
The Biology of Stress Intolerance in Patients with Chronic Pain—State of the Art and Future Directions
 , , , , , and
, , , , , and 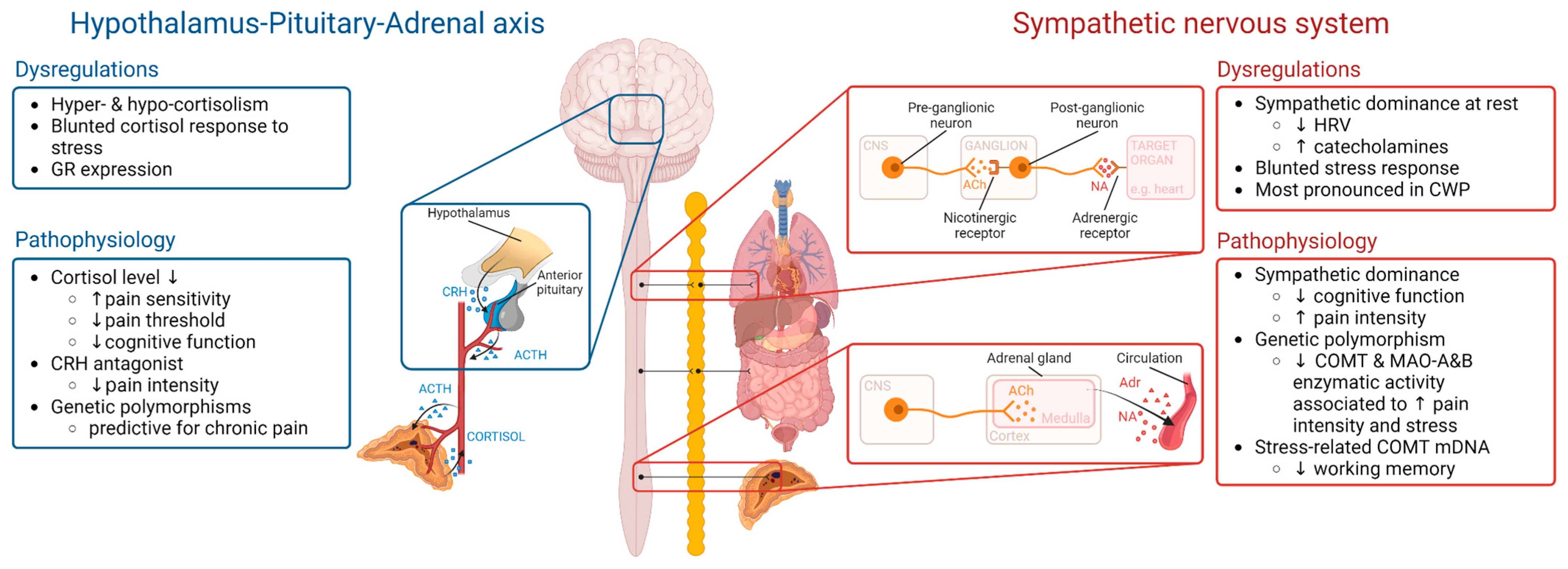{kind=link}
{kind=link}
Abstract
:1. Stress Intolerance Plays a Major Role in Chronic Widespread Pain
2. Objectives
3. Methodology
4. Two Major Stress Systems: The Autonomic Nervous System and the Hypothala-Mus-Pituitary-Adrenal Axis
5. Sympathetic and Adrenergic Activity Have a Role in Stress Intolerance
6. The HPA Axis Is Deregulated in Chronic Pain Syndromes
7. A Key Regulatory Role for Genetics and Epigenetics in Stress Intolerance
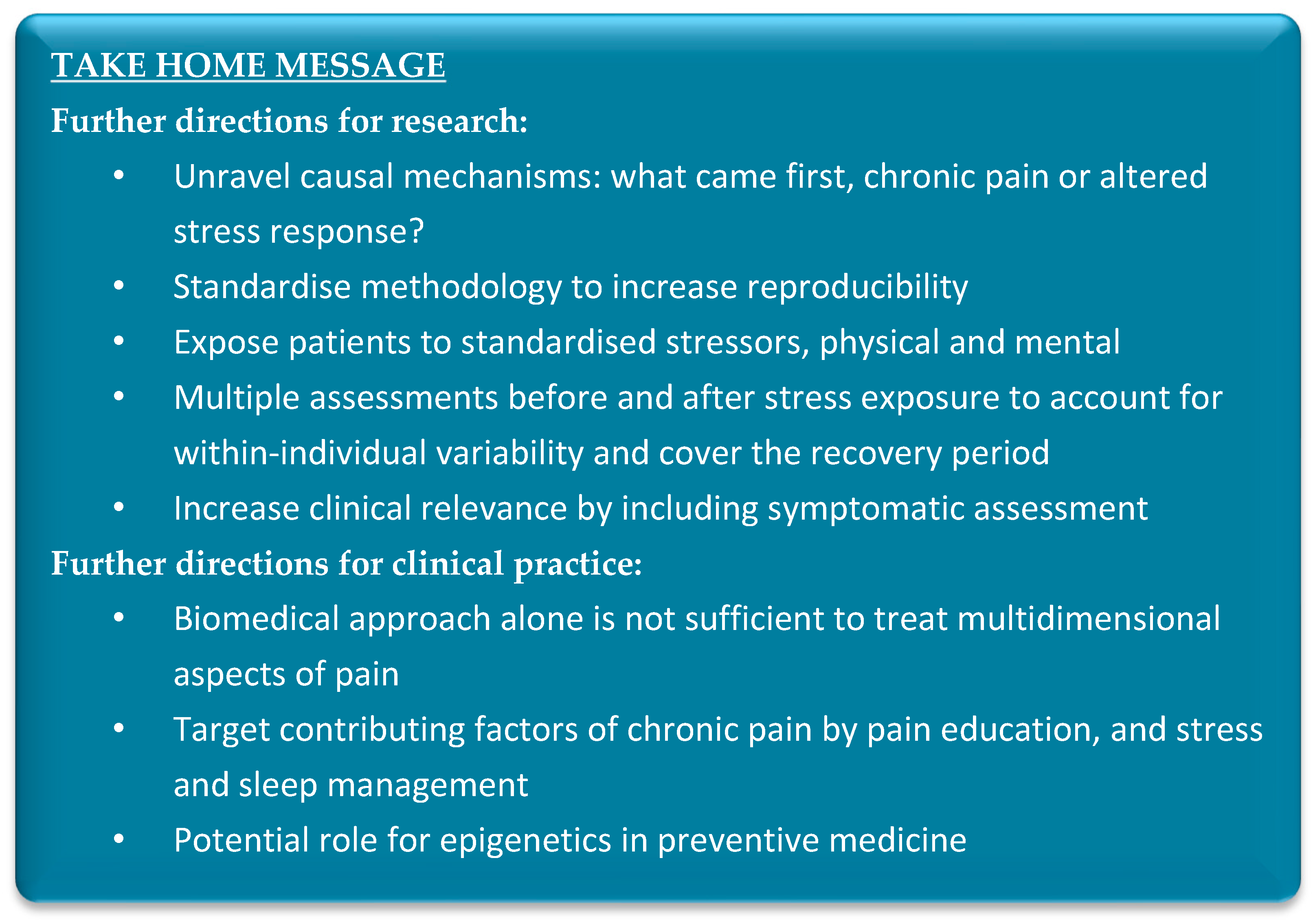
8. Future Directions for Research
9. Future Directions for Clinical Practice
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Treede, R.D.; Rief, W.; Barke, A.; Aziz, Q.; Bennett, M.I.; Benoliel, R.; Cohen, M.; Evers, S.; Finnerup, N.B.; First, M.B.; et al. A classification of chronic pain for ICD-11. Pain 2015, 156, 1003–1007. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meints, S.M.; Edwards, R.R. Evaluating psychosocial contributions to chronic pain outcomes. Prog. Neuropsychopharmacol. Biol. Psychiatry 2018, 87, 168–182. [Google Scholar] [CrossRef]
- Generaal, E.; Vogelzangs, N.; Macfarlane, G.J.; Geenen, R.; Smit, J.H.; de Geus, E.J.; Penninx, B.W.; Dekker, J. Biological stress systems, adverse life events and the onset of chronic multisite musculoskeletal pain: A 6-year cohort study. Ann. Rheum. Dis. 2016, 75, 847–854. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Stress. 2021. Available online: https://www.who.int/news-room/questions-and-answers/item/stress#:~:text=Stress%20can%20be%20defined%20as,to%20your%20overall%20well%2Dbeing (accessed on 15 January 2023).
- Selye, H.; Fortier, C. Adaptive reaction to stress. Psychosom. Med. 1950, 12, 149–157. [Google Scholar] [CrossRef]
- Fechir, M.; Breimhorst, M.; Kritzmann, S.; Geber, C.; Schlereth, T.; Baier, B.; Birklein, F. Naloxone inhibits not only stress-induced analgesia but also sympathetic activation and baroreceptor-reflex sensitivity. Eur. J. Pain. 2012, 16, 82–92. [Google Scholar] [CrossRef]
- al’Absi, M.; Nakajima, M.; Bruehl, S. Stress and pain: Modality-specific opioid mediation of stress-induced analgesia. J. Neural. Transm. 2021, 128, 1397–1407. [Google Scholar] [CrossRef] [PubMed]
- Ferdousi, M.; Finn, D.P. Chapter 4—Stress-induced modulation of pain: Role of the endogenous opioid system. In Progress in Brain Research; O’Mara, S., Ed.; Elsevier: Amsterdam, The Netherlands, 2018; Volume 239, pp. 121–177. [Google Scholar]
- Abdallah, C.G.; Geha, P. Chronic Pain and Chronic Stress: Two Sides of the Same Coin? Chronic. Stress 2017, 1, 2470547017704763. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Åkerblom, S.; Perrin, S.; Rivano Fischer, M.; McCracken, L.M. The Relationship Between Posttraumatic Stress Disorder and Chronic Pain in People Seeking Treatment for Chronic Pain: The Mediating Role of Psychological Flexibility. Clin. J. Pain 2018, 34, 487–496. [Google Scholar] [CrossRef]
- Yalcin, I.; Barrot, M. The anxiodepressive comorbidity in chronic pain. Curr. Opin. Anesthesiol. 2014, 27, 520–527. [Google Scholar] [CrossRef] [PubMed]
- Turner, A.I.; Smyth, N.; Hall, S.J.; Torres, S.J.; Hussein, M.; Jayasinghe, S.U.; Ball, K.; Clow, A.J. Psychological stress reactivity and future health and disease outcomes: A systematic review of prospective evidence. Psychoneuroendocrinology 2020, 114, 104599. [Google Scholar] [CrossRef]
- Dennis, N.L.; Larkin, M.; Derbyshire, S.W.G. ‘A giant mess’—Making sense of complexity in the accounts of people with fibromyalgia. Br. J. Health Psychol. 2013, 18, 763–781. [Google Scholar] [CrossRef]
- Alok, R.; Das, S.; Agarwal, G.; Salwahan, L.; Srivastava, R. Relationship of severity of depression, anxiety and stress with severity of fibromyalgia. Clin. Exp. Rheumatol.-Incl Suppl. 2011, 29, S70. [Google Scholar]
- Drolet, G.; Dumont, E.C.; Gosselin, I.; Kinkead, R.; Laforest, S.; Trottier, J.F. Role of endogenous opioid system in the regulation of the stress response. Prog. Neuropsychopharmacol. Biol. Psychiatry 2001, 25, 729–741. [Google Scholar] [CrossRef] [PubMed]
- Malafoglia, V.; Ilari, S.; Vitiello, L.; Tenti, M.; Balzani, E.; Muscoli, C.; Raffaeli, W.; Bonci, A. The Interplay between Chronic Pain, Opioids, and the Immune System. Neuroscientist 2022, 28, 613–627. [Google Scholar] [CrossRef]
- Morena, M.; Patel, S.; Bains, J.S.; Hill, M.N. Neurobiological Interactions Between Stress and the Endocannabinoid System. Neuropsychopharmacology 2016, 41, 80–102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zieglgänsberger, W.; Brenneisen, R.; Berthele, A.; Wotjak, C.T.; Bandelow, B.; Tölle, T.R.; Lutz, B. Chronic Pain and the Endocannabinoid System: Smart Lipids—A Novel Therapeutic Option? Med. Cannabis. Cannabinoids. 2022, 5, 61–75. [Google Scholar] [CrossRef] [PubMed]
- Kenney, M.J.; Ganta, C.K. Autonomic nervous system and immune system interactions. Compr. Physiol. 2014, 4, 1177–1200. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Godoy, L.; Rossignoli, M.; Delfino-Pereira, P.; Garcia-Cairasco, N.; de Lima Umeoka, E. A Comprehensive Overview on Stress Neurobiology: Basic Concepts and Clinical Implications. Front. Behav. Neurosci. 2018, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ulrich-Lai, Y.M.; Herman, J.P. Neural regulation of endocrine and autonomic stress responses. Nat. Rev. Neurosci. 2009, 10, 397–409. [Google Scholar] [CrossRef] [Green Version]
- Joëls, M.; Baram, T.Z. The neuro-symphony of stress. Nat. Rev. Neurosci. 2009, 10, 459–466. [Google Scholar] [CrossRef]
- Elenkov, I.; Wilder, R.; Chrousos, G.; Vizi, E. The sympathetic nerve—An integrative interface between two supersystems: The brain and the immune system. Pharmacol. Rev. 2000, 52, 595–638. [Google Scholar] [PubMed]
- Wehrwein, E.; Orer, H.; Barman, S. Overview of the Anatomy, Physiology, and Pharmacology of the Autonomic Nervous System. Compr. Physiol. 2016, 6, 1239–1278. [Google Scholar] [CrossRef] [PubMed]
- Tank, A.; Lee Wong, D. Peripheral and central effects of circulating catecholamines. Compr. Physiol. 2015, 5, 1–15. [Google Scholar] [CrossRef]
- Van Oosterwijck, J.; Marusic, U.; De Wandele, I.; Meeus, M.; Paul, L.; Lambrecht, L.; Moorkens, G.; Danneels, L.; Nijs, J. Reduced Parasympathetic Reactivation during Recovery from Exercise in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome. J. Clin. Med. 2021, 10, 4527. [Google Scholar] [CrossRef]
- Akgöz, H.; Gürkan, U.; Dayi, S.; Terzi, S.; Akbulut, T.; Torun, A.; Tayyareci, G. The relationship between beta-receptor sensitivity and nocturnal blood pressure and heart rate recovery in normotensive people. Angiology 2006, 57, 495–500. [Google Scholar] [CrossRef] [PubMed]
- Yu, B.-H.; Kang, E.-H.; Ziegler, M.G.; Mills, P.J.; Dimsdale, J.E. Mood states, sympathetic activity, and in vivo β-adrenergic receptor function in a normal population. Depress. Anxiety 2008, 25, 559–564. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baerwald, C.; Graefe, C.; Muhl, C.; Von Wichert, P.; Krause, A. Beta 2-adrenergic receptors on peripheral blood mononuclear cells in patients with rheumatic diseases. Eur. J. Clin. Investig. 1992, 22 (Suppl. S1), 42–46. [Google Scholar]
- Leite, F.; Lima, M.; Marino, F.; Cosentino, M.; Ribeiro, L. β2 Adrenoceptors are underexpressed in peripheral blood mononuclear cells and associated with a better metabolic profile in central obesity. Int. J. Med. Sci. 2017, 14, 853–861. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sawchenko, P.; Brown, E.; Chan, R.; Ericsson, A.; Li, H.; Roland, B.; Kovács, K. The paraventricular nucleus of the hypothalamus and the functional neuroanatomy of visceromotor responses to stress. Prog. Brain Res. 1996, 107, 201–222. [Google Scholar] [CrossRef]
- Vale, W.; Spiess, J.; Rivier, C.; Rivier, J. Characterization of a 41-residue ovine hypothalamic peptide that stimulates secretion of corticotropin and beta-endorphin. Science 1981, 213, 1394–1397. [Google Scholar] [CrossRef]
- Vale, W.; Rivier, C.; Yang, L.; Minick, S.; Guillemin, R. Effects of purified hypothalamic corticotropin-releasing factor and other substances on the secretion of adrenocorticotropin and beta-endorphin-like immunoactivities in vitro. Endocrinology 1978, 103, 1910–1915. [Google Scholar] [CrossRef] [PubMed]
- Spencer, R.L.; Deak, T. A users guide to HPA axis research. Physiol. Behav. 2017, 178, 43–65. [Google Scholar] [CrossRef] [PubMed]
- Mcewen, B.S.; Akil, H. Revisiting the Stress Concept: Implications for Affective Disorders. J. Neurosci. 2020, 40, 12–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lauren, T.; Jayashree, G.; Sandeep, S. Physiology, Cortisol. 2022. Available online: https://www.ncbi.nlm.nih.gov/books/NBK538239/ (accessed on 22 December 2022).
- Kadmiel, M.; Cidlowski, J.A. Glucocorticoid receptor signaling in health and disease. Trends Pharmacol. Sci. 2013, 34, 518–530. [Google Scholar] [CrossRef] [Green Version]
- Zen, M.; Canova, M.; Campana, C.; Bettio, S.; Nalotto, L.; Rampudda, M.; Ramonda, R.; Iaccarino, L.; Doria, A. The kaleidoscope of glucorticoid effects on immune system. Autoimmun. Rev. 2011, 10, 305–310. [Google Scholar] [CrossRef]
- Monaco, A.; Cattaneo, R.; Marci, M.C.; Pietropaoli, D.; Ortu, E. Central Sensitization-Based Classification for Temporomandibular Disorders: A Pathogenetic Hypothesis. Pain Res. Manag. 2017, 2017, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Van Cauwenbergh, D.; Nijs, J.; Kos, D.; Van Weijnen, L.; Struyf, F.; Meeus, M. Malfunctioning of the autonomic nervous system in patients with chronic fatigue syndrome: A systematic literature review. Eur. J. Clin. Investig. 2014, 44, 516–526. [Google Scholar] [CrossRef]
- Ortiz, R.; Gemmill, J.A.L.; Sinaii, N.; Stegmann, B.; Khachikyan, I.; Chrousos, G.; Segars, J.; Stratton, P. Hypothalamic-Pituitary-Adrenal Axis Responses in Women with Endometriosis-Related Chronic Pelvic Pain. Reprod. Sci. 2020, 27, 1839–1847. [Google Scholar] [CrossRef]
- Generaal, E.; Vogelzangs, N.; Macfarlane, G.J.; Geenen, R.; Smit, J.H.; Penninx, B.W.; Dekker, J. Reduced hypothalamic-pituitary-adrenal axis activity in chronic multi-site musculoskeletal pain: Partly masked by depressive and anxiety disorders. BMC Musculoskelet. Disord. 2014, 15, 227. [Google Scholar] [CrossRef] [Green Version]
- Koenig, J.; Falvay, D.; Clamor, A.; Wagner, J.; Jarczok, M.N.; Ellis, R.J.; Weber, C.; Thayer, J.F. Pneumogastric (Vagus) Nerve Activity Indexed by Heart Rate Variability in Chronic Pain Patients Compared to Healthy Controls: A Systematic Review and Meta-Analysis. Pain. Physician. 2016, 19, E55–E78. [Google Scholar] [CrossRef]
- Tracy, L.M.; Ioannou, L.; Baker, K.S.; Gibson, S.J.; Georgiou-Karistianis, N.; Giummarra, M.J. Meta-analytic evidence for decreased heart rate variability in chronic pain implicating parasympathetic nervous system dysregulation. Pain 2016, 157, 7–29. [Google Scholar] [CrossRef]
- Martinez-Lavin, M. Biology and therapy of fibromyalgia. Stress, the stress response system, and fibromyalgia. Arthritis Res. Ther. 2007, 9, 216. [Google Scholar] [CrossRef] [Green Version]
- El-Badawy, M.A.; El Mikkawy, D.M. Sympathetic Dysfunction in Patients with Chronic Low Back Pain and Failed Back Surgery Syndrome. Clin. J. Pain. 2016, 32, 226–231. [Google Scholar] [CrossRef]
- Koenig, J.; Loerbroks, A.; Jarczok, M.N.; Fischer, J.E.; Thayer, J.F. Chronic Pain and Heart Rate Variability in a Cross-Sectional Occupational Sample: Evidence for Impaired Vagal Control. Clin. J. Pain. 2016, 32, 218–225. [Google Scholar] [CrossRef]
- Nilsen, K.B.; Sand, T.; Westgaard, R.H.; Stovner, L.J.; White, L.R.; Leistad, R.B.; Helde, G.; Ro, M. Autonomic activation and pain in response to low-grade mental stress in fibromyalgia and shoulder/neck pain patients. Eur. J. Pain 2007, 11, 743–755. [Google Scholar] [CrossRef] [PubMed]
- Reyes del Paso, G.A.; Garrido, S.; Pulgar, Á.; Duschek, S. Autonomic cardiovascular control and responses to experimental pain stimulation in fibromyalgia syndrome. J. Psychosom. Res. 2011, 70, 125–134. [Google Scholar] [CrossRef]
- Contreras-Merino, A.M.; Davydov, D.M.; Galvez-Sánchez, C.M.; Reyes Del Paso, G.A. Blunted short-term autonomic cardiovascular reactivity to orthostatic and clinostatic challenges in fibromyalgia as an indicator of the severity of chronic pain. Int. J. Psychophysiol. 2022, 175, 61–70. [Google Scholar] [CrossRef]
- Reyes Del Paso, G.A.; Garrido, S.; Pulgar, A.; Martín-Vázquez, M.; Duschek, S. Aberrances in autonomic cardiovascular regulation in fibromyalgia syndrome and their relevance for clinical pain reports. Psychosom. Med. 2010, 72, 462–470. [Google Scholar] [CrossRef]
- López-López, A.; Matías-Pompa, B.; Fernández-Carnero, J.; Gil-Martínez, A.; Alonso-Fernández, M.; Alonso Pérez, J.L.; González Gutierrez, J.L. Blunted Pain Modulation Response to Induced Stress in Women with Fibromyalgia with and without Posttraumatic Stress Disorder Comorbidity: New Evidence of Hypo-Reactivity to Stress in Fibromyalgia? Behav. Med. 2021, 47, 311–323. [Google Scholar] [CrossRef] [PubMed]
- Matías Pompa, B.; López López, A.; Alonso Fernández, M.; Vargas Moreno, E.; González Gutiérrez, J.L. Stress-Recovery State in Fibromyalgia Patients and Healthy People. Relationship with the Cardiovascular Response to Stress in Laboratory Conditions. Int. J. Environ. Res. Public Health 2020, 17, 3138. [Google Scholar] [CrossRef] [PubMed]
- De Kooning, M.; Daenen, L.; Cras, P.; Gidron, Y.; Roussel, N.; Nijs, J. Autonomic response to pain in patients with chronic whiplash associated disorders. Pain Physician 2013, 16, E277–E285. [Google Scholar] [PubMed]
- Rus, A.; Molina, F.; Del Moral, M.L.; Ramírez-Expósito, M.J.; Martínez-Martos, J.M. Catecholamine and Indolamine Pathway: A Case-Control Study in Fibromyalgia. Biol. Res. Nurs. 2018, 20, 577–586. [Google Scholar] [CrossRef] [PubMed]
- Bote, M.E.; García, J.J.; Hinchado, M.D.; Ortega, E. Inflammatory/stress feedback dysregulation in women with fibromyalgia. Neuroimmunomodulation 2012, 19, 343–351. [Google Scholar] [CrossRef] [PubMed]
- Kaufmann, I.; Schelling, G.; Eisner, C.; Richter, H.P.; Krauseneck, T.; Vogeser, M.; Hauer, D.; Campolongo, P.; Chouker, A.; Beyer, A.; et al. Anandamide and neutrophil function in patients with fibromyalgia. Psychoneuroendocrinology 2008, 33, 676–685. [Google Scholar] [CrossRef]
- Bote, M.E.; Garcia, J.J.; Hinchado, M.D.; Ortega, E. Fibromyalgia: Anti-inflammatory and stress responses after acute moderate exercise. PLoS ONE 2013, 8, e74524. [Google Scholar] [CrossRef] [PubMed]
- Harden, R.N.; Rudin, N.J.; Bruehl, S.; Kee, W.; Parikh, D.K.; Kooch, J.; Duc, T.; Gracely, R.H. Increased systemic catecholamines in complex regional pain syndrome and relationship to psychological factors: A pilot study. Anesth. Analg. 2004, 99, 1478–1485. [Google Scholar] [CrossRef]
- Giske, L.; Røe, C.; Knardahl, S.; Vøllestad, N.K. Pain and Sympathoadrenal Responses to Dynamic Exercise in Women with the Fibromyalgia Syndrome. J. Musculoskelet. Pain 2007, 15, 25–38. [Google Scholar] [CrossRef] [Green Version]
- Adler, G.K.; Kinsley, B.T.; Hurwitz, S.; Mossey, C.J.; Goldenberg, D.L. Reduced hypothalamic-pituitary and sympathoadrenal responses to hypoglycemia in women with fibromyalgia syndrome. Am. J. Med. 1999, 106, 534–543. [Google Scholar] [CrossRef] [PubMed]
- Rizzi, M.; Radovanovic, D.; Santus, P.; Airoldi, A.; Frassanito, F.; Vanni, S.; Cristiano, A.; Masala, I.F.; Sarzi-Puttini, P. Influence of autonomic nervous system dysfunction in the genesis of sleep disorders in fibromyalgia patients. Clin. Exp. Rheumatol. 2017, 35 (Suppl. S105), 74–80. [Google Scholar] [CrossRef]
- Riva, R.; Mork, P.J.; Westgaard, R.H.; Okkenhaug Johansen, T.; Lundberg, U. Catecholamines and heart rate in female fibromyalgia patients. J. Psychosom. Res. 2012, 72, 51–57. [Google Scholar] [CrossRef]
- Kadetoff, D.; Kosek, E. Evidence of reduced sympatho-adrenal and hypothalamic-pituitary activity during static muscular work in patients with fibromyalgia. J. Rehabil. Med. 2010, 42, 765–772. [Google Scholar] [CrossRef] [Green Version]
- Forte, G.; Favieri, F.; Casagrande, M. Heart Rate Variability and Cognitive Function: A Systematic Review. Front. Neurosci. 2019, 13, 710. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Forte, G.; Troisi, G.; Pazzaglia, M.; Pascalis, V.; Casagrande, M. Heart Rate Variability and Pain: A Systematic Review. Brain. Sci. 2022, 12, 153. [Google Scholar] [CrossRef] [PubMed]
- Zamunér, A.R.; Barbic, F.; Dipaola, F.; Bulgheroni, M.; Diana, A.; Atzeni, F.; Marchi, A.; Sarzi-Puttini, P.; Porta, A.; Furlan, R. Relationship between sympathetic activity and pain intensity in fibromyalgia. Clin. Exp. Rheumatol. 2015, 33, S53–S57. [Google Scholar]
- Khasar, S.G.; Burkham, J.; Dina, O.A.; Brown, A.S.; Bogen, O.; Alessandri-Haber, N.; Green, P.G.; Reichling, D.B.; Levine, J.D. Stress induces a switch of intracellular signaling in sensory neurons in a model of generalized pain. J. Neurosci. 2008, 28, 5721–5730. [Google Scholar] [CrossRef] [Green Version]
- Khasar, S.G.; Dina, O.A.; Green, P.G.; Levine, J.D. Sound stress-induced long-term enhancement of mechanical hyperalgesia in rats is maintained by sympathoadrenal catecholamines. J. Pain. 2009, 10, 1073–1077. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Donello, J.E.; Guan, Y.; Tian, M.; Cheevers, C.V.; Alcantara, M.; Cabrera, S.; Raja, S.N.; Gil, D.W. A peripheral adrenoceptor-mediated sympathetic mechanism can transform stress-induced analgesia into hyperalgesia. Anesthesiology 2011, 114, 1403–1416. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nackley, A.G.; Tan, K.S.; Fecho, K.; Flood, P.; Diatchenko, L.; Maixner, W. Catechol-O-methyltransferase inhibition increases pain sensitivity through activation of both beta2- and beta3-adrenergic receptors. Pain 2007, 128, 199–208. [Google Scholar] [CrossRef] [Green Version]
- Oyadeyi, A.; Ajao, F.; Ibironke, G.; Afolabi, A. Acute restraint stress induces hyperalgesia via non-adrenergic mechanisms in rats. Afr. J. Biomed. Res. 2005, 8, 123–125. [Google Scholar] [CrossRef]
- Biondi, M.; Picardi, A. Psychological stress and neuroendocrine function in humans: The last two decades of research. Psychother. Psychosom. 1999, 68, 114–150. [Google Scholar] [CrossRef]
- Heuser, I.; Lammers, C. Stress and the brain. Neurobiol. Aging 2003, 24 (Suppl. S1), S69–S76. [Google Scholar] [CrossRef]
- Woda, A.; Picard, P.; Dutheil, F. Dysfunctional stress responses in chronic pain. Psychoneuroendocrinology 2016, 71, 127–135. [Google Scholar] [CrossRef] [PubMed]
- Essex, M.; Klein, M.; Cho, E.; Kalin, N. Maternal stress beginning in infancy may sensitize children to later stress exposure: Effects on cortisol and behavior. Biol. Psychiatry 2002, 52, 776–784. [Google Scholar] [CrossRef] [PubMed]
- Tosato, J.D.P.; Caria, P.H.F.; Gomes, C.A.F.D.P.; Berzin, F.; Politti, F.; Gonzalez, T.D.O.; Biasotto-Gonzalez, D.A. Correlation of stress and muscle activity of patients with different degrees of temporomandibular disorder. J. Phys. Ther. Sci. 2015, 27, 1227–1231. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.-I.; Kim, Y.-Y.; Chang, J.-Y.; Ko, J.-Y.; Kho, H.-S. Salivary cortisol, 17β-estradiol, progesterone, dehydroepiandrosterone, and α-amylase in patients with burning mouth syndrome. Oral Dis. 2012, 18, 613–620. [Google Scholar] [CrossRef]
- Tops, M.; Riese, H.; Oldehinkel, A.J.; Rijsdijk, F.V.; Ormel, J. Rejection sensitivity relates to hypocortisolism and depressed mood state in young women. Psychoneuroendocrinology 2008, 33, 551–559. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nijhof, S.; Rutten, J.; Uiterwaal, C.; Bleijenberg, G.; Kimpen, J.; Putte, E. The role of hypocortisolism in chronic fatigue syndrome. Psychoneuroendocrinology 2014, 42, 119–206. [Google Scholar] [CrossRef]
- Chang, L.; Sundaresh, S.; Elliott, J.; Anton, P.A.; Baldi, P.; Licudine, A.; Mayer, M.; Vuong, T.; Hirano, M.; Naliboff, B.D.; et al. Dysregulation of the hypothalamic-pituitary-adrenal (HPA) axis in irritable bowel syndrome. Neurogastroenterol. Motil. 2009, 21, 149–159. [Google Scholar] [CrossRef] [Green Version]
- Heim, C.; Ehlert, U.; Hanker, J.; Hellhammer, D. Abuse-related posttraumatic stress disorder and alterations of the hypothalamic-pituitary-adrenal axis in women with chronic pelvic pain. Psychosom. Med. 1998, 60, 309–318. [Google Scholar] [CrossRef]
- Bagnato, G.; Cordova, F.; Sciortino, D.; Miceli, G.; Bruno, A.; Ferrera, A.; Sangari, D.; Coppolino, G.; Muscatello, M.R.A.; Pandolfo, G.; et al. Association between cortisol levels and pain threshold in systemic sclerosis and major depression. Rheumatol. Int. 2018, 38, 433–441. [Google Scholar] [CrossRef]
- Paananen, M.; O’Sullivan, P.; Straker, L.; Beales, D.; Coenen, P.; Karppinen, J.; Pennell, C.; Smith, A. A low cortisol response to stress is associated with musculoskeletal pain combined with increased pain sensitivity in young adults: A longitudinal cohort study. Arthritis. Res. 2015, 17, 355. [Google Scholar] [CrossRef] [Green Version]
- Trevino, C.; Geier, T.; Morris, R.; Cronn, S.; deRoon-Cassini, T. Relationship Between Decreased Cortisol and Development of Chronic Pain in Traumatically Injured. J. Surg. Res. 2022, 270, 286–292. [Google Scholar] [CrossRef] [PubMed]
- Ennis, G.E.; Moffat, S.D.; Hertzog, C. The cortisol awakening response and cognition across the adult lifespan. Brain. Cogn. 2016, 105, 66–77. [Google Scholar] [CrossRef] [Green Version]
- Riva, R.; Mork, P.; Westgaard, R.; Rø, M.; Lundberg, U. Fibromyalgia syndrome is associated with hypocortisolism. Int. J. Behav. Med. 2010, 17, 223–233. [Google Scholar] [CrossRef] [PubMed]
- Torgrimson-Ojerio, B.; Ross, R.L.; Dieckmann, N.F.; Avery, S.; Bennett, R.M.; Jones, K.D.; Guarino, A.J.; Wood, L.J. Preliminary evidence of a blunted anti-inflammatory response to exhaustive exercise in fibromyalgia. J. Neuroimmunol. 2014, 277, 160–167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pereira Pernambuco, A.; De Souza Cota Carvalho, L.; Pereira Leite Schetino, L.; Cunha Polese, J.; De Souza Viana, R.; D’ Ávila Reis, D. Effects of a health education program on cytokines and cortisol levels in fibromyalgia patients: A randomized controlled trial. Adv. Rheumatol. 2018, 58. [Google Scholar] [CrossRef]
- Tak, L.; Cleare, A.; Ormel, J.; Manoharan, A.; Kok, I.; Wessely, S.; Rosmalen, J. Meta-analysis and meta-regression of hypothalamic-pituitary-adrenal axis activity in functional somatic disorders. Biol. Psychol. 2011, 87, 183–194. [Google Scholar] [CrossRef] [PubMed]
- Úbeda-D’Ocasar, E.; Jiménez Díaz-Benito, V.; Gallego-Sendarrubias, G.M.; Valera-Calero, J.A.; Vicario-Merino, Á.; Hervás-Pérez, J.P. Pain and Cortisol in Patients with Fibromyalgia: Systematic Review and Meta-Analysis. Diagnostics 2020, 10, 922. [Google Scholar] [CrossRef]
- McEwen, B.S. Physiology and Neurobiology of Stress and Adaptation: Central Role of the Brain. Physiol. Rev. 2007, 87, 873–904. [Google Scholar] [CrossRef] [Green Version]
- Coppens, E.; Kempke, S.; Van Wambeke, P.; Claes, S.; Morlion, B.; Luyten, P.; Van Oudenhove, L. Cortisol and Subjective Stress Responses to Acute Psychosocial Stress in Fibromyalgia Patients and Control Participants. Psychosom. Med. 2018, 80, 317–326. [Google Scholar] [CrossRef]
- Bale, T.; Vale, W. CRF and CRF receptors: Role in stress responsivity and other behaviors. Annu. Rev. Pharmacol. Toxicol. 2004, 44, 525–557. [Google Scholar] [CrossRef]
- Olango, W.M.; Finn, D.P. Neurobiology of Stress-Induced Hyperalgesia. In Behavioral Neurobiology of Chronic Pain; Taylor, B.K., Finn, D.P., Eds.; Springer: Berlin/Heidelberg, Germany, 2014; pp. 251–280. [Google Scholar] [CrossRef]
- Schwetz, I.; Bradesi, S.; McRoberts, J.; Sablad, M.; Miller, J.; Zhou, H.; Ohning, G.; Mayer, E. Delayed stress-induced colonic hypersensitivity in male Wistar rats: Role of neurokinin-1 and corticotropin-releasing factor-1 receptors. Am. J. Physiol. Gastrointest. Liver Physiol. 2004, 286, G683–G691. [Google Scholar] [CrossRef] [Green Version]
- Million, M.; Grigoriadis, D.; Sullivan, S.; Crowe, P.; McRoberts, J.; Zhou, H.; Saunders, P.; Maillot, C.; Mayer, E.; Taché, Y. A novel water-soluble selective CRF1 receptor antagonist, NBI 35965, blunts stress-induced visceral hyperalgesia and colonic motor function in rats. Brain Res. 2003, 985, 32–42. [Google Scholar] [CrossRef] [PubMed]
- Abdelhamid, R.E.; Kovacs, K.J.; Pasley, J.D.; Nunez, M.G.; Larson, A.A. Forced swim-induced musculoskeletal hyperalgesia is mediated by CRF2 receptors but not by TRPV1 receptors. Neuropharmacology 2013, 72, 29–37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sagami, Y. Effect of a corticotropin releasing hormone receptor antagonist on colonic sensory and motor function in patients with irritable bowel syndrome. Gut 2004, 53, 958–964. [Google Scholar] [CrossRef] [PubMed]
- Schwetz, I.; Naliboff, B.; Munakata, J.; Lembo, T.; Chang, L.; Matin, K.; Ohning, G.; Mayer, E. Anti-hyperalgesic effect of octreotide in patients with irritable bowel syndrome. Aliment. Pharmacol. Ther. 2004, 19, 123–131. [Google Scholar] [CrossRef]
- Geva, N.; Defrin, R. Opposite Effects of Stress on Pain Modulation Depend on the Magnitude of Individual Stress Response. J. Pain 2018, 19, 360–371. [Google Scholar] [CrossRef] [PubMed]
- Bouma, E.M.C.; Riese, H.; Doornbos, B.; Ormel, J.; Oldehinkel, A.J. Genetically based reduced MAOA and COMT functioning is associated with the cortisol stress response: A replication study. Mol. Psychiatry 2012, 17, 119–121. [Google Scholar] [CrossRef] [Green Version]
- Hernaus, D.; Collip, D.; Lataster, J.; Ceccarini, J.; Kenis, G.; Booij, L.; Pruessner, J.; Van Laere, K.; van Winkel, R.; van Os, J.; et al. COMT Val158Met genotype selectively alters prefrontal [18F]fallypride displacement and subjective feelings of stress in response to a psychosocial stress challenge. PLoS ONE 2013, 8, e65662. [Google Scholar] [CrossRef]
- Papaleo, F.; Crawley, J.N.; Song, J.; Lipska, B.K.; Pickel, J.; Weinberger, D.R.; Chen, J. Genetic dissection of the role of catechol-O-methyltransferase in cognition and stress reactivity in mice. J. Neurosci. 2008, 28, 8709–8723. [Google Scholar] [CrossRef] [Green Version]
- Tammimäki, A.; Männistö, P.T. Catechol-O-methyltransferase gene polymorphism and chronic human pain: A systematic review and meta-analysis. Pharm. Genom. 2012, 22, 673–691. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Antypa, N.; Giegling, I.; Calati, R.; Schneider, B.; Hartmann, A.M.; Friedl, M.; Konte, B.; Lia, L.; De Ronchi, D.; Serretti, A.; et al. MAOA and MAOB polymorphisms and anger-related traits in suicidal participants and controls. Eur. Arch. Psychiatry Clin. Neurosci. 2013, 263, 393–403. [Google Scholar] [CrossRef]
- Melas, P.A.; Wei, Y.; Wong, C.C.Y.; Sjöholm, L.K.; Åberg, E.; Mill, J.; Schalling, M.; Forsell, Y.; Lavebratt, C. Genetic and epigenetic associations of MAOA and NR3C1 with depression and childhood adversities. Int. J. Neuropsychopharmacol. 2013, 16, 1513–1528. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.; Lee, H.; Rowan, J.; Brahim, J.; Dionne, R.A. Genetic polymorphisms in monoamine neurotransmitter systems show only weak association with acute post-surgical pain in humans. Mol. Pain 2006, 2, 24. [Google Scholar] [CrossRef] [Green Version]
- Serý, O.; Hrazdilová, O.; Didden, W.; Klenerová, V.; Staif, R.; Znojil, V.; Sevcík, P. The association of monoamine oxidase B functional polymorphism with postoperative pain intensity. Neuro Endocrinol. Lett. 2006, 27, 333–337. [Google Scholar]
- Treister, R.; Pud, D.; Ebstein, R.P.; Laiba, E.; Gershon, E.; Haddad, M.; Eisenberg, E. Associations between polymorphisms in dopamine neurotransmitter pathway genes and pain response in healthy humans. Pain 2009, 147, 187–193. [Google Scholar] [CrossRef] [PubMed]
- Buhck, M.; Achenbach, J.; Wiese, B.; Tran, A.T.; Stuhrmann, M.; Jaeger, B.; Bernateck, M.; Schneider, N.; Karst, M. The interplay of chronic stress and genetic traits discriminates between patients suffering from multisomatoform disorder with pain as the leading symptom and matched controls. J. Affect. Disord. 2022, 308, 466–472. [Google Scholar] [CrossRef]
- Diatchenko, L.; Slade, G.D.; Nackley, A.G.; Bhalang, K.; Sigurdsson, A.; Belfer, I.; Goldman, D.; Xu, K.; Shabalina, S.A.; Shagin, D.; et al. Genetic basis for individual variations in pain perception and the development of a chronic pain condition. Hum. Mol. Genet. 2004, 14, 135–143. [Google Scholar] [CrossRef] [Green Version]
- Wüst, S.; Van Rossum, E.; Federenko, I.; Koper, J.; Kumsta, R.; Hellhammer, D. Common polymorphisms in the glucocorticoid receptor gene are associated with adrenocortical responses to psychosocial stress. J. Clin. Endocrinol. Metab. 2004, 89, 565–573. [Google Scholar] [CrossRef] [Green Version]
- Linnstaedt, S.D.; Riker, K.D.; Rueckeis, C.A.; Kutchko, K.M.; Lackey, L.; Mccarthy, K.R.; Tsai, Y.-H.; Parker, J.S.; Kurz, M.C.; Hendry, P.L.; et al. A Functional riboSNitch in the 3′ Untranslated Region of FKBP5 Alters MicroRNA-320a Binding Efficiency and Mediates Vulnerability to Chronic Post-Traumatic Pain. J. Neurosci. 2018, 38, 8407–8420. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Linnstaedt, S.D.; Bortsov, A.V.; Soward, A.C.; Swor, R.; Peak, D.A.; Jones, J.; Rathlev, N.; Lee, D.C.; Domeier, R.; Hendry, P.L.; et al. CRHBP polymorphisms predict chronic pain development following motor vehicle collision. Pain 2016, 157, 273–279. [Google Scholar] [CrossRef] [Green Version]
- Mogil, J.S. Pain genetics: Past, present and future. Trends. Genet. 2012, 28, 258–266. [Google Scholar] [CrossRef] [PubMed]
- Mueller, A.; Strahler, J.; Armbruster, D.; Lesch, K.-P.; Brocke, B.; Kirschbaum, C. Genetic contributions to acute autonomic stress responsiveness in children. Int. J. Psychophysiol. 2012, 83, 302–308. [Google Scholar] [CrossRef]
- Gutierrez-Arcelus, M.; Lappalainen, T.; Montgomery, S.B.; Buil, A.; Ongen, H.; Yurovsky, A.; Bryois, J.; Giger, T.; Romano, L.; Planchon, A.; et al. Passive and active DNA methylation and the interplay with genetic variation in gene regulation. Elife 2013, 2, e00523. [Google Scholar] [CrossRef]
- Polli, A.; Godderis, L.; Ghosh, M.; Ickmans, K.; Nijs, J. Epigenetic and miRNA Expression Changes in People with Pain: A Systematic Review. J. Pain 2020, 21, 763–780. [Google Scholar] [CrossRef]
- Unternaehrer, E.; Luers, P.; Mill, J.; Dempster, E.; Meyer, A.H.; Staehli, S.; Lieb, R.; Hellhammer, D.H.; Meinlschmidt, G. Dynamic changes in DNA methylation of stress-associated genes (OXTR, BDNF ) after acute psychosocial stress. Transl. Psychiatry 2012, 2, e150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wiegand, A.; Blickle, A.; Brückmann, C.; Weller, S.; Nieratschker, V.; Plewnia, C. Dynamic DNA Methylation Changes in the COMT Gene Promoter Region in Response to Mental Stress and Its Modulation by Transcranial Direct Current Stimulation. Biomolecules 2021, 11, 1726. [Google Scholar] [CrossRef] [PubMed]
- Ziegler, C.; Richter, J.; Mahr, M.; Gajewska, A.; Schiele, M.A.; Gehrmann, A.; Schmidt, B.; Lesch, K.P.; Lang, T.; Helbig-Lang, S.; et al. MAOA gene hypomethylation in panic disorder—Reversibility of an epigenetic risk pattern by psychotherapy. Transl. Psychiatry 2016, 6, e773. [Google Scholar] [CrossRef] [Green Version]
- Ursini, G.; Bollati, V.; Fazio, L.; Porcelli, A.; Iacovelli, L.; Catalani, A.; Sinibaldi, L.; Gelao, B.; Romano, R.; Rampino, A.; et al. Stress-related methylation of the catechol-O-methyltransferase Val 158 allele predicts human prefrontal cognition and activity. J. Neurosci. 2011, 31, 6692–6698. [Google Scholar] [CrossRef] [Green Version]
- Peng, H.; Zhu, Y.; Strachan, E.; Fowler, E.; Bacus, T.; Roy-Byrne, P.; Goldberg, J.; Vaccarino, V.; Zhao, J. Childhood Trauma, DNA Methylation of Stress-Related Genes, and Depression: Findings From Two Monozygotic Twin Studies. Psychosom. Med. 2018, 80, 599–608. [Google Scholar] [CrossRef]
- Xu, Q.; Jiang, M.; Gu, S.; Wang, F.; Yuan, B. Early Life Stress Induced DNA Methylation of Monoamine Oxidases Leads to Depressive-Like Behavior. Front. Cell Dev. Biol. 2020, 8, 582247. [Google Scholar] [CrossRef] [PubMed]
- Bakusic, J.; Vrieze, E.; Ghosh, M.; Bekaert, B.; Claes, S.; Godderis, L. Increased methylation of NR3C1 and SLC6A4 is associated with blunted cortisol reactivity to stress in major depression. Neurobiol. Stress 2020, 13, 100272. [Google Scholar] [CrossRef] [PubMed]
- Schartner, C.; Ziegler, C.; Schiele, M.A.; Kollert, L.; Weber, H.; Zwanzger, P.; Arolt, V.; Pauli, P.; Deckert, J.; Reif, A.; et al. CRHR1 promoter hypomethylation: An epigenetic readout of panic disorder? Eur. Neuropsychopharmacol. 2017, 27, 360–371. [Google Scholar] [CrossRef] [PubMed]
- Oberlander, T.F.; Weinberg, J.; Papsdorf, M.; Grunau, R.; Misri, S.; Devlin, A.M. Prenatal exposure to maternal depression, neonatal methylation of human glucocorticoid receptor gene (NR3C1) and infant cortisol stress responses. Epigenetics 2008, 3, 97–106. [Google Scholar] [CrossRef] [Green Version]
- Radtke, K.M.; Ruf, M.; Gunter, H.M.; Dohrmann, K.; Schauer, M.; Meyer, A.; Elbert, T. Transgenerational impact of intimate partner violence on methylation in the promoter of the glucocorticoid receptor. Transl. Psychiatry 2011, 1, e21. [Google Scholar] [CrossRef] [Green Version]
- McGowan, P.O.; Sasaki, A.; D’Alessio, A.C.; Dymov, S.; Labonté, B.; Szyf, M.; Turecki, G.; Meaney, M.J. Epigenetic regulation of the glucocorticoid receptor in human brain associates with childhood abuse. Nat. Neurosci. 2009, 12, 342–348. [Google Scholar] [CrossRef] [Green Version]
- Hawe, J.S.; Wilson, R.; Schmid, K.T.; Zhou, L.; Lakshmanan, L.N.; Lehne, B.C.; Kühnel, B.; Scott, W.R.; Wielscher, M.; Yew, Y.W.; et al. Genetic variation influencing DNA methylation provides insights into molecular mechanisms regulating genomic function. Nat. Genet. 2022, 54, 18–29. [Google Scholar] [CrossRef] [PubMed]
- Gaunt, T.R.; Shihab, H.A.; Hemani, G.; Min, J.L.; Woodward, G.; Lyttleton, O.; Zheng, J.; Duggirala, A.; McArdle, W.L.; Ho, K.; et al. Systematic identification of genetic influences on methylation across the human life course. Genome Biol. 2016, 17, 61. [Google Scholar] [CrossRef] [Green Version]
- Hannon, E.; Gorrie-Stone, T.J.; Smart, M.C.; Burrage, J.; Hughes, A.; Bao, Y.; Kumari, M.; Schalkwyk, L.C.; Mill, J. Leveraging DNA-Methylation Quantitative-Trait Loci to Characterize the Relationship between Methylomic Variation, Gene Expression, and Complex Traits. Am. J. Hum. Genet. 2018, 103, 654–665. [Google Scholar] [CrossRef] [Green Version]
- Bonder, M.J.; Luijk, R.; Zhernakova, D.V.; Moed, M.; Deelen, P.; Vermaat, M.; van Iterson, M.; van Dijk, F.; van Galen, M.; Bot, J.; et al. Disease variants alter transcription factor levels and methylation of their binding sites. Nat. Genet. 2017, 49, 131–138. [Google Scholar] [CrossRef] [Green Version]
- Bonder, M.J.; Kasela, S.; Kals, M.; Tamm, R.; Lokk, K.; Barragan, I.; Buurman, W.A.; Deelen, P.; Greve, J.-W.; Ivanov, M.; et al. Genetic and epigenetic regulation of gene expression in fetal and adult human livers. BMC Genom. 2014, 15, 860. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Polli, A.; Hendrix, J.; Ickmans, K.; Bakusic, J.; Ghosh, M.; Monteyne, D.; Velkeniers, B.; Bekaert, B.; Nijs, J.; Godderis, L. Genetic and epigenetic regulation of Catechol-O-methyltransferase in relation to inflammation in chronic fatigue syndrome and Fibromyalgia. J. Transl. Med. 2022, 20, 487. [Google Scholar] [CrossRef] [PubMed]
- Schreiner, F.; El-Maarri, O.; Gohlke, B.; Stutte, S.; Nuesgen, N.; Mattheisen, M.; Fimmers, R.; Bartmann, P.; Oldenburg, J.; Woelfle, J. Association of COMT genotypes with S-COMT promoter methylation in growth-discordant monozygotic twins and healthy adults. BMC Med. Genet. 2011, 12, 115. [Google Scholar] [CrossRef] [Green Version]
- Crofford, L.J. Adverse effects of chronic opioid therapy for chronic musculoskeletal pain. Nat. Rev. Rheumatol. 2010, 6, 191–197. [Google Scholar] [CrossRef]
- Crofford, L.J. Chronic Pain: Where the Body Meets the Brain. Trans. Am. Clin. Clim. Assoc. 2015, 126, 167–183. [Google Scholar]
- Michaelides, A.; Zis, P. Depression, anxiety and acute pain: Links and management challenges. Postgrad Med. 2019, 131, 438–444. [Google Scholar] [CrossRef]
- Marshall, P.W.M.; Schabrun, S.; Knox, M.F. Physical activity and the mediating effect of fear, depression, anxiety, and catastrophizing on pain related disability in people with chronic low back pain. PLoS ONE 2017, 12, e0180788. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Louw, A.; Diener, I.; Butler, D.S.; Puentedura, E.J. The Effect of Neuroscience Education on Pain, Disability, Anxiety, and Stress in Chronic Musculoskeletal Pain. Arch. Phys. Med. Rehabil. 2011, 92, 2041–2056. [Google Scholar] [CrossRef] [PubMed]
- Watson, J.A.; Ryan, C.G.; Cooper, L.; Ellington, D.; Whittle, R.; Lavender, M.; Dixon, J.; Atkinson, G.; Cooper, K.; Martin, D.J. Pain Neuroscience Education for Adults With Chronic Musculoskeletal Pain: A Mixed-Methods Systematic Review and Meta-Analysis. J. Pain. 2019, 20, 1140.e1–1140.e22. [Google Scholar] [CrossRef] [PubMed]
- Tegner, H.; Frederiksen, P.; Esbensen, B.A.; Juhl, C. Neurophysiological Pain Education for Patients With Chronic Low Back Pain: A Systematic Review and Meta-Analysis. Clin. J. Pain. 2018, 34, 778–786. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Keeffe, M.; O’Sullivan, P.; Purtill, H.; Bargary, N.; O’Sullivan, K. Cognitive functional therapy compared with a group-based exercise and education intervention for chronic low back pain: A multicentre randomised controlled trial (RCT). Br. J. Sport. Med. 2020, 54, 782–789. [Google Scholar] [CrossRef] [PubMed]
- Veehof, M.M.; Trompetter, H.R.; Bohlmeijer, E.T.; Schreurs, K.M. Acceptance- and mindfulness-based interventions for the treatment of chronic pain: A meta-analytic review. Cogn. Behav. 2016, 45, 5–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soundararajan, K.; Prem, V.; Kishen, T.J. The effectiveness of mindfulness-based stress reduction intervention on physical function in individuals with chronic low back pain: Systematic review and meta-analysis of randomized controlled trials. Complement. Clin. Pr. 2022, 49, 101623. [Google Scholar] [CrossRef]
- Haugmark, T.; Hagen, K.B.; Smedslund, G.; Zangi, H.A. Mindfulness- and acceptance-based interventions for patients with fibromyalgia—A systematic review and meta-analyses. PLoS ONE 2019, 14, e0221897. [Google Scholar] [CrossRef] [PubMed]
- Hajihasani, A.; Rouhani, M.; Salavati, M.; Hedayati, R.; Kahlaee, A.H. The Influence of Cognitive Behavioral Therapy on Pain, Quality of Life, and Depression in Patients Receiving Physical Therapy for Chronic Low Back Pain: A Systematic Review. Pm. R. 2019, 11, 167–176. [Google Scholar] [CrossRef] [PubMed]
- Nijs, J.; D’Hondt, E.; Clarys, P.; Deliens, T.; Polli, A.; Malfliet, A.; Coppieters, I.; Willaert, W.; Tumkaya Yilmaz, S.; Elma, Ö.; et al. Lifestyle and Chronic Pain across the Lifespan: An Inconvenient Truth? Pm. R. 2020, 12, 410–419. [Google Scholar] [CrossRef]
- Denis, D.; Akhtar, R.; Holding, B.C.; Murray, C.; Panatti, J.; Claridge, G.; Sadeh, A.; Barclay, N.L.; O’Leary, R.; Maughan, B.; et al. Externalizing Behaviors and Callous-Unemotional Traits: Different Associations with Sleep Quality. Sleep 2017, 40. [Google Scholar] [CrossRef] [Green Version]
- Nakamura, M.; Nagamine, T. Neuroendocrine, Autonomic, and Metabolic Responses to an Orexin Antagonist, Suvorexant, in Psychiatric Patients with Insomnia. Innov. Clin. Neurosci. 2017, 14, 30–37. [Google Scholar]
- Nijs, J.; Loggia, M.L.; Polli, A.; Moens, M.; Huysmans, E.; Goudman, L.; Meeus, M.; Vanderweeën, L.; Ickmans, K.; Clauw, D. Sleep disturbances and severe stress as glial activators: Key targets for treating central sensitization in chronic pain patients? Expert Opin. Targets 2017, 21, 817–826. [Google Scholar] [CrossRef]
- Haack, M.; Simpson, N.; Sethna, N.; Kaur, S.; Mullington, J. Sleep deficiency and chronic pain: Potential underlying mechanisms and clinical implications. Neuropsychopharmacology 2020, 45, 205–216. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, G.M., Jr.; Toffoli, L.V.; Manfredo, M.H.; Francis-Oliveira, J.; Silva, A.S.; Raquel, H.A.; Martins-Pinge, M.C.; Moreira, E.G.; Fernandes, K.B.; Pelosi, G.G.; et al. Acute stress affects the global DNA methylation profile in rat brain: Modulation by physical exercise. Behav. Brain Res. 2015, 279, 123–128. [Google Scholar] [CrossRef] [PubMed]
- Sales, A.J.; Joca, S.R.L. Antidepressant administration modulates stress-induced DNA methylation and DNA methyltransferase expression in rat prefrontal cortex and hippocampus. Behav. Brain Res. 2018, 343, 8–15. [Google Scholar] [CrossRef] [PubMed]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wyns, A.; Hendrix, J.; Lahousse, A.; De Bruyne, E.; Nijs, J.; Godderis, L.; Polli, A. The Biology of Stress Intolerance in Patients with Chronic Pain—State of the Art and Future Directions. J. Clin. Med. 2023, 12, 2245. https://doi.org/10.3390/jcm12062245
Wyns A, Hendrix J, Lahousse A, De Bruyne E, Nijs J, Godderis L, Polli A. The Biology of Stress Intolerance in Patients with Chronic Pain—State of the Art and Future Directions. Journal of Clinical Medicine. 2023; 12(6):2245. https://doi.org/10.3390/jcm12062245
Chicago/Turabian StyleWyns, Arne, Jolien Hendrix, Astrid Lahousse, Elke De Bruyne, Jo Nijs, Lode Godderis, and Andrea Polli. 2023. "The Biology of Stress Intolerance in Patients with Chronic Pain—State of the Art and Future Directions" Journal of Clinical Medicine 12, no. 6: 2245. https://doi.org/10.3390/jcm12062245