
Monitoring Systems in Home Ventilation

Abstract
:1. Introduction
2. Data Recorded by the Ventilator
2.1. Measurements and Calculations
2.1.1. Airway Pressure
2.1.2. Flow
2.1.3. Volume
2.1.4. Leaks
2.1.5. Other Measurements
2.2. Interpretation
2.2.1. Daily Use
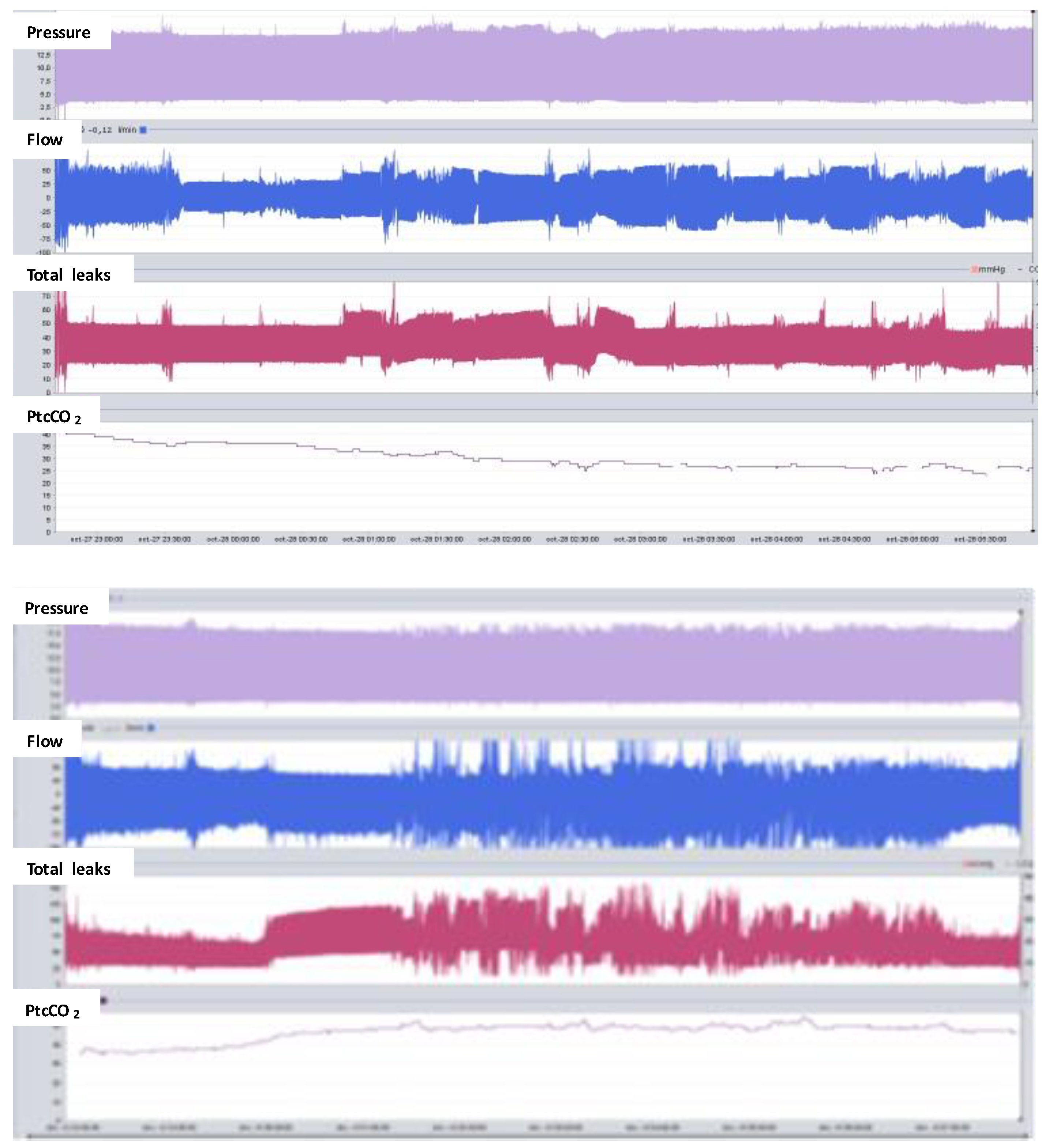
2.2.2. Leaks
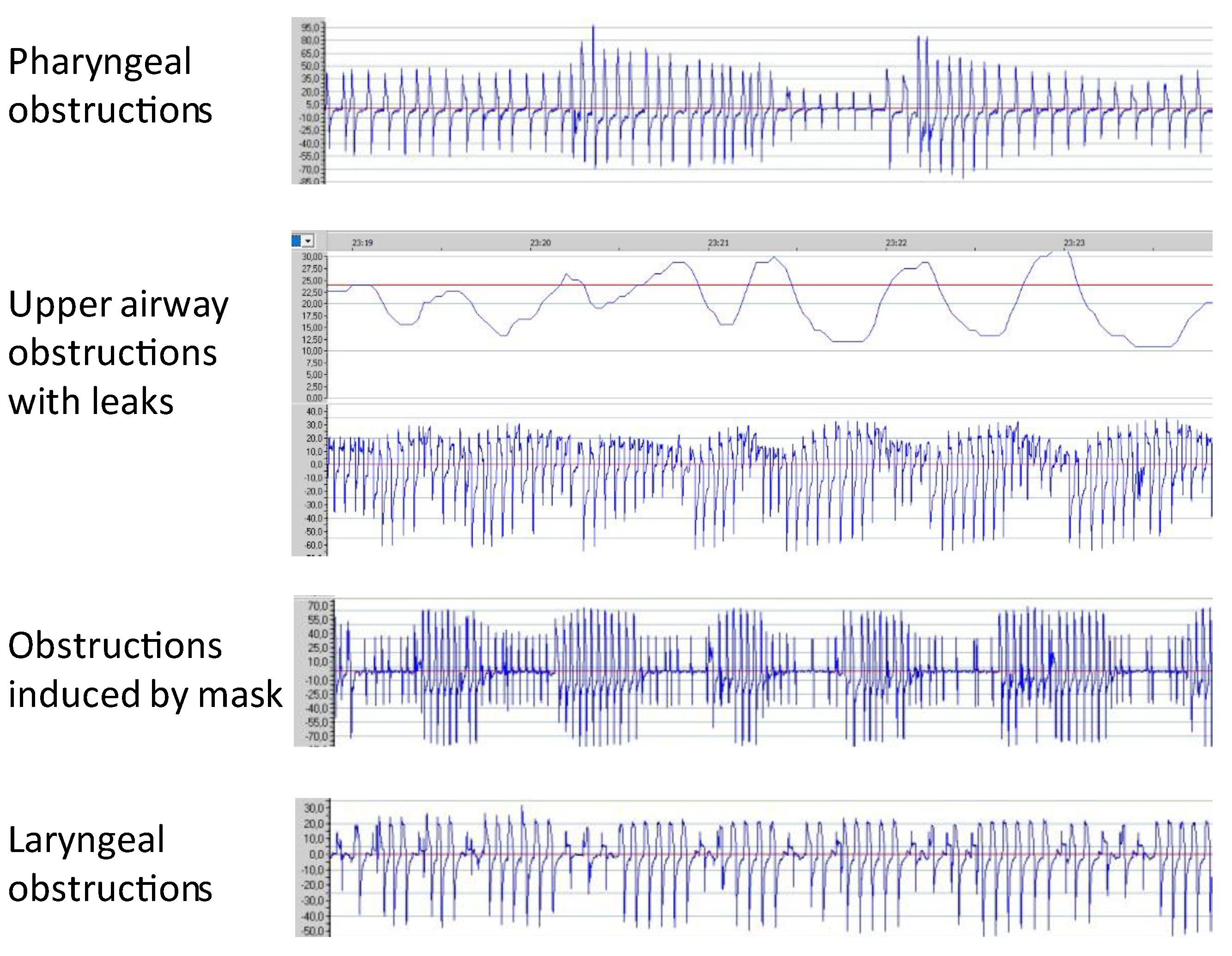
2.2.3. Upper Airway Obstructions
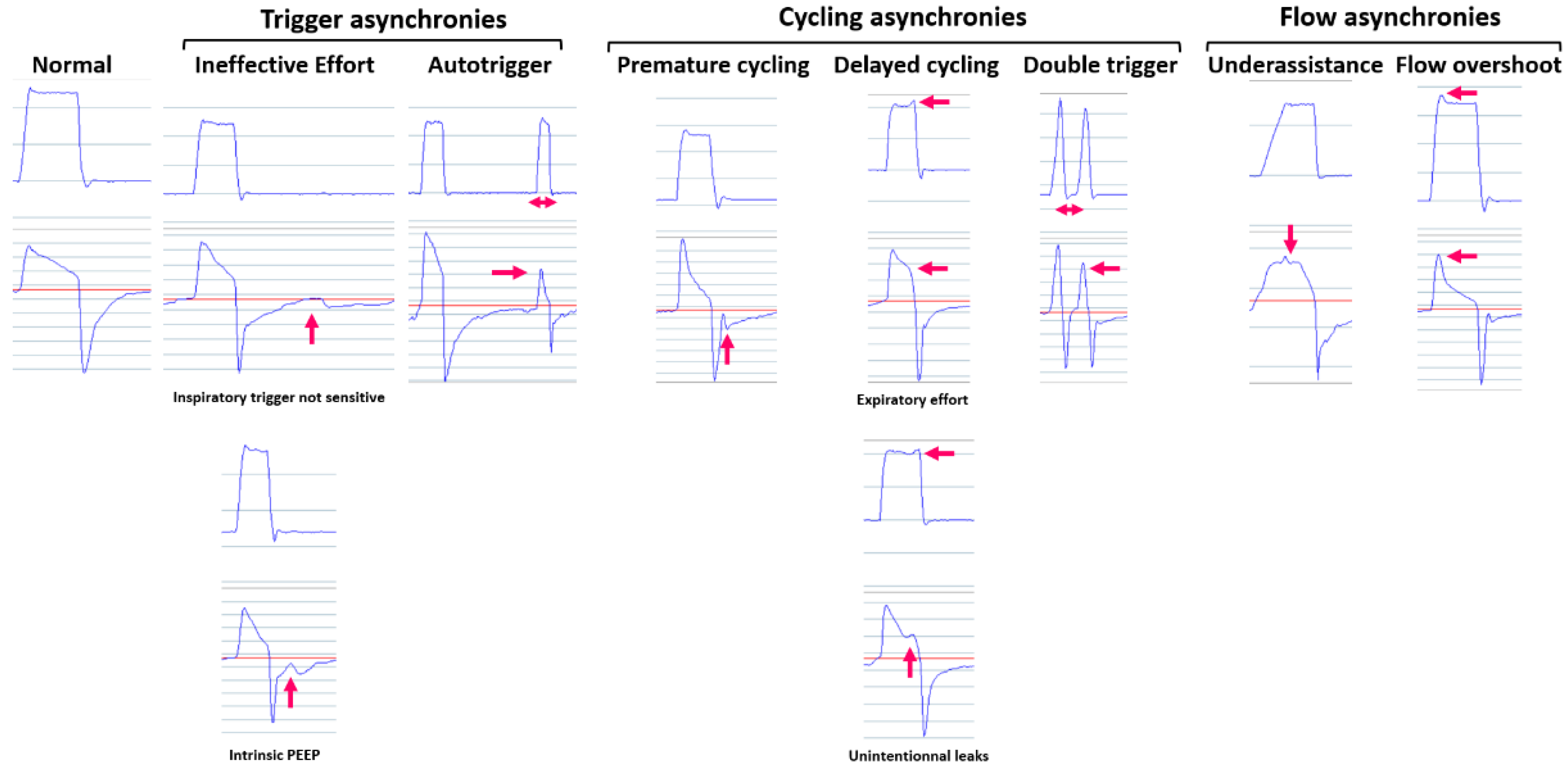
2.2.4. Patient–Ventilator Synchrony
2.2.5. Other Variables
3. Nocturnal Recordings
3.1. Nocturnal Pulse Oximetry
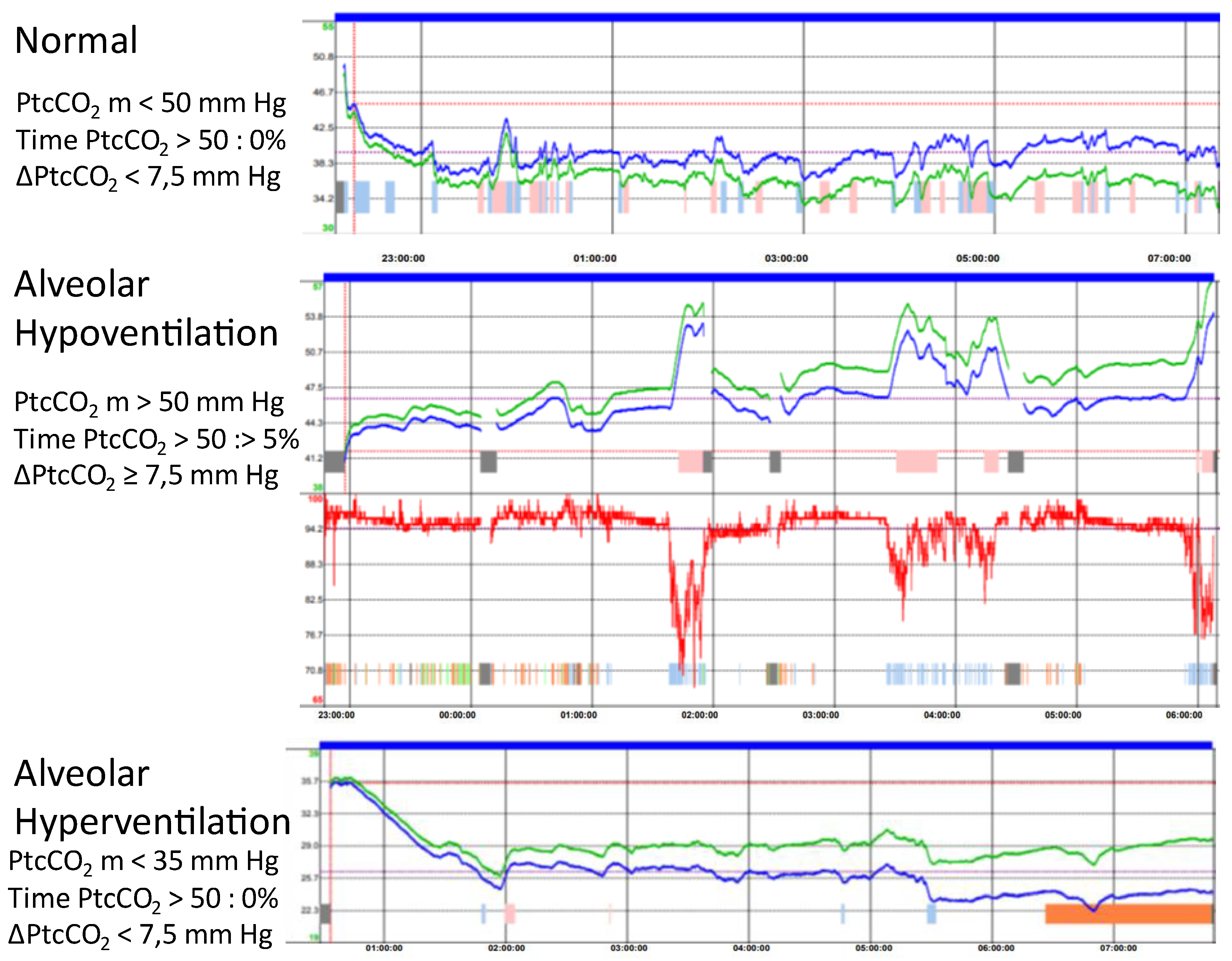
3.2. Transcutaneous Capnography
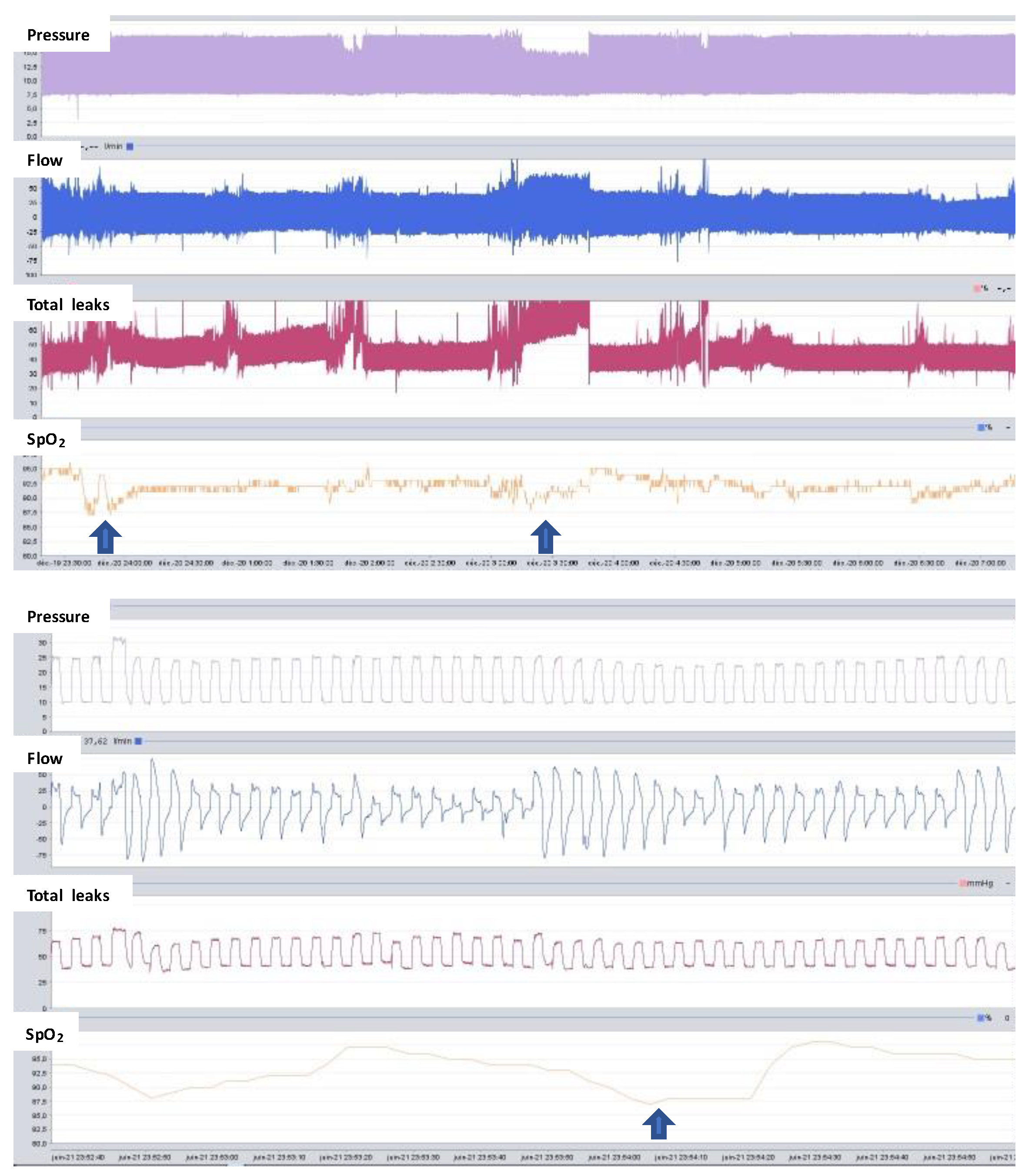
3.3. Respiratory Polygraphy
3.4. Polysomnography
4. Telemonitoring
4.1. Ventilator Data Collection Methods
4.2. Variables Telemonitored
4.3. Applications
4.4. Clinical Utility and Evidence
5. Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Janssens, J.-P.; Michel, F.; Schwarz, E.I.; Prella, M.; Bloch, K.; Adler, D.; Brill, A.-K.; Geenens, A.; Karrer, W.; Ogna, A.; et al. Long-Term Mechanical Ventilation: Recommendations of the Swiss Society of Pulmonology. Respiration 2020, 99, 867–902. [Google Scholar] [CrossRef] [PubMed]
- Janssens, J.-P.; Cantero, C.; Pasquina, P.; Georges, M.; Rabec, C. Monitoring Long Term Noninvasive Ventilation: Benefits, Caveats and Perspectives. Front. Med. 2022, 9, 874523. [Google Scholar] [CrossRef] [PubMed]
- Luján, M.; Sogo, A.; Pomares, X.; Monsó, E.; Sales, B.; Blanch, L. Effect of Leak and Breathing Pattern on the Accuracy of Tidal Volume Estimation by Commercial Home Ventilators: A Bench Study. Respir. Care 2013, 58, 770–777. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luján, M.; Lalmolda, C.; Ergan, B. Basic Concepts for Tidal Volume and Leakage Estimation in Non-Invasive Ventilation. Turk. Thorac. J. 2019, 20, 140–146. [Google Scholar] [CrossRef] [PubMed]
- Borel, J.-C.; Pepin, J.-L.; Pison, C.; Vesin, A.; Gonzalez-Bermejo, J.; Court-Fortune, I.; Timsit, J.-F. Long-term adherence with non-invasive ventilation improves prognosis in obese COPD patients. Respirology 2014, 19, 857–865. [Google Scholar] [CrossRef]
- Struik, F.M.; Lacasse, Y.; Goldstein, R.S.; Kerstjens, H.A.; Wijkstra, P.J. Nocturnal noninvasive positive pressure ventilation in stable COPD: A systematic review and individual patient data meta-analysis. Respir. Med. 2014, 108, 329–337. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Georges, M.; Adler, D.; Contal, O.; Espa, F.; Perrig, S.; Pépin, J.-L.; Janssens, J.-P. Reliability of Apnea-Hypopnea Index Measured by a Home Bi-Level Pressure Support Ventilator Versus a Polysomnographic Assessment. Respir. Care 2015, 60, 1051–1056. [Google Scholar] [CrossRef] [Green Version]
- Alvarez, R.F.; Rabec, C.; Cuadrado, G.R.; Hernandez, J.A.C.; Rodriguez, P.; Georges, M.; Casan, P. Monitoring Noninvasive Ventilation in Patients with Obesity Hypoventilation Syndrome: Comparison between Ventilator Built-in Software and Respiratory Polygraphy. Respiration 2017, 93, 162–169. [Google Scholar] [CrossRef]
- Vignaux, L.; Vargas, F.; Roeseler, J.; Tassaux, D.; Thille, A.W.; Kossowsky, M.P.; Brochard, L.; Jolliet, P. Patient–ventilator asynchrony during non-invasive ventilation for acute respiratory failure: A multicenter study. Intensive Care Med. 2009, 35, 840–846. [Google Scholar] [CrossRef] [Green Version]
- Mojoli, F.; Pozzi, M.; Orlando, A.; Bianchi, I.M.; Arisi, E.; Iotti, G.A.; Braschi, A.; Brochard, L. Timing of inspiratory muscle activity detected from airway pressure and flow during pressure support ventilation: The waveform method. Crit. Care 2022, 26, 32. [Google Scholar] [CrossRef]
- Georges, M.; Nguyen-Baranoff, D.; Griffon, L.; Foignot, C.; Bonniaud, P.; Camus, P.; Pepin, J.-L.; Rabec, C. Usefulness of transcutaneous PCO2 to assess nocturnal hypoventilation in restrictive lung disorders. Respirology 2016, 21, 1300–1306. [Google Scholar] [CrossRef]
- Ogna, A.; Salva, M.-A.Q.; Prigent, H.; Mroue, G.; Vaugier, I.; Annane, D.; Lofaso, F.; Orlikowski, D. Nocturnal hypoventilation in neuromuscular disease: Prevalence according to different definitions issued from the literature. Sleep Breath. 2015, 20, 575–581. [Google Scholar] [CrossRef]
- Jubran, A. Pulse oximetry. Crit. Care 2015, 19, 272. [Google Scholar] [CrossRef] [Green Version]
- Berry, R.B.; Budhiraja, R.; Gottlieb, D.J.; Gozal, D.; Iber, C.; Kapur, V.K.; Marcus, C.L.; Mehra, R.; Parthasarathy, S.; Quan, S.F.; et al. Rules for Scoring Respiratory Events in Sleep: Update of the 2007 AASM Manual for the Scoring of Sleep and Associated Events. Deliberations of the Sleep Apnea Definitions Task Force of the American Academy of Sleep Medicine. J. Clin. Sleep Med. 2012, 8, 597–619. [Google Scholar] [CrossRef] [Green Version]
- Vaidya, S.; Gothi, D.; Patro, M. COPD sleep phenotypes: Genesis of respiratory failure in COPD. Monaldi Arch. Chest Dis. 2021, 92. [Google Scholar] [CrossRef]
- Gonzalez-Bermejo, J.; Morélot-Panzini, C.; Arnol, N.; Meininger, V.; Kraoua, S.; Salachas, F.; Similowski, T. Prognostic value of efficiently correcting nocturnal desaturations after one month of non-invasive ventilation in amyotrophic lateral sclerosis: A retrospective monocentre observational cohort study. Amyotroph. Lateral Scler. Front. Degener. 2013, 14, 373–379. [Google Scholar] [CrossRef]
- Bote, S.M.; Martinez, N.P.; Amarilla, C.E.; Ugalde, P.F.; Gonzalez-Bermejo, J.; Collado, N.F.; Gamez, B.J. Overnight Pulse Oximetry to Determine Prognostic Factors in Subjects with Amyotrophic Lateral Sclerosis. Respir. Care 2020, 65, 1128–1134. [Google Scholar] [CrossRef] [PubMed]
- Pinto, A.; Almeida, J.P.; Pinto, S.; Pereira, J.; Oliveira, A.; de Carvalho, M. Home telemonitoring of non-invasive ventilation decreases healthcare utilisation in a prospective controlled trial of patients with amyotrophic lateral sclerosis. J. Neurol. Neurosurg. Psychiatry 2010, 81, 1238–1242. [Google Scholar] [CrossRef] [PubMed]
- Yoshizaki, A.; Nagano, T.; Izumi, S.; Nishiuma, T.; Nakata, K.; Yamamoto, M.; Yasuda, Y.; Hazama, D.; Umezawa, K.; Katsurada, N.; et al. Characteristics of the nocturnal desaturation waveform pattern of SpO2 in COPD patients: An observational study. Respir. Res. 2021, 22, 276. [Google Scholar] [CrossRef] [PubMed]
- Janssens, J.-P.; Borel, J.-C.; Pépin, J.-L.; SomnoNIV Group. Nocturnal monitoring of home non-invasive ventilation: The contribution of simple tools such as pulse oximetry, capnography, built-in ventilator software and autonomic markers of sleep fragmentation. Thorax 2010, 66, 438–445. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nardi, J.; Prigent, H.; Adala, A.; Bohic, M.; Lebargy, F.; Quera-Salva, M.-A.; Orlikowski, D.; Lofaso, F. Nocturnal Oximetry and Transcutaneous Carbon Dioxide in Home-Ventilated Neuromuscular Patients. Respir. Care 2012, 57, 1425–1430. [Google Scholar] [CrossRef] [Green Version]
- Georges, M.; Rabec, C.; Monin, E.; Aho, S.; Beltramo, G.; Janssens, J.-P.; Bonniaud, P. Monitoring of noninvasive ventilation: Comparative analysis of different strategies. Respir. Res. 2020, 21, 324. [Google Scholar] [CrossRef]
- Huttmann, S.E.; Windisch, W.; Storre, J.H. Techniques for the Measurement and Monitoring of Carbon Dioxide in the Blood. Ann. Am. Thorac. Soc. 2014, 11, 645–652. [Google Scholar] [CrossRef]
- De Braekeleer, K.; Toussaint, M. Transcutaneous Carbon Dioxide Measurement in Adult Patients with Neuromuscular Disorders: A quality Level Assessment. J. Neuromuscul. Dis. 2021, 8, 305–313. [Google Scholar] [CrossRef]
- Mycroft, K.; Nasiłowski, J.; Klimiuk, J.; Przybyłowski, T. Complex home assessment of long-term non-invasive ventilation efficacy using transcutaneous monitoring of PCO2 and polygraphy—A feasibility study. Adv. Med. Sci. 2021, 66, 105–112. [Google Scholar] [CrossRef] [PubMed]
- Nassar, B.S.; Schmidt, G.A. Estimating Arterial Partial Pressure of Carbon Dioxide in Ventilated Patients: How Valid Are Surrogate Measures? Ann. Am. Thorac. Soc. 2017, 14, 1005–1014. [Google Scholar] [CrossRef]
- Stieglitz, S.; Matthes, S.; Priegnitz, C.; Hagmeyer, L.; Randerath, W. Comparison of Transcutaneous and Capillary Measurement of PCO2 in Hypercapnic Subjects. Respir. Care 2016, 61, 98–105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bauman, K.A.; Kurili, A.; Schmidt, S.L.; Rodriguez, G.M.; Chiodo, A.E.; Sitrin, R.G. Home-Based Overnight Transcutaneous Capnography/Pulse Oximetry for Diagnosing Nocturnal Hypoventilation Associated with Neuromuscular Disorders. Arch. Phys. Med. Rehabil. 2013, 94, 46–52. [Google Scholar] [CrossRef]
- Boentert, M.; Glatz, C.; Helmle, C.; Okegwo, A.; Young, P. Prevalence of sleep apnoea and capnographic detection of nocturnal hypoventilation in amyotrophic lateral sclerosis. J. Neurol. Neurosurg. Psychiatry 2018, 89, 418–424. [Google Scholar] [CrossRef] [PubMed]
- Ogna, A.; Nardi, J.; Prigent, H.; Salva, M.-A.Q.; Chaffaut, C.; Lamothe, L.; Chevret, S.; Annane, D.; Orlikowski, D.; Lofaso, F. Prognostic Value of Initial Assessment of Residual Hypoventilation Using Nocturnal Capnography in Mechanically Ventilated Neuromuscular Patients: A 5-Year Follow-up Study. Front. Med. 2016, 3, 40. [Google Scholar] [CrossRef] [Green Version]
- Crescimanno, G.; Greco, F.; Canino, M.; Bertini, M.; Marrone, O. Contribution of transcutaneous capnography to the interpretation of abnormal respiratory events during noninvasive ventilation. Sleep Med. 2019, 62, 77–79. [Google Scholar] [CrossRef]
- Gonzalez-Bermejo, J.; Perrin, C.; Janssens, J.P.; Pepin, J.L.; Mroue, G.; Léger, P.; Langevin, B.; Rouault, S.; Rabec, C.; Rodenstein, D.; et al. Proposal for a systematic analysis of polygraphy or polysomnography for identifying and scoring abnormal events occurring during non-invasive ventilation. Thorax 2010, 67, 546–552. [Google Scholar] [CrossRef] [Green Version]
- López-Brull, H.; Mira-Padilla, E.; Hussein, S.; Guerder, A.; Wozniak, E.; Esteban-Ronda, V.; Gonzalez-Bermejo, J. Ventilator integrated polygraphy for patients using non-invasive ventilation; Case report. Front. Med. 2022, 9, 852896. [Google Scholar] [CrossRef] [PubMed]
- Vrijsen, B.; Buyse, B.; Belge, C.; Robberecht, W.; Van Damme, P.; Decramer, M.; Testelmans, D. Noninvasive Ventilation Improves Sleep in Amyotrophic Lateral Sclerosis: A Prospective Polysomnographic Study. J. Clin. Sleep Med. 2015, 11, 559–566. [Google Scholar] [CrossRef] [Green Version]
- Vrijsen, B.; Chatwin, M.; Contal, O.; Derom, E.; Janssens, J.-P.; Kampelmacher, M.J.; Muir, J.-F.; Pinto, S.; Rabec, C.; Ramsay, M.; et al. Hot Topics in Noninvasive Ventilation: Report of a Working Group at the International Symposium on Sleep-Disordered Breathing in Leuven, Belgium. Respir. Care 2015, 60, 1337–1362. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hannan, L.M.; Rautela, L.; Berlowitz, D.J.; McDonald, C.F.; Cori, J.M.; Sheers, N.; Chao, C.; O’Donoghue, F.J.; Howard, M.E. Randomised controlled trial of polysomnographic titration of noninvasive ventilation. Eur. Respir. J. 2019, 53, 1802118. [Google Scholar] [CrossRef]
- Hwang, D.; Chang, J.W.; Benjafield, A.V.; Crocker, M.E.; Kelly, C.; Becker, K.A.; Kim, J.B.; Woodrum, R.R.; Liang, J.; Derose, S.F. Effect of Telemedicine Education and Telemonitoring on Continuous Positive Airway Pressure Adherence. The Tele-OSA Randomized Trial. Am. J. Respir. Crit. Care Med. 2018, 197, 117–126. [Google Scholar] [CrossRef]
- Pépin, J.-L.; Jullian-Desayes, I.; Sapène, M.; Treptow, E.; Joyeux-Faure, M.; Benmerad, M.; Bailly, S.; Grillet, Y.; Stach, B.; Richard, P.; et al. Multimodal Remote Monitoring of High Cardiovascular Risk Patients with OSA Initiating CPAP. Chest 2019, 155, 730–739. [Google Scholar] [CrossRef] [PubMed]
- Hoet, F.; Libert, W.; Sanida, C.; Van den Broecke, S.; Bruyneel, A.; Bruyneel, M. Telemonitoring in continuous positive airway pressure-treated patients improves delay to first intervention and early compliance: A randomized trial. Sleep Med. 2017, 39, 77–83. [Google Scholar] [CrossRef] [PubMed]
- Ackrivo, J.; Elman, L.; Hansen-Flaschen, J. Telemonitoring for Home-assisted Ventilation: A Narrative Review. Ann. Am. Thorac. Soc. 2021, 18, 1761–1772. [Google Scholar] [CrossRef]
- Cheng, S.-L.; Chan, V.L.; Chu, C.-M. Compliance with home non-invasive ventilation. Respirology 2012, 17, 735–736. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, E.I.; Mackie, M.; Weston, N.; Tincknell, L.; Beghal, G.; Cheng, M.C.; Ramsay, M.; Suh, E.-S.; Kaltsakas, G.; Pattani, H.; et al. Time-to-death in chronic respiratory failure on home mechanical ventilation: A cohort study. Respir. Med. 2020, 162, 105877. [Google Scholar] [CrossRef] [PubMed]
- Contal, O.; Vignaux, L.; Combescure, C.; Pepin, J.-L.; Jolliet, P.; Janssens, J.-P. Monitoring of Noninvasive Ventilation by Built-in Software of Home Bilevel Ventilators: A bench study. Chest 2012, 141, 469–476. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhu, K.; Rabec, C.; Gonzalez-Bermejo, J.; Hardy, S.; Aouf, S.; Escourrou, P.; Roisman, G. Combined effects of leaks, respiratory system properties and upper airway patency on the performance of home ventilators: A bench study. BMC Pulm. Med. 2017, 17, 145. [Google Scholar] [CrossRef] [Green Version]
- Sogo, A.; Montanyà, J.; Monsó, E.; Blanch, L.; Pomares, X.; Lujàn, M. Effect of dynamic random leaks on the monitoring accuracy of home mechanical ventilators: A bench study. BMC Pulm. Med. 2013, 13, 75. [Google Scholar] [CrossRef] [Green Version]
- Fauroux, B.; Leroux, K.; Pépin, J.L.; Lofaso, F.; Louis, B. Are home ventilators able to guarantee a minimal tidal volume? Intensive Care Med. 2010, 36, 1008–1014. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez, J.; Sharshar, T.; Hart, N.; Chadda, K.; Raphaël, J.C.; Lofaso, F. Air leaks during mechanical ventilation as a cause of persistent hypercapnia in neuromuscular disorders. Intensive Care Med. 2003, 29, 596–602. [Google Scholar] [CrossRef] [PubMed]
- Mansell, S.K.; Cutts, S.; Hackney, I.; Wood, M.J.; Hawksworth, K.; Creer, D.D.; Kilbride, C.; Mandal, S. Using domiciliary non-invasive ventilator data downloads to inform clinical decision-making to optimise ventilation delivery and patient compliance. BMJ Open Respir. Res. 2018, 5, e000238. [Google Scholar] [CrossRef] [Green Version]
- Borel, J.-C.; Pelletier, J.; Taleux, N.; Briault, A.; Arnol, N.; Pison, C.; Tamisier, R.; Timsit, J.-F.; Pepin, J.-L. Parameters recorded by software of non-invasive ventilators predict COPD exacerbation: A proof-of-concept study. Thorax 2015, 70, 284–285. [Google Scholar] [CrossRef] [Green Version]
- Blouet, S.; Sutter, J.; Fresnel, E.; Kerfourn, A.; Cuvelier, A.; Patout, M. Prediction of severe acute exacerbation using changes in breathing pattern of COPD patients on home noninvasive ventilation. Int. J. Chronic Obstr. Pulm. Dis. 2018, 13, 2577–2586. [Google Scholar] [CrossRef] [Green Version]
- Jiang, W.; Chao, Y.; Wang, X.; Chen, C.; Zhou, J.; Song, Y. Day-to-Day Variability of Parameters Recorded by Home Noninvasive Positive Pressure Ventilation for Detection of Severe Acute Exacerbations in COPD. Int. J. Chronic Obstr. Pulm. Dis. 2021, 16, 727–737. [Google Scholar] [CrossRef] [PubMed]
- Jeganathan, V.; Rautela, L.; Conti, S.; Saravanan, K.; Rigoni, A.; Graco, M.; Hannan, L.M.; Howard, M.E.; Berlowitz, D.J. Typical within and between person variability in non-invasive ventilator derived variables among clinically stable, long-term users. BMJ Open Respir. Res. 2021, 8, e000824. [Google Scholar] [CrossRef] [PubMed]
- Duiverman, M.L.; Vonk, J.M.; Bladder, G.; van Melle, J.P.; Nieuwenhuis, J.; Hazenberg, A.; Kerstjens, H.A.M.; van Boven, J.F.M.; Wijkstra, P.J. Home initiation of chronic non-invasive ventilation in COPD patients with chronic hypercapnic respiratory failure: A randomised controlled trial. Thorax 2020, 75, 244–252. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hazenberg, A.; Kerstjens, H.A.; Prins, S.C.; Vermeulen, K.M.; Wijkstra, P.J. Initiation of home mechanical ventilation at home: A randomised controlled trial of efficacy, feasibility and costs. Respir. Med. 2014, 108, 1387–1395. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murphy, P.B.; Patout, M.; Arbane, G.; Mandal, S.; Kaltsakas, G.; I Polkey, M.; Elliott, M.; Muir, J.-F.; Douiri, A.; Parkin, D.; et al. Cost-effectiveness of outpatient versus inpatient non-invasive ventilation setup in obesity hypoventilation syndrome: The OPIP trial. Thorax 2023, 78, 24–31. [Google Scholar] [CrossRef] [PubMed]
- Vitacca, M.; Paneroni, M.; Grossetti, F.; Ambrosino, N. Is There Any Additional Effect of Tele-Assistance on Long-Term Care Programmes in Hypercapnic COPD Patients? A Retrospective Study. COPD 2016, 13, 576–582. [Google Scholar] [CrossRef] [PubMed]
- Vitacca, M.; Bianchi, L.; Guerra, A.; Fracchia, C.; Spanevello, A.; Balbi, B.; Scalvini, S. Tele-assistance in chronic respiratory failure patients: A randomised clinical trial. Eur. Respir. J. 2009, 33, 411–418. [Google Scholar] [CrossRef] [Green Version]
- de Almeida, J.P.L.; Pinto, A.; Pinto, S.; Ohana, B.; de Carvalho, M. Economic cost of home-telemonitoring care for BiPAP-assisted ALS individuals. Amyotroph. Lateral Scler. 2012, 13, 533–537. [Google Scholar] [CrossRef]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Accuracy | Variables | Comments |
|---|---|---|
| Good | Mean/Median Daily use | |
| Hours of use | ||
| Total leaks | ||
| Respiratory rate | Ventilatory rate ≠ patient’s respiratory rate | |
| Percentage of triggered breath | ||
| Percentage of spontaneous cycled breath | ||
| Inspiratory time | ||
| I/E ratio | ||
| Acceptable | Unintentional leaks | Better if intentional leaks are adjustable |
| Apnea hypopnea index | Depends on the type of obstruction and the presence of leaks | |
| Sub-optimal | Tidal volume | ±20% if no leaks, less precise if additional unintentional leaks |
| Minute volume |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Arnal, J.-M.; Oranger, M.; Gonzalez-Bermejo, J. Monitoring Systems in Home Ventilation. J. Clin. Med. 2023, 12, 2163. https://doi.org/10.3390/jcm12062163
Arnal J-M, Oranger M, Gonzalez-Bermejo J. Monitoring Systems in Home Ventilation. Journal of Clinical Medicine. 2023; 12(6):2163. https://doi.org/10.3390/jcm12062163
Chicago/Turabian StyleArnal, Jean-Michel, Mathilde Oranger, and Jésus Gonzalez-Bermejo. 2023. "Monitoring Systems in Home Ventilation" Journal of Clinical Medicine 12, no. 6: 2163. https://doi.org/10.3390/jcm12062163