
Effects of Tele-Pilates and Tele-Yoga on Biochemicals, Physical, and Psychological Parameters of Females with Multiple Sclerosis
 , ,
, ,
Abstract
:1. Introduction
2. Methodology
2.1. Trial Design
2.2. Participants
2.3. Intervention
2.3.1. Tele-Yoga
2.3.2. Tele-Pilates
2.3.3. Control Min
2.4. Outcomes
2.4.1. Blood Samples Analysis
2.4.2. Depression
2.4.3. Mental Health
2.4.4. Physical Activity Levels
2.4.5. Timed 25-Foot Walk (T25FW)
2.4.6. Quality of Life (QoL)
2.5. Sample Size
2.6. Randomization
2.7. Data Analysis
3. Results
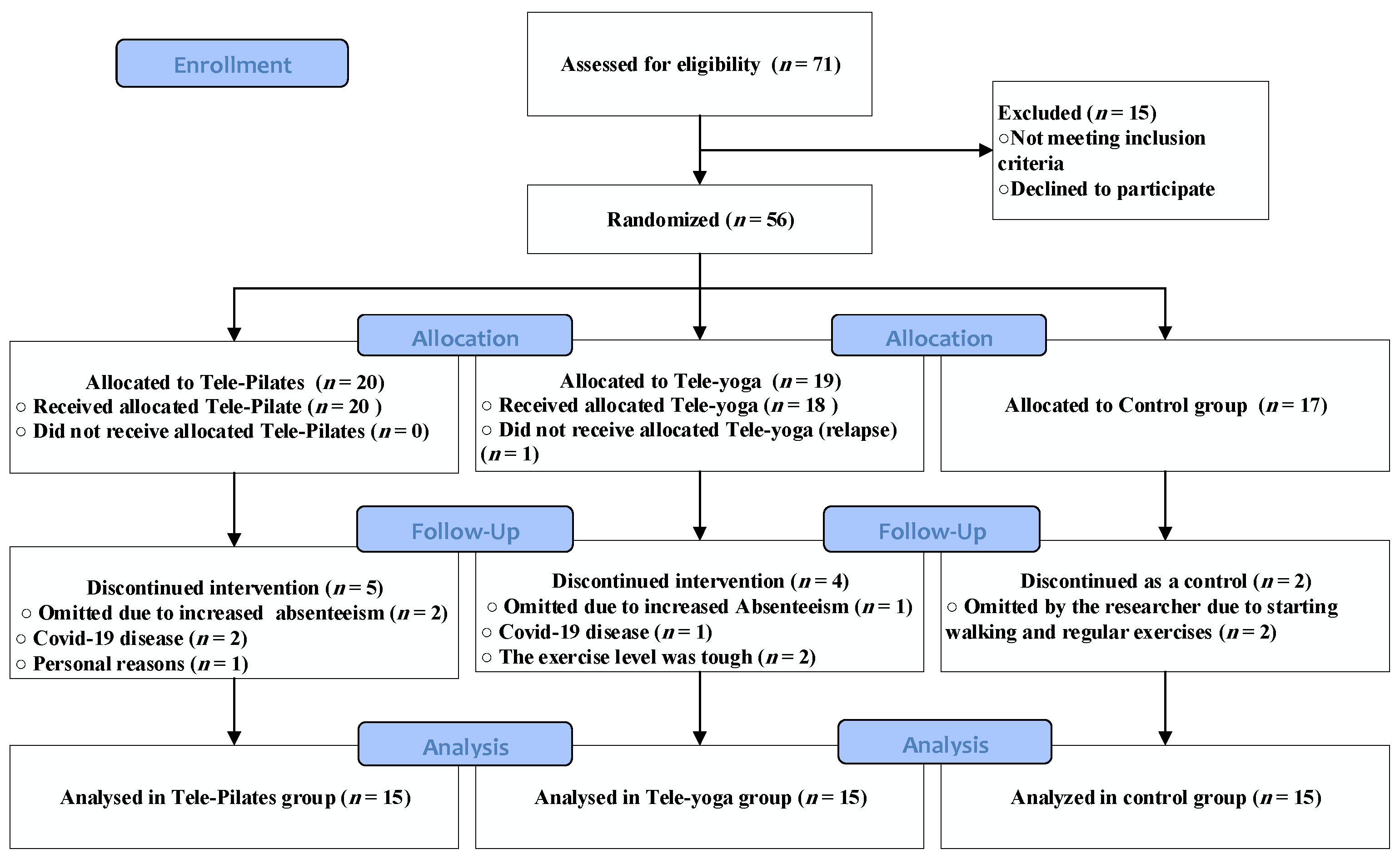
3.1. Characteristics of Feasibility
3.2. Outcomes and Estimations
3.2.1. Resting and Post-Exercise Serum Prolactin Levels
3.2.2. Resting and Post-Exercise Serum Cortisol Levels
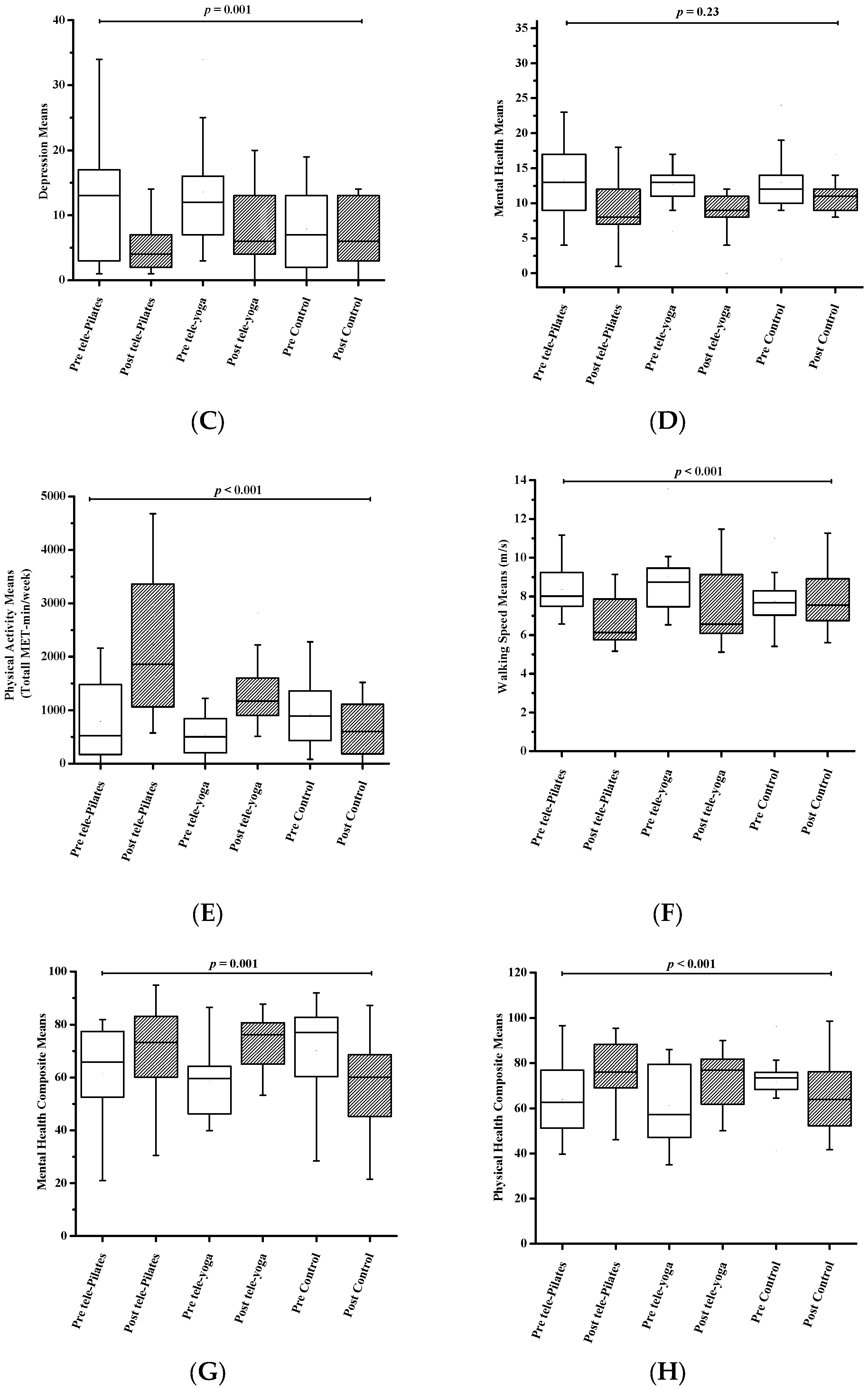
3.2.3. Depression
3.2.4. Mental Health
3.2.5. Physical Activity
3.2.6. Timed 25-Foot Walk
3.2.7. Quality of Life (QoL)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Najafi, P.; Hadizadeh, M.; Cheong, J.P.G.; Mohafez, H.; Abdullah, S. Cytokine Profile in Patients with Multiple Sclerosis Following Exercise: A Systematic Review of Randomized Clinical Trials. Int. J. Environ. Res. Public Health 2022, 19, 8151. [Google Scholar] [CrossRef] [PubMed]
- Grazioli, E.; Tranchita, E.; Borriello, G.; Cerulli, C.; Minganti, C.; Parisi, A. The effects of concurrent resistance and aerobic exercise training on functional status in patients with multiple sclerosis. Curr. Sport. Med. Rep. 2019, 18, 452–457. [Google Scholar] [CrossRef] [PubMed]
- Anagnostouli, M.; Markoglou, N.; Chrousos, G. Psycho-neuro-endocrino-immunologic issues in multiple sclerosis: A critical review of clinical and therapeutic implications. Hormones 2020, 19, 485–496. [Google Scholar] [CrossRef] [PubMed]
- Ysrraelit, M.C.; Correale, J. Impact of sex hormones on immune function and multiple sclerosis development. Immunology 2019, 156, 9–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pereira, G.M.; Becker, J.; Soares, N.M.; de Azeredo, L.A.; Grassi-Oliveira, R.; Rysdyk, A.; de Almeida, R.M.M. Hair cortisol concentration, cognitive, behavioral, and motor impairment in multiple sclerosis. J. Neural Transm. 2019, 126, 1145–1154. [Google Scholar] [CrossRef]
- Borba, V.V.; Zandman-Goddard, G.; Shoenfeld, Y. Prolactin and autoimmunity: The hormone as an inflammatory cytokine. Best Pract. Res. Clin. Endocrinol. Metab. 2019, 33, 101324. [Google Scholar] [CrossRef]
- Costanza, M.; Binart, N.; Steinman, L.; Pedotti, R. Prolactin: A versatile regulator of inflammation and autoimmune pathology. Autoimmun. Rev. 2015, 14, 223–230. [Google Scholar] [CrossRef]
- Costanza, M.; Pedotti, R. Prolactin: Friend or foe in central nervous system autoimmune inflammation? Int. J. Mol. Sci. 2016, 17, 2026. [Google Scholar] [CrossRef] [Green Version]
- Azar, S.T.; Yamout, B. Prolactin secretion is increased in patients with multiple sclerosis. Endocr. Res. 1999, 25, 207–214. [Google Scholar] [CrossRef]
- Correale, J.; Farez, M.F.; Ysrraelit, M.C. Role of prolactin in B cell regulation in multiple sclerosis. J. Neuroimmunol. 2014, 269, 76–86. [Google Scholar] [CrossRef]
- Hackney, A.C.; Saeidi, A. The thyroid axis, prolactin, and exercise in humans. Curr. Opin. Endocr. Metab. Res. 2019, 9, 45–50. [Google Scholar] [CrossRef] [PubMed]
- Eftekhari, E.; Etemadifar, M.; Mostahfezian, M.; Zafari, A. Effects of resistance training and vibration on hormonal changes in female patients with multiple sclerosis. Neurol. Asia 2014, 19, 63–67. [Google Scholar]
- Avandi, M.; Heidarian, A.; Ebrahimi, M. The effects of eight week yoga training on serum levels of Dehydroepiandrestrone sulfate and prolactin in women with multiple sclerosis. Int. J. Appl. Exerc. Physiol. 2017, 6, 8–13. [Google Scholar] [CrossRef] [Green Version]
- Powell, D.J.; Moss-Morris, R.; Liossi, C.; Schlotz, W. Circadian cortisol and fatigue severity in relapsing-remitting multiple sclerosis. Psychoneuroendocrinology 2015, 56, 120–131. [Google Scholar] [CrossRef] [PubMed]
- Pereira, G.M.; Soares, N.M.; Souza, A.R.d.; Becker, J.; Finkelsztejn, A.; Almeida, R.M.M.d. Basal cortisol levels and the relationship with clinical symptoms in multiple sclerosis: A systematic review. Arq. Neuro-Psiquiatr. 2018, 76, 622–634. [Google Scholar] [CrossRef] [Green Version]
- Dziurkowska, E.; Wesolowski, M. Cortisol as a biomarker of mental disorder severity. J. Clin. Med. 2021, 10, 5204. [Google Scholar] [CrossRef]
- Kern, S.; Schultheiss, T.; Schneider, H.; Schrempf, W.; Reichmann, H.; Ziemssen, T. Circadian cortisol, depressive symptoms and neurological impairment in early multiple sclerosis. Psychoneuroendocrinology 2011, 36, 1505–1512. [Google Scholar] [CrossRef]
- Gold, S.M.; Krüger, S.; Ziegler, K.J.; Krieger, T.; Schulz, K.-H.; Otte, C.; Heesen, C. Endocrine and immune substrates of depressive symptoms and fatigue in multiple sclerosis patients with comorbid major depression. J. Neurol. Neurosurg. Psychiatry 2011, 82, 814–818. [Google Scholar] [CrossRef] [Green Version]
- Sajedi, D.; Shabani, R.; Elmieh, A. Changes in leptin, serotonin, and cortisol after eight weeks of aerobic exercise with probiotic intake in a cuprizone-induced demyelination mouse model of multiple sclerosis. Cytokine 2021, 144, 155590. [Google Scholar] [CrossRef]
- Kraemer, W.J.; Ratamess, N.A.; Hymer, W.C.; Nindl, B.C.; Fragala, M.S. Growth hormone (s), testosterone, insulin-like growth factors, and cortisol: Roles and integration for cellular development and growth with exercise. Front. Endocrinol. 2020, 11, 33. [Google Scholar] [CrossRef]
- Najafi, P.; Moghadasi, M. The effect of yoga training on enhancement of Adrenocorticotropic hormone (ACTH) and cortisol levels in female patients with multiple sclerosis. Complement. Ther. Clin. Pract. 2017, 26, 21–25. [Google Scholar] [CrossRef] [PubMed]
- Motl, R.W. Exercise and multiple sclerosis. Phys. Exerc. Hum. Health 2020, 34, 1077–1100. [Google Scholar]
- Campbell, E.; Coulter, E.H.; Paul, L. High intensity interval training for people with multiple sclerosis: A systematic review. Mult. Scler. Relat. Disord. 2018, 24, 55–63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Akbar, N.; Sandroff, B.M.; Wylie, G.R.; Strober, L.B.; Smith, A.; Goverover, Y.; Motl, R.W.; DeLuca, J.; Genova, H. Progressive resistance exercise training and changes in resting-state functional connectivity of the caudate in persons with multiple sclerosis and severe fatigue: A proof-of-concept study. Neuropsychol. Rehabil. 2020, 30, 54–66. [Google Scholar] [CrossRef] [PubMed]
- Halabchi, F.; Alizadeh, Z.; Sahraian, M.A.; Abolhasani, M. Exercise prescription for patients with multiple sclerosis; potential benefits and practical recommendations. BMC Neurol. 2017, 17, 185. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alphonsus, K.B.; Su, Y.; D’Arcy, C. The effect of exercise, yoga and physiotherapy on the quality of life of people with multiple sclerosis: Systematic review and meta-analysis. Complement. Ther. Med. 2019, 43, 188–195. [Google Scholar] [CrossRef]
- Khayat-Khoei, M.; Bhattacharyya, S.; Katz, J.; Harrison, D.; Tauhid, S.; Bruso, P.; Houtchens, M.K.; Edwards, K.R.; Bakshi, R. COVID-19 mRNA vaccination leading to CNS inflammation: A case series. J. Neurol. 2021, 269, 1093–1106. [Google Scholar] [CrossRef]
- Mares, J.; Hartung, H. Multiple sclerosis and COVID-19. Biomed. Pap. Med. Fac. Univ. Palacky Olomouc. Czech Repub. 2020, 164, 1–9. [Google Scholar] [CrossRef]
- Motl, R.W.; Sandroff, B.M.; Kwakkel, G.; Dalgas, U.; Feinstein, A.; Heesen, C.; Feys, P.; Thompson, A.J. Exercise in patients with multiple sclerosis. Lancet Neurol. 2017, 16, 848–856. [Google Scholar] [CrossRef] [PubMed]
- Andreu-Caravaca, L.; Ramos-Campo, D.J.; Chung, L.H.; Manonelles, P.; Abellán-Aynés, O.; Rubio-Arias, J.Á. The impact of COVID-19 home confinement on neuromuscular performance, functional capacity, and psychological state in Spanish people with Multiple Sclerosis. Mult. Scler. Relat. Disord. 2021, 53, 103047. [Google Scholar] [CrossRef] [PubMed]
- Carotenuto, A.; Scandurra, C.; Costabile, T.; Lavorgna, L.; Borriello, G.; Moiola, L.; Inglese, M.; Trojsi, F.; Petruzzo, M.; Ianniello, A. Physical exercise moderates the effects of disability on depression in people with multiple sclerosis during the COVID-19 outbreak. J. Clin. Med. 2021, 10, 1234. [Google Scholar] [CrossRef]
- Amatya, B.; Galea, M.P.; Kesselring, J.; Khan, F. Effectiveness of telerehabilitation interventions in persons with multiple sclerosis: A systematic review. Mult. Scler. Relat. Disord. 2015, 4, 358–369. [Google Scholar] [CrossRef]
- Lai, B.; Chiu, C.-Y.; Pounds, E.; Tracy, T.; Mehta, T.; Young, H.-J.; Riser, E.; Rimmer, J. COVID-19 modifications for remote teleassessment and teletraining of a complementary alternative medicine intervention for people with multiple sclerosis: Protocol for a randomized controlled trial. JMIR Res. Protoc. 2020, 9, e18415. [Google Scholar] [CrossRef] [PubMed]
- Abasıyanık, Z.; Ertekin, Ö.; Kahraman, T.; Yigit, P.; Özakbaş, S. The effects of Clinical Pilates training on walking, balance, fall risk, respiratory, and cognitive functions in persons with multiple sclerosis: A randomized controlled trial. Explore 2020, 16, 12–20. [Google Scholar] [CrossRef] [PubMed]
- Abasıyanık, Z.; Yiğit, P.; Özdoğar, A.T.; Kahraman, T.; Ertekin, Ö.; Özakbaş, S. A comparative study of the effects of yoga and clinical Pilates training on walking, cognition, respiratory functions, and quality of life in persons with multiple sclerosis: A quasi-experimental study. Explore 2021, 17, 424–429. [Google Scholar] [CrossRef] [PubMed]
- Thompson, A.J.; Banwell, B.L.; Barkhof, F.; Carroll, W.M.; Coetzee, T.; Comi, G.; Correale, J.; Fazekas, F.; Filippi, M.; Freedman, M.S. Diagnosis of multiple sclerosis: 2017 revisions of the McDonald criteria. Lancet Neurol. 2018, 17, 162–173. [Google Scholar] [CrossRef]
- Ghaem, H.; Haghighi, A.B.; Jafari, P.; Nikseresht, A. Validity and reliability of the Persian version of the multiple sclerosis quality of life questionnaire. Neurol. India 2007, 55, 369. [Google Scholar] [CrossRef]
- Fattahi, M.-R.; Noormohammadpour, P.; Ramezani, M.; Sahraian, M.A.; Mansournia, M.A.; Tabesh, M.R.; Mesgarof, M.A.; Abolhasani, M. Translation and validation of the Persian version of Godin Leisure-Time Exercise Questionnaire in patients with multiple sclerosis. BMC Neurol. 2021, 21, 431. [Google Scholar] [CrossRef]
- Abhari, M.B.; Fisher, J.W.; Kheiltash, A.; Nojomi, M. Validation of the Persian version of spiritual well-being questionnaires. Iran. J. Med. Sci. 2018, 43, 276. [Google Scholar]
- Ghajarzadeh, M.; Jalilian, R.; Eskandari, G.; Ali Sahraian, M.; Reza Azimi, A. Validity and reliability of Persian version of Modified Fatigue Impact Scale (MFIS) questionnaire in Iranian patients with multiple sclerosis. Disabil. Rehabil. 2013, 35, 1509–1512. [Google Scholar] [CrossRef]
- Ayatollahi, P.; Nafissi, S.; Eshraghian, M.; Kaviani, H.; Tarazi, A. Impact of depression and disability on quality of life in Iranian patients with multiple sclerosis. Mult. Scler. J. 2007, 13, 275–277. [Google Scholar] [CrossRef] [PubMed]
- Armeni, E.; Delialis, D.; Georgiopoulos, G.; Augoulea, A.; Stergiotis, S.; Kontou, L.; Chatzivasileiou, P.; Rizos, D.; Kaparos, G.; Baka, S. Serum prolactin levels interact with menstrual fluctuations of arterial stiffness. Hell. J. Cardiol. HJC Hellenike Kardiologike Epitheorese 2021, 63, 89–91. [Google Scholar] [CrossRef] [PubMed]
- Alwakil, H.A.; Al-Malt, A.M.; Ragab, O.A.; Ghafar, M.T.A.; Tageldin, E.A. Serum prolactin in patients with relapsing remitting multiple sclerosis. Egypt. J. Neurol. Psychiatry Neurosurg. 2020, 56, 77. [Google Scholar] [CrossRef]
- Zych-Twardowska, E.; Wajgt, A. Serum prolactin and sex hormone concentrations in patients with multiple sclerosis. Med. Sci. Monit. 1999, 5, CR216–CR220. [Google Scholar]
- De Giglio, L.; Marinelli, F.; Prosperini, L.; Contessa, G.; Gurreri, F.; Piattella, M.; De Angelis, F.; Barletta, V.; Tomassini, V.; Pantano, P. Relationship between prolactin plasma levels and white matter volume in women with multiple sclerosis. Mediat. Inflamm. 2015, 2015, 732539. [Google Scholar] [CrossRef] [PubMed]
- Castellano, V.; Patel, D.I.; White, L.J. Cytokine responses to acute and chronic exercise in multiple sclerosis. J. Appl. Physiol. 2008, 104, 1697–1702. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Negaresh, R.; Motl, R.W.; Mokhtarzade, M.; Dalgas, U.; Patel, D.; Shamsi, M.M.; Majdinasab, N.; Ranjbar, R.; Zimmer, P.; Baker, J.S. Effects of exercise training on cytokines and adipokines in multiple sclerosis: A systematic review. Mult. Scler. Relat. Disord. 2018, 24, 91–100. [Google Scholar] [CrossRef] [Green Version]
- Benedict, R.H.; Fishman, I.; McClellan, M.; Bakshi, R.; Weinstock-Guttman, B. Validity of the beck depression inventory-fast screen in multiple sclerosis. Mult. Scler. J. 2003, 9, 393–396. [Google Scholar] [CrossRef]
- Beck, A.T.; Ward, C.; Mendelson, M.; Mock, J.; Erbaugh, J. Beck depression inventory (BDI). Arch. Gen. Psychiatry 1961, 4, 561–571. [Google Scholar] [CrossRef] [Green Version]
- Anjara, S.; Bonetto, C.; Van Bortel, T.; Brayne, C. Using the GHQ-12 to screen for mental health problems among primary care patients: Psychometrics and practical considerations. Int. J. Ment. Health Syst. 2020, 14, 1–13. [Google Scholar] [CrossRef]
- Goldberg, D.P.; Gater, R.; Sartorius, N.; Ustun, T.B.; Piccinelli, M.; Gureje, O.; Rutter, C. The validity of two versions of the GHQ in the WHO study of mental illness in general health care. Psychol. Med. 1997, 27, 191–197. [Google Scholar] [CrossRef] [PubMed]
- Sparaco, M.; Lavorgna, L.; Bonavita, S. Psychiatric disorders in multiple sclerosis. J. Neurol. 2021, 268, 45–60. [Google Scholar] [CrossRef] [PubMed]
- Van Holle, V.; De Bourdeaudhuij, I.; Deforche, B.; Van Cauwenberg, J.; Van Dyck, D. Assessment of physical activity in older Belgian adults: Validity and reliability of an adapted interview version of the long International Physical Activity Questionnaire (IPAQ-L). BMC Public Health 2015, 15, 433. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ainsworth, B.E.; Haskell, W.L.; Whitt, M.C.; Irwin, M.L.; Swartz, A.M.; Strath, S.J.; O Brien, W.L.; Bassett, D.R.; Schmitz, K.H.; Emplaincourt, P.O. Compendium of physical activities: An update of activity codes and MET intensities. Med. Sci. Sport. Exerc. 2000, 32, S498–S504. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heiskanen, S.; Meriläinen, P.; Pietilä, A.M. Health-related quality of life–testing the reliability of the MSQOL-54 instrument among MS patients. Scand. J. Caring Sci. 2007, 21, 199–206. [Google Scholar] [CrossRef]
- Simeoni, M.; Auquier, P.; Fernandez, O.; Flachenecker, P.; Stecchi, S.; Constantinescu, C.; Idiman, E.; Boyko, A.; Beiske, A.; Vollmer, T. Validation of the multiple sclerosis international quality of life questionnaire. Mult. Scler. J. 2008, 14, 219–230. [Google Scholar] [CrossRef]
- Ochoa-Morales, A.; Hernández-Mojica, T.; Paz-Rodríguez, F.; Jara-Prado, A.; Trujillo-De Los Santos, Z.; Sánchez-Guzmán, M.; Guerrero-Camacho, J.; Corona-Vázquez, T.; Flores, J.; Camacho-Molina, A. Quality of life in patients with multiple sclerosis and its association with depressive symptoms and physical disability. Mult. Scler. Relat. Disord. 2019, 36, 101386. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Hillsdale, L., Ed.; Routledge: Oxfordshire, UK, 1988. [Google Scholar]
- Ahmadi, A.; Arastoo, A.A.; Nikbakht, M.; Zahednejad, S.; Rajabpour, M. Comparison of the effect of 8 weeks aerobic and yoga training on ambulatory function, fatigue and mood status in MS patients. Iran. Red Crescent Med. J. 2013, 15, 449. [Google Scholar] [CrossRef] [Green Version]
- Öztuna, D.; Elhan, A.H.; Tüccar, E. Investigation of four different normality tests in terms of type 1 error rate and power under different distributions. Turk. J. Med. Sci. 2006, 36, 171–176. [Google Scholar]
- Ghasemi, A.; Zahediasl, S. Normality tests for statistical analysis: A guide for non-statisticians. Int. J. Endocrinol. Metab. 2012, 10, 486. [Google Scholar] [CrossRef] [Green Version]
- Samperi, I.; Lithgow, K.; Karavitaki, N. Hyperprolactinaemia. J. Clin. Med. 2019, 8, 2203. [Google Scholar] [CrossRef] [Green Version]
- Goud, S.; Thar, Y.Y. SAT-676 Pembrolizumab Induced Worsening Glycemic Control and DKA in Type 2 Diabetes Mellitus. J. Endocr. Soc. 2020, 4, SAT-676. [Google Scholar] [CrossRef]
- Belal, T.; El-Mitwalli, A.; El-Diasty, A.; El Mongui, A. Serum prolactin level in patients with multiple sclerosis. Egypt. J. Neurol. Psychiatr. Neurosurg. 2015, 1, 52. [Google Scholar]
- Gold, S.M.; Kern, K.C.; O’Connor, M.-F.; Montag, M.J.; Kim, A.; Yoo, Y.S.; Giesser, B.S.; Sicotte, N.L. Smaller cornu ammonis 2–3/dentate gyrus volumes and elevated cortisol in multiple sclerosis patients with depressive symptoms. Biol. Psychiatry 2010, 68, 553–559. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arji, G.; Rezaeizadeh, H.; Moghadasi, A.N.; Sahraian, M.A.; Karimi, M.; Alizadeh, M. Complementary and alternative therapies in multiple sclerosis: A systematic literature classification and analysis. Acta Neurol. Belg. 2022, 122, 1–23. [Google Scholar] [CrossRef]
- Fleming, K.M.; Coote, S.B.; Herring, M.P. Home-based Pilates for symptoms of anxiety, depression and fatigue among persons with multiple sclerosis: An 8-week randomized controlled trial. Mult. Scler. J. 2021, 27, 2267–2279. [Google Scholar] [CrossRef]
- Sánchez-Lastra, M.A.; Martínez-Aldao, D.; Molina, A.J.; Ayán, C. Pilates for people with multiple sclerosis: A systematic review and meta-analysis. Mult. Scler. Relat. Disord. 2019, 28, 199–212. [Google Scholar] [CrossRef]
- Shohani, M.; Badfar, G.; Nasirkandy, M.P.; Kaikhavani, S.; Rahmati, S.; Modmeli, Y.; Soleymani, A.; Azami, M. The effect of yoga on stress, anxiety, and depression in women. Int. J. Prev. Med. 2018, 9, 21. [Google Scholar] [CrossRef]
- Leavitt, V.M.; Aguerre, I.M.; Lee, N.; Riley, C.S.; De Jager, P.L.; Bloom, S. RCT of a Telehealth Group-Based Intervention to Increase Physical Activity in Multiple Sclerosis: eFIT. Neurol. Clin. Pract. 2021, 11, 291–297. [Google Scholar] [CrossRef]
- Van Geel, F.; Geurts, E.; Abasıyanık, Z.; Coninx, K.; Feys, P. Feasibility study of a 10-week community-based program using the WalkWithMe application on physical activity, walking, fatigue and cognition in persons with Multiple Sclerosis. Mult. Scler. Relat. Disord. 2020, 42, 102067. [Google Scholar] [CrossRef]
- Kalron, A.; Rosenblum, U.; Frid, L.; Achiron, A. Pilates exercise training vs. physical therapy for improving walking and balance in people with multiple sclerosis: A randomized controlled trial. Clin. Rehabil. 2017, 31, 319–328. [Google Scholar] [CrossRef] [PubMed]
- Buoite Stella, A.; Pasquin, F.; Morrison, S.A.; Morelli, M.E.; Dinoto, A.; Bratina, A.; Bosco, A.; Sartori, A.; Giudici, F.; Manganotti, P. Effects of a cooling vest with sham condition on walking capacity in heat-sensitive people with multiple sclerosis. Eur. J. Appl. Physiol. 2020, 120, 2467–2476. [Google Scholar] [CrossRef] [PubMed]
- Carmen, E.-V.; Zorina, S.A.; Silviu, D.A.; Andrei, P.; Daniel, D.A.; Any, D.A. PILATES AS AN INSTRUMENT IN IMPROVING THE QUALITY OF LIFE IN MULTIPLE SCLEROSIS PATIENTS. Ovidius Univ. Ann. Ser. Phys. Educ. Sport/Sci. Mov. Health 2020, 20, 227–233. [Google Scholar]
- Lim, E.J.; Park, J.E. The effects of Pilates and yoga participant’s on engagement in functional movement and individual health level. J. Exerc. Rehabil. 2019, 15, 553. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jeitler, M.; Högl, M.; Peters, A.; Schumann, D.; Murthy, V.; Bringmann, H.; Seifert, G.; Michalsen, A.; Stöckigt, B.; Kessler, C.S. Qualitative study of yoga for Young adults in school sports. Complement. Ther. Med. 2020, 55, 102584. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Tele-Pilates Group (n = 15) | Tele-Yoga Group (n = 15) | Control Group (n = 15) | Total (n = 45) | |
|---|---|---|---|---|
| Age (year) | 36.20 ± 4.33 | 37.40 ± 6.03 | 40.40 ± 5.35 | 38.00 ± 5.46 |
| EDSS | 2.5 ± 1.32 | 2.5 ± 1.19 | 2.66 ± 1.03 | 2.55 ± 1.16 |
| BMI (kg/m2) | 22.14 ± 1.27 | 23.06 ± 1.07 | 23.99 ± 0.82 | 23.06 ± 1.30 |
| EMPL/UEMPL | 4/11 | 4/11 | 6/9 | 14/31 |
| Dip/UE | 6/9 | 7/8 | 4/11 | 17/28 |
| MDO (year) | 10.93 ± 4.38 | 8.00 ± 5.84 | 9.27 ± 8.37 | 9.40 ± 5.61 |
| Tele-Pilates Exercising (n = 15) | Tele-Yoga Exercising (n = 15) | Control Group (n = 15) | (p-Value) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Pre-Intervention | Post-Intervention | Pre-Intervention | Post-Intervention | Pre-Intervention | Post-Intervention | Time | Group | Time Group * | |
| Prolactin (ng/mL) | 20.79 ± 6.78 | 25.83 ± 8.66 | 20.33 ± 11.72 | 32.62 ± 23.84 | 21.74 ± 9.16 | 20.46 ± 9.08 | 0.001 * | 0.46 | 0.004 * |
| Cortisol (mcg/dL) | 24.62 ± 8.86 | 21.06 ± 8.81 | 22.26 ± 12.09 | 16.31 ± 7.84 | 17.86 ± 2.68 | 19.62 ± 5.78 | 0.04 * | 0.34 | 0.04 * |
| BDI scores | 13.00 ± 9.46 | 8.73 ± 8.25 | 13.60 ± 8.37 | 5.53 ± 4.71 | 7.93 ± 6.27 | 6.87 ± 4.91 | <0.001 * | 0.24 | 0.001 * |
| GHQ-12 scores | 13.33 ± 5.03 | 9.31 ± 4.37 | 12.67 ± 2.99 | 8.07 ± 3.80 | 13.07 ± 5.62 | 11.26 ± 2.89 | <0.001 * | 0.38 | 0.23 |
| IPAQ scores (MET-min/week) | 790.47 ± 707.26 | 2230.00 ± 1351.60 | 535.60 ± 381.27 | 1296.00 ± 636.79 | 917.27 ± 651.68 | 636.67 ± 505.60 | <0.001 * | 0.004 * | <0.001 * |
| T25FW (m/s) | 8.36 ± 1.25 | 6.62 ± 1.21 | 9.02 ± 2.04 | 7.49 ± 2.02 | 7.75 ± 1.32 | 7.91 ± 1.44 | <0.001 * | 0.38 | <0.001 * |
| MSQoL-54 Scores | |||||||||
| MHC scores | 61.45 ± 17.99 | 71.37 ± 16.90 | 58.34 ± 13.69 | 73.25 ± 9.97 | 70.10 ± 17.51 | 57.39 ± 19.59 | 0.001 * | 0.87 | 0.001 * |
| PHC scores | 63.93 ± 17.44 | 74.42 ± 14.51 | 61.16 ± 16.86 | 72.72 ± 12.69 | 71.56 ± 12.22 | 65.02 ± 14.60 | 0.01 * | 0.90 | <0.001 * |
| Tele-Pilates Exercising | Tele-yoga Exercising | Control Group | (p-Value) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Pre-Intervention | Post-Intervention | Pre-Intervention | Post-Intervention | Pre-Intervention | Post-Intervention | Time | Group | Time Group * | |
| Vigorous activity | 161.13 ± 112.27 | 610.67 ± 235.92 | 58.67 ± 31.68 | 322.67 ± 129.85 | 472.00 ± 284.19 | 109.33 ± 46.59 | 0.32 | 0.59 | 0.02 * |
| Moderate activity | 466.67 ± 157.98 | 822.67 ± 86.34 | 351.47 ± 75.25 | 720.00 ± 85.05 | 561.33 ± 161.59 | 282.67 ± 92.55 | 0.07 | 0.25 | 0.002 * |
| Walking activity | 162.67 ± 33.42 | 796.67 ± 152.86 | 125.47 ± 31.78 | 253.33 ± 56.35 | 306.27 ± 60.26 | 244.67 ± 68.28 | <0.001 * | <0.001 * | <0.001 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Najafi, P.; Hadizadeh, M.; Cheong, J.P.G.; Mohafez, H.; Abdullah, S.; Poursadeghfard, M. Effects of Tele-Pilates and Tele-Yoga on Biochemicals, Physical, and Psychological Parameters of Females with Multiple Sclerosis. J. Clin. Med. 2023, 12, 1585. https://doi.org/10.3390/jcm12041585
Najafi P, Hadizadeh M, Cheong JPG, Mohafez H, Abdullah S, Poursadeghfard M. Effects of Tele-Pilates and Tele-Yoga on Biochemicals, Physical, and Psychological Parameters of Females with Multiple Sclerosis. Journal of Clinical Medicine. 2023; 12(4):1585. https://doi.org/10.3390/jcm12041585
Chicago/Turabian StyleNajafi, Parisa, Maryam Hadizadeh, Jadeera Phaik Geok Cheong, Hamidreza Mohafez, Suhailah Abdullah, and Maryam Poursadeghfard. 2023. "Effects of Tele-Pilates and Tele-Yoga on Biochemicals, Physical, and Psychological Parameters of Females with Multiple Sclerosis" Journal of Clinical Medicine 12, no. 4: 1585. https://doi.org/10.3390/jcm12041585