
Comparison between the Flapless Surgical Approach and a Novel Single Incision Access in Terms of Recovery Time and Comfort after Extraction of Impacted Inferior Third Molars: A Randomised, Blinded, Split-Mouth Controlled Clinical Trial

 , ,
, , 

Abstract
:1. Introduction
2. Materials and Methods
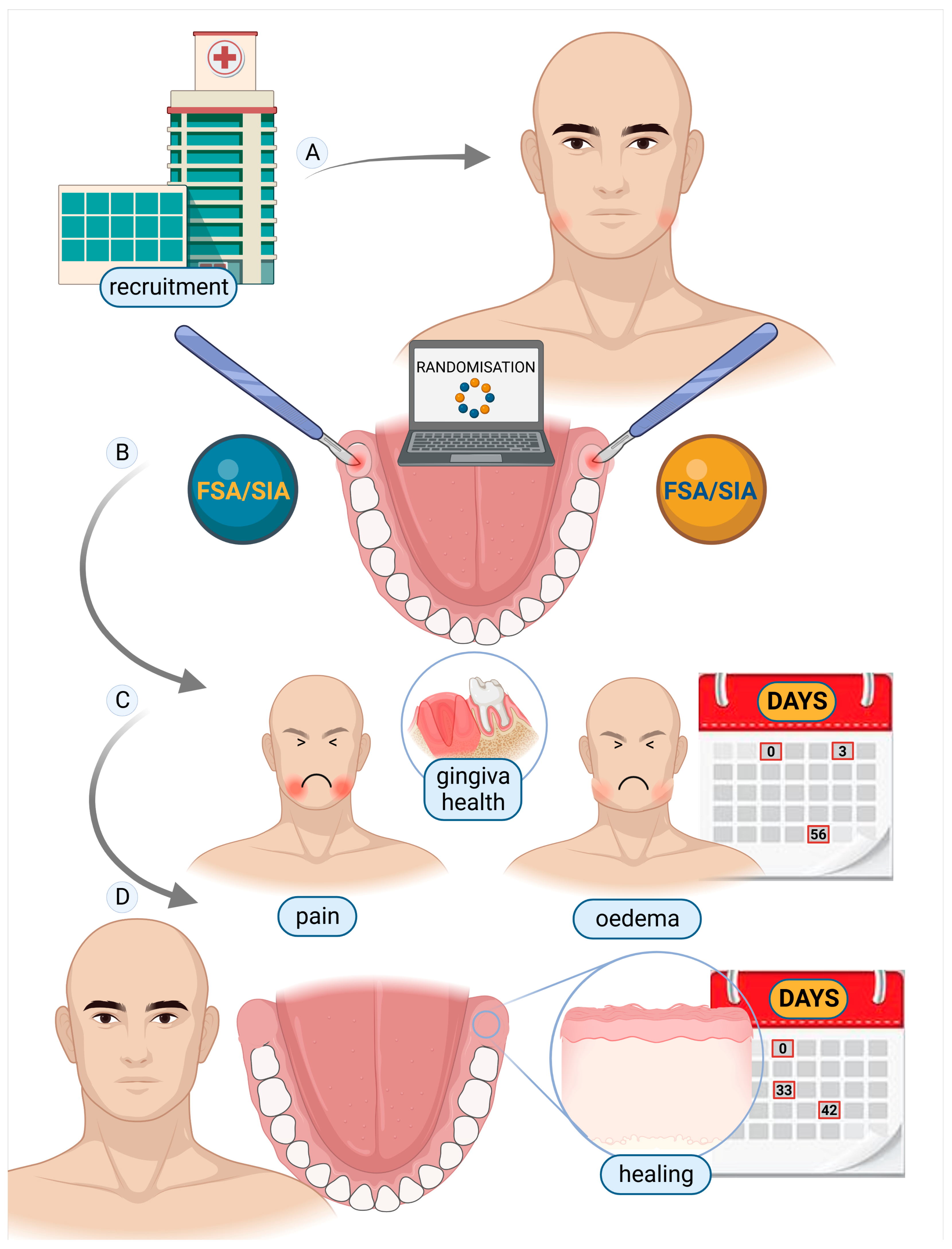
2.1. Study Participants and Design
2.2. Randomisation and Masking
2.3. Pre-Surgical Treatment and Procedure
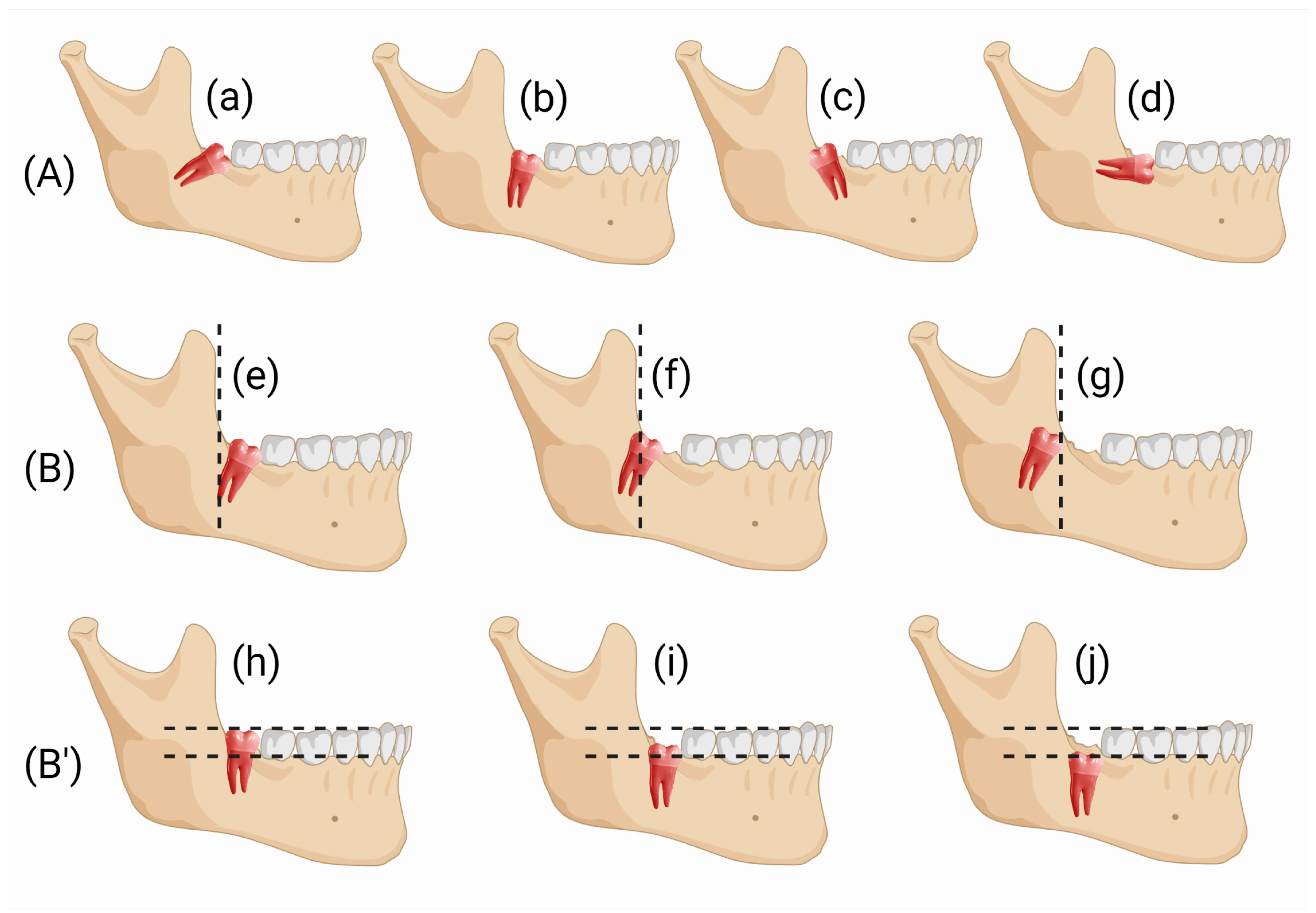
2.4. Surgical Design
2.4.1. FSA Surgical Design
2.4.2. SIA Surgical Design
2.5. Post-Surgical Treatment and Procedure
2.6. Outcomes and Endpoints Evaluation
2.7. Statistical Analysis
3. Results
3.1. Patient and Baseline Characteristics
3.2. Clinical Follow-Up and Outcome Measures
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Galvão, E.L.; da Silveira, E.M.; de Oliveira, E.S.; da Cruz, T.M.M.; Flecha, O.D.; Falci, S.G.M.; Gonçalves, P.F. Association between Mandibular Third Molar Position and the Occurrence of Pericoronitis: A Systematic Review and Meta-Analysis. Arch. Oral Biol. 2019, 107, 104486. [Google Scholar] [CrossRef]
- Candotto, V.; Oberti, L.; Gabrione, F.; Scarano, A.; Rossi, D.; Romano, M. Complication in Third Molar Extractions. J. Biol. Regul. Homeost. Agents 2019, 33, 169–172. [Google Scholar]
- Duarte-Rodrigues, L.; Miranda, E.F.P.; Souza, T.O.; de Paiva, H.N.; Falci, S.G.M.; Galvão, E.L. Third Molar Removal and Its Impact on Quality of Life: Systematic Review and Meta-Analysis. Qual. Life Res. 2018, 27, 2477–2489. [Google Scholar] [CrossRef] [PubMed]
- Kang, F.; Sah, M.K.; Fei, G. Determining the Risk Relationship Associated with Inferior Alveolar Nerve Injury Following Removal of Mandibular Third Molar Teeth: A Systematic Review. J. Stomatol. Oral Maxillofac. Surg. 2020, 121, 63–69. [Google Scholar] [CrossRef]
- Negreiros, R.M.; Biazevic, M.G.H.; Jorge, W.A.; Michel-Crosato, E. Relationship between Oral Health-Related Quality of Life and the Position of the Lower Third Molar: Postoperative Follow-Up. J. Oral Maxillofac. Surg. 2012, 70, 779–786. [Google Scholar] [CrossRef] [PubMed]
- Qiao, F.; Zhang, M.; Zhang, T.; Zhu, D. Dental Anxiety Is Related to Postoperative Symptoms in Third Molar Surgery. Front Psychiatry 2022, 13, 956566. [Google Scholar] [CrossRef] [PubMed]
- di Nardo, D.; Mazzucchi, G.; Lollobrigida, M.; Passariello, C.; Guarnieri, R.; Galli, M.; de Biase, A.; Testarelli, L. Immediate or Delayed Retrieval of the Displaced Third Molar: A Review. J. Clin. Exp. Dent. 2019, 11, e55. [Google Scholar] [CrossRef]
- Glera-Suárez, P.; Soto-Peñaloza, D.; Peñarrocha-Oltra, D.; Peñarrocha-Diago, M. Patient Morbidity after Impacted Third Molar Extraction with Different Flap Designs. A Systematic Review and Meta-Analysis. Med. Oral Patol. Oral Cir. Bucal 2020, 25, e233–e239. [Google Scholar] [CrossRef]
- Materni, A.; de Angelis, N.; di Tullio, N.; Colombo, E.; Benedicenti, S.; Amaroli, A. Flapless Surgical Approach to Extract Impacted Inferior Third Molars: A Retrospective Clinical Study. J. Clin. Med. 2021, 10, 593. [Google Scholar] [CrossRef]
- Ramalingam, S.; Bhargava, D. Advances in Surgical Extraction of the Mandibular Third Molars. In Transalveolar of the Mandibular Third Molars; CRC Press: Boca Raton, FL, USA, 2022; pp. 163–175. [Google Scholar] [CrossRef]
- Khojastepour, L.; Khaghaninejad, M.S.; Hasanshahi, R.; Forghani, M.; Ahrari, F. Does the Winter or Pell and Gregory Classification System Indicate the Apical Position of Impacted Mandibular Third Molars? J. Oral Maxillofac. Surg. 2019, 77, 2222.e1–2222.e9. [Google Scholar] [CrossRef]
- Silva, S.A.; Horliana, A.C.R.T.; Pannuti, C.M.; Braz-Silva, P.H.; Bispo, C.G.C.; Buscariolo, I.A.; Rocha, R.G.; Tortamano, I.P. Comparative Evaluation of Anesthetic Efficacy of 1.8 ML and 3.6 ML of Articaine in Irreversible Pulpitis of the Mandibular Molar: A Randomized Clinical Trial. PLoS ONE 2019, 14, e0219536. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Hare, P.E.; Wilson, B.J.; Loga, M.G.; Ariyawardana, A. Effect of Submucosal Dexamethasone Injections in the Prevention of Postoperative Pain, Trismus, and Oedema Associated with Mandibular Third Molar Surgery: A Systematic Review and Meta-Analysis. Int. J. Oral Maxillofac. Surg. 2019, 48, 1456–1469. [Google Scholar] [CrossRef] [PubMed]
- Longman, L.P.; Martin, M.V. The Use of Antibiotics in the Prevention of Post-Operative Infection: A Re-Appraisal. Br. Dent. J. 1991, 170, 257–262. [Google Scholar] [CrossRef]
- Peterson, L.J. Antibiotic Prophylaxis against Wound Infections in Oral and Maxillofacial Surgery. J. Oral Maxillofac. Surg. 1990, 48, 617–620. [Google Scholar] [CrossRef] [PubMed]
- Slade, G.D.; Foy, S.P.; Shugars, D.A.; Phillips, C.; White, R.P. The Impact of Third Molar Symptoms, Pain, and Swelling on Oral Health-Related Quality of Life. J. Oral Maxillofac. Surg. 2004, 62, 1118–1124. [Google Scholar] [CrossRef] [PubMed]
- Shugars, D.A.; Gentile, M.A.; Ahmad, N.; Stavropoulos, M.F.; Slade, G.D.; Phillips, C.; Conrad, S.M.; Fleuchaus, P.T.; White, R.P. Assessment of Oral Health-Related Quality of Life before and after Third Molar Surgery. J. Oral Maxillofac. Surg. 2006, 64, 1721–1730. [Google Scholar] [CrossRef] [PubMed]
- Hallab, L.; Azzouzi, A.; Chami, B. Quality of Life after Extraction of Mandibular Wisdom Teeth: A Systematic Review. Ann. Med. Surg. 2022, 81, 104387. [Google Scholar] [CrossRef]
- McGrath, C.; Comfort, M.B.; Lo, E.C.M.; Luo, Y. Can Third Molar Surgery Improve Quality of Life? A 6-Month Cohort Study. J. Oral Maxillofac. Surg. 2003, 61, 759–763. [Google Scholar] [CrossRef]
- Bhargava, D. Surgical techniques for transalveolar extraction of the mandibular third molars. In Transalveolar Extraction of the Mandibular Third Molars, 1st ed.; CRC Press: Boca Raton, FL, USA, 2022; Chapter 10; pp. 99–119. [Google Scholar]
- Korkmaz, Y.T.; Mollaoglu, N.; Ozmeriç, N. Does Laterally Rotated Flap Design Influence the Short-Term Periodontal Status of Second Molars and Postoperative Discomfort after Partially Impacted Third Molar Surgery? J. Oral Maxillofac. Surg. 2015, 73, 1031–1041. [Google Scholar] [CrossRef]
- Kirtiloǧlu, T.; Bulut, E.; Sümer, M.; Cengiz, I. Comparison of 2 Flap Designs in the Periodontal Healing of Second Molars after Fully Impacted Mandibular Third Molar Extractions. J. Oral Maxillofac. Surg. 2007, 65, 2206–2210. [Google Scholar] [CrossRef]
- Choudhury, R.; Rastogi, S.; Rohatgi, R.G.; Abdulrahman, B.I.; Dutta, S.; Giri, K.Y. Does Pedicle Flap Design Influence the Postoperative Sequel of Lower Third Molar Surgery and Quality of Life? J. Oral Biol. Craniofac. Res. 2022, 12, 694–701. [Google Scholar] [CrossRef] [PubMed]
- Colorado-Bonnin, M.; Valmaseda-Castellón, E.; Berini-Aytés, L.; Gay-Escoda, C. Quality of Life Following Lower Third Molar Removal. Int. J. Oral Maxillofac. Surg. 2006, 35, 343–347. [Google Scholar] [CrossRef] [PubMed]
- Dar, M.M.; Shah, A.A.; Latief Najar, A.; Younis, M.; Kapoor, M.; Dar, J.I. Healing Potential of Platelet Rich Fibrin in Impacted Mandibular Third Molar Extraction Sockets. Ann. Maxillofac. Surg. 2018, 8, 206. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| VARIABLE | FSA | SIA |
|---|---|---|
| Days (Weeks) | Days (Weeks) | |
| RT | 42.1 ± 5.4 (6.0) | 33.6 ± 4.3 * (4.8) |
| VARIABLE | FSA | SIA | ||
|---|---|---|---|---|
| T0 | T1 | T0 | T1 | |
| AG | 2.6 ± 0.9 | 3.6 ± 0.8 * | 2.4 ± 1.3 | 3.5 ± 0.5 * |
| PPD | 4.4 ± 1.0 | 3.6 ± 0.6 * | 4.3 ± 0.6 | 3.6 ± 0.5 * |
| VARIABLE | FSA | SIA | ||||
|---|---|---|---|---|---|---|
| T0 | T1 | T2 | T0 | T1 | T2 | |
| OED | 0.0 (0.0) | 0.2 (0.4) * | 0.2 (0.4) | 0.0 (0.0) | 0.2 (0.2) * | 0.2 (0.2) |
| PS | 0.5 (1.1) | 0.3 (0.4) | 0.2 (0.3) | 0.4 (0.9) | 0.3 (0.5) | 0.2 (0.4) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Materni, A.; Pasquale, C.; Signore, A.; Benedicenti, S.; Amaroli, A. Comparison between the Flapless Surgical Approach and a Novel Single Incision Access in Terms of Recovery Time and Comfort after Extraction of Impacted Inferior Third Molars: A Randomised, Blinded, Split-Mouth Controlled Clinical Trial. J. Clin. Med. 2023, 12, 1995. https://doi.org/10.3390/jcm12051995
Materni A, Pasquale C, Signore A, Benedicenti S, Amaroli A. Comparison between the Flapless Surgical Approach and a Novel Single Incision Access in Terms of Recovery Time and Comfort after Extraction of Impacted Inferior Third Molars: A Randomised, Blinded, Split-Mouth Controlled Clinical Trial. Journal of Clinical Medicine. 2023; 12(5):1995. https://doi.org/10.3390/jcm12051995
Chicago/Turabian StyleMaterni, Alberto, Claudio Pasquale, Antonio Signore, Stefano Benedicenti, and Andrea Amaroli. 2023. "Comparison between the Flapless Surgical Approach and a Novel Single Incision Access in Terms of Recovery Time and Comfort after Extraction of Impacted Inferior Third Molars: A Randomised, Blinded, Split-Mouth Controlled Clinical Trial" Journal of Clinical Medicine 12, no. 5: 1995. https://doi.org/10.3390/jcm12051995