Wodzin, E. Association for the Advancement of Automotive Medicine. In Abbreviated Injury Scale 2005: Update 2008; Association for the Advancement of Automative Medicine: Barrington, IL, USA, 2008; ISBN 978-0-00-000202-0. [Google Scholar]
- Gennarelli, T.A.; Wodzin, E. AIS 2005: A Contemporary Injury Scale. Injury 2006, 37, 1083–1091. [Google Scholar] [CrossRef]
- von Steinbuechel, N.; Wilson, L.; Gibbons, H.; Muehlan, H.; Schmidt, H.; Schmidt, S.; Sasse, N.; Koskinen, S.; Sarajuuri, J.; Höfer, S.; et al. QOLIBRI Overall Scale: A Brief Index of Health-Related Quality of Life after Traumatic Brain Injury. J. Neurol. Neurosurg. Psychiatry 2012, 83, 1041–1047. [Google Scholar] [CrossRef]
- Muehlan, H.; Wilson, L.; von Steinbüchel, N. A Rasch Analysis of the QOLIBRI Six-Item Overall Scale. Assessment 2016, 23, 124–130. [Google Scholar] [CrossRef]
- Wilson, L.; Marsden-Loftus, I.; Koskinen, S.; Bakx, W.; Bullinger, M.; Formisano, R.; Maas, A.; Neugebauer, E.; Powell, J.; Sarajuuri, J.; et al. Interpreting Quality of Life after Brain Injury Scores: Cross-Walk with the Short Form-36. J. Neurotrauma 2017, 34, 59–65. [Google Scholar] [CrossRef]
- Ware, J.E.; Kosinski, M.; Keller, S.D. A 12-Item Short-Form Health Survey: Construction of Scales and Preliminary Tests of Reliability and Validity. Med. Care 1996, 34, 220–233. [Google Scholar] [CrossRef] [Green Version]
- Ware, J.E.; Kosinski, M.; Turner-Bowker, D.M.; Gandek, B. User’s Manual for the SF12v2 Health Survey; Lippincott Williams & Wilkins, Inc.: Lincoln, RI, USA, 2009; ISBN 1-891810-10-3. [Google Scholar]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.W.; Löwe, B. A Brief Measure for Assessing Generalized Anxiety Disorder: The GAD-7. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef] [Green Version]
- Teymoori, A.; Gorbunova, A.; Haghish, F.E.; Real, R.; Zeldovich, M.; Wu, Y.-J.; Polinder, S.; Asendorf, T.; Menon, D.; CENTER-TBI Investigators and Participants; et al. Factorial Structure and Validity of Depression (PHQ-9) and Anxiety (GAD-7) Scales after Traumatic Brain Injury. J. Clin. Med. 2020, 9, 873. [Google Scholar] [CrossRef] [Green Version]
- Kroenke, K.; Spitzer, R.L. The PHQ-9: A New Depression Diagnostic and Severity Measure. Psychiatr. Ann. 2002, 32, 509–515. [Google Scholar] [CrossRef] [Green Version]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B.W. The PHQ-9: Validity of a Brief Depression Severity Measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef]
- Blevins, C.A.; Weathers, F.W.; Davis, M.T.; Witte, T.K.; Domino, J.L. The Posttraumatic Stress Disorder Checklist for DSM-5 (PCL-5): Development and Initial Psychometric Evaluation. J. Trauma. Stress 2015, 28, 489–498. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-5, 5th ed.; American Psychiatric Publishing: Washington, DC, USA, 2013; ISBN 978-0-89042-555-8. [Google Scholar]
- Ashbaugh, A.R.; Houle-Johnson, S.; Herbert, C.; El-Hage, W.; Brunet, A. Psychometric Validation of the English and French Versions of the Posttraumatic Stress Disorder Checklist for DSM-5 (PCL-5). PLoS ONE 2016, 11, e0161645. [Google Scholar] [CrossRef]
- von Steinbuechel, N.; Rauen, K.; Bockhop, F.; Covic, A.; Krenz, U.; Plass, A.; Cunitz, K.; Polinder, S.; Wilson, L.; Steyerberg, E.; et al. Psychometric Characteristics of the Patient-Reported Outcome Measures Applied in the CENTER-TBI Study. J. Clin. Med. 2021, 10, 2396. [Google Scholar] [CrossRef]
- King, N.S.; Crawford, S.; Wenden, F.J.; Moss, N.E.; Wade, D.T. The Rivermead Post Concussion Symptoms Questionnaire: A Measure of Symptoms Commonly Experienced after Head Injury and Its Reliability. J. Neurol. 1995, 242, 587–592. [Google Scholar] [CrossRef] [PubMed]
- Potter, S.; Leigh, E.; Wade, D.; Fleminger, S. The Rivermead Post Concussion Symptoms Questionnaire: A Confirmatory Factor Analysis. J. Neurol. 2006, 253, 1603–1614. [Google Scholar] [CrossRef] [PubMed]
- Proust-Lima, C.; Philipps, V.; Liquet, B. Estimation of Extended Mixed Models Using Latent Classes and Latent Processes: The R Package Lcmm. J. Stat. Softw. 2017, 78, 1–56. [Google Scholar] [CrossRef] [Green Version]
- Nylund, K.L.; Asparouhov, T.; Muthén, B.O. Deciding on the Number of Classes in Latent Class Analysis and Growth Mixture Modeling: A Monte Carlo Simulation Study. Struct. Equ. Model. Multidiscip. J. 2007, 14, 535–569. [Google Scholar] [CrossRef]
- Nagin, D.S. Group-Based Modeling of Development; Harvard University Press: Cambridge, MA, USA, 2005; ISBN 978-0-674-01686-6. [Google Scholar]
- Lo, Y. Testing the Number of Components in a Normal Mixture. Biometrika 2001, 88, 767–778. [Google Scholar] [CrossRef]
- Nylund-Gibson, K.; Choi, A.Y. Ten Frequently Asked Questions about Latent Class Analysis. Transl. Issues Psychol. Sci. 2018, 4, 440–461. [Google Scholar] [CrossRef]
- Bartlett, J. Bootstrap Inference for Multiple Imputation. 2021. Available online: https://cran.r-project.org/package=bootImpute (accessed on 10 March 2023).
- van Buuren, S.; Groothuis-Oudshoorn, K. Mice: Multivariate Imputation by Chained Equations in R. J. Stat. Softw. 2011, 45, 1–67. [Google Scholar] [CrossRef] [Green Version]
- R Core Team. A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2022. [Google Scholar]
- Von Steinbuechel, N.; Rauen, K.; Covic, A.; Krenz, U.; Bockhop, F.; Mueller, I.; Cunitz, K.; Polinder, S.; Steyerberg, E.W.; Vester, J.; et al. Sensitivity of Outcome Instruments in Different Patient Groups after Traumatic Brain Injury: Results from the CENTER-TBI Study. PLoS ONE 2023. [Google Scholar] [CrossRef]
- Chiang, C.-C.; Guo, S.-E.; Huang, K.-C.; Lee, B.-O.; Fan, J.-Y. Trajectories and Associated Factors of Quality of Life, Global Outcome, and Post-Concussion Symptoms in the First Year Following Mild Traumatic Brain Injury. Qual. Life Res. 2016, 25, 2009–2019. [Google Scholar] [CrossRef] [PubMed]
- McMahon, P.J.; Hricik, A.; Yue, J.K.; Puccio, A.M.; Inoue, T.; Lingsma, H.F.; Beers, S.R.; Gordon, W.A.; Valadka, A.B.; Manley, G.T.; et al. Symptomatology and Functional Outcome in Mild Traumatic Brain Injury: Results from the Prospective TRACK-TBI Study. J. Neurotrauma 2014, 31, 26–33. [Google Scholar] [CrossRef] [PubMed]
- Nelson, L.D.; Temkin, N.R.; Dikmen, S.; Barber, J.; Giacino, J.T.; Yuh, E.; Levin, H.S.; McCrea, M.A.; Stein, M.B.; Mukherjee, P.; et al. Recovery After Mild Traumatic Brain Injury in Patients Presenting to US Level I Trauma Centers: A Transforming Research and Clinical Knowledge in Traumatic Brain Injury (TRACK-TBI) Study. JAMA Neurol. 2019, 76, 1049. [Google Scholar] [CrossRef]
- Nelson, L.D.; Ranson, J.; Ferguson, A.R.; Giacino, J.; Okonkwo, D.O.; Valadka, A.B.; Manley, G.T.; McCrea, M.A.; The TRACK-TBI Investigators. Validating Multi-Dimensional Outcome Assessment Using the Traumatic Brain Injury Common Data Elements: An Analysis of the TRACK-TBI Pilot Study Sample. J. Neurotrauma 2017, 34, 3158–3172. [Google Scholar] [CrossRef]
- Zahniser, E.; Nelson, L.D.; Dikmen, S.S.; Machamer, J.E.; Stein, M.B.; Yuh, E.; Manley, G.T.; Temkin, N.R.; TRACK-TBI Investigators. The Temporal Relationship of Mental Health Problems and Functional Limitations Following MTBI: A TRACK-TBI and TED Study. J. Neurotrauma 2019, 36, 1786–1793. [Google Scholar] [CrossRef]
- Penna, S.; Novack, T.A.; Carlson, N.; Grote, M.; Corrigan, J.D.; Hart, T. Residence Following Traumatic Brain Injury: A Longitudinal Study. J. Head Trauma Rehabil. 2010, 25, 52–60. [Google Scholar] [CrossRef]
- Kilaru, S.; Garb, J.; Emhoff, T.; Fiallo, V.; Simon, B.; Swiencicki, T.; Lee, K.F. Long-Term Functional Status and Mortality of Elderly Patients with Severe Closed Head Injuries. J. Trauma Inj. Infect. Crit. Care 1996, 41, 957–963. [Google Scholar] [CrossRef]
- Stein, M.B.; Jain, S.; Giacino, J.T.; Levin, H.; Dikmen, S.; Nelson, L.D.; Vassar, M.J.; Okonkwo, D.O.; Diaz-Arrastia, R.; Robertson, C.S.; et al. Risk of Posttraumatic Stress Disorder and Major Depression in Civilian Patients After Mild Traumatic Brain Injury: A TRACK-TBI Study. JAMA Psychiatry 2019, 76, 249. [Google Scholar] [CrossRef]
- Graham, J.E.; Radice-Neumann, D.M.; Reistetter, T.A.; Hammond, F.M.; Dijkers, M.; Granger, C.V. Influence of Sex and Age on Inpatient Rehabilitation Outcomes Among Older Adults With Traumatic Brain Injury. Arch. Phys. Med. Rehabil. 2010, 91, 43–50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marquez de la Plata, C.D.; Hart, T.; Hammond, F.M.; Frol, A.B.; Hudak, A.; Harper, C.R.; O’Neil-Pirozzi, T.M.; Whyte, J.; Carlile, M.; Diaz-Arrastia, R. Impact of Age on Long-Term Recovery From Traumatic Brain Injury. Arch. Phys. Med. Rehabil. 2008, 89, 896–903. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- von Steinbuechel, N.; Real, R.G.L.; Sasse, N.; Wilson, L.; Otto, C.; Mullins, R.; Behr, R.; Deinsberger, W.; Martinez-Olivera, R.; Puschendorf, W.; et al. German Validation of Quality of Life after Brain Injury (QOLIBRI) Assessment and Associated Factors. PLoS ONE 2017, 12, e0176668. [Google Scholar] [CrossRef] [PubMed] [Green Version]







| N (Valid %) | Missing, N (%) | |||
|---|---|---|---|---|
| Sociodemographic characteristics | Age (in years) | M (SD) | 48.86 (19.49) | 0 (0.0) |
| Median | 50.00 | |||
| Range | 16.00–95.00 | |||
| Sex, N (%) | Female | 886 (34.7%) | 0 (0.0) | |
| Male | 1669 (65.3%) | |||
| Education level, N (%) | None/primary school | 327 (14.4) | 281 (11.0) | |
| At least secondary/high school | 852 (37.5) | |||
| Post-high school training | 469 (20.6) | |||
| College/university | 626 (27.5) | |||
| Employment status | Full-time employed | 1072 (44.7) | 159 (6.2) | |
| Part-time employed | 269 (11.2) | |||
| In training | 241 (10.1) | |||
| Unemployed | 216 (9.0) | |||
| Retired | 598 (25.0) | |||
| Marital status | Never been married | 756 (31.3) | 142 (5.6) | |
| Married | 1073 (44.5) | |||
| Living together/common law | 221 (9.2) | |||
| Divorced/separated | 229 (9.5) | |||
| Widowed | 134 (5.6) | |||
| Living alone | No | 2026 (79.4) | 3 (0.1) | |
| Yes | 526 (20.6) | |||
| Premorbid health status | Physical health Status (ASA) a | Normal healthy | 1510 (59.8) | 31 (1.2) |
| Mild disease | 805 (31.9) | |||
| Severe disease | 209 (8.3) | |||
| Psychological problems | No | 2212 (87.9) | 39 (1.5) | |
| Yes | 304 (12.1) | |||
| TBI history | No | 2190 (89.8) | 116 (4.5) | |
| Yes | 249 (10.2) | |||
| Developmental problems | No | 2483 (99.0) | 46 (1.8) | |
| Yes | 26 (1.0) | |||
| Injury-related factors | Cause of injury | Road traffic incident | 1026 (41.0) | 53 (2.1) |
| Incidental fall | 1113 (44.5) | |||
| Other a | 363 (14.5) | |||
| Clinical care pathways | ER | 530 (20.7) | 0 (0.0) | |
| Admission | 974 (38.1) | |||
| ICU | 1051 (41.1) | |||
| Length of hospital stay (days) | M (SD) | 11.44 (18.86) | 58 (2.3) | |
| Median | 4.22 | |||
| Range | 0.00–370.50 | |||
| Injury Severity Score (ISS) | M (SD) | 18.62 (14.90) | 33 (1.3) | |
| Median | 14.00 | |||
| Range | 1.00–75.00 | |||
| Brain Injury Score (AIS) | M (SD) | 2.99 (1.35) | 34 (1.3) | |
| Median | 3.00 | |||
| Range | 0.00– 6.00 | |||
| TBI severity | Uncomplicated mild | 935 (39.7) | 198 (7.7) | |
| Complicated mild | 829 (35.2) | |||
| Moderate | 183 (7.8) | |||
| Severe | 410 (17.4) | |||
| GOSE (3 months) | Vegetative State/Lower Severe Disability | 204 (8.0) | 0 (0.0) | |
| Upper Severe Disability | 274 (10.7) | |||
| Lower Moderate Disability | 226 (8.9) | |||
| Upper Moderate Disability | 398 (15.6) | |||
| Lower Good Recovery | 529 (20.7) | |||
| Upper Good Recovery | 924 (36.2) |
| 3 Months (N = 2309) | 6 Months (N = 2281) | 12 Months (N = 1802) | Number of Observations N (%) | |||
|---|---|---|---|---|---|---|
| SF-12v2 MCS | M (SD) | 47.05 (11.17) | 47.72 (11.30) | 47.44 (11.18) | 1 | 518 (20.3%) |
| Median | 48.76 | 49.84 | 49.64 | 2 | 918 (35.9%) | |
| Range | 9.71–72.86 | 7.56–71.98 | 10.16–73.80 | 3 | 1119 (43.8%) | |
| Missing | 417 (16.5%) | 367 (14.7%) | 495 (25.4%) | |||
| SF-12v2 PCS | M (SD) | 43.65 (11.29) | 45.73 (10.78) | 46.43 (10.20) | 1 | 506 (19.8%) |
| Median | 45.34 | 48.33 | 49.39 | 2 | 946 (37.0%) | |
| Range | 11.63–69.52 | 9.86–65.11 | 12.28–65.49 | 3 | 1103 (43.2%) | |
| Missing | 417 (16.5%) | 367 (14.7%) | 495 (25.4%) | |||
| QoLIBRI-OS | M (SD) | 67.39 (22.37) | 68.62 (21.59) | 68.27 (22.04) | 1 | 506 (19.8%) |
| Median | 71.00 | 71.00 | 71.00 | 2 | 946 (37.0%) | |
| Range | 0.00–100.00 | 0.00–100.00 | 0.00–100.00 | 3 | 1103 (43.2%) | |
| Missing | 409 (16.1%) | 373 (14.9%) | 493 (25.3%) | |||
| GAD-7 | M (SD) | 3.71 (4.57) | 3.58 (4.49) | 3.50 (4.38) | 1 | 626 (24.5%) |
| Median | 2.00 | 2.00 | 2.00 | 2 | 903 (35.3%) | |
| Range | 0.00–21.00 | 0.00–21.00 | 0.00–21.00 | 3 | 1026 (40.2%) | |
| Missing | 524 (20.7%) | 412 (16.5%) | 540 (27.7%) | |||
| PHQ-9 | M (SD) | 5.29 (5.40) | 5.01 (5.31) | 4.97 (5.38) | 1 | 625 (24.5%) |
| Median | 4.00 | 3.00 | 3.00 | 2 | 905 (35.4%) | |
| Range | 0.00–27.00 | 0.00–27.00 | 0.00–27.00 | 3 | 1025 (40.1%) | |
| Missing | 519 (20.5%) | 409 (16.3%) | 548 (28.1%) | |||
| PCL-5 | M (SD) | 13.12 (13.97) | 12.20 (13.64) | 12.30 (13.77) | 1 | 632 (24.7%) |
| Median | 8.00 | 8.00 | 7.00 | 2 | 902 (35.3%) | |
| Range | 0.00–79.00 | 0.00–80.00 | 0.00–79.00 | 3 | 1021 (40.0%) | |
| Missing | 516 (20.4%) | 414 (16.5%) | 557 (28.6%) | |||
| RPQ | M (SD) | 11.29 (12.57) | 10.96 (12.39) | 11.00 (12.25) | 1 | 587 (23.0%) |
| Median | 7.00 | 6.00 | 7.00 | 2 | 925 (36.2%) | |
| Range | 0.00–61.00 | 0.00–64.00 | 0.00–57.00 | 3 | 1043 (40.8%) | |
| Missing | 497 (19.6%) | 391 (15.6%) | 532 (27.3%) | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
von Steinbuechel, N.; Hahm, S.; Muehlan, H.; Arango-Lasprilla, J.C.; Bockhop, F.; Covic, A.; Schmidt, S.; Steyerberg, E.W.; Maas, A.I.R.; Menon, D.; et al. Impact of Sociodemographic, Premorbid, and Injury-Related Factors on Patient-Reported Outcome Trajectories after Traumatic Brain Injury (TBI). J. Clin. Med. 2023, 12, 2246. https://doi.org/10.3390/jcm12062246
von Steinbuechel N, Hahm S, Muehlan H, Arango-Lasprilla JC, Bockhop F, Covic A, Schmidt S, Steyerberg EW, Maas AIR, Menon D, et al. Impact of Sociodemographic, Premorbid, and Injury-Related Factors on Patient-Reported Outcome Trajectories after Traumatic Brain Injury (TBI). Journal of Clinical Medicine. 2023; 12(6):2246. https://doi.org/10.3390/jcm12062246
Chicago/Turabian Stylevon Steinbuechel, Nicole, Stefanie Hahm, Holger Muehlan, Juan Carlos Arango-Lasprilla, Fabian Bockhop, Amra Covic, Silke Schmidt, Ewout W. Steyerberg, Andrew I. R. Maas, David Menon, and et al. 2023. "Impact of Sociodemographic, Premorbid, and Injury-Related Factors on Patient-Reported Outcome Trajectories after Traumatic Brain Injury (TBI)" Journal of Clinical Medicine 12, no. 6: 2246. https://doi.org/10.3390/jcm12062246