
Inferior Vena Cava Ultrasonography for Volume Status Evaluation: An Intriguing Promise Never Fulfilled


Abstract
:1. Introduction
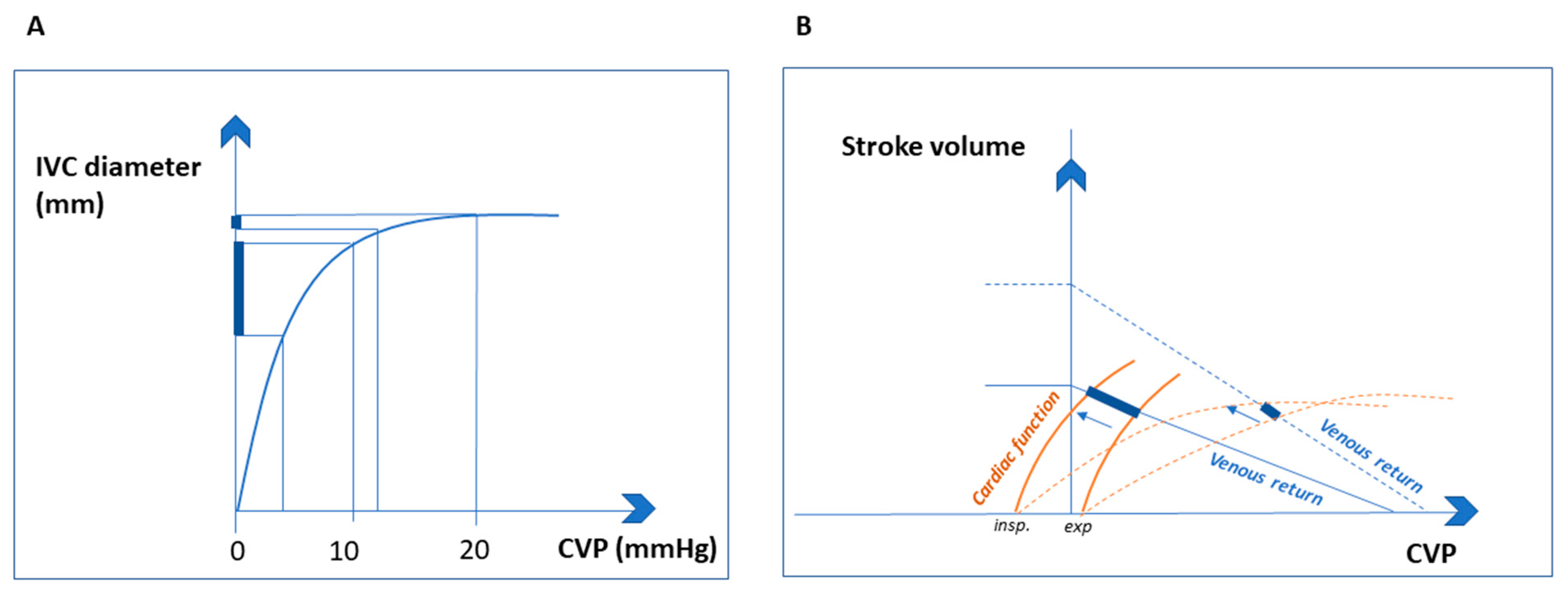
2. Pathophysiological Assumptions
2.1. Intrathoracic Pressure
2.2. Intra-Abdominal Pressure
2.3. Cardiac Function
3. Anatomical Variations of Inferior Vena Cava and Their Clinical Significance
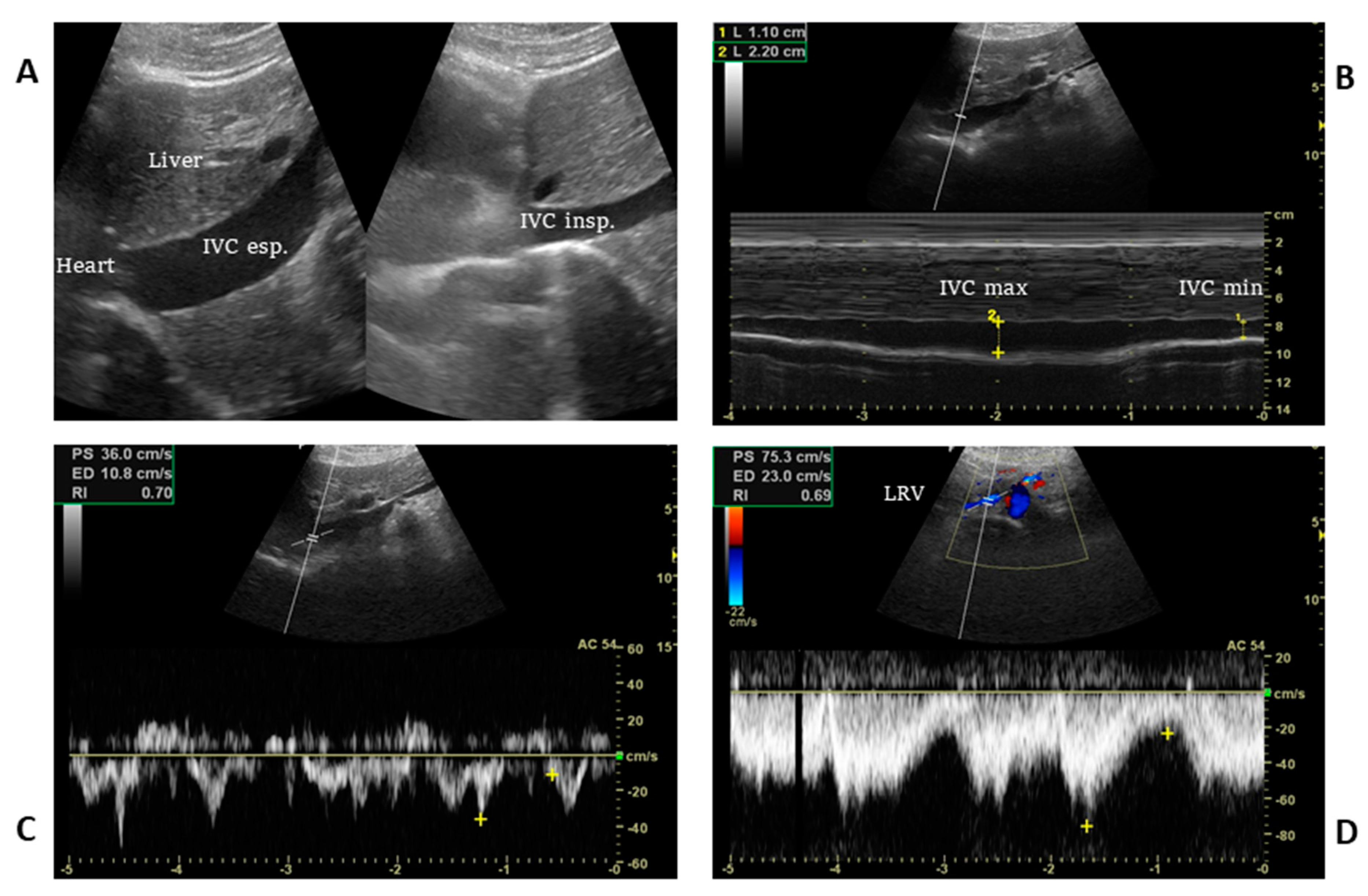
4. Ultrasound Technique, Static and Dynamic IVC Indexes
5. Evidence for Volaemic Status Evaluation with IVC Ultrasonography
5.1. Volaemic Status Evaluation in Spontaneously Breathing Patient
5.2. Volaemic Status Evaluation in Mechanically Ventilated Patients
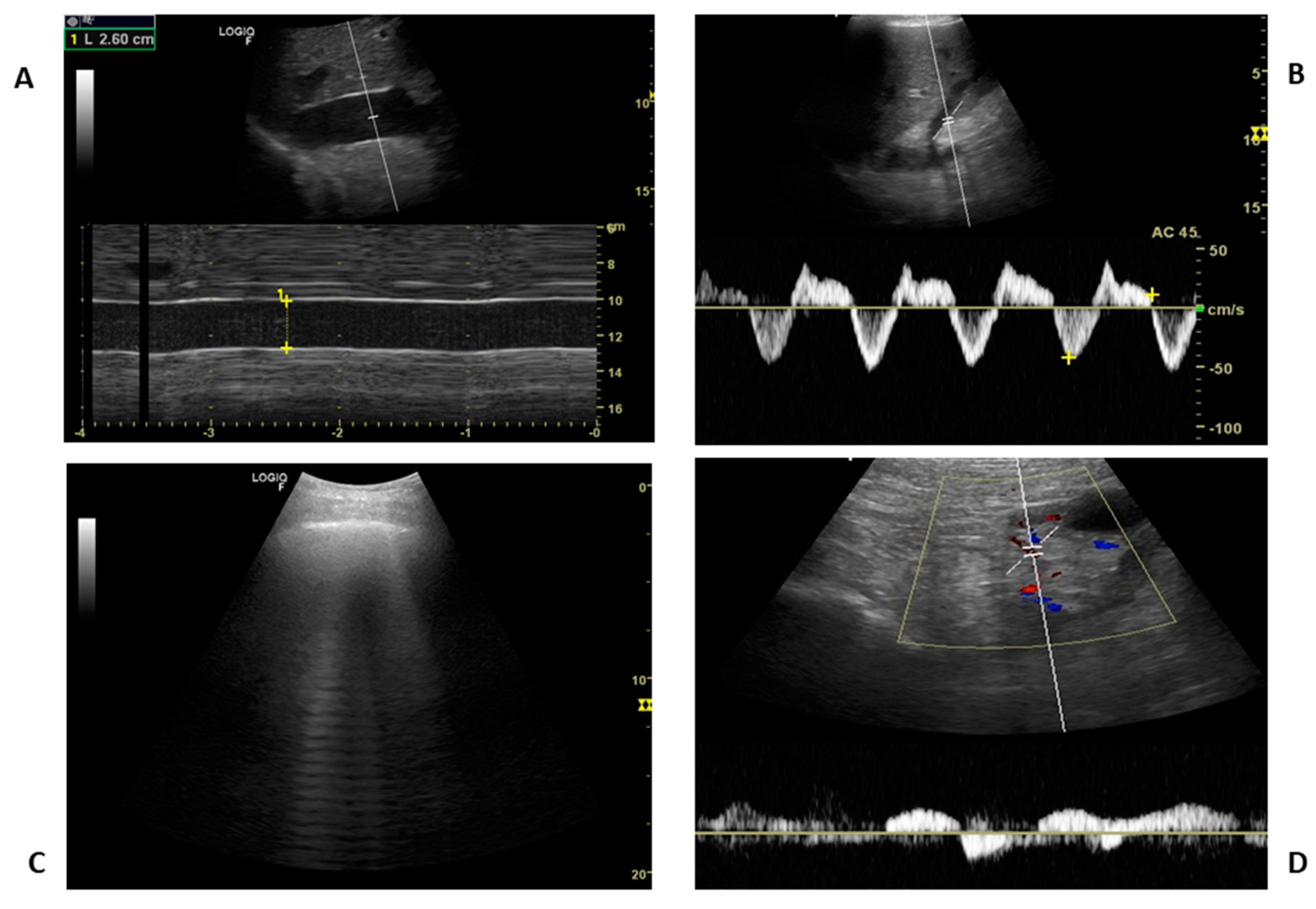
6. Pitfalls That May Lead to Misinterpretation of Volume Status
7. IVC Ultrasonography: Current Knowledge and Future Directions
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Marik, P.E.; Linde-Zwirble, W.T.; Bittner, E.A.; Sahatjian, J.; Hansell, D. Fluid Administration in Severe Sepsis and Septic Shock, Patterns and Outcomes: An Analysis of a Large National Database. Intensive Care Med. 2017, 43, 625–632. [Google Scholar] [CrossRef] [PubMed]
- Damman, K.; van Deursen, V.M.; Navis, G.; Voors, A.A.; van Veldhuisen, D.J.; Hillege, H.L. Increased Central Venous Pressure Is Associated with Impaired Renal Function and Mortality in a Broad Spectrum of Patients with Cardiovascular Disease. J. Am. Coll. Cardiol. 2009, 53, 582–588. [Google Scholar] [CrossRef] [Green Version]
- Jeffrey, R.B.; Federle, M.P. The Collapsed Inferior Vena Cava: CT Evidence of Hypovolemia. AJR Am. J. Roentgenol. 1988, 150, 431–432. [Google Scholar] [CrossRef] [PubMed]
- Nakao, S.; Come, P.C.; McKay, R.G.; Ransil, B.J. Effects of Positional Changes on Inferior Vena Caval Size and Dynamics and Correlations with Right-Sided Cardiac Pressure. Am. J. Cardiol. 1987, 59, 125–132. [Google Scholar] [CrossRef] [PubMed]
- Wexler, L.; Bergel, D.H.; Gabe, I.T.; Makin, G.S.; Mills, C.J. Velocity of Blood Flow in Normal Human Venae Cavae. Circ. Res. 1968, 23, 349–359. [Google Scholar] [CrossRef] [Green Version]
- Kadoya, Y.; Miyati, T.; Kobayashi, S.; Ohno, N.; Gabata, T. Evaluation of Gravity Effect on Inferior Vena Cava and Abdominal Aortic Flow Using Multi-Posture MRI. Acta Radiol. 2021, 62, 1122–1128. [Google Scholar] [CrossRef]
- Lloyd, T.C. Effect of Inspiration on Inferior Vena Caval Blood Flow in Dogs. J. Appl. Physiol. Respir. Environ. Exerc. Physiol. 1983, 55, 1701–1708. [Google Scholar] [CrossRef]
- Fessler, H.E.; Brower, R.G.; Shapiro, E.P.; Permutt, S. Effects of Positive End-Expiratory Pressure and Body Position on Pressure in the Thoracic Great Veins. Am. Rev. Respir. Dis. 1993, 148, 1657–1664. [Google Scholar] [CrossRef] [PubMed]
- Bodson, L.; Vieillard-Baron, A. Respiratory Variation in Inferior Vena Cava Diameter: Surrogate of Central Venous Pressure or Parameter of Fluid Responsiveness? Let the Physiology Reply. Crit. Care 2012, 16, 181. [Google Scholar] [CrossRef] [Green Version]
- Takata, M.; Wise, R.A.; Robotham, J.L. Effects of Abdominal Pressure on Venous Return: Abdominal Vascular Zone Conditions. J. Appl. Physiol. (1985) 1990, 69, 1961–1972. [Google Scholar] [CrossRef] [PubMed]
- Takata, M.; Robotham, J.L. Effects of Inspiratory Diaphragmatic Descent on Inferior Vena Caval Venous Return. J. Appl. Physiol. (1985) 1992, 72, 597–607. [Google Scholar] [CrossRef]
- Dagar, G.; Taneja, A.; Nanchal, R.S. Abdominal Circulatory Interactions. Crit. Care Clin. 2016, 32, 265–277. [Google Scholar] [CrossRef]
- Gullace, G.; Savoia, M.T. Echocardiographic Assessment of the Inferior Vena Cava Wall Motion for Studies of Right Heart Dynamics and Function. Clin. Cardiol. 1984, 7, 393–404. [Google Scholar] [CrossRef]
- Schmidt, G.A. Rebuttal from Dr Schmidt. Chest 2017, 151, 536–537. [Google Scholar] [CrossRef] [Green Version]
- Barbier, C.; Loubières, Y.; Schmit, C.; Hayon, J.; Ricôme, J.-L.; Jardin, F.; Vieillard-Baron, A. Respiratory Changes in Inferior Vena Cava Diameter Are Helpful in Predicting Fluid Responsiveness in Ventilated Septic Patients. Intensive Care Med. 2004, 30, 1740–1746. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Labropoulos, N.; Blake, A.M.; Desai, K. Prevalence of Inferior Vena Cava Anomalies and Their Significance and Impact in Clinical Practice. Eur. J. Vasc. Endovasc. Surg. 2022, 64, 388–394. [Google Scholar] [CrossRef] [PubMed]
- Bass, J.E.; Redwine, M.D.; Kramer, L.A.; Huynh, P.T.; Harris, J.H., Jr. Spectrum of congenital anomalies of the inferior vena cava: Cross-sectional imaging findings. Radiographics 2000, 20, 639–652. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, S.J.; Lee, J.; Hall, J.; Sutherland, T.R. The inferior vena cava: Anatomical variants and acquired pathologies. Insights Imaging 2021, 12, 123. [Google Scholar] [CrossRef]
- Li, W.R.; Feng, H.; Jin, L.; Chen, X.M.; Zhang, Z.W. Duplication of the inferior vena cava: A case series. J. Int. Med. Res. 2022, 50, 3000605221100771. [Google Scholar] [CrossRef] [PubMed]
- Wallace, D.J.; Allison, M.; Stone, M.B. Inferior Vena Cava Percentage Collapse during Respiration Is Affected by the Sampling Location: An Ultrasound Study in Healthy Volunteers. Acad. Emerg. Med. 2010, 17, 96–99. [Google Scholar] [CrossRef]
- Denault, A.Y.; Langevin, S.; Lessard, M.R.; Courval, J.F.; Desjardins, G. Transthoracic Echocardiographic Evaluation of the Heart and Great Vessels. Can. J. Anaesth. 2018, 65, 449–472. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Valk, S.; Olgers, T.J.; Holman, M.; Ismael, F.; Ligtenberg, J.J.M.; Ter Maaten, J.C. The Caval Index: An Adequate Non-Invasive Ultrasound Parameter to Predict Fluid Responsiveness in the Emergency Department? BMC Anesthesiol. 2014, 14, 114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheriex, E.C.; Leunissen, K.M.; Janssen, J.H.; Mooy, J.M.; van Hooff, J.P. Echography of the Inferior Vena Cava Is a Simple and Reliable Tool for Estimation of “dry Weight” in Haemodialysis Patients. Nephrol. Dial. Transplant. 1989, 4, 563–568. [Google Scholar] [PubMed]
- Millington, S.J. Ultrasound Assessment of the Inferior Vena Cava for Fluid Responsiveness: Easy, Fun, but Unlikely to Be Helpful. Can. J. Anaesth. 2019, 66, 633–638. [Google Scholar] [CrossRef] [Green Version]
- Kircher, B.J.; Himelman, R.B.; Schiller, N.B. Noninvasive Estimation of Right Atrial Pressure from the Inspiratory Collapse of the Inferior Vena Cava. Am. J. Cardiol. 1990, 66, 493–496. [Google Scholar] [CrossRef]
- Feissel, M.; Michard, F.; Faller, J.-P.; Teboul, J.-L. The Respiratory Variation in Inferior Vena Cava Diameter as a Guide to Fluid Therapy. Intensive Care Med. 2004, 30, 1834–1837. [Google Scholar] [CrossRef]
- Yao, B.; Liu, J.-Y.; Sun, Y.-B.; Zhao, Y.-X.; Li, L. The Value of the Inferior Vena Cava Area Distensibility Index and Its Diameter Ratio for Predicting Fluid Responsiveness in Mechanically Ventilated Patients. Shock 2019, 52, 37–42. [Google Scholar] [CrossRef]
- Di Nicolò, P.; Zanoli, L.; Figuera, M.; Granata, A. Study Group of Ultrasonography of the Italian Society of Nephrology An Unusual Cause of Lumbar Pain after Physical Exercise: Caval Vein Duplicity and Its Detection by Ultrasound. J. Ultrasound 2016, 19, 289–293. [Google Scholar] [CrossRef] [Green Version]
- Ranjan, R.; Mostafavi Toroghi, H.; Pressman, G.S.; Schiller, N.B. Doppler Recognition of Low or Normal Central Venous Pressure from Continuous Flow from Inferior Vena Cava into Right Atrium. Am. J. Cardiol. 2019, 124, 448–452. [Google Scholar] [CrossRef] [PubMed]
- Long, E.; Oakley, E.; Duke, T.; Babl, F.E. Paediatric Research in Emergency Departments International Collaborative (PREDICT) Does Respiratory Variation in Inferior Vena Cava Diameter Predict Fluid Responsiveness: A Systematic Review and Meta-Analysis. Shock 2017, 47, 550–559. [Google Scholar] [CrossRef]
- Blehar, D.J.; Resop, D.; Chin, B.; Dayno, M.; Gaspari, R. Inferior Vena Cava Displacement during Respirophasic Ultrasound Imaging. Crit. Ultrasound J. 2012, 4, 18. [Google Scholar] [CrossRef] [Green Version]
- Beigel, R.; Cercek, B.; Luo, H.; Siegel, R.J. Noninvasive Evaluation of Right Atrial Pressure. J. Am. Soc. Echocardiogr. 2013, 26, 1033–1042. [Google Scholar] [CrossRef] [PubMed]
- Ciozda, W.; Kedan, I.; Kehl, D.W.; Zimmer, R.; Khandwalla, R.; Kimchi, A. The Efficacy of Sonographic Measurement of Inferior Vena Cava Diameter as an Estimate of Central Venous Pressure. Cardiovasc Ultrasound 2016, 14, 33. [Google Scholar] [CrossRef] [Green Version]
- Moreno, F.L.; Hagan, A.D.; Holmen, J.R.; Pryor, T.A.; Strickland, R.D.; Castle, C.H. Evaluation of Size and Dynamics of the Inferior Vena Cava as an Index of Right-Sided Cardiac Function. Am. J. Cardiol. 1984, 53, 579–585. [Google Scholar] [CrossRef] [PubMed]
- Lang, R.M.; Bierig, M.; Devereux, R.B.; Flachskampf, F.A.; Foster, E.; Pellikka, P.A.; Picard, M.H.; Roman, M.J.; Seward, J.; Shanewise, J.S.; et al. Recommendations for Chamber Quantification: A Report from the American Society of Echocardiography’s Guidelines and Standards Committee and the Chamber Quantification Writing Group, Developed in Conjunction with the European Association of Echocardiography, a Branch of the European Society of Cardiology. J. Am. Soc. Echocardiogr. 2005, 18, 1440–1463. [Google Scholar] [CrossRef] [PubMed]
- Brennan, J.M.; Blair, J.E.; Goonewardena, S.; Ronan, A.; Shah, D.; Vasaiwala, S.; Kirkpatrick, J.N.; Spencer, K.T. Reappraisal of the Use of Inferior Vena Cava for Estimating Right Atrial Pressure. J. Am. Soc. Echocardiogr. 2007, 20, 857–861. [Google Scholar] [CrossRef] [PubMed]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for Cardiac Chamber Quantification by Echocardiography in Adults: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2015, 28, 1–39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taniguchi, T.; Ohtani, T.; Nakatani, S.; Hayashi, K.; Yamaguchi, O.; Komuro, I.; Sakata, Y. Impact of Body Size on Inferior Vena Cava Parameters for Estimating Right Atrial Pressure: A Need for Standardization? J. Am. Soc. Echocardiogr. 2015, 28, 1420–1427. [Google Scholar] [CrossRef] [PubMed]
- Guiotto, G.; Masarone, M.; Paladino, F.; Ruggiero, E.; Scott, S.; Verde, S.; Schiraldi, F. Inferior Vena Cava Collapsibility to Guide Fluid Removal in Slow Continuous Ultrafiltration: A Pilot Study. Intensive Care Med. 2010, 36, 692–696. [Google Scholar] [CrossRef] [PubMed]
- Lyon, M.; Blaivas, M.; Brannam, L. Sonographic Measurement of the Inferior Vena Cava as a Marker of Blood Loss. Am. J. Emerg. Med. 2005, 23, 45–50. [Google Scholar] [CrossRef] [PubMed]
- Osman, D.; Ridel, C.; Ray, P.; Monnet, X.; Anguel, N.; Richard, C.; Teboul, J.-L. Cardiac Filling Pressures Are Not Appropriate to Predict Hemodynamic Response to Volume Challenge. Crit. Care Med. 2007, 35, 64–68. [Google Scholar] [CrossRef] [PubMed]
- Airapetian, N.; Maizel, J.; Alyamani, O.; Mahjoub, Y.; Lorne, E.; Levrard, M.; Ammenouche, N.; Seydi, A.; Tinturier, F.; Lobjoie, E.; et al. Does Inferior Vena Cava Respiratory Variability Predict Fluid Responsiveness in Spontaneously Breathing Patients? Crit. Care 2015, 19, 400. [Google Scholar] [CrossRef] [Green Version]
- Lanspa, M.J.; Grissom, C.K.; Hirshberg, E.L.; Jones, J.P.; Brown, S.M. Applying Dynamic Parameters to Predict Hemodynamic Response to Volume Expansion in Spontaneously Breathing Patients with Septic Shock. Shock 2013, 39, 155–160. [Google Scholar] [CrossRef] [Green Version]
- Bortolotti, P.; Colling, D.; Preau, S. Inferior Vena Cava Respiratory Variations: A Useful Tool at Bedside to Guide Fluid Therapy in Spontaneously Breathing Patients. Shock 2018, 49, 235–236. [Google Scholar] [CrossRef] [PubMed]
- Vignon, P.; Repessé, X.; Bégot, E.; Léger, J.; Jacob, C.; Bouferrache, K.; Slama, M.; Prat, G.; Vieillard-Baron, A. Comparison of Echocardiographic Indices Used to Predict Fluid Responsiveness in Ventilated Patients. Am. J. Respir. Crit. Care Med. 2017, 195, 1022–1032. [Google Scholar] [CrossRef] [PubMed]
- Byon, H.-J.; Lim, C.-W.; Lee, J.-H.; Park, Y.-H.; Kim, H.-S.; Kim, C.-S.; Kim, J.-T. Prediction of Fluid Responsiveness in Mechanically Ventilated Children Undergoing Neurosurgery. Br. J. Anaesth. 2013, 110, 586–591. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, D.Y.; Kwak, H.J.; Park, H.Y.; Kim, Y.B.; Choi, C.H.; Lee, J.Y. Respiratory Variation in Aortic Blood Flow Velocity as a Predictor of Fluid Responsiveness in Children after Repair of Ventricular Septal Defect. Pediatr. Cardiol. 2010, 31, 1166–1170. [Google Scholar] [CrossRef] [PubMed]
- Weber, T.; Wagner, T.; Neumann, K.; Deusch, E. Low Predictability of Three Different Noninvasive Methods to Determine Fluid Responsiveness in Critically Ill Children. Pediatr. Crit. Care Med. 2015, 16, e89–e94. [Google Scholar] [CrossRef] [PubMed]
- Muller, L.; Bobbia, X.; Toumi, M.; Louart, G.; Molinari, N.; Ragonnet, B.; Quintard, H.; Leone, M.; Zoric, L.; Lefrant, J.Y.; et al. Respiratory Variations of Inferior Vena Cava Diameter to Predict Fluid Responsiveness in Spontaneously Breathing Patients with Acute Circulatory Failure: Need for a Cautious Use. Crit. Care 2012, 16, R188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Preau, S.; Bortolotti, P.; Colling, D.; Dewavrin, F.; Colas, V.; Voisin, B.; Onimus, T.; Drumez, E.; Durocher, A.; Redheuil, A.; et al. Diagnostic Accuracy of the Inferior Vena Cava Collapsibility to Predict Fluid Responsiveness in Spontaneously Breathing Patients with Sepsis and Acute Circulatory Failure. Crit. Care Med. 2017, 45, e290–e297. [Google Scholar] [CrossRef]
- Corl, K.A.; George, N.R.; Romanoff, J.; Levinson, A.T.; Chheng, D.B.; Merchant, R.C.; Levy, M.M.; Napoli, A.M. Inferior Vena Cava Collapsibility Detects Fluid Responsiveness among Spontaneously Breathing Critically-Ill Patients. J. Crit. Care 2017, 41, 130–137. [Google Scholar] [CrossRef] [PubMed]
- Doucet, J.J.; Ferrada, P.; Murthi, S.; Nirula, R.; Edwards, S.; Cantrell, E.; Han, J.; Haase, D.; Singleton, A.; Birkas, Y.; et al. Ultrasonographic Inferior Vena Cava Diameter Response to Trauma Resuscitation after 1 Hour Predicts 24-Hour Fluid Requirement. J. Trauma Acute Care Surg. 2020, 88, 70–79. [Google Scholar] [CrossRef] [PubMed]
- Machare-Delgado, E.; Decaro, M.; Marik, P.E. Inferior Vena Cava Variation Compared to Pulse Contour Analysis as Predictors of Fluid Responsiveness: A Prospective Cohort Study. J. Intensive Care Med. 2011, 26, 116–124. [Google Scholar] [CrossRef] [PubMed]
- Charbonneau, H.; Riu, B.; Faron, M.; Mari, A.; Kurrek, M.M.; Ruiz, J.; Geeraerts, T.; Fourcade, O.; Genestal, M.; Silva, S. Predicting Preload Responsiveness Using Simultaneous Recordings of Inferior and Superior Vena Cavae Diameters. Crit. Care 2014, 18, 473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Theerawit, P.; Morasert, T.; Sutherasan, Y. Inferior Vena Cava Diameter Variation Compared with Pulse Pressure Variation as Predictors of Fluid Responsiveness in Patients with Sepsis. J. Crit. Care 2016, 36, 246–251. [Google Scholar] [CrossRef] [PubMed]
- Lu, N.; Xi, X.; Jiang, L.; Yang, D.; Yin, K. Exploring the Best Predictors of Fluid Responsiveness in Patients with Septic Shock. Am. J. Emerg. Med. 2017, 35, 1258–1261. [Google Scholar] [CrossRef]
- Zhang, X.; Feng, J.; Zhu, P.; Luan, H.; Wu, Y.; Zhao, Z. Ultrasonographic Measurements of the Inferior Vena Cava Variation as a Predictor of Fluid Responsiveness in Patients Undergoing Anesthesia for Surgery. J. Surg. Res. 2016, 204, 118–122. [Google Scholar] [CrossRef]
- Sobczyk, D.; Nycz, K.; Andruszkiewicz, P. Bedside Ultrasonographic Measurement of the Inferior Vena Cava Fails to Predict Fluid Responsiveness in the First 6 Hours after Cardiac Surgery: A Prospective Case Series Observational Study. J. Cardiothorac. Vasc. Anesth. 2015, 29, 663–669. [Google Scholar] [CrossRef] [PubMed]
- Sobczyk, D.; Nycz, K.; Andruszkiewicz, P.; Wierzbicki, K.; Stapor, M. Ultrasonographic Caval Indices Do Not Significantly Contribute to Predicting Fluid Responsiveness Immediately after Coronary Artery Bypass Grafting When Compared to Passive Leg Raising. Cardiovasc. Ultrasound 2016, 14, 23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moretti, R.; Pizzi, B. Inferior Vena Cava Distensibility as a Predictor of Fluid Responsiveness in Patients with Subarachnoid Hemorrhage. Neurocrit. Care 2010, 13, 3–9. [Google Scholar] [CrossRef]
- Brown, B.P.; Heistad, D.D. Capacitance of the Rabbit Portal Vein and Inferior Vena Cava. J. Physiol. 1986, 381, 417–425. [Google Scholar] [CrossRef] [PubMed]
- Orso, D.; Paoli, I.; Piani, T.; Cilenti, F.L.; Cristiani, L.; Guglielmo, N. Accuracy of Ultrasonographic Measurements of Inferior Vena Cava to Determine Fluid Responsiveness: A Systematic Review and Meta-Analysis. J. Intensive Care Med. 2020, 35, 354–363. [Google Scholar] [CrossRef] [PubMed]
- Taccheri, T.; Gavelli, F.; Teboul, J.-L.; Shi, R.; Monnet, X. Do Changes in Pulse Pressure Variation and Inferior Vena Cava Distensibility during Passive Leg Raising and Tidal Volume Challenge Detect Preload Responsiveness in Case of Low Tidal Volume Ventilation? Crit. Care 2021, 25, 110. [Google Scholar] [CrossRef] [PubMed]
- Nath, J.; Vacek, J.L.; Heidenreich, P.A. A Dilated Inferior Vena Cava Is a Marker of Poor Survival. Am. Heart J. 2006, 151, 730–735. [Google Scholar] [CrossRef] [PubMed]
- Guinot, P.G.; Abou-Arab, O.; Longrois, D.; Dupont, H. Right Ventricular Systolic Dysfunction and Vena Cava Dilatation Precede Alteration of Renal Function in Adult Patients Undergoing Cardiac Surgery: An Observational Study. Eur. J. Anaesthesiol. 2015, 32, 535–542. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Montilla, R.; Mukundan, S.; Heitner, S.B.; Khan, A. Inferior Vena Cava Dilation Predicts Global Cardiac Dysfunction in Acute Respiratory Distress Syndrome: A Strain Echocardiographic Study. Echocardiography 2021, 38, 238–248. [Google Scholar] [CrossRef]
- Goldhammer, E.; Mesnick, N.; Abinader, E.G.; Sagiv, M. Dilated Inferior Vena Cava: A Common Echocardiographic Finding in Highly Trained Elite Athletes. J. Am. Soc. Echocardiogr. 1999, 12, 988–993. [Google Scholar] [CrossRef] [PubMed]
- Styczynski, G.; Jaltuszewska, M.; Kosiorowska, N.; Kostrzewska, M.; Szmigielski, C. Dilated Inferior Vena Cava in Young Adults with Vasovagal Syncope. Arch. Intern. Med. 2009, 169, 1634–1635. [Google Scholar] [CrossRef] [Green Version]
- Brun, C.; Zieleskiewicz, L.; Textoris, J.; Muller, L.; Bellefleur, J.-P.; Antonini, F.; Tourret, M.; Ortega, D.; Vellin, A.; Lefrant, J.-Y.; et al. Prediction of Fluid Responsiveness in Severe Preeclamptic Patients with Oliguria. Intensive Care Med. 2013, 39, 593–600. [Google Scholar] [CrossRef] [PubMed]
- Blanco, P.; Volpicelli, G. Common Pitfalls in Point-of-Care Ultrasound: A Practical Guide for Emergency and Critical Care Physicians. Crit. Ultrasound J. 2016, 8, 15. [Google Scholar] [CrossRef] [Green Version]
- Via, G.; Tavazzi, G.; Price, S. Ten Situations Where Inferior Vena Cava Ultrasound May Fail to Accurately Predict Fluid Responsiveness: A Physiologically Based Point of View. Intensive Care Med. 2016, 42, 1164–1167. [Google Scholar] [CrossRef]
- Rahman, O.; Markl, M.; Balte, P.; Berhane, H.; Blanken, C.; Suwa, K.; Dashnaw, S.; Wieben, O.; Bluemke, D.A.; Prince, M.R.; et al. Reproducibility and Changes in Vena Caval Blood Flow by Using 4D Flow MRI in Pulmonary Emphysema and Chronic Obstructive Pulmonary Disease (COPD): The Multi-Ethnic Study of Atherosclerosis (MESA) COPD Substudy. Radiology 2019, 292, 585–594. [Google Scholar] [CrossRef] [PubMed]
- Juhl-Olsen, P.; Frederiksen, C.A.; Sloth, E. Ultrasound Assessment of Inferior Vena Cava Collapsibility Is Not a Valid Measure of Preload Changes during Triggered Positive Pressure Ventilation: A Controlled Cross-over Study. Ultraschall Med. 2012, 33, 152–159. [Google Scholar] [CrossRef] [PubMed]
- Beaubien-Souligny, W.; Rola, P.; Haycock, K.; Bouchard, J.; Lamarche, Y.; Spiegel, R.; Denault, A.Y. Quantifying Systemic Congestion with Point-Of-Care Ultrasound: Development of the Venous Excess Ultrasound Grading System. Ultrasound J. 2020, 12, 16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Corradi, F.; Via, G.; Tavazzi, G. What’s New in Ultrasound-Based Assessment of Organ Perfusion in the Critically Ill: Expanding the Bedside Clinical Monitoring Window for Hypoperfusion in Shock. Intensive Care Med. 2020, 46, 775–779. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Patients (n) | Setting | Parameter | Cut-Off (%) | S (%) | Sp (%) |
|---|---|---|---|---|---|---|
| Spontaneously breathing patients | ||||||
| Airapetian et al. [42] | 59 | Hypovolaemia | cIVC | ≥42 | 31 | 97 |
| Lanspa et al. [43] | 14 | Sepsis | cIVC | ≥50 | NR | NR |
| Bortolotti et al. [44] | 55 | Sepsis | cIVC-st | ≥39 | 93 | 88 |
| Vignon et al. [45] | 422 | Shock | dIVC | >18 | 28 | 90 |
| Byon et al. [46] | 33 | Paediatric neurosurgery | ΔDIVC | NR | NR | NR |
| Choi et al. [47] | 21 | Paediatric cardiac surgery | ΔDIVC | NR | NR | NR |
| Weber et al. [48] | 31 | Paediatric | dIVC | NR | NR | NR |
| Muller et al. [49] | 40 | Shock | cIVC | >40 | 70 | 80 |
| Preau et al. [50] | 90 | Sepsis | cIVC-st | ≥48 | 84 | 90 |
| Corl et al. [51] | 124 | Shock | cIVC | ≥25 | 87 | 81 |
| Doucet et al. [52] | 144 | Trauma | cIVC | ≥51 | NR | NR |
| Machare-Delgado [53] | 25 | Shock | dIVC | >12 | 100 | 53 |
| Charbonneau et al. [54] | 44 | Sepsis | dIVC | >21 | 38 | 61 |
| Theerawit et al. [55] | 29 | Sepsis | dIVC | ≥10 | 75 | 77 |
| Lu et al. [56] | 49 | Sepsis | dIVC | ≥20 | 67 | 77 |
| Zhang et al. [57] | 40 | Elective GI surgery | dIVC | ≥46 | 69 | 93 |
| Sobczyk et al. [58] | 50 | Cardiac Surgery | dIVC | > 18 | NR | NR |
| Sobczyk et al. [59] | 35 | Cardiac Surgery | dIVC | ≥ 18 | 82 | 73 |
| Moretti et al. [60] | 29 | SAH | dIVC | >16 | 70 | 100 |
| De Valk et al. [17] | 45 | Shock | cIVC | ≥36.5 | 83 | 67 |
| Long et al. [30] | 291 | Meta-analysis | cIVC | >42 | 52 | 77 |
| Mechanical Ventilated patients | ||||||
| Barbier et al. [15] | 20 | Sepsis | dIVC | >18 | 90 | 90 |
| Feissel et al. [26] | 39 | Sepsis | dIVC | >12 | NR | NR |
| Yao et al. [27] | 67 | Mixed | IVC ADI | ≥10.2 | 97 | 40 |
| dIVC | ≥25.5 | 46 | 90 | |||
| Long et al. [30] | 242 | Meta-analysis | dIVC | >16 | 67 | 68 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Di Nicolò, P.; Tavazzi, G.; Nannoni, L.; Corradi, F. Inferior Vena Cava Ultrasonography for Volume Status Evaluation: An Intriguing Promise Never Fulfilled. J. Clin. Med. 2023, 12, 2217. https://doi.org/10.3390/jcm12062217
Di Nicolò P, Tavazzi G, Nannoni L, Corradi F. Inferior Vena Cava Ultrasonography for Volume Status Evaluation: An Intriguing Promise Never Fulfilled. Journal of Clinical Medicine. 2023; 12(6):2217. https://doi.org/10.3390/jcm12062217
Chicago/Turabian StyleDi Nicolò, Pierpaolo, Guido Tavazzi, Luca Nannoni, and Francesco Corradi. 2023. "Inferior Vena Cava Ultrasonography for Volume Status Evaluation: An Intriguing Promise Never Fulfilled" Journal of Clinical Medicine 12, no. 6: 2217. https://doi.org/10.3390/jcm12062217