
Anatomical Changes after Transcatheter Edge-to-Edge Repair in Functional MR According to MitraClip Generation
 ,
,  , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Echocardiographic Study
2.2. Study Outcomes
2.3. Statistical Analysis
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Iung, B.; Vahanian, A. Epidemiology of valvular heart disease in the adult. Nat. Rev. Cardiol. 2011, 8, 162–172. [Google Scholar] [CrossRef] [PubMed]
- Vahanian, A.; Beyersdorf, F.; Praz, F.; Milojevic, M.; Baldus, S.; Bauersachs, J.; Capodanno, D.; Conradi, L.; De Bonis, M.; De Paulis, R.; et al. 2021 ESC/EACTS Guidelines for the management of valvular heart disease. Eur. Heart J. 2022, 43, 561–632. [Google Scholar] [CrossRef] [PubMed]
- Stone, G.W.; Lindenfeld, J.; Abraham, W.T.; Kar, S.; Lim, D.S.; Mishell, J.M.; Whisenant, B.; Grayburn, P.A.; Rinaldi, M.; Kapadia, S.R.; et al. Transcatheter mitral-valve repair in patients with heart failure. N. Engl. J. Med. 2018, 379, 2307–2318. [Google Scholar] [CrossRef] [PubMed]
- Mack, M.; Carroll, J.D.; Thourani, V.; Vemulapalli, S.; Squiers, J.; Manandhar, P.; Deeb, G.M.; Batchelor, W.; Herrmann, H.C.; Cohen, D.J.; et al. Transcatheter Mitral Valve Therapy in the United States: A Report from the STS/ACC TVT Registry. Ann. Thorac. Surg. 2022, 113, 337–365. [Google Scholar] [CrossRef] [PubMed]
- Schueler, R.; Kaplan, S.; Melzer, C.; Öztürk, C.; Weber, M.; Sinning, J.-M.; Welz, A.; Werner, N.; Nickenig, G.; Hammerstingl, C. Impact of interventional edge-to-edge repair on mitral valve geometry. Int. J. Cardiol. 2017, 230, 468–475. [Google Scholar] [CrossRef]
- Noack, T.; Kiefer, P.; Mallon, L.; Lurz, P.; Bevilacqua, C.; Banusch, J.; Emrich, F.; Holzhey, D.M.; Vannan, M.; Thiele, H.; et al. Changes in dynamic mitral valve geometry during percutaneous edge–edge mitral valve repair with the MitraClip system. J. Echocardiogr. 2019, 17, 84–94. [Google Scholar] [CrossRef] [PubMed]
- Zoghbi, W.A.; Adams, D.; Bonow, R.O.; Enriquez-Sarano, M.; Foster, E.; Grayburn, P.A.; Hahn, R.T.; Han, Y.; Hung, J.; Lang, R.M.; et al. Recommendations for Noninvasive Evaluation of Native Valvular Regurgitation: A Report from the American Society of Echocardiography Developed in Collaboration with the Society for Cardiovascular Magnetic Resonance. J. Am. Soc. Echocardiogr. 2017, 30, 303–371. [Google Scholar] [CrossRef] [PubMed]
- Lancellotti, P.; Tribouilloy, C.; Hagendorff, A.; Popescu, B.A.; Edvardsen, T.; Pierard, L.A.; Badano, L.; Zamorano, J.L. Recommendations for the echocardiographic assessment of native valvular regurgitation: An executive summary from the European Association of Cardiovascular Imaging. Eur. Heart J. Cardiovasc. Imaging 2013, 14, 611–644. [Google Scholar] [CrossRef] [PubMed]
- Feldman, T.; Foster, E.; Glower, D.D.; Kar, S.; Rinaldi, M.J.; Fail, P.S.; Smalling, R.W.; Siegel, R.; Rose, G.A.; Engeron, E.; et al. Percutaneous Repair or Surgery for Mitral Regurgitation. N. Engl. J. Med. 2011, 364, 1395–1406. Available online: http://www.nejm.org/doi/abs/10.1056/NEJMoa1009355 (accessed on 7 May 2020). [CrossRef] [PubMed]
- Zoghbi, W.A.; Asch, F.M.; Bruce, C.; Gillam, L.D.; Grayburn, P.A.; Hahn, R.T.; Inglessis, I.; Islam, A.M.; Lerakis, S.; Little, S.H.; et al. Guidelines for the Evaluation of Valvular Regurgitation After Percutaneous Valve Repair or Replacement: A Report from the American Society of Echocardiography Developed in Collaboration with the Society for Cardiovascular Angiography and Interventions, Ja. J. Am. Soc. Echocardiogr. 2019, 32, 431–475. [Google Scholar] [CrossRef] [PubMed]
- Kang, D.H.; Park, S.J.; Shin, S.H.; Hong, G.R.; Lee, S.; Kim, M.S.; Yun, S.C.; Song, J.M.; Park, S.W.; Kim, J.J. Angiotensin Receptor Neprilysin Inhibitor for Functional Mitral Regurgitation: PRIME Study. Circulation 2019, 139, 1354–1365. [Google Scholar] [CrossRef] [PubMed]
- Hidalgo, F.; Mesa, D.; Ruiz, M.; Delgado, M.; Rodríguez, S.; Pardo, L.; Pan, M.; López, A.; Romero, M.A.; de Lezo, J.S. Effects of Mitral Annulus Remodeling Following MitraClip Procedure on Reduction of Functional Mitral Regurgitation. Rev. Esp. Cardiol. 2016, 69, 1020–1025. [Google Scholar] [CrossRef] [PubMed]
- Remy, T.; Bertog, S.C.; Wunderlich, N.; Vaskelyte, L.; Hofmann, I.; Gafoor, S.; Sievert, H. Change in mitral annular size and geometry after mitraclip® implantation in patients with functional and degenerative mitral regurgitation. J. Interv. Cardiol. 2014, 27, 516–524. [Google Scholar] [CrossRef] [PubMed]
- Schueler, R.; Momcilovic, D.; Weber, M.; Welz, A.; Werner, N.; Mueller, C.; Ghanem, A.; Nickenig, G.; Hammerstingl, C. Acute changes of mitral valve geometry during interventional edge-to-edge repair with the MitraClip system are associated with midterm outcomes in patients with functional valve disease: Preliminary results from a prospective single-center study. Circ. Cardiovasc. Interv. 2014, 7, 390–399. [Google Scholar] [CrossRef] [PubMed]
- Hirasawa, K.; Namazi, F.; Pio, S.M.; Vo, N.M.; Marsan, N.A.; Bax, J.J.; Delgado, V. Insufficient Mitral Leaflet Remodeling in Relation to Annular Dilation and Risk of Residual Mitral Regurgitation After MitraClip Implantation. JACC Cardiovasc. Imaging 2021, 14, 756–765. [Google Scholar] [CrossRef] [PubMed]
- Silva, I.; Turgeon, P.Y.; Paradis, J.-M.; Beaudoin, J.; O’Connor, K.; Ternacle, J.; Alperi, A.; Panagides, V.; Mesnier, J.; Gravel, C.; et al. Percutaneous Transcatheter Edge-to-Edge Mitral Valve Repair With MitraClip System in the Era of G4. Struct. Heart 2022, 100114. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Overall (n = 116) | Early-Generation (n = 76) | 4th-Generation (n = 40) | p Value | |
|---|---|---|---|---|
| Age, years | 73.8 ± 8.8 | 74.5 ± 7.9 | 72.8 ± 10.3 | 0.32 |
| Female | 41 (35.4) | 25 (32.9) | 16 (40) | 0.45 |
| Body surface area | 1.84 ± 0.22 | 1.82 ± 0.22 | 1.86 ± 0.23 | 0.33 |
| Hypertension | 85 (73.2) | 58 (76.3) | 27 (67.5) | 0.31 |
| Diabetes | 46 (39.7) | 31 (40.8) | 15 (37.5) | 0.73 |
| Dyslipidemia | 69 (59.5) | 42 (55.3) | 27 (67.5) | 0.21 |
| Chronic kidney disease | 67 (57.8) | 42 (55.3) | 25 (62.5) | 0.45 |
| Peripheral artery disease | 21 (18.1) | 13 (17.1) | 8 (20) | 0.71 |
| Chronic obstructive pulmonary disease | 27 (23.3) | 19 (25) | 8 (20) | 0.55 |
| Malignancy | 5 (6.6) | 2 (5) | 0.74 | |
| PCI | 45 (38.8) | 28 (36.8) | 17 (42.5) | 0.55 |
| CABG | 13 (11.3) | 9 (12) | 4 (10) | 0.75 |
| Atrial fibrillation | 71 (61.2) | 47 (61.8) | 24 (60) | 0.85 |
| Prior aortic valve replacement | 1 (0.9) | 1 (1.3) | 0 | 0.46 |
| Pacemaker | 10 (8.6) | 7 (9.2) | 3 (7.5) | 0.76 |
| ICD | 27 (23.3) | 19 (25) | 8 (20) | 0.55 |
| Cardiac resynchronization therapy | 13 (11.2) | 10 (13.2) | 3 (7.5) | 0.35 |
| Creatinine, mg/dl | 1.5 ± 0.8 | 1.49 ± 1.1 | 1.52 ± 0.67 | 0.85 |
| Hemoglobin, g/dl | 11.94 ± 1.8 | 11.97 ± 1.9 | 11.91 ± 1.6 | 0.86 |
| NYHA I-III | 75 (64.6) | 51 (77.1) | 25 (62.5) | 0.62 |
| NYHA IV | 41 (35.4) | 25 (32.9) | 15 (37.5) | |
| STS-PROM | 4.3 (2.61–2.16) | 4.2 (2.7–6.7) | 4.6 (2.3–5.8) | 0.85 |
| Baseline medical treatment | ||||
| ARNI/RASI | 74 (63.8) | 50 (65.8) | 24 (60) | 0.54 |
| MRA | 8 (7) | 6 (8) | 2 (5) | 0.55 |
| Beta-blockers | 97 (84.4) | 64 (85.3) | 33 (82.5) | 0.69 |
| Loop diuretics | 107 (93) | 72 (96) | 35 (87.5) | 0.11 |
| OAC | 73 (62.9) | 47 (61.8) | 26 (65) | 0.74 |
| Overall (n = 116) | Early-Generation (n = 76) | 4th-Generation (n = 40) | p Value | |
|---|---|---|---|---|
| LVEF, % | 41.4 ± 13 | 41.1 ± 12.9 | 41.9 ± 14.3 | 0.77 |
| iTDLVV, mL/m2 | 79 ± 29 | 82.1 ± 31.1 | 72 ± 25 | 0.11 |
| iTDLVD, mm/m2 | 31.9 ± 6.9 | 32.4 ± 7.1 | 30.6 ± 6.3 | 0.19 |
| Left atrial volume, mL | 108.8 ± 42 | 108.2 ± 50 | 110.8 ± 36 | 0.83 |
| TAPSE, mm | 18 ± 3.8 | 18 ± 3.6 | 18.1 ± 4.2 | 0.92 |
| RVTDD, mm | 42.5 ± 6.4 | 42.4 ± 5.9 | 42.9 ± 7.3 | 0.74 |
| PASP, mmHg | 47.1 ± 14.5 | 46.2 ± 14.4 | 48.6 ± 14.8 | 0.47 |
| MR grade, | 0.09 | |||
| Grade 3+ | 22 (19) | 18 (23.7) | 4 (10) | |
| Grade 4+ | 94 (81) | 58 (76.3) | 36 (90) | |
| ERO, cm2 | 0.39 ± 0.12 | 0.39 ± 0.10 | 0.39 ± 0.17 | 0.77 |
| Systolic reversal pulmonary vein flow (n = 76) | 42 (55.3) | 27 (47.4) | 15 (78.9) | 0.03 |
| Mitral valve anatomical characteristics | ||||
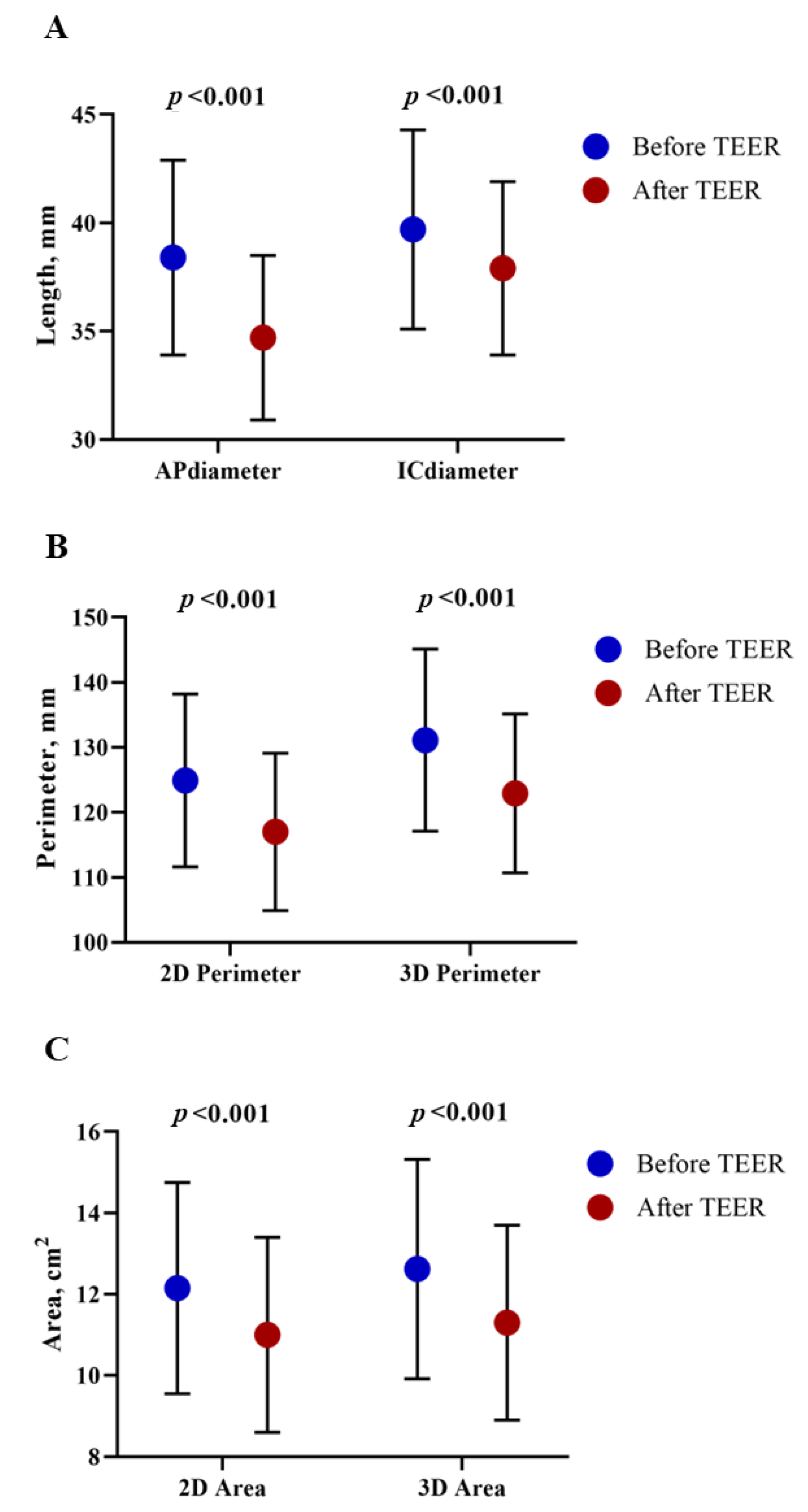
| Anteroposterior diameter, mm | 38.4 ± 4.5 | 38.3 ± 4.9 | 38.8 ± 3.7 | 0.53 |
| Intercommissural diameter, mm | 39.7 ± 4.6 | 39.44 ± 4.72 | 40.41 ± 4.33 | 0.27 |
| 2D annular perimeter, mm | 124.9 ± 13.3 | 124.4 ± 13.4 | 126.1 ± 13.3 | 0.50 |
| 3D annular perimeter, mm | 131.1 ± 14 | 130.3 ± 14.4 | 132.5 ± 13.2 | 0.43 |
| 2D annular area, cm2 | 12.15 ± 2.7 | 12.01 ± 2.7 | 12.4 ± 2.6 | 0.43 |
| 3D annular area, cm2 | 12.62 ± 2.8 | 12.49 ± 2.8 | 12.88 ± 2.7 | 0.46 |
| Anterior leaflet angulation, ° | 26.8 ± 5.6 | 27.1 ± 6.1 | 25.7 ± 3.5 | 0.18 |
| Posterior leaflet angulation, ° | 40.3 ± 8.7 | 40.7 ± 9.8 | 39.4 ± 5.2 | 0.49 |
| Anterior leaflet length, mm | 26.1 ± 3.2 | 25.81 ± 3.1 | 26.4 ± 3.4 | 0.34 |
| Posterior leaflet length, mm | 13.22 ± 2.5 | 13.4 ± 2.42 | 12.9 ± 2.83 | 0.32 |
| Overall (n = 116) | Early-Generation (n = 76) | 4th-Generation (n = 40) | p Value | |
|---|---|---|---|---|
| Numbers of Clips implanted | 1.51 ± 0.5 | 1.47 ± 0.5 | 1.57 ± 0.6 | 0.37 |
| Types of Clips | ||||
| 1st Generation | 18 (23.7) | |||
| 2nd Generation | 17 (22.4) | |||
| 3rd Generation | ||||
| NTr | 8 (10.5) | |||
| XTr | 33 (43.4) | |||
| 4th Generation | ||||
| NT | 1 (2.5) | |||
| NTw | 13 (32.5) | |||
| XT | 3 (7.5) | |||
| XTw | 23 (57.5) | |||
| Vascular access | 0.35 | |||
| Right femoral | 115 (99.1) | 76 (100) | 39 (97.5) | |
| Left femoral | 1 (0.9) | 1 (2.5) | ||
| Timing of intervention | 0.04 | |||
| Elective | 77 (66.4) | 56 (73.7) | 21 (52.5) | |
| Urgent | 26 (22.4) | 13 (17.1) | 13 (32.5) | |
| Emergent | 13 (11.2) | 7 (9.2) | 6 (15) | |
| Procedural complications | ||||
| Tamponade | 2 (1.7) | 1 (1.3) | 1 (2.5) | 0.98 |
| Stroke | 0 | 0 | 0 | NA |
| SLDA | 2 (1.7) | 1 (1.3) | 1 (2.5) | 0.98 |
| Embolization | 0 | 0 | 0 | NA |
| Technical success | 113 (97.4) | 74 (97.3) | 39 (97.5) | 0.99 |
| MR after intervention | 0.65 | |||
| 1+ | 84 (72.41) | 55 (72.36) | 29 (72.5) | |
| 2+ | 20 (17.24) | 14 (18.42) | 7 (17.5) | |
| 3+ | 10 (8.62) | 6 (7.89) | 3 (7.5) | |
| 4+ | 2 (1.72) | 1 (1.32) | 1 (2.5) | |
| Mean diastolic gradient, mmHg | 3.45 ± 1.3 | 3.43 ± 1.3 | 3.50 ± 1.5 | 0.79 |
| Early Generation (n = 76) | 4th Generation (n = 40) | Difference † | p Value | |
|---|---|---|---|---|
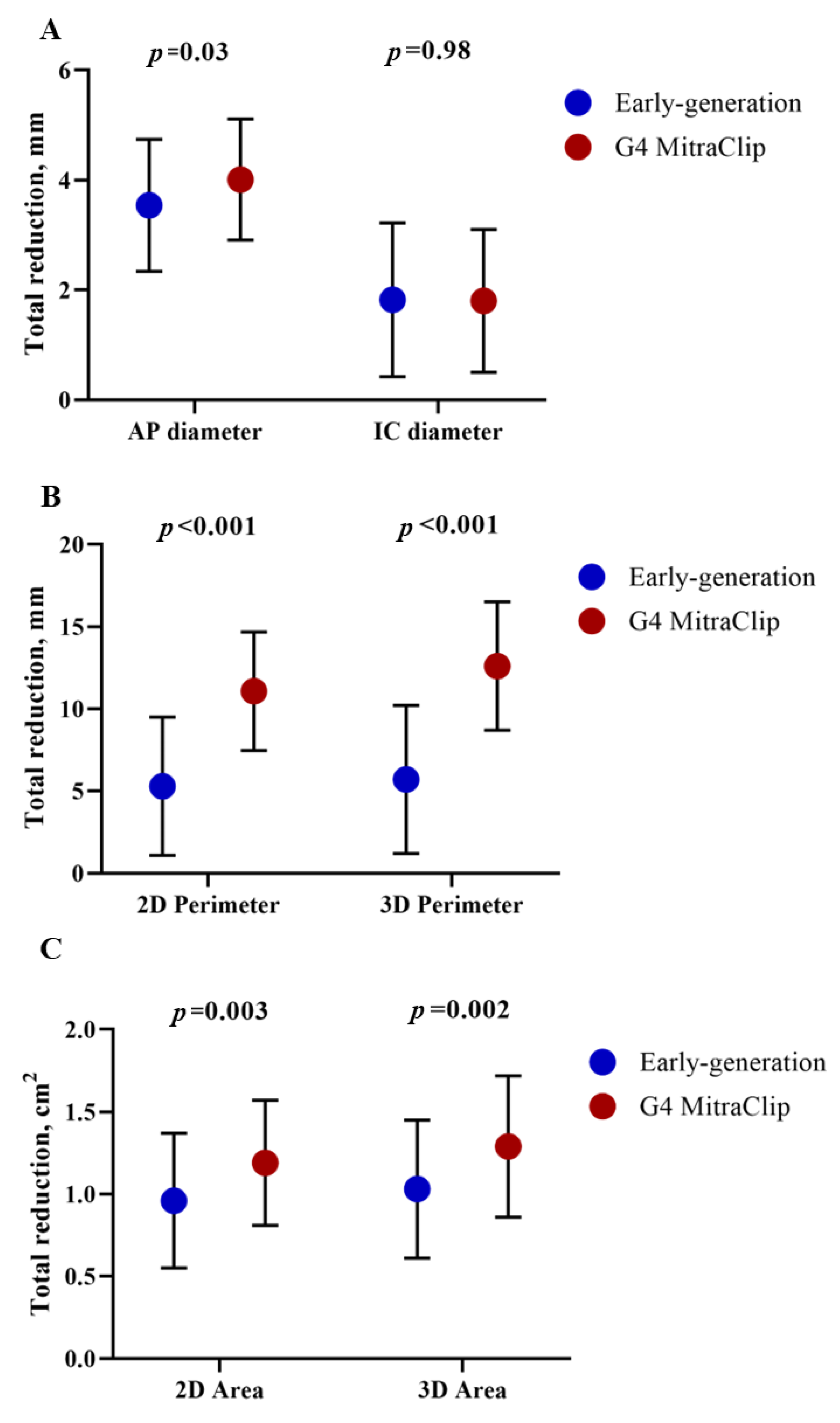
| δAnteroposterior diameter, mm | 3.54 ± 1.2 | 4.01 ± 1.1 | 0.47 | 0.03 |
| δIntercommissural diameter, mm | 1.82 ± 1.4 | 1.81 ± 1.3 | 0.01 | 0.98 |
| δ2D annular perimeter, mm | 5.29 ± 4.2 | 11.07 ± 3.6 | 5.8 | 0.001 |
| δ3D annular perimeter, mm | 5.70 ± 4.5 | 12.61 ± 3.9 | 6.9 | 0.001 |
| δ2D annular area, cm2 | 0.96 ± 0.41 | 1.19 ± 0.38 | 0.22 | 0.003 |
| δ3D annular area, cm2 | 1.03 ± 0.42 | 1.29 ± 0.43 | 0.26 | 0.002 |
| Overall (n = 116) | Early Generation (n = 76) | 4th Generation (n = 40) | p Value | |
|---|---|---|---|---|
| All-cause mortality | 2 (1.72) | 1 (1.32) | 1 (2.5) | 0.64 |
| Stroke | 0 | 0 | 0 | NA |
| Major vascular complication | 0 | 0 | 0 | NA |
| Minor vascular complication | 3 (2.59) | 2 (2.63) | 1 (2.5) | 0.97 |
| Major bleeding | 2 (1.72) | 1 (1.32) | 1 (2.5) | 0.64 |
| AKI stages 2 or 3 | 8 (6.9) | 5 (6.6) | 3 (7.5) | 0.86 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alperi, A.; Avanzas, P.; Martinez, J.; Adeba, A.; Silva, I.; Leon, V.; Antuna, P.; Hernández-Vaquero, D.; Barja, N.; Fernández, F.; et al. Anatomical Changes after Transcatheter Edge-to-Edge Repair in Functional MR According to MitraClip Generation. J. Clin. Med. 2023, 12, 1486. https://doi.org/10.3390/jcm12041486
Alperi A, Avanzas P, Martinez J, Adeba A, Silva I, Leon V, Antuna P, Hernández-Vaquero D, Barja N, Fernández F, et al. Anatomical Changes after Transcatheter Edge-to-Edge Repair in Functional MR According to MitraClip Generation. Journal of Clinical Medicine. 2023; 12(4):1486. https://doi.org/10.3390/jcm12041486
Chicago/Turabian StyleAlperi, Alberto, Pablo Avanzas, Javier Martinez, Antonio Adeba, Iria Silva, Victor Leon, Paula Antuna, Daniel Hernández-Vaquero, Noemi Barja, Félix Fernández, and et al. 2023. "Anatomical Changes after Transcatheter Edge-to-Edge Repair in Functional MR According to MitraClip Generation" Journal of Clinical Medicine 12, no. 4: 1486. https://doi.org/10.3390/jcm12041486