
Papillary Muscle Involvement during Acute Myocardial Infarction: Detection by Cardiovascular Magnetic Resonance Using T1 Mapping Technique and Papillary Longitudinal Strain

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
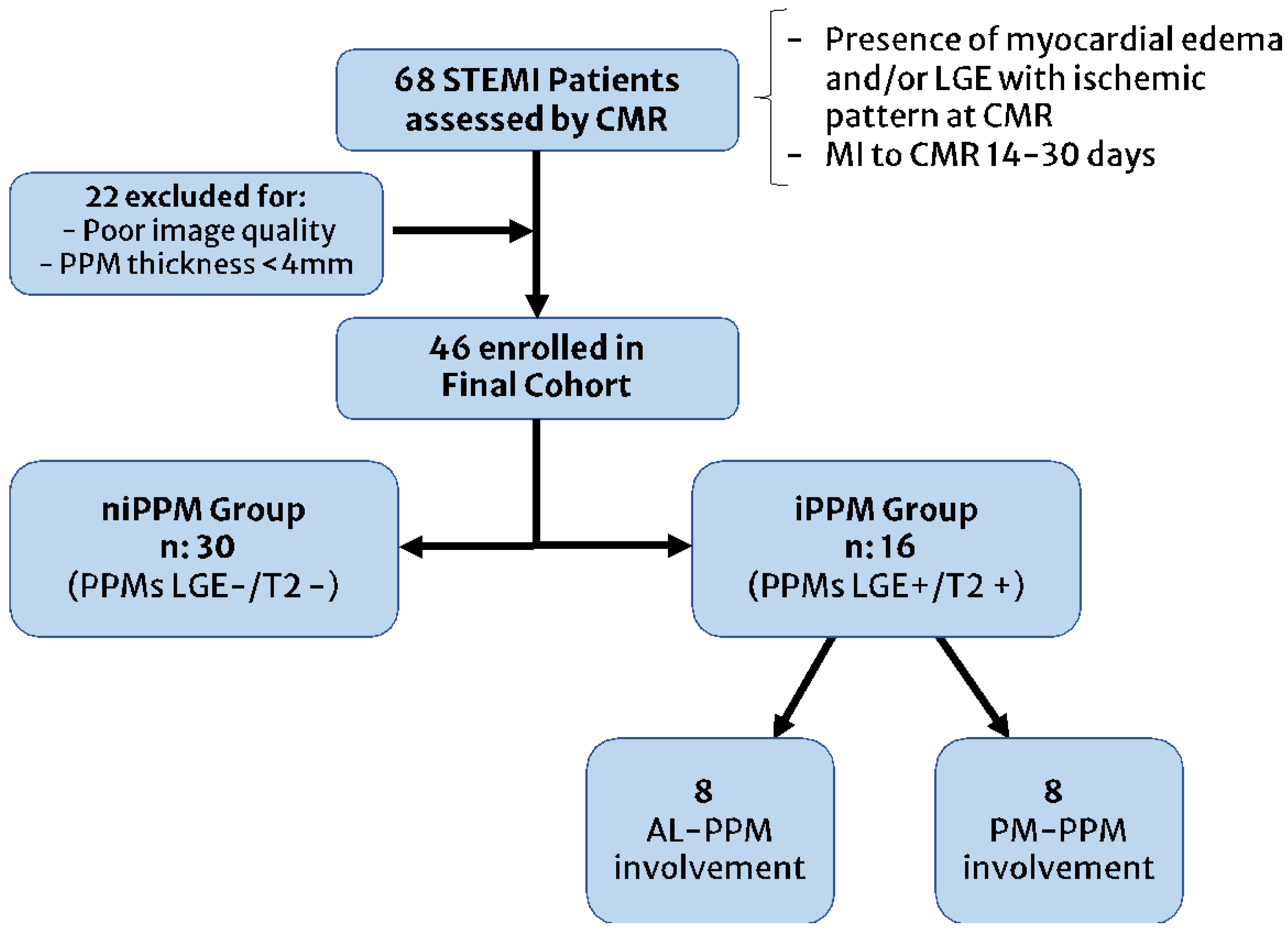
2.1. Study Subjects
- Poor CMR image quality (non-diagnostic images for the presence of artifacts or excessive noise) or papillary muscle thickness < 4 mm;
- Known or evidence of prior myocardial infarction or non-ischemic cardiomyopathies at CMR;
- Rapid ventricular response-atrial fibrillation (RVR-AF) or tachyarrhythmias;
- Implantable cardioverter-defibrillator/pacemaker bearers;
2.2. CMR Protocol
- T2-weighted Short Tau Inversion Recovery (T2-STIR) sequence acquired on the short axis (from base to apex, 8 slices at least), on 2-chamber and 4-chamber views (TR: 2 R-R intervals; TE: 75 ms; FA: 180°; TI: 170 ms; Slice thickness: 8 mm; FoV: 320–400 mm; Matrix: 256 × 256, Voxel size: 2.3 × 1.3 × 8 mm);
- Modified Look-Locker Inversion Recovery sequence for nT1 mapping, acquired on three short-axis slices at basal, mid-ventricular, and apical views and one four-chamber view before the administration of a single dose of 0.15 mMol/Kg gadoterate dimeglumine (TR: 314 ms; TE: 1.12 ms; FA: 12°; Slice thickness: 8 mm; FoV: 340–400 mm; matrix 256 × 256; Voxel size: 1.6 × 1.3 × 8 mm);
- Cine-Steady State Free Precession sequences for cineMR imaging, acquired on the short axis (from the base to the cardiac apex, 10–12 slices) and 2-, 3- and 4-chamber views (TR: 51.3 ms; TE: 1.21 ms; FA: 45°; Slice thickness: 8 mm; Matrix: 256 × 256; FoV: 340–400 mm; Voxel size: 1.6 × 1.3 × 8.0 mm);
- Contrast-enhanced Inversion Recovery T1-weighted images acquired from 15 to 20 min after GBCA injection, during breath-hold at end-diastole in the short axis (from the base to the cardiac apex, 10–12 slices) and then on the 2-, 3- and 4-chamber views (TI: 350–400 ms; TR: 9.6 ms; TE: 4.4 ms; matrix 256 × 208, FA: 25°; Slice thickness: 8 mm; interslice gap: 2 mm) for LGE imaging.
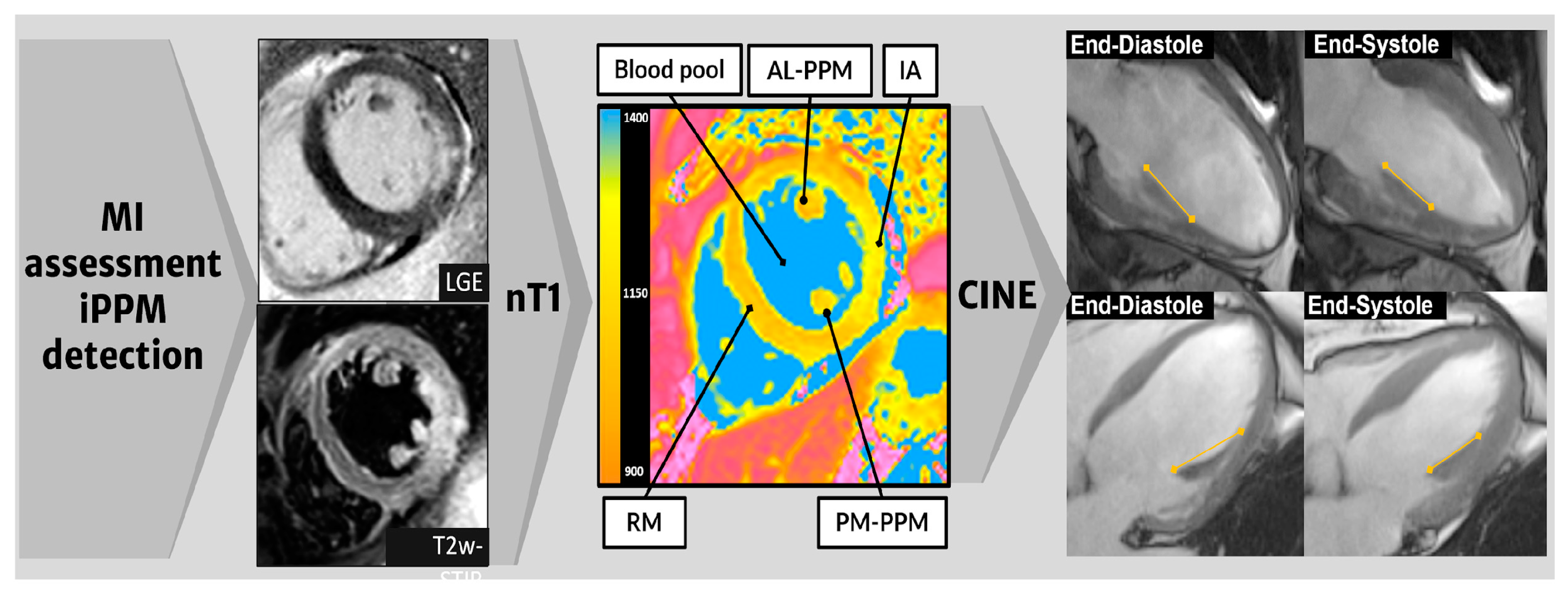
2.3. Image Analysis
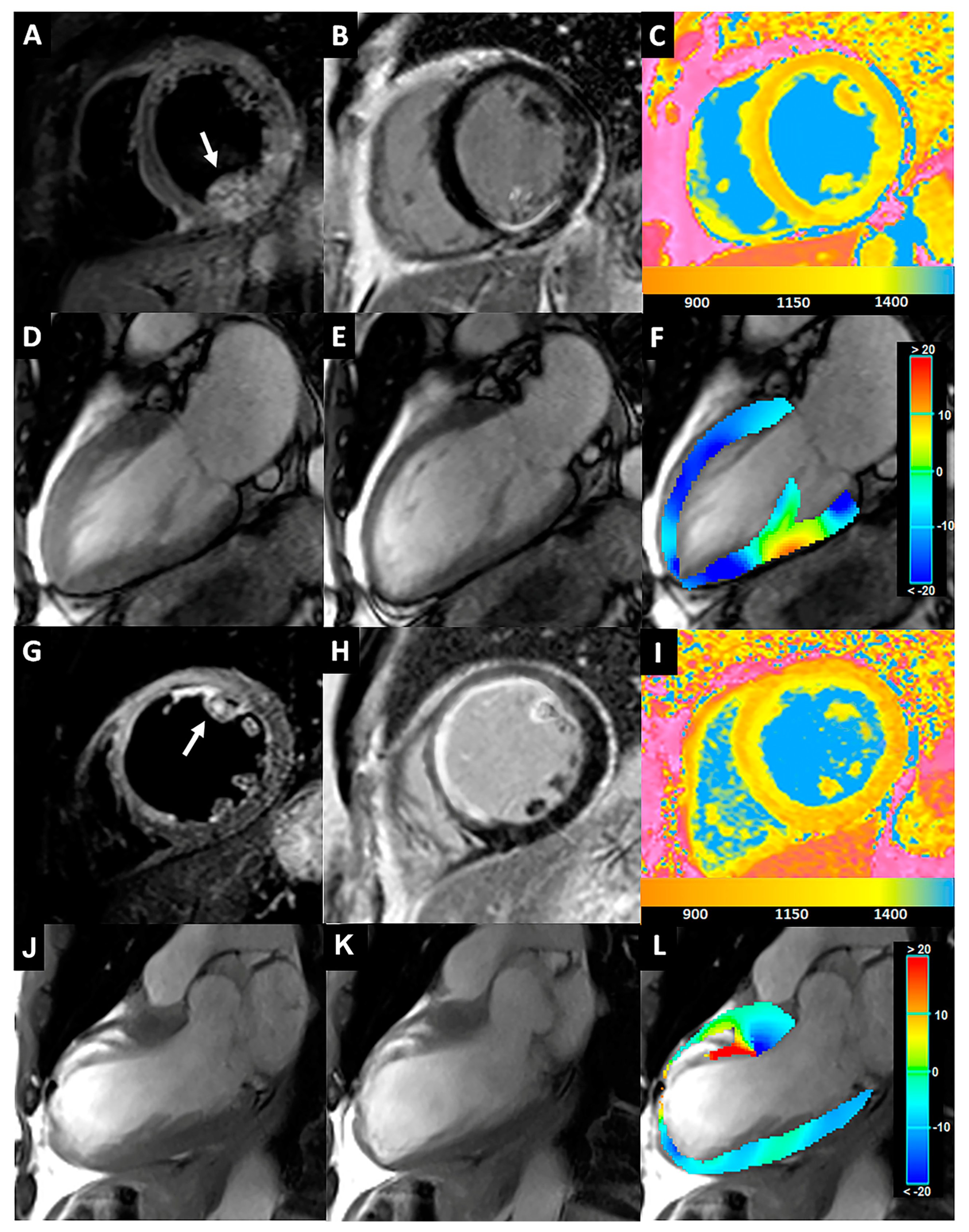
- Hyperintense area within AM- or PM- PPM on T2-STIR images (short and/or long axis views);
- Hyperintense area within AM- or PM- PPM on LGE images (short and/or long axis views);
- Obstructive coronary artery disease at coronary angiography in the culprit vessel (RCA-posterior descending branch or LCX for the PM-PPM, LCX, or ADA for the AM-PPM).
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
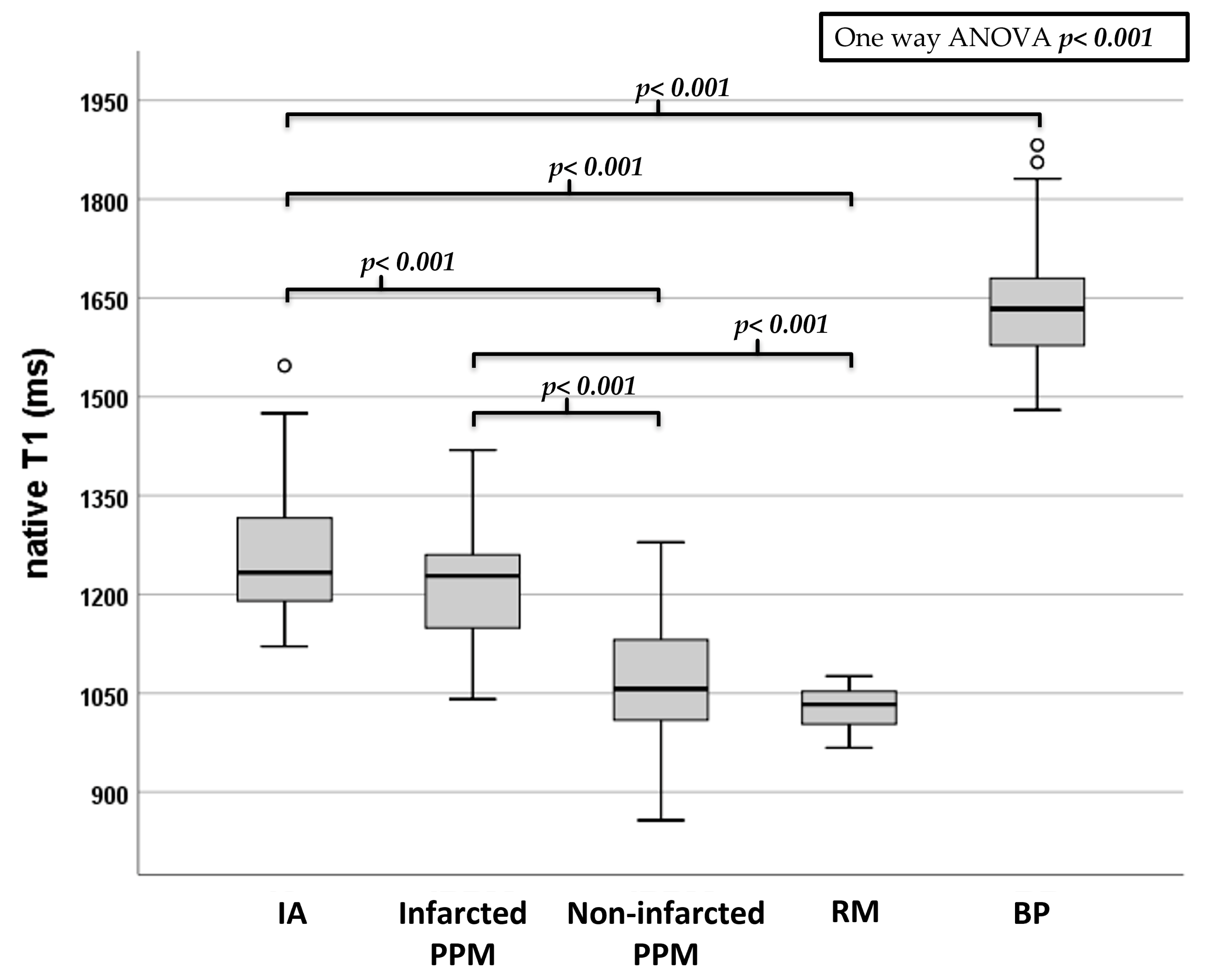
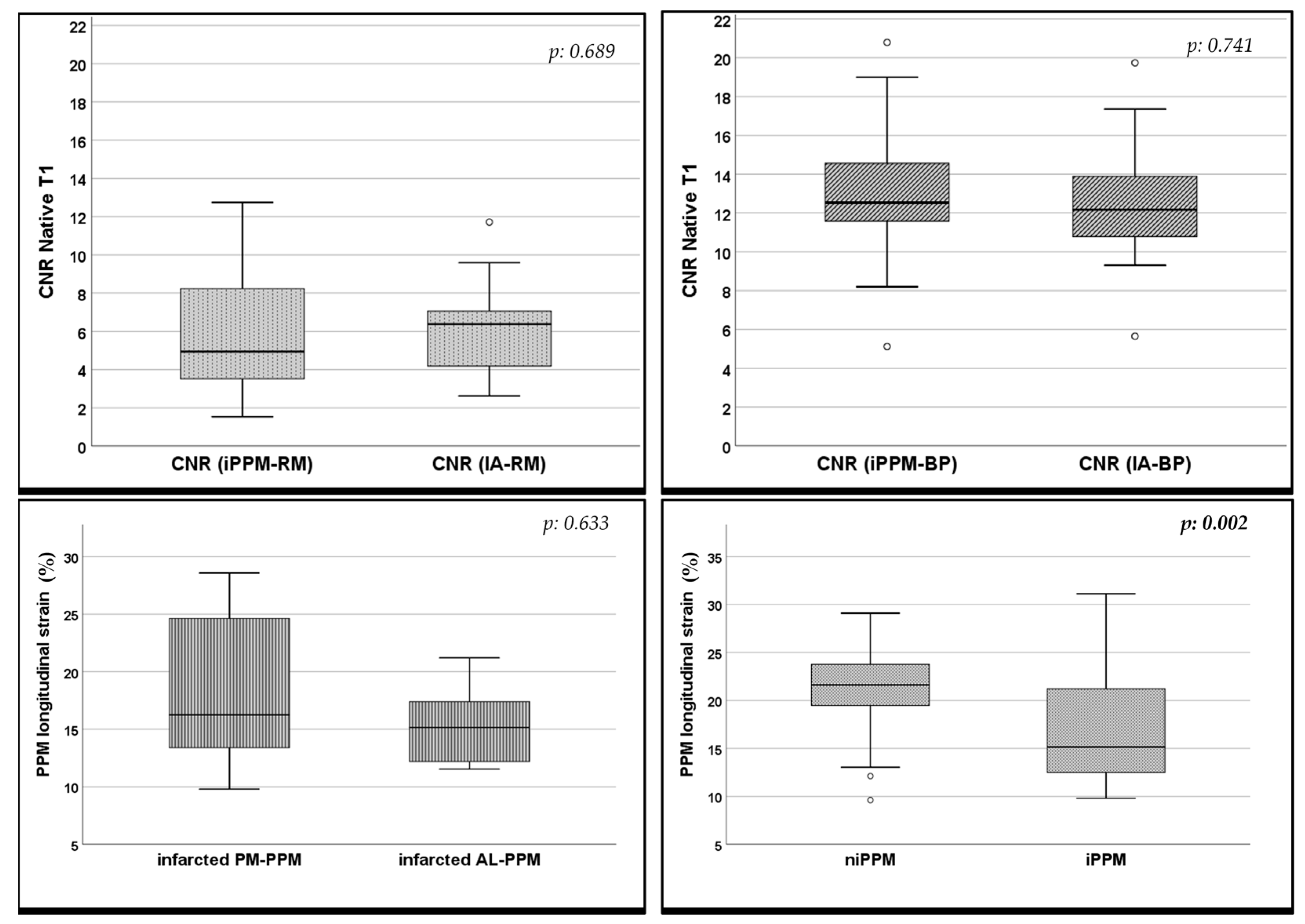
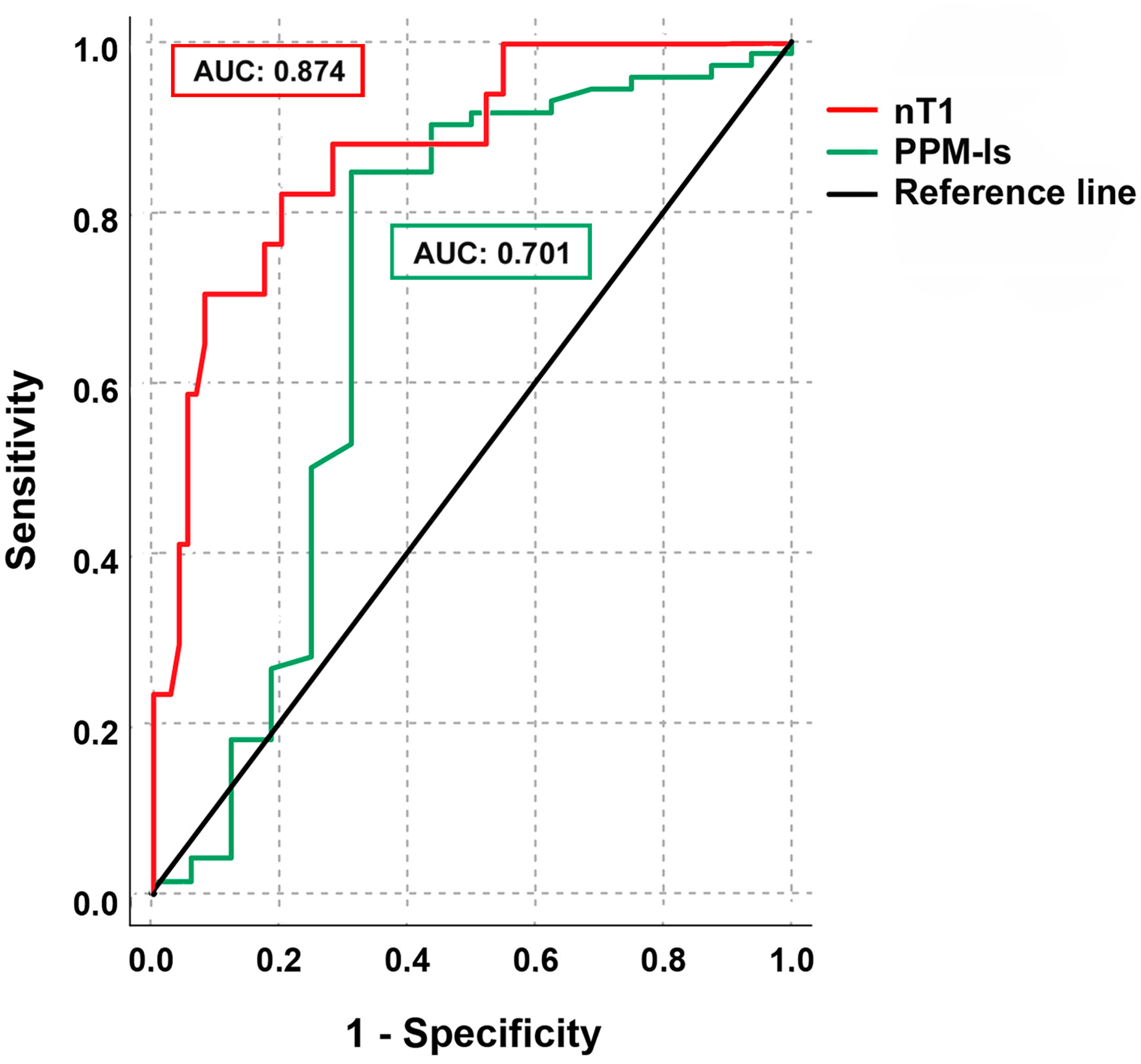
3.2. CMR Features
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AAR | Area at risk |
| AL-PPM | Anterolateral papillary muscles |
| ANOVA | Analysis of variance |
| AUC | Area under the curve |
| BMI | Body mass index |
| BP | Blood pool |
| BSA | Body surface area |
| CI | Confidence interval |
| CMR | Cardiac magnetic resonance |
| CNR | Contrast to noise ratio |
| DM | Diabetes mellitus |
| EDV | Indexed end-diastolic volume |
| EDV/BSA | End-diastolic volume/body surface area |
| EF | Ejection fraction |
| ESV | End-systolic volume |
| ESV/BSA | End-systolic volume/body surface area |
| GBCA | Gadolinium-based contrast agent |
| HR | Heart rate |
| HTN | Systemic arterial hypertension |
| IA | Infarcted area |
| ICC | Intraclass correlation coefficient |
| iPPM | Papillary muscle infarction |
| LAD | Left anterior descending artery |
| LCX | Left circumflex artery |
| LGE | Late gadolinium enhancement |
| LV | Left ventricle |
| MI | Myocardial infarction |
| MR | Magnetic resonance |
| MV | Mitral valve |
| MVO | Microvascular obstruction |
| MVR | Mitral valve regurgitation |
| niPPM | Non infarcted papillary muscle |
| OM | Obtuse marginal branch |
| PPM | Papillary muscle |
| PPM-ls | Longitudinal strain of papillary muscle |
| PM-PPM | Posteromedial papillary muscles |
| RCA | Right coronary artery |
| RM | Remote myocardium |
| ROC | Receiver operating characteristic |
| ROI | Region of interest |
| RV | Right ventricular |
| RVR-AF | Rapid ventricular response-atrial fibrillation |
| SD | Standard deviation |
| STEMI | ST elevation myocardial infarction |
| STIR | Short Tau inversion recovery |
| SV | Stroke volume |
| SV/BSA | Stroke volume/body surface area |
| TE | Time to echo |
| TR | Repetition time |
| TTE | Transthoracic echocardiogram |
References
- Velasco Forte, M.N.; Nassar, M.; Byrne, N.; Silva Vieira, M.; Pérez, I.V.; Ruijsink, B.; Simpson, J.; Hussain, T. Morphological Three-Dimensional Analysis of Papillary Muscles in Borderline Left Ventricles. Cardiol. Young 2017, 27, 1369–1376. [Google Scholar] [CrossRef]
- Tanimoto, T.; Imanishi, T.; Kitabata, H.; Nakamura, N.; Kimura, K.; Yamano, T.; Ishibashi, K.; Komukai, K.; Ino, Y.; Takarada, S.; et al. Prevalence and Clinical Significance of Papillary Muscle Infarction Detected by Late Gadolinium-Enhanced Magnetic Resonance Imaging in Patients With ST-Segment Elevation Myocardial Infarction. Circulation 2010, 122, 2281–2287. [Google Scholar] [CrossRef]
- Bouma, W.; Wijdh-den Hamer, I.J.; Koene, B.M.; Kuijpers, M.; Natour, E.; Erasmus, M.E.; Jainandunsing, J.S.; van der Horst, I.C.; Gorman, J.H.; Gorman, R.C.; et al. Long-Term Survival after Mitral Valve Surgery for Post-Myocardial Infarction Papillary Muscle Rupture. J. Cardiothorac. Surg. 2015, 10, 11. [Google Scholar] [CrossRef]
- Eitel, I.; Gehmlich, D.; Amer, O.; Wöhrle, J.; Kerber, S.; Lauer, B.; Pauschinger, M.; Schwab, J.; Birkemeyer, R.; Zimmermann, R.; et al. Prognostic Relevance of Papillary Muscle Infarction in Reperfused Infarction as Visualized by Cardiovascular Magnetic Resonance. Circ. Cardiovasc. Imaging 2013, 6, 890–898. [Google Scholar] [CrossRef] [PubMed]
- Lei, D.; Xie, J.; Dai, Q.; Huang, Y.; Wei, X.; Mu, D.; Bao, X.; Li, J.; Xu, B. Prognostic Relevance and Clinical Features of Papillary Muscle Infarction with Mitral Regurgitation in Patients with ST Segment Elevation Myocardial Infarction. J. Thorac. Dis. 2021, 13, 334–342. [Google Scholar] [CrossRef]
- Kisanuki, A.; Otsuji, Y.; Kuroiwa, R.; Murayama, T.; Matsushita, R.; Shibata, K.; Yutsudo, T.; Nakao, S.; Nomoto, K.; Tomari, T.; et al. Two-Dimensional Echocardiographic Assessment of Papillary Muscle Contractility in Patients with Prior Myocardial Infarction. J. Am. Coll. Cardiol. 1993, 21, 932–938. [Google Scholar] [CrossRef]
- Nappi, F.; Nenna, A.; Sing, S.S.A.; Timofeeva, I.; Mihos, C.; Gentile, F.; Chello, M. Mitral Regurgitation: Lessons Learned from COAPT and MITRA-Fr. J. Thorac. Dis. 2020, 12, 2936–2944. [Google Scholar] [CrossRef]
- Galea, N.; Dacquino, G.M.; Ammendola, R.M.; Coco, S.; Agati, L.; De Luca, L.; Carbone, I.; Fedele, F.; Catalano, C.; Francone, M. Microvascular Obstruction Extent Predicts Major Adverse Cardiovascular Events in Patients with Acute Myocardial Infarction and Preserved Ejection Fraction. Eur. Radiol. 2019, 29, 2369–2377. [Google Scholar] [CrossRef] [PubMed]
- Dagdelen, S.; Yuce, M.; Ergelen, M.; Pala, S.; Kyrma, C. Quantitation of Papillary Muscle Function with Tissue and Strain Doppler Echocardiography Measures Papillary Muscle Contractile Functions. Echocardiography 2003, 20, 137–144. [Google Scholar] [CrossRef] [PubMed]
- Dall’Armellina, E.; Piechnik, S.K.; Ferreira, V.M.; Si, Q.L.; Robson, M.D.; Francis, J.M.; Cuculi, F.; Kharbanda, R.K.; Banning, A.P.; Choudhury, R.P.; et al. Cardiovascular Magnetic Resonance by Non Contrast T1-Mapping Allows Assessment of Severity of Injury in Acute Myocardial Infarction. J. Cardiovasc. Magn. Reson. 2012, 14, 15. [Google Scholar] [CrossRef] [Green Version]
- Liu, D.; Borlotti, A.; Viliani, D.; Jerosch-Herold, M.; Alkhalil, M.; De Maria, G.L.; Fahrni, G.; Dawkins, S.; Wijesurendra, R.; Francis, J.; et al. CMR Native T1 Mapping Allows Differentiation of Reversible Versus Irreversible Myocardial Damage in ST-Segment–Elevation Myocardial Infarction. Circ. Cardiovasc. Imaging 2017, 10, e005986. [Google Scholar] [CrossRef] [PubMed]
- Rajiah, P.; Fulton, N.L.; Bolen, M. Magnetic Resonance Imaging of the Papillary Muscles of the Left Ventricle: Normal Anatomy, Variants, and Abnormalities. Insights Imaging 2019, 10, 83. [Google Scholar] [CrossRef]
- Kılıcgedik, A.; Kahveci, G.; Gurbuz, A.S.; Karabay, C.Y.; Guler, A.; Efe, S.C.; Aung, S.M.; Arslantas, U.; Demir, S.; Izgi, I.A.; et al. Papillary Muscle Free Strain in Patients with Severe Degenerative and Functional Mitral Regurgitation. Arq. Bras. Cardiol. 2017, 108, 339–346. [Google Scholar] [CrossRef] [PubMed]
- Uemura, T.; Otsuji, Y.; Nakashiki, K.; Yoshifuku, S.; Maki, Y.; Yu, B.; Mizukami, N.; Kuwahara, E.; Hamasaki, S.; Biro, S.; et al. Papillary Muscle Dysfunction Attenuates Ischemic Mitral Regurgitation in Patients With Localized Basal Inferior Left Ventricular Remodeling. J. Am. Coll. Cardiol. 2005, 46, 113–119. [Google Scholar] [CrossRef] [PubMed]
- Carrick, D.; Haig, C.; Ahmed, N.; Rauhalammi, S.; Clerfond, G.; Carberry, J.; Mordi, I.; McEntegart, M.; Petrie, M.C.; Eteiba, H.; et al. Temporal Evolution of Myocardial Hemorrhage and Edema in Patients after Acute St-Segment Elevation Myocardial Infarction: Pathophysiological Insights and Clinical Implications. J. Am. Heart Assoc. 2016, 5, e002834. [Google Scholar] [CrossRef]
- Fernández-Jiménez, R.; Sánchez-González, J.; Agüero, J.; García-Prieto, J.; López-Martín, G.J.; García-Ruiz, J.M.; Molina-Iracheta, A.; Rosselló, X.; Fernández-Friera, L.; Pizarro, G.; et al. Myocardial Edema after Ischemia/Reperfusion Is Not Stable and Follows a Bimodal Pattern: Imaging and Histological Tissue Characterization. J. Am. Coll. Cardiol. 2015, 65, 315–323. [Google Scholar] [CrossRef]
- Galea, N.; Francone, M.; Zaccagna, F.; Ciolina, F.; Cannata, D.; Algeri, E.; Agati, L.; Catalano, C.; Carbone, I. Ultra Low-Dose of Gadobenate Dimeglumine for Late Gadolinium Enhancement (LGE) Imaging in Acute Myocardial Infarction: A Feasibility Study. Eur. J. Radiol. 2014, 83, 2151–2158. [Google Scholar] [CrossRef]
- Smiseth, O.A.; Torp, H.; Opdahl, A.; Haugaa, K.H.; Urheim, S. Myocardial Strain Imaging: How Useful Is It in Clinical Decision Making? Eur. Heart J. 2016, 37, 1196–1207. [Google Scholar] [CrossRef]
- Messroghli, D.R.; Walters, K.; Plein, S.; Sparrow, P.; Friedrich, M.G.; Ridgway, J.P.; Sivananthan, M.U. Myocardial T 1 Mapping: Application to Patients with Acute and Chronic Myocardial Infarction. Magn. Reson. Med. 2007, 58, 34–40. [Google Scholar] [CrossRef]
- Piechnik, S.K.; Ferreira, V.M.; Dall’Armellina, E.; Cochlin, L.E.; Greiser, A.; Neubauer, S.; Robson, M.D. Shortened Modified Look-Locker Inversion Recovery (ShMOLLI) for Clinical Myocardial T1-Mapping at 1.5 and 3 T within a 9 Heartbeat Breathhold. J. Cardiovasc. Magn. Reson. 2010, 12, 69. [Google Scholar] [CrossRef] [Green Version]
- Demirkiran, A.; Everaars, H.; Amier, R.P.; Beijnink, C.; Bom, M.J.; Götte, M.J.W.; van Loon, R.B.; Selder, J.L.; van Rossum, A.C.; Nijveldt, R. Cardiovascular Magnetic Resonance Techniques for Tissue Characterization after Acute Myocardial Injury. Eur. Heart J. Cardiovasc. Imaging 2019, 20, 723–734. [Google Scholar] [CrossRef] [PubMed]
- Kellman, P.; Hansen, M.S. T1-Mapping in the Heart: Accuracy and Precision. J. Cardiovasc. Magn. Reson. 2014, 16, 2. [Google Scholar] [CrossRef] [PubMed]
- Xue, H.; Shah, S.; Greiser, A.; Guetter, C.; Littmann, A.; Jolly, M.-P.; Arai, A.E.; Zuehlsdorff, S.; Guehring, J.; Kellman, P. Motion Correction for Myocardial T1 Mapping Using Image Registration with Synthetic Image Estimation. Magn. Reson. Med. 2012, 67, 1644–1655. [Google Scholar] [CrossRef] [PubMed]
- Xue, H.; Greiser, A.; Zuehlsdorff, S.; Jolly, M.-P.; Guehring, J.; Arai, A.E.; Kellman, P. Phase-Sensitive Inversion Recovery for Myocardial T 1 Mapping with Motion Correction and Parametric Fitting. Magn. Reson. Med. 2013, 69, 1408–1420. [Google Scholar] [CrossRef] [PubMed]
- Madu, E.C.; D’Cruz, I.A. The Vital Role of Papillary Muscles in Mitral and Ventricular Function: Echocardiographic Insights. Clin. Cardiol. 1997, 20, 93–98. [Google Scholar] [CrossRef]
- Yiu, S.F.; Enriquez-Sarano, M.; Tribouilloy, C.; Seward, J.B.; Tajik, A.J. Determinants of the Degree of Functional Mitral Regurgitation in Patients with Systolic Left Ventricular Dysfunction: A Quantitative Clinical Study. Circulation 2000, 102, 1400–1406. [Google Scholar] [CrossRef]
- Demirelli, S.; Degirmenci, H.; Bilen, H.; Ermis, E.; Duman, H.; Arisoy, A.; Bakirci, E.M.; Ipek, E.; Askin, L. Left Ventricular Mechanics in Behcet’s Disease: A Speckle Tracking Echocardiographic Study. Bosn. J. Basic Med. Sci. 2014, 14, 160. [Google Scholar] [CrossRef]
- Zhang, K.; Fu, W.; Dai, Q.; Zheng, J.; Biekan, J.; Wang, Y.; Yan, P.; Gu, X.; Mu, J.; Dong, R. The Number of Myocardial Infarction Segments Connected to Papillary Muscle Is Associated with the Improvement in Moderate Ischemic Mitral Regurgitation. Cardiovasc. Diagn. Ther. 2022, 12, 828–839. [Google Scholar] [CrossRef]
- Dudzinski, D.M.; Hung, J. Echocardiographic Assessment of Ischemic Mitral Regurgitation. Cardiovasc. Ultrasound 2014, 12, 46. [Google Scholar] [CrossRef]
- Kumanohoso, T.; Otsuji, Y.; Yoshifuku, S.; Matsukida, K.; Koriyama, C.; Kisanuki, A.; Minagoe, S.; Levine, R.A.; Tei, C. Mechanism of Higher Incidence of Ischemic Mitral Regurgitation in Patients with Inferior Myocardial Infarction: Quantitative Analysis of Left Ventricular and Mitral Valve Geometry in 103 Patients with Prior Myocardial Infarction. J. Thorac. Cardiovasc. Surg. 2003, 125, 135–143. [Google Scholar] [CrossRef] [Green Version]
- O’Gara, P.T.; Mack, M.J. Secondary Mitral Regurgitation. N. Engl. J. Med. 2020, 383, 1458–1467. [Google Scholar] [CrossRef] [PubMed]
- Chinitz, J.S.; Chen, D.; Goyal, P.; Wilson, S.; Islam, F.; Nguyen, T.; Wang, Y.; Hurtado-Rua, S.; Simprini, L.; Cham, M.; et al. Mitral Apparatus Assessment by Delayed Enhancement CMR. JACC Cardiovasc. Imaging 2013, 6, 220–234. [Google Scholar] [CrossRef] [PubMed]
- Bax, J.J.; Delgado, V. Papillary Muscle Infarction, Mitral Regurgitation, and Long-Term Prognosis. Circ. Cardiovasc. Imaging 2013, 6, 855–857. [Google Scholar] [CrossRef]
- Calvieri, C.; Riva, A.; Sturla, F.; Dominici, L.; Conia, L.; Gaudio, C.; Miraldi, F.; Secchi, F.; Galea, N. Left Ventricular Adverse Remodeling in Ischemic Heart Disease: Emerging Cardiac Magnetic Resonance Imaging Biomarkers. J. Clin. Med. 2023, 12, 334. [Google Scholar] [CrossRef] [PubMed]
- Filomena, D.; Cimino, S.; Monosilio, S.; Galea, N.; Mancuso, G.; Francone, M.; Tonti, G.; Pedrizzetti, G.; Maestrini, V.; Fedele, F.; et al. Impact of Intraventricular Haemodynamic Forces Misalignment on Left Ventricular Remodelling after Myocardial Infarction. ESC Heart Fail. 2022, 9, 496–505. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Total | iPPM | niPPM | p-Value |
|---|---|---|---|---|
| Population (n, %) | 46 (100) | 16 (35) | 30 (65) | - |
| Age (Years, mean ± SD) | 59 ± 13 | 60 ± 9 | 59 ± 14 | 0.815 |
| Sex (n men, %) | 38/46 (83) | 14/16 (88) | 24/30 (80) | 0.694 |
| MI-to-CMR interval (days, mean ± SD) | 18 ± 7 | 17 ± 8 | 18 ± 6 | 0.917 |
| BMI (kg/m2, mean ± SD) | 26.1 ± 4.2 | 25.2 ± 4.6 | 26.6 ± 3.9 | 0.581 |
| HTN (n°. %) | 30 (65) | 10 (63) | 20 (67) | 0.697 |
| HR (bpm, mean ± SD) | 71 ± 5 | 74 ± 8 | 70 ± 3 | 0.031 |
| DM (n°. %) | 6 (13) | 2 (13) | 4 (13) | 0.936 |
| Current Smoker (n°. %) | 29 (63) | 10 (63) | 19 (63) | 0.943 |
| Family history of MI (n°. %) | 15 (33) | 6 (38) | 9 (30) | 0.734 |
| Parameter | Total (N: 46) | iPPM Group (N:16) | niPPM Group (N:30) | p-Value |
|---|---|---|---|---|
| MI location anterior/lateral/inferior, n (%) | 28/5/13 (61/11/28) | 9/1/6 (56/6/38) | 19/4/7 (64/13/23) | - |
| AL-/PL-PPM infarction, n (%) | 8 (17)/8 (17) | 8 (50)/8 (50) | - | - |
| LV EDV/BSA (mL/mq) | 89.59 ± 26.53 | 96.01 ± 27.51 | 86.16 ± 25.79 | 0.235 |
| LV ESV/BSA (mL/mq) | 54.37 ± 23.72 | 61.41 ± 23.70 | 50.61 ± 23.24 | 0.143 |
| LV SV/BSA (mL/mq) | 35.22 ± 11.02 | 34.59 ± 12.35 | 35.55 ± 10.45 | 0.781 |
| LV EF (%) | 41.03 ± 11.36 | 37.14 ± 11.13 | 43.11 ± 11.11 | 0.090 |
| RV EDV/BSA (mL/mq) | 70.25 ± 25.66 | 64.59 ± 18.91 | 73.48 ± 28.63 | 0.274 |
| RV ESV/BSA (mL/mq) | 36.04 ± 20.69 | 35.59 ± 20.00 | 36.29 ± 21.42 | 0.915 |
| RV SV/BSA (mL/mq) | 34.21 ± 16.94 | 28.99 ± 24.19 | 37.19 ± 10.34 | 0.124 |
| RV EF (%) | 51.89 ± 9.69 | 51.61 ± 11.83 | 52.05 ± 8.46 | 0.889 |
| nT1 PPM (ms) | 1096.84 ± 104.81 | 1219.35 ± 102.55 * | 1052.20 ± 80.45 | <0.001 |
| nT1 AL-PPM (ms) | 1082.46 ± 105.65 | 1217.9 ± 78.6 ** | 1052.2 ± 80.4 | <0.001 |
| nT1 PM-PPM (ms) | 1111.53 ± 103.04 | 1232.29 ± 123.04 *** | 1080.69 ± 77.64 | <0.001 |
| nT1 RM (ms) | 1.032.13 ± 37.19 | 1029.50 ± 29.82 | 1038.87 ± 39.38 | 0.093 |
| nT1 IA (ms) | 1264.48 ± 98.48 | 1233.44 ± 64.7 | 1281.03 ± 109.9 | 0.120 |
| nT1 BP (ms) | 1646.50 ± 92.75 | 1658.81 ± 98.7 | 1639.93 ± 90.5 | 0.517 |
| Noise (muscle SD) | 34.17 ± 7.41 | 34.79 ± 6.64 | 33.83 ± 7.87 | 0.680 |
| No MVR (n) | 37 | 13 | 24 | 0.879 |
| MVR mild/moderate/severe (n) | 8/1/0 | 3/0/0 | 5/1/0 | 0.892 |
| Morpho-Dynamics Parameters (Mean ± SD) | Total (N: 46) | IPPM Group (N: 16) | niPPM Group (N: 30) | p-Value |
|---|---|---|---|---|
| Diastolic Length (mm) | 42.56 ± 6.23 | 41.88 ± 5.92 * | 42.72 ± 6.33 | 0.622 |
| Systolic Length (mm) | 33.69 ± 5.49 | 34.59 ± 6.14 * | 33.48 ± 5.35 | 0.457 |
| PPM-ls (%) | 20.88 ± 4.94 | 17.56 ± 6.30 * | 21.65 ± 4.26 | 0.002 |
| AL-PPM-ls (%) | 20.99 ± 4.63 | 16.98 ± 6.41 ** | 23.02 ± 4.84 | 0.009 |
| PM-PPM-ls (%) | 20.71 ± 5.32 | 15.18 ± 4.59 *** | 21.74 ± 5.21 | 0.011 |
| CNR | Value |
|---|---|
| nT1 (IA/RM) | 6.27 ± 2.42 |
| nT1 (infarcted PPM/RM) * | 5.87 ± 3.31 |
| nT1 (IA/BP) | −12.56 ± 3.21 |
| nT1 (infarcted PPM/BP) * | −12.96 ± 3.77 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pambianchi, G.; Giannetti, M.; Marchitelli, L.; Cundari, G.; Maestrini, V.; Mancone, M.; Francone, M.; Catalano, C.; Galea, N. Papillary Muscle Involvement during Acute Myocardial Infarction: Detection by Cardiovascular Magnetic Resonance Using T1 Mapping Technique and Papillary Longitudinal Strain. J. Clin. Med. 2023, 12, 1497. https://doi.org/10.3390/jcm12041497
Pambianchi G, Giannetti M, Marchitelli L, Cundari G, Maestrini V, Mancone M, Francone M, Catalano C, Galea N. Papillary Muscle Involvement during Acute Myocardial Infarction: Detection by Cardiovascular Magnetic Resonance Using T1 Mapping Technique and Papillary Longitudinal Strain. Journal of Clinical Medicine. 2023; 12(4):1497. https://doi.org/10.3390/jcm12041497
Chicago/Turabian StylePambianchi, Giacomo, Martina Giannetti, Livia Marchitelli, Giulia Cundari, Viviana Maestrini, Massimo Mancone, Marco Francone, Carlo Catalano, and Nicola Galea. 2023. "Papillary Muscle Involvement during Acute Myocardial Infarction: Detection by Cardiovascular Magnetic Resonance Using T1 Mapping Technique and Papillary Longitudinal Strain" Journal of Clinical Medicine 12, no. 4: 1497. https://doi.org/10.3390/jcm12041497