
COVID-19 Accelerated Cognitive Decline in Elderly Patients with Pre-Existing Dementia Followed up in an Outpatient Memory Care Facility
 and
and
Abstract
:1. Introduction
2. Methods
2.1. Patients
2.2. Dementia Diagnosis, Cognitive Function, and ADL Assessment of Patients
2.3. Statistical Methods
3. Results
3.1. Predictors of COVID-19 and Cognitive Decline
3.2. Effect of COVID-19 on the Yearly Change in MMSE Score and ADL Indexes
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Crivelli, L.; Palmer, K.; Calandri, I.; Guekht, A.; Beghi, E.; Carroll, W.; Frontera, J.; García-Azorín, D.; Westenberg, E.; Winkler, A.S.; et al. Changes in Cognitive Functioning after COVID-19: A Systematic Review and Meta-Analysis. Alzheimers Dement. J. Alzheimers Assoc. 2022, 18, 1047–1066. [Google Scholar] [CrossRef] [PubMed]
- Tabacof, L.; Tosto-Mancuso, J.; Wood, J.; Cortes, M.; Kontorovich, A.; McCarthy, D.; Rizk, D.; Rozanski, G.; Breyman, E.; Nasr, L.; et al. Post-Acute COVID-19 Syndrome Negatively Impacts Physical Function, Cognitive Function, Health-Related Quality of Life, and Participation. Am. J. Phys. Med. Rehabil. 2022, 101, 48–52. [Google Scholar] [CrossRef]
- Xia, X.; Wang, Y.; Zheng, J. COVID-19 and Alzheimer’s Disease: How One Crisis Worsens the Other. Transl. Neurodegener. 2021, 10, 15. [Google Scholar] [CrossRef]
- Holwerda, T.J.; Deeg, D.J.H.; Beekman, A.T.F.; van Tilburg, T.G.; Stek, M.L.; Jonker, C.; Schoevers, R.A. Feelings of Loneliness, but Not Social Isolation, Predict Dementia Onset: Results from the Amsterdam Study of the Elderly (AMSTEL). J. Neurol. Neurosurg. Psychiatry 2014, 85, 135–142. [Google Scholar] [CrossRef]
- Scarlata, S.; Cardaci, V.; Santangelo, C.; Matarese, M.; Cesari, M.; Antonelli Incalzi, R. Distancing Measures in COVID-19 Pandemic: Loneliness, More than Physical Isolation, Affects Health Status and Psycho-Cognitive Wellbeing in Elderly Patients with Chronic Obstructive Pulmonary Disease. COPD 2021, 18, 443–448. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.-C.; Liu, S.; Gan, J.; Ma, L.; Du, X.; Zhu, H.; Han, J.; Xu, J.; Wu, H.; Fei, M.; et al. The Impact of the COVID-19 Pandemic and Lockdown on Mild Cognitive Impairment, Alzheimer’s Disease and Dementia With Lewy Bodies in China: A 1-Year Follow-Up Study. Front. Psychiatry 2021, 12, 711658. [Google Scholar] [CrossRef]
- Soysal, P.; Smith, L.; Trott, M.; Alexopoulos, P.; Barbagallo, M.; Tan, S.G.; Koyanagi, A.; Shenkin, S.; Veronese, N. European Society of Geriatric Medicine Special Interest Group in Dementia and Systematic Reviews and Meta-Analyses The Effects of COVID-19 Lockdown on Neuropsychiatric Symptoms in Patients with Dementia or Mild Cognitive Impairment: A Systematic Review and Meta-Analysis. Psychogeriatrics 2022, 22, 402–412. [Google Scholar] [CrossRef] [PubMed]
- Ginsberg, T.B.; Powell, L.; Emrani, S.; Wasserman, V.; Higgins, S.; Chopra, A.; Cavalieri, T.A.; Libon, D.J. Instrumental Activities of Daily Living, Neuropsychiatric Symptoms, and Neuropsychological Impairment in Mild Cognitive Impairment. J. Am. Osteopath. Assoc. 2019, 119, 96–101. [Google Scholar] [CrossRef] [PubMed]
- Covinsky, K.E.; Palmer, R.M.; Fortinsky, R.H.; Counsell, S.R.; Stewart, A.L.; Kresevic, D.; Burant, C.J.; Landefeld, C.S. Loss of Independence in Activities of Daily Living in Older Adults Hospitalized with Medical Illnesses: Increased Vulnerability with Age. J. Am. Geriatr. Soc. 2003, 51, 451–458. [Google Scholar] [CrossRef]
- Ehlenbach, W.J.; Hough, C.L.; Crane, P.K.; Haneuse, S.J.P.A.; Carson, S.S.; Curtis, J.R.; Larson, E.B. Association between Acute Care and Critical Illness Hospitalization and Cognitive Function in Older Adults. JAMA 2010, 303, 763–770. [Google Scholar] [CrossRef]
- Andrei Appelt, P.; Taciana Sisconetto, A.; Baldo Sucupira, K.S.M.; de Moura Neto, E.; de Jesus Chagas, T.; Bazan, R.; Moura Cabral, A.; de Oliveira Andrade, A.; de Souza, L.A.P.S.; José Luvizutto, G. Changes in Electrical Brain Activity and Cognitive Functions Following Mild to Moderate COVID-19: A One-Year Prospective Study After Acute Infection. Clin. EEG Neurosci. 2022, 53, 543–557. [Google Scholar] [CrossRef] [PubMed]
- Miners, S.; Kehoe, P.G.; Love, S. Cognitive Impact of COVID-19: Looking beyond the Short Term. Alzheimers Res. Ther. 2020, 12, 170. [Google Scholar] [CrossRef] [PubMed]
- van Lith, T.J.; Sluis, W.M.; Wijers, N.T.; Meijer, F.J.; Kamphuis-van Ulzen, K.; de Bresser, J.; Dankbaar, J.W.; van den Heuvel, F.M.; Antoni, M.L.; Mulders-Manders, C.M.; et al. Prevalence, Risk Factors, and Long-Term Outcomes of Cerebral Ischemia in Hospitalized COVID-19 Patients—Study Rationale and Protocol of the CORONIS Study: A Multicentre Prospective Cohort Study. Eur. Stroke J. 2022, 7, 180–187. [Google Scholar] [CrossRef]
- Calagnan, E.; Gobbato, M.; Burba, I.; Del Zotto, S.; Toffolutti, F.; Serraino, D.; Tonutti, G. COVID-19 Infections in the Friuli Venezia Giulia Region (Northern Italy): A Population-Based Retrospective Analysis. Epidemiol. Prev. 2020, 44, 323–329. [Google Scholar] [CrossRef] [PubMed]
- Moretti, R.; Caruso, P.; Giuffré, M.; Tiribelli, C. COVID-19 Lockdown Effect on Not Institutionalized Patients with Dementia and Caregivers. Healthcare 2021, 9, 893. [Google Scholar] [CrossRef]
- WHO. Laboratory Testing of 2019 Novel Coronavirus (2019-NCoV) in Suspected Human Cases: Interim Guidance; WHO: Geneva, Switzerland, 2020. [Google Scholar]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F.; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A New Equation to Estimate Glomerular Filtration Rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef]
- Postuma, R.B.; Berg, D.; Stern, M.; Poewe, W.; Olanow, C.W.; Oertel, W.; Obeso, J.; Marek, K.; Litvan, I.; Lang, A.E.; et al. MDS Clinical Diagnostic Criteria for Parkinson’s Disease. Mov. Disord. Off. J. Mov. Disord. Soc. 2015, 30, 1591–1601. [Google Scholar] [CrossRef]
- Doody, R.S.; Massman, P.; Dunn, J.K. A Method for Estimating Progression Rates in Alzheimer Disease. Arch. Neurol. 2001, 58, 449–454. [Google Scholar] [CrossRef] [Green Version]
- Reisberg, B. Diagnostic Criteria in Dementia: A Comparison of Current Criteria, Research Challenges, and Implications for DSM-V. J. Geriatr. Psychiatry Neurol. 2006, 19, 137–146. [Google Scholar] [CrossRef]
- Hugo, J.; Ganguli, M. Dementia and Cognitive Impairment: Epidemiology, Diagnosis, and Treatment. Clin. Geriatr. Med. 2014, 30, 421–442. [Google Scholar] [CrossRef] [Green Version]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-Mental State”. A Practical Method for Grading the Cognitive State of Patients for the Clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Magni, E.; Binetti, G.; Bianchetti, A.; Rozzini, R.; Trabucchi, M. Mini-Mental State Examination: A Normative Study in Italian Elderly Population. Eur. J. Neurol. 1996, 3, 198–202. [Google Scholar] [CrossRef]
- Katz, S.; Downs, T.D.; Cash, H.R.; Grotz, R.C. Progress in Development of the Index of ADL. Gerontologist 1970, 10, 20–30. [Google Scholar] [CrossRef] [PubMed]
- Lawton, M.P.; Brody, E.M. Assessment of Older People: Self-Maintaining and Instrumental Activities of Daily Living. Gerontologist 1969, 9, 179–186. [Google Scholar] [CrossRef] [PubMed]
- Fong, C.; Hazlett, C.; Imai, K. Covariate Balancing Propensity Score for a Continuous Treatment: Application to the Efficacy of Political Advertisements. Ann. Appl. Stat. 2018, 12, 156–177. [Google Scholar] [CrossRef] [Green Version]
- Clark, C.M.; Sheppard, L.; Fillenbaum, G.G.; Galasko, D.; Morris, J.C.; Koss, E.; Mohs, R.; Heyman, A.; the CERAD Investigators. Variability in Annual Mini-Mental State Examination Score in Patients With Probable Alzheimer Disease: A Clinical Perspective of Data From the Consortium to Establish a Registry for Alzheimer’s Disease. Arch. Neurol. 1999, 56, 857–862. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, Y.-H.; Wang, Y.-R.; Wang, Q.-H.; Chen, Y.; Chen, X.; Li, Y.; Cen, Y.; Xu, C.; Hu, T.; Liu, X.-D.; et al. Post-Infection Cognitive Impairments in a Cohort of Elderly Patients with COVID-19. Mol. Neurodegener. 2021, 16, 48. [Google Scholar] [CrossRef]
- Liu, Y.-H.; Chen, Y.; Wang, Q.-H.; Wang, L.-R.; Jiang, L.; Yang, Y.; Chen, X.; Li, Y.; Cen, Y.; Xu, C.; et al. One-Year Trajectory of Cognitive Changes in Older Survivors of COVID-19 in Wuhan, China: A Longitudinal Cohort Study. JAMA Neurol. 2022, 79, 509–517. [Google Scholar] [CrossRef]
- Weihe, S.; Mortensen, C.B.; Haase, N.; Andersen, L.P.K.; Mohr, T.; Siegel, H.; Ibsen, M.; Jørgensen, V.R.L.; Buck, D.L.; Pedersen, H.B.S.; et al. Long-Term Cognitive and Functional Status in Danish ICU Patients with COVID-19. Acta Anaesthesiol. Scand. 2022, 66, 978–986. [Google Scholar] [CrossRef]
- Latronico, N.; Peli, E.; Calza, S.; Rodella, F.; Novelli, M.P.; Cella, A.; Marshall, J.; Needham, D.M.; Rasulo, F.A.; Piva, S.; et al. Physical, Cognitive and Mental Health Outcomes in 1-Year Survivors of COVID-19-Associated ARDS. Thorax 2022, 77, 300–303. [Google Scholar] [CrossRef]
- de Medeiros, M.M.D.; Carletti, T.M.; Magno, M.B.; Maia, L.C.; Cavalcanti, Y.W.; Rodrigues-Garcia, R.C.M. Does the Institutionalization Influence Elderly’s Quality of Life? A Systematic Review and Meta–Analysis. BMC Geriatr. 2020, 20, 44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iyamu, I.; Plottel, L.; Snow, M.E.; Zhang, W.; Havaei, F.; Puyat, J.; Sawatzky, R.; Salmon, A. Culture Change in Long-Term Care-Post COVID-19: Adapting to a New Reality Using Established Ideas and Systems. Can. J. Aging Rev. Can. Vieil. 2022, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Borges-Machado, F.; Barros, D.; Ribeiro, Ó.; Carvalho, J. The Effects of COVID-19 Home Confinement in Dementia Care: Physical and Cognitive Decline, Severe Neuropsychiatric Symptoms and Increased Caregiving Burden. Am. J. Alzheimers Dis. Other Demen. 2020, 35, 1533317520976720. [Google Scholar] [CrossRef] [PubMed]
- Gan, J.; Liu, S.; Wu, H.; Chen, Z.; Fei, M.; Xu, J.; Dou, Y.; Wang, X.; Ji, Y. The Impact of the COVID-19 Pandemic on Alzheimer’s Disease and Other Dementias. Front. Psychiatry 2021, 12, 703481. [Google Scholar] [CrossRef] [PubMed]
- Vernuccio, L.; Sarà, D.; Inzerillo, F.; Catanese, G.; Catania, A.; Vesco, M.; Cacioppo, F.; Dominguez, L.J.; Veronese, N.; Barbagallo, M. Effect of COVID-19 Quarantine on Cognitive, Functional and Neuropsychiatric Symptoms in Patients with Mild Cognitive Impairment and Dementia. Aging Clin. Exp. Res. 2022, 34, 1187–1194. [Google Scholar] [CrossRef] [PubMed]
- Rainero, I.; Bruni, A.C.; Marra, C.; Cagnin, A.; Bonanni, L.; Cupidi, C.; Laganà, V.; Rubino, E.; Vacca, A.; Di Lorenzo, R.; et al. The Impact of COVID-19 Quarantine on Patients With Dementia and Family Caregivers: A Nation-Wide Survey. Front. Aging Neurosci. 2020, 12, 625781. [Google Scholar] [CrossRef]
- Douaud, G.; Lee, S.; Alfaro-Almagro, F.; Arthofer, C.; Wang, C.; McCarthy, P.; Lange, F.; Andersson, J.L.R.; Griffanti, L.; Duff, E.; et al. SARS-CoV-2 Is Associated with Changes in Brain Structure in UK Biobank. Nature 2022, 604, 697–707. [Google Scholar] [CrossRef] [PubMed]
- Yang, A.C.; Kern, F.; Losada, P.M.; Agam, M.R.; Maat, C.A.; Schmartz, G.P.; Fehlmann, T.; Stein, J.A.; Schaum, N.; Lee, D.P.; et al. Dysregulation of Brain and Choroid Plexus Cell Types in Severe COVID-19. Nature 2021, 595, 565–571. [Google Scholar] [CrossRef]
- Creditor, M.C. Hazards of hospitalization of the elderly. Ann. Intern. Med. 1993, 118, 219–223. [Google Scholar] [CrossRef]
- Starr, J.M.; Whalley, L.J. Drug-induced dementia. Incidence, management and prevention. Drug Saf. 1994, 11, 310–317. [Google Scholar] [CrossRef]
- Krogseth, M.; Wyller, T.B.; Engedal, K.; Juliebø, V. Delirium is a risk factor for institutionalization and functional decline in older hip fracture patients. J. Psychosom. Res. 2014, 76, 68–74. [Google Scholar] [CrossRef] [PubMed]
- Giostra, F.; Mirarchi, M.G.; Farina, G.; Paolillo, C.; Sepe, C.; Benedusi, F.; Bellone, A.; Ghiadoni, L.; Barbieri, G.; Santini, M.; et al. Impact of COVID-19 Pandemic and Lockdown on Emergency Room Access in Northern and Central Italy. Emerg. Care J. 2021, 17, 9705. [Google Scholar] [CrossRef]
- Petermann-Rocha, F.; Hanlon, P.; Gray, S.R.; Welsh, P.; Gill, J.M.R.; Foster, H.; Katikireddi, S.V.; Lyall, D.; Mackay, D.F.; O’Donnell, C.A.; et al. Comparison of two different frailty measurements and risk of hospitalisation or death from COVID-19: Findings from UK Biobank. BMC Med. 2020, 18, 355. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All | Without COVID-19 | With COVID-19 | p | |
|---|---|---|---|---|
| Patients (n) | 111 | 80 | 31 | - |
| Baseline variables | ||||
| Age (years) | 82 ± 5 | 82 ± 5 | 83 ± 5 | 0.315 |
| Male sex (n (%)) | 35 (32) | 24 (30) | 11 (36) | 0.651 |
| Hypertension (n (%)) | 66 (60) | 44 (55) | 22 (71) | 0.138 |
| Diabetes (n (%)) | 27 (24) | 15 (19) | 12 (39) | 0.047 |
| Dyslipidemia (n (%)) | 41 (37) | 30 (38) | 11 (36) | 1.000 |
| Cerebrovascular disease (n (%)) | 11 (9.9) | 8 (10) | 3 (9.7) | 1.000 |
| Cardiovascular disease (n (%)) | 37 (33) | 26 (33) | 11 (36) | 0.824 |
| Chronic kidney disease (n (%)) | 10 (9.0) | 7 (8.8) | 3 (9.7) | 1.000 |
| Parkinson’s disease (n (%)) | 7 (6.3) | 7 (8.8) | 0 | 0.187 |
| Self-sufficient (n (%)) | 26 (23) | 22 (28) | 4 (13) | 0.136 |
| Institutionalized (n (%)) | 7 (6.3) | 2 (2.5) | 5 (16) | 0.018 |
| Dementia type (n (%)): | 0.729 | |||
| 28 (25) | 21 (26) | 7 (23) | |
| 25 (23) | 19 (24) | 6 (19) | |
| 37 (33) | 24 (30) | 13 (42) | |
| 21 (19) | 16 (20) | 5 (16) | |
| BADL index | 5.0 [3.0, 5.5] | 5.0 [3, 6] | 3.0 [2, 4] | 0.006 |
| IADL index | 2.0 [1.0, 4.0] | 3.0 [1, 4] | 1.0 [0, 3] | 0.020 |
| MMSE score | 19.1 ± 5.0 | 19.8 ± 4.3 | 17.5 ± 6.3 | 0.027 |
| Total drugs number | 4.0 [2.0, 6.0] | 3.5 [2.0, 6.0] | 5.0 [3.0, 6.0] | 0.107 |
| Memantine (n (%)) | 5 (4.5) | 4 (5.0) | 1 (3.2) | 1.000 |
| Anticholinergic drug (n (%)) | 17 (15) | 11 (14) | 6 (19) | 0.558 |
| Antipsychotic drug (n (%)) | 22 (20) | 15 (19) | 7 (23) | 0.791 |
| Antidepressant drug (n (%)) | 23 (21) | 16 (20) | 7 (23) | 0.797 |
| Benzodiazepines (n (%)) | 21 (19) | 16 (20) | 5 (16) | 0.790 |
| Follow-up variables | ||||
| Follow-up time (years) | 1.1 [0.7–1.7] | 1.2 [0.8, 1.9] | 0.9 [0.6, 1.2] | 0.013 |
| Change in MMSE score | −3.0 [−6.8, −1.4] | −2.7 [−5.8, −1.0] | −6.0 [−10, −3.2] | 0.002 |
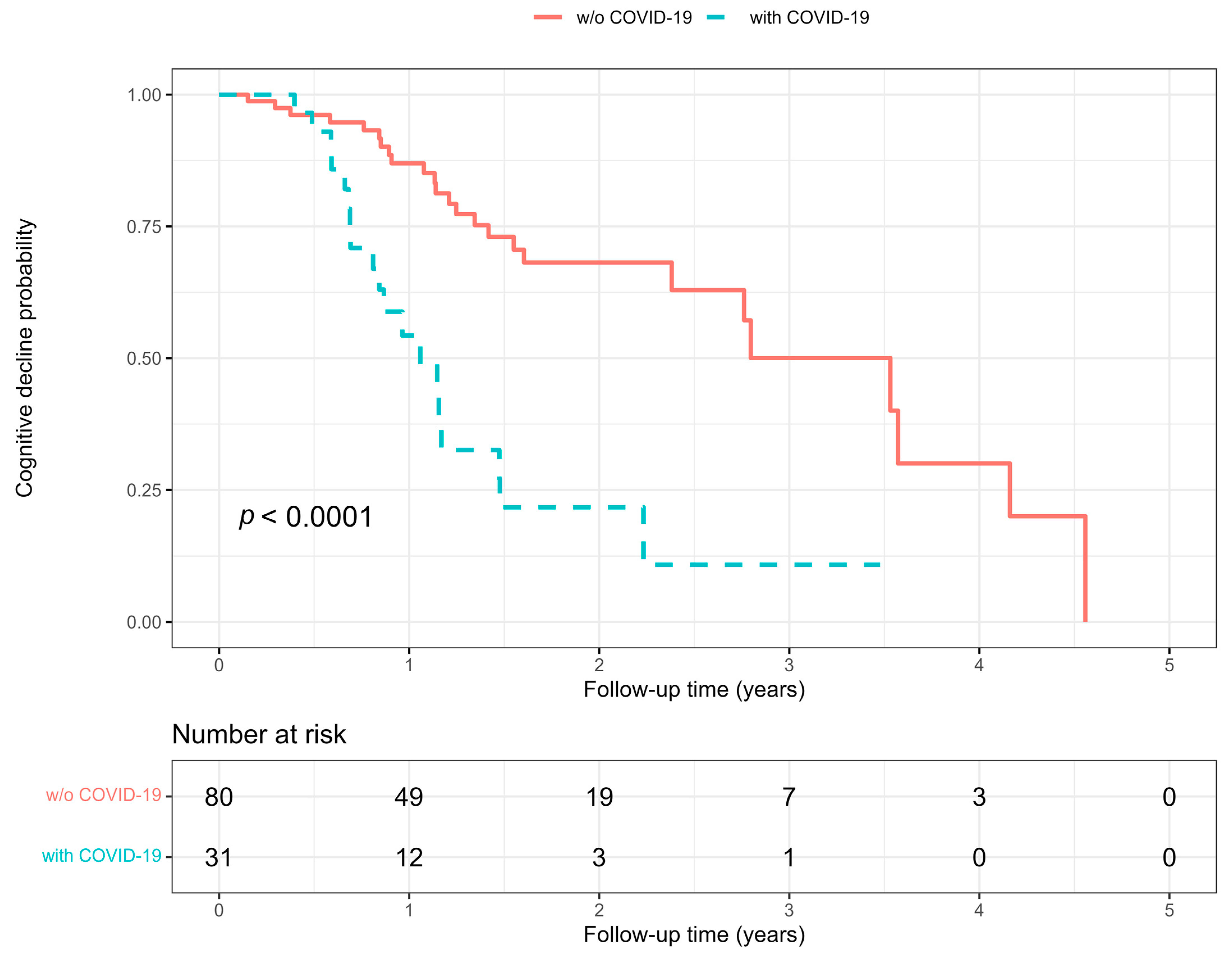
| Significant cognitive decline (n (%)) | 44 (40) | 25 (31) | 19 (61) | 0.005 |
| Change in BADL index | −1.0 [−2.0, 0.0] | −1.0 [−2.0, 0.0] | −1.0 [−2.0, 0.0] | 0.848 |
| Change in IADL index | −1.0 [−2.5, 0.0] | −1.0 [−3.0, 0.0] | −1.0 [−2.0, 0.0] | 0.235 |
| Hospitalization for any cause (n (%)) | 6 (5.4) | 0 | 6 (19) | <0.001 |
| New institutionalization (n (%)) | 30 (27) | 16 (20) | 14 (45) | 0.016 |
| Without Cognitive Decline | With Cognitive Decline | p | |
|---|---|---|---|
| Patients (n) | 67 | 44 | - |
| Baseline variables | |||
| Age (years) | 82 ± 5 | 82 ± 6 | 0.734 |
| Male sex (n (%)) | 19 (28) | 16 (36) | 0.409 |
| Hypertension (n (%)) | 38 (57) | 28 (64) | 0.555 |
| Diabetes (n (%)) | 14 (21) | 13 (30) | 0.367 |
| Dyslipidemia (n (%)) | 26 (39) | 15 (34) | 0.690 |
| Cerebrovascular disease (n (%)) | 4 (6.0) | 7 (16) | 0.109 |
| Cardiovascular disease (n (%)) | 23 (34) | 14 (32) | 0.839 |
| Chronic kidney disease (n (%)) | 5 (7.5) | 5 (11) | 0.514 |
| Parkinson’s disease (n (%)) | 4 (6.0) | 3 (6.8) | 1.000 |
| Self-sufficient (n (%)) | 21 (31) | 5 (11) | 0.021 |
| Institutionalized (n (%)) | 3 (4.5) | 4 (9.1) | 0.432 |
| Dementia type (n (%)) | 0.808 | ||
| 18 (27) | 10 (23) | |
| 13 (19) | 12 (28) | |
| 23 (34) | 14 (32) | |
| 13 (19) | 8 (18) | |
| MMSE score | 18.8 ± 4.4 | 19.6 ± 5.7 | 0.390 |
| BADL index | 5.0 [3.0, 5.5] | 4.5 [3.0, 5.25] | 0.963 |
| IADL index | 2.0 [1.0, 5.0] | 2.0 [1.0, 4.0] | 0.552 |
| Total drugs number (n) | 4.0 [2.0, 6.0] | 4.0 [2.0, 6.0] | 0.340 |
| Memantine (n (%)) | 1 (1.5) | 4 (9.1) | 0.079 |
| Anticholinergic drug (n (%)) | 10 (15) | 7 (16) | 1.000 |
| Antipsychotic drug (n (%)) | 14 (21) | 8 (18) | 0.811 |
| Antidepressant drug (n (%)) | 14 (21) | 9 (21) | 1.000 |
| Benzodiazepine drug (n (%)) | 14 (21) | 7 (16) | 0.623 |
| Follow-up variables | |||
| COVID-19 (n (%)) | 12 (18) | 19 (43) | 0.005 |
| Follow-up time (years) | 1.1 [0.8, 1.8] | 1.1 [0.7, 1.5] | 0.602 |
| Change in MMSE score | −2.0 [−3.0, 0.0] | −8.2 [−10.1, −6.0] | <0.001 |
| Change in BADL index | 0.0 [−1.0, 0.0] | −1.0 [−2.25, 0.0] | 0.001 |
| Change in IADL index | −1.0 [−2.0, 0.0] | −1.0 [−3.0, −1.0] | 0.192 |
| Hospitalization for any cause (n (%)) | 1 (1.5) | 5 (11) | 0.035 |
| New institutionalization (n (%)) | 14 (21) | 16 (36) | 0.084 |
| COVID-19 | Cognitive Decline | |||
|---|---|---|---|---|
| Variable | HR (95% CI) | p | HR (95% CI) | p |
| Age (every 10 years) | 1.43 (0.73, 2.80) | 0.293 | 0.98 (0.56–1.71) | 0.936 |
| Male sex (yes/no) | 1.39 (0.66, 2.91) | 0.382 | 1.62 (0.86, 3.02) | 0.133 |
| Hypertension (yes/no) | 2.12 (0.97, 4.63) | 0.059 | 1.77 (0.94, 3.33) | 0.078 |
| Diabetes (yes/no) | 2.31 (1.11, 4.78) | 0.025 | 1.38 (0.71, 2.67) | 0.344 |
| Dyslipidemia (yes/no) | 0.99 (0.47, 2.09) | 0.988 | 1.07 (0.56, 2.03) | 0.841 |
| Cerebrovascular disease (yes/no) | 1.00 (0.30, 3.30) | 0.994 | 2.28 (0.99, 5.25) | 0.053 |
| Cardiovascular disease (yes/no) | 1.29 (0.62, 2.69) | 0.503 | 1.17 (0.61, 2.23) | 0.635 |
| Chronic kidney disease (yes/no) | 1.06 (032, 3.52) | 0.919 | 1.62 (0.63, 4.17) | 0.319 |
| Parkinson’s disease (yes/no) | - | - | 0.98 (0.30, 3.22) | 0.973 |
| Self-sufficient (yes/no) | 0.46 (0.16, 1.32) | 0.148 | 0.42 (0.17, 1.08) | 0.073 |
| Institutionalized (yes/no) | 2.86 (1.10, 7.48) | 0.032 | 1.69 (0.60, 4.79) | 0.320 |
| Dementia type (yes/no): | ||||
| 1.00 | - | 1.00 | - |
| 0.99 (0.33, 2.93) | 0.980 | 1.52 (0.65, 3.54) | 0.331 |
| 1.58 (0.63, 3.97) | 0.329 | 1.33 (0.58, 3.02) | 0.498 |
| 0.84 (0.26, 2.64) | 0.759 | 0.68 (0.26, 1.80) | 0.434 |
| BADL (every 1 point) | 0.66 (0.51, 0.85) | 0.001 | 0.79 (0.64, 0.99) | 0.039 |
| IADL (every 1 point) | 0.80 (0.67, 0.96) | 0.014 | 0.86 (0.75, 0.98) | 0.026 |
| MMSE score (every 1 point) | 0.92 (0.86, 0.99) | 0.024 | 0.98 (0.92, 1.04) | 0.548 |
| New institutionalization (yes/no) | - | - | 1.71 (0.91, 3.20) | 0.096 |
| Drug numbers (every 1 drug) | 1.15 (1.00, 1.32) | 0.054 | 1.13 (1.01, 1.27) | 0.038 |
| Memantine (yes/no) | 0.83 (0.11, 6.12) | 0.853 | 4.13 (1.42, 12.0) | 0.009 |
| Anticholinergic drug (yes/no) | 1.63 (0.66, 4.01) | 0.290 | 1.83 (0.79, 4.21) | 0.157 |
| Antipsychotic drug (yes/no) | 1.43 (0.61, 3.34) | 0.412 | 1.48 (0.67, 3.23) | 0.330 |
| Antidepressant drug (yes/no) | 1.25 (0.54, 2.92) | 0.604 | 1.30 (0.62, 2.76) | 0.487 |
| Anxiolytic drug (yes/no) | 0.78 (0.30, 2.04) | 0.616 | 0.67 (0.28, 1.60) | 0.368 |
| COVID-19 (yes/no) | - | - | 3.94 (2.09, 7.43) | <0.001 |
| Hospitalization for any cause (yes/no) | - | - | 4.10 (1.59, 10.6) | 0.003 |
| Dependent Variable | |||
|---|---|---|---|
| MMSE Score | Basic ADL | Instrumental ADL | |
| Independent Variable | Estimate (95% CI) | Estimate (95% CI) | Estimate (95% CI) |
| A | |||
| COVID-19 (yes/no) | −3.1 (−5.4, −0.9) ** | −0.9 (−1.5, −0.2) ** | −1.0 (−1.9, −0.2) * |
| Follow-up (year) | −1.7 (−2.3, −1.1) *** | −0.5 (−0.7, −0.4) *** | −0.8 (−1.0, −0.6) *** |
| COVID x Follow-up | −1.6 (−3.0, −0.2) * | −0.2 (−0.6, 0.2) | −0.1 (−0.6, 0.4) |
| B | |||
| COVID-19 (yes/no) | −3.4 (−5.7, −1.0) ** | −0.8 (−1.5, −0.1) * | −1.0 (−1.9, −0.05) * |
| Follow-up (year) | −1.7 (−2.2, −1.1) *** | −0.5 (−0.7, −0.4) *** | −0.8 (−1.0, −0.6) *** |
| COVID x Follow-up | −1.5 (−2.9, −0.06) * | −0.2 (−0.6, 0.2) | −0.1 (−0.6, 0.4) |
| C | |||
| COVID-19 (yes/no) | −1.6 (−3.9, 0.7) | −0.6 (−1.3, 0.1) | −0.7 (−1.7, 0.3) |
| Follow-up (year) | −1.7 (−2.2, −1.1) *** | −0.5 (−0.7, −0.4) *** | −0.8 (−1.0, −0.6) *** |
| COVID x Follow-up | −1.5 (−2.9, −0.08) * | −0.2 (−0.6, 0.2) | −0.1 (−0.6, 0.4) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Merla, L.; Montesi, M.C.; Ticali, J.; Bais, B.; Cavarape, A.; Colussi, G. COVID-19 Accelerated Cognitive Decline in Elderly Patients with Pre-Existing Dementia Followed up in an Outpatient Memory Care Facility. J. Clin. Med. 2023, 12, 1845. https://doi.org/10.3390/jcm12051845
Merla L, Montesi MC, Ticali J, Bais B, Cavarape A, Colussi G. COVID-19 Accelerated Cognitive Decline in Elderly Patients with Pre-Existing Dementia Followed up in an Outpatient Memory Care Facility. Journal of Clinical Medicine. 2023; 12(5):1845. https://doi.org/10.3390/jcm12051845
Chicago/Turabian StyleMerla, Lucia, Maria Cristina Montesi, Jessica Ticali, Bruno Bais, Alessandro Cavarape, and GianLuca Colussi. 2023. "COVID-19 Accelerated Cognitive Decline in Elderly Patients with Pre-Existing Dementia Followed up in an Outpatient Memory Care Facility" Journal of Clinical Medicine 12, no. 5: 1845. https://doi.org/10.3390/jcm12051845