
Aneurysmal Subarachnoid Hemorrhage in Hospitalized Patients on Anticoagulants—A Two Center Matched Case-Control Study
 , , ,
, , ,
Abstract
:1. Introduction
2. Methods
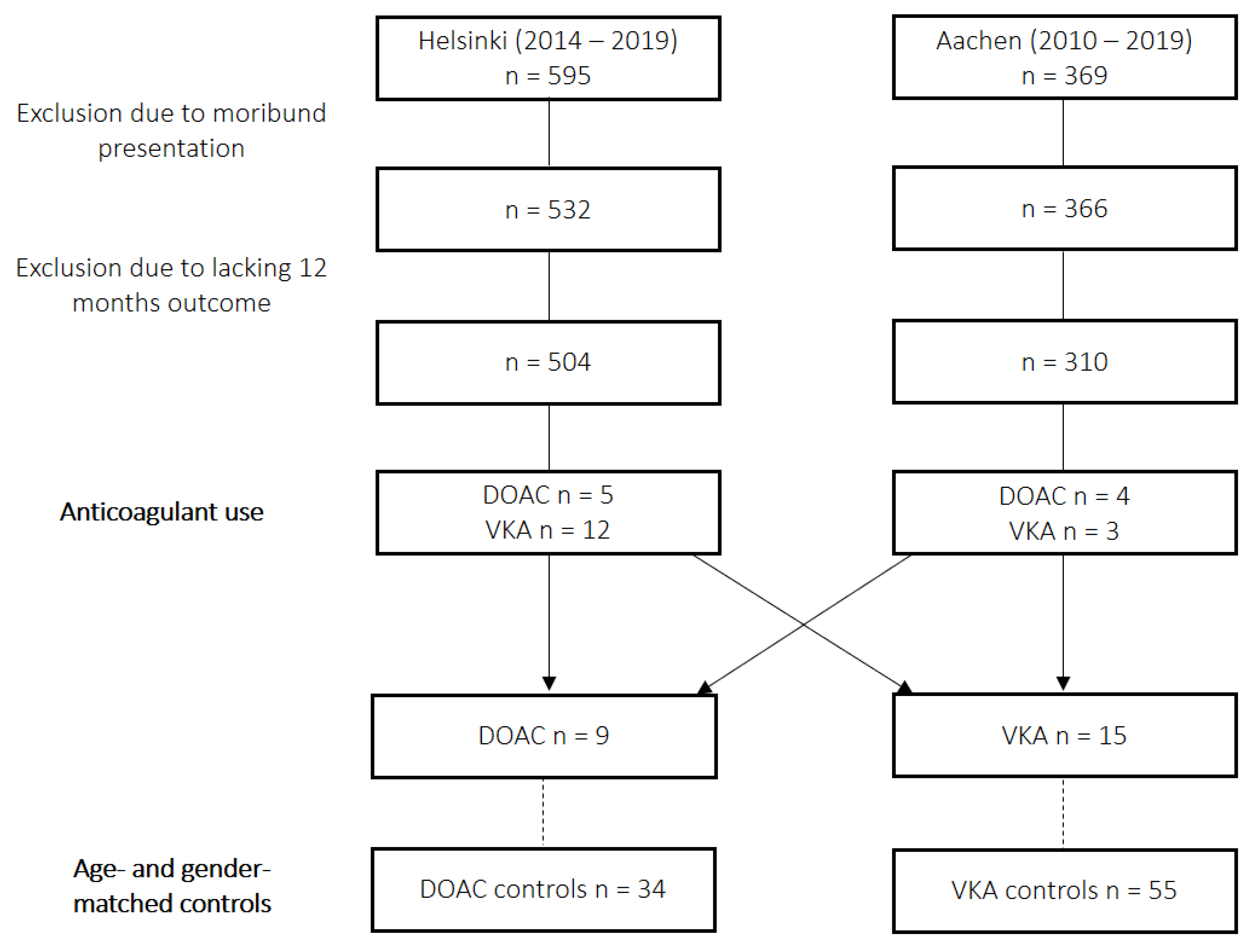
2.1. Patient Population and Study Design
2.2. Standard of Care
2.3. Design and Outcome Parameters
2.4. Statistical Analysis
3. Results
3.1. Patient Inclusion and Baseline Characteristics
3.2. Hemorrhage Severity
3.3. Effects on Clinical Outcome
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| aOR | Adjusted odds ratio |
| CI | Confidence interval |
| CT | Computed tomography |
| DCI | Delayed cerebral ischemia |
| DOAC | Direct oral anticoagulant |
| GOS | Glasgow outcome scale |
| ICH | Intracerebral hemorrhage |
| ICP | Intracranial pressure |
| INR | International normalized ratio |
| IVH | Intraventricular hemorrhage |
| IQR | Interquartile range |
| PCC | Prothrombin complex concentrate |
| PT | Prothrombin time |
| SAH | Aneurysmal subarachnoid hemorrhage |
| VKA | Vitamin K antagonist |
| WFNS | World Federation of Neurological Surgeons |
References
- Connolly, S.J.; Ezekowitz, M.D.; Yusuf, S.; Eikelboom, J.; Oldgren, J.; Parekh, A.; Pogue, J.; Reilly, P.A.; Themeles, E.; Varrone, J.; et al. Dabigatran versus warfarin in patients with atrial fibrillation. N. Engl. J. Med. 2009, 361, 1139–1151. [Google Scholar] [CrossRef] [PubMed]
- Giugliano, R.P.; Ruff, C.T.; Braunwald, E.; Murphy, S.A.; Wiviott, S.D.; Halperin, J.L.; Waldo, A.L.; Ezekowitz, M.D.; Weitz, J.I.; Špinar, J.; et al. Edoxaban versus warfarin in patients with atrial fibrillation. N. Engl. J. Med. 2013, 369, 2093–2104. [Google Scholar] [CrossRef] [PubMed]
- Granger, C.B.; Alexander, J.H.; McMurray, J.J.; Lopes, R.D.; Hylek, E.M.; Hanna, M.; Al-Khalidi, H.R.; Ansell, J.; Atar, D.; Avezum, A.; et al. Apixaban versus warfarin in patients with atrial fibrillation. N. Engl. J. Med. 2011, 365, 981–992. [Google Scholar] [CrossRef]
- Patel, M.R.; Mahaffey, K.W.; Garg, J.; Pan, G.; Singer, D.E.; Hacke, W.; Breithardt, G.; Halperin, J.L.; Hankey, G.J.; Piccini, J.P.; et al. Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. N. Engl. J. Med. 2011, 365, 883–891. [Google Scholar] [CrossRef] [PubMed]
- Raval, A.N.; Cigarroa, J.E.; Chung, M.K.; Diaz-Sandoval, L.J.; Diercks, D.; Piccini, J.P.; Jung, H.S.; Washam, J.B.; Welch, B.G.; Zazulia, A.R.; et al. Management of patients on non-vitamin k antagonist oral anticoagulants in the acute care and periprocedural setting: A scientific statement from the american heart association. Circulation 2017, 135, e604–e633. [Google Scholar] [CrossRef]
- Chan, N.; Sobieraj-Teague, M.; Eikelboom, J.W. Direct oral anticoagulants: Evidence and unresolved issues. Lancet 2020, 396, 1767–1776. [Google Scholar] [CrossRef]
- Mekaj, Y.H.; Mekaj, A.Y.; Duci, S.B.; Miftari, E.I. New oral anticoagulants: Their advantages and disadvantages compared with vitamin K antagonists in the prevention and treatment of patients with thromboembolic events. Ther. Clin. Risk Manag. 2015, 11, 967–977. [Google Scholar] [CrossRef]
- Croci, D.M.; Kamenova, M.; Guzman, R.; Mariani, L.; Soleman, J. Novel oral anticoagulants in patients undergoing cranial surgery. World Neurosurg. 2017, 105, 841–848. [Google Scholar] [CrossRef]
- Pollack, C.V., Jr.; Reilly, P.A.; Eikelboom, J.; Glund, S.; Verhamme, P.; Bernstein, R.A.; Dubiel, R.; Huisman, M.V.; Hylek, E.M.; Kamphuisen, P.W.; et al. Idarucizumab for dabigatran reversal. N. Engl. J. Med. 2015, 373, 511–520. [Google Scholar] [CrossRef]
- Ansell, J.; Laulicht, B.E.; Bakhru, S.H.; Burnett, A.; Jiang, X.; Chen, L.; Baker, C.; Villano, S.; Steiner, S. Ciraparantag, an anticoagulant reversal drug: Mechanism of action, pharmacokinetics, and reversal of anticoagulants. Blood 2021, 137, 115–125. [Google Scholar] [CrossRef]
- Siegal, D.M.; Curnutte, J.T.; Connolly, S.J.; Lu, G.; Conley, P.B.; Wiens, B.L.; Mathur, V.S.; Castillo, J.; Bronson, M.D.; Leeds, J.M.; et al. Andexanet alfa for the reversal of factor xa inhibitor activity. N. Engl. J. Med. 2015, 373, 2413–2424. [Google Scholar] [CrossRef] [PubMed]
- Claassen, J.; Park, S. Spontaneous subarachnoid haemorrhage. Lancet 2022, 400, 846–862. [Google Scholar] [CrossRef] [PubMed]
- Rautalin, I.; Korja, M. Transient intracranial circulatory arrest evidenced at the time of intracranial aneurysm rupture: Case report. Neurocrit. Care 2021, 34, 340–342. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.; van Gelder, J.M. The probability of sudden death from rupture of intracranial aneurysms: A meta-analysis. Neurosurgery 2002, 51, 1101–1105, discussion 1105–1107. [Google Scholar] [CrossRef] [PubMed]
- Swieringa, F.; Spronk, H.M.H.; Heemskerk, J.W.M.; van der Meijden, P.E.J. Integrating platelet and coagulation activation in fibrin clot formation. Res. Pract. Thromb. Haemost. 2018, 2, 450–460. [Google Scholar] [CrossRef] [PubMed]
- Naidech, A.M.; Janjua, N.; Kreiter, K.T.; Ostapkovich, N.D.; Fitzsimmons, B.F.; Parra, A.; Commichau, C.; Connolly, E.S.; Mayer, S.A. Predictors and impact of aneurysm rebleeding after subarachnoid hemorrhage. Arch Neurol. 2005, 62, 410–416. [Google Scholar] [CrossRef] [PubMed]
- Tang, C.; Zhang, T.S.; Zhou, L.F. Risk factors for rebleeding of aneurysmal subarachnoid hemorrhage: A meta-analysis. PLoS ONE 2014, 9, e99536. [Google Scholar] [CrossRef]
- Garbe, E.; Kreisel, S.H.; Behr, S. Risk of subarachnoid hemorrhage and early case fatality associated with outpatient antithrombotic drug use. Stroke 2013, 44, 2422–2426. [Google Scholar] [CrossRef]
- Risselada, R.; Straatman, H.; van Kooten, F.; Dippel, D.W.; van der Lugt, A.; Niessen, W.J.; Firouzian, A.; Herings, R.M.; Sturkenboom, M.C. Platelet aggregation inhibitors, vitamin K antagonists and risk of subarachnoid hemorrhage. J. Thromb. Haemost. 2011, 9, 517–523. [Google Scholar] [CrossRef]
- Witt, D.M.; Nieuwlaat, R.; Clark, N.P.; Ansell, J.; Holbrook, A.; Skov, J.; Shehab, N.; Mock, J.; Myers, T.; Dentali, F.; et al. American society of hematology 2018 guidelines for management of venous thromboembolism: Optimal management of anticoagulation therapy. Blood Adv. 2018, 2, 3257–3291. [Google Scholar] [CrossRef]
- Cuker, A.; Burnett, A.; Triller, D.; Crowther, M.; Ansell, J.; Van Cott, E.M.; Wirth, D.; Kaatz, S. Reversal of direct oral anticoagulants: Guidance from the anticoagulation forum. Am. J. Hematol. 2019, 94, 697–709. [Google Scholar] [CrossRef] [PubMed]
- Piran, S.; Khatib, R.; Schulman, S.; Majeed, A.; Holbrook, A.; Witt, D.M.; Wiercioch, W.; Schünemann, H.J.; Nieuwlaat, R. Management of direct factor xa inhibitor-related major bleeding with prothrombin complex concentrate: A meta-analysis. Blood Adv. 2019, 3, 158–167. [Google Scholar] [CrossRef] [PubMed]
- Virta, J.J.; Satopää, J.; Luostarinen, T.; Raj, R. One-year outcome after aneurysmal subarachnoid hemorrhage in elderly patients. World Neurosurg. 2020, 143, e334–e343. [Google Scholar] [CrossRef] [PubMed]
- Veldeman, M.; Albanna, W.; Weiss, M.; Conzen, C.; Schmidt, T.P.; Schulze-Steinen, H.; Wiesmann, M.; Clusmann, H.; Schubert, G.A. Invasive neuromonitoring with an extended definition of delayed cerebral ischemia is associated with improved outcome after poor-grade subarachnoid hemorrhage. J. Neurosurg. 2020, 134, 1527–1534. [Google Scholar] [CrossRef] [PubMed]
- Frontera, J.A.; Claassen, J.; Schmidt, J.M.; Wartenberg, K.E.; Temes, R.; Connolly, E.S., Jr.; MacDonald, R.L.; Mayer, S.A. Prediction of symptomatic vasospasm after subarachnoid hemorrhage: The modified fisher scale. Neurosurgery 2006, 59, 21–27, discussion 21–27. [Google Scholar] [CrossRef]
- Rosen, D.S.; Macdonald, R.L. Subarachnoid hemorrhage grading scales: A systematic review. Neurocrit. Care 2005, 2, 110–118. [Google Scholar] [CrossRef]
- Jennett, B.; Bond, M. Assessment of outcome after severe brain damage. Lancet 1975, 1, 480–484. [Google Scholar] [CrossRef]
- Vergouwen, M.D.; Vermeulen, M.; van Gijn, J.; Rinkel, G.J.; Wijdicks, E.F.; Muizelaar, J.P.; Mendelow, A.D.; Juvela, S.; Yonas, H.; Terbrugge, K.G.; et al. Definition of delayed cerebral ischemia after aneurysmal subarachnoid hemorrhage as an outcome event in clinical trials and observational studies: Proposal of a multidisciplinary research group. Stroke 2010, 41, 2391–2395. [Google Scholar] [CrossRef]
- Schmidt, T.P.; Weiss, M.; Hoellig, A.; Nikoubashman, O.; Schulze-Steinen, H.; Albanna, W.; Clusmann, H.; Schubert, G.A.; Veldeman, M. Revisiting the timeline of delayed cerebral ischemia after aneurysmal subarachnoid hemorrhage: Toward a temporal risk profile. Neurocrit. Care 2022, 37, 735–743. [Google Scholar] [CrossRef]
- Levy, M.M.; Fink, M.P.; Marshall, J.C.; Abraham, E.; Angus, D.; Cook, D.; Cohen, J.; Opal, S.M.; Vincent, J.L.; Ramsay, G. 2001 sccm/esicm/accp/ats/sis international sepsis definitions conference. Crit Care Med. 2003, 31, 1250–1256. [Google Scholar] [CrossRef]
- Ye, F.; Keep, R.F.; Hua, Y.; Garton, H.J.; Xi, G. Acute micro-thrombosis after subarachnoid hemorrhage: A new therapeutic target? J. Cereb. Blood Flow Metab. 2021, 41, 2470–2472. [Google Scholar] [CrossRef]
- Dienel, A.; Ammassam Veettil, R.; Hong, S.H.; Matsumura, K.; Kumar, T.P.; Yan, Y.; Blackburn, S.L.; Ballester, L.Y.; Marrelli, S.P.; McCullough, L.D.; et al. Microthrombi correlates with infarction and delayed neurological deficits after subarachnoid hemorrhage in mice. Stroke 2020, 51, 2249–2254. [Google Scholar] [CrossRef] [PubMed]
- Kole, M.J.; Wessell, A.P.; Ugiliweneza, B.; Cannarsa, G.J.; Fortuny, E.; Stokum, J.A.; Shea, P.; Chryssikos, T.; Khattar, N.K.; Crabill, G.A.; et al. Low-dose intravenous heparin infusion after aneurysmal subarachnoid hemorrhage is associated with decreased risk of delayed neurological deficit and cerebral infarction. Neurosurgery 2021, 88, 523–530. [Google Scholar] [CrossRef]
- James, R.F. Aneurysmal Subarachnoid Hemorrhage Trial Randomizing Heparin (Astroh). 2015. Available online: https://clinicaltrials.gov/ct2/show/NCT02501434 (accessed on 5 January 2023).
- Afzal, S.; Zaidi, S.T.R.; Merchant, H.A.; Babar, Z.U.; Hasan, S.S. Prescribing trends of oral anticoagulants in England over the last decade: A focus on new and old drugs and adverse events reporting. J. Thromb. Thrombolysis 2021, 52, 646–653. [Google Scholar] [CrossRef]
- Flaherty, M.L.; Kissela, B.; Woo, D.; Kleindorfer, D.; Alwell, K.; Sekar, P.; Moomaw, C.J.; Haverbusch, M.; Broderick, J.P. The increasing incidence of anticoagulant-associated intracerebral hemorrhage. Neurology 2007, 68, 116–121. [Google Scholar] [CrossRef] [PubMed]
- Zirlik, A.; Bode, C. Vitamin K antagonists: Relative strengths and weaknesses vs. Direct oral anticoagulants for stroke prevention in patients with atrial fibrillation. J. Thromb. Thrombolysis 2017, 43, 365–379. [Google Scholar] [CrossRef] [PubMed]
- Foerch, C.; Lo, E.H.; van Leyen, K.; Lauer, A.; Schaefer, J.H. Intracerebral hemorrhage formation under direct oral anticoagulants. Stroke 2019, 50, 1034–1042. [Google Scholar] [CrossRef] [PubMed]
- Inohara, T.; Xian, Y.; Liang, L.; Matsouaka, R.A.; Saver, J.L.; Smith, E.E.; Schwamm, L.H.; Reeves, M.J.; Hernandez, A.F.; Bhatt, D.L.; et al. Association of intracerebral hemorrhage among patients taking non-vitamin k antagonist vs vitamin k antagonist oral anticoagulants with in-hospital mortality. JAMA 2018, 319, 463–473. [Google Scholar] [CrossRef] [PubMed]
- Kurogi, R.; Nishimura, K.; Nakai, M.; Kada, A.; Kamitani, S.; Nakagawara, J.; Toyoda, K.; Ogasawara, K.; Ono, J.; Shiokawa, Y.; et al. Comparing intracerebral hemorrhages associated with direct oral anticoagulants or warfarin. Neurology 2018, 90, e1143–e1149. [Google Scholar] [CrossRef]
- Vlak, M.H.; Algra, A.; Brandenburg, R.; Rinkel, G.J. Prevalence of unruptured intracranial aneurysms, with emphasis on sex, age, comorbidity, country, and time period: A systematic review and meta-analysis. Lancet Neurol. 2011, 10, 626–636. [Google Scholar] [CrossRef]
- Schievink, W.I. Intracranial aneurysms. N. Engl. J. Med. 1997, 336, 28–40. [Google Scholar] [CrossRef] [PubMed]
- Lawton, M.T.; Vates, G.E. Subarachnoid hemorrhage. N. Engl. J. Med. 2017, 377, 257–266. [Google Scholar] [CrossRef] [PubMed]
- Tarlov, N.; Norbash, A.M.; Nguyen, T.N. The safety of anticoagulation in patients with intracranial aneurysms. J. Neurointerv. Surg. 2013, 5, 405–409. [Google Scholar] [CrossRef] [PubMed]
- Shono, Y.; Sugimori, H.; Matsuo, R.; Fukushima, Y.; Wakisaka, Y.; Kuroda, J.; Ago, T.; Kamouchi, M.; Kitazono, T. Safety of antithrombotic therapy for patients with acute ischemic stroke harboring unruptured intracranial aneurysm. Int. J. Stroke 2018, 13, 734–742. [Google Scholar] [CrossRef]
- Olsen, M.; Johansen, M.B.; Christensen, S.; Sørensen, H.T. Use of vitamin K antagonists and risk of subarachnoid haemorrhage: A population-based case-control study. Eur. J. Intern. Med. 2010, 21, 297–300. [Google Scholar] [CrossRef]
- Vergouwen, M.D.; Rinkel, G.J.; Algra, A.; Fiehler, J.; Steinmetz, H.; Vajkoczy, P.; Rutten, F.H.; Luntz, S.; Hänggi, D.; Etminan, N. Prospective Randomized open-label Trial to evaluate risk factor management in patients with unruptured intracranial aneurysms: Study protocol. Int. J. Stroke 2018, 13, 992–998. [Google Scholar] [CrossRef]
- Rinkel, G.J.; Prins, N.E.; Algra, A. Outcome of aneurysmal subarachnoid hemorrhage in patients on anticoagulant treatment. Stroke 1997, 28, 6–9. [Google Scholar] [CrossRef]
- Bijlenga, P.; Gondar, R.; Schilling, S.; Morel, S.; Hirsch, S.; Cuony, J.; Corniola, M.V.; Perren, F.; Rüfenacht, D.; Schaller, K. PHASES score for the management of intracranial aneurysm: A cross-sectional population-based retrospective study. Stroke 2017, 48, 2105–2112. [Google Scholar] [CrossRef]
- Bassand, J.P.; Virdone, S.; Badoz, M.; Verheugt, F.W.A.; Camm, A.J.; Cools, F.; Fox, K.A.A.; Goldhaber, S.Z.; Goto, S.; Haas, S.; et al. Bleeding and related mortality with noacs and vkas in newly diagnosed atrial fibrillation: Results from the garfield-af registry. Blood Adv. 2021, 5, 1081–1091. [Google Scholar] [CrossRef]


{kind=link}
| All (n = 43) | DOAC (n = 9) | Controls (n = 34) | p-Value | |
|---|---|---|---|---|
| Demographics | ||||
| Age—yrs.—median (Q1–Q3) | 67.5 (62.1–76.5) | 66.6 (61.5–78.7) | 68.1 (61.9–75.6) | 0.895 |
| Sex—Female/Male- no. (%) | 25 (58.1)/18 (41.9) | 5 (55.6)/4 (44.4) | 20 (58.8)/14 (41.2) | 0.860 |
| Comorbidity—no. (%) | ||||
| Hypertension | 26 (60.5) | 5 (55.6) | 21 (61.8) | 0.735 |
| Smoking | 13 (30.2) | 2 (22.2) | 11 (32.4) | 0.556 |
| Diabetes type 2 | 2 (4.7) | 2 (22.2) | 0 | n/a |
| Coronary artery disease | 2 (4.7) | 1 (11.1) | 1 (2.9) | 0.301 |
| Coagulation status on admission | ||||
| INR—median (Q1–Q3) | 1.1 (1.0–1.1) | 1.1 (1.1–1.2) | 1.0 (1.0–1.1) | 0.081 |
| Thrombocyte count (103/µL)—median (Q1–Q3) | 241.0 (209.0–291.0) | 235.0 (185.0–452.0) | 243.5 (211.5–283.5) | 0.895 |
| Aneurysm location—no. (%) | ||||
| Acomm | 16 (37.2) | 4 (44.4) | 12 (35.3) | 0.256 |
| MCA | 10 (23.3) | 1 (11.1) | 9 (26.5) | |
| ICA (incl. Pcomm) | 11 (25.6) | 4 (44.4) | 7 (20.6) | |
| Others | 6 (14.0) | 0 (0) | 6 (17.6) | |
| Ant. circulation | 37 (86.0) | 9 (100.0) | 28 (82.4) | 0.174 |
| Max. diameter (mm)—median (Q1–Q3) | 6.0 (4.3–9.0) | 5.0 (3.0–7.0) | 7.0 (4.9–9.5) | 0.135 |
| Aneurysm occlusion—no. (%) | ||||
| Clipping/Endovascular | 13 (30.2)/30 (69.8) | 1 (11.1)/8 (88.9) | 12 (35.3)/22 (64.7) | 0.160 |
| Hemorrhage severity | ||||
| WFNS grade—no. (%) | 0.777 | |||
| Grade 1 | 9 (20.9) | 1 (11.1) | 8 (23.5) | |
| Grade 2 | 10 (23.3) | 2 (22.2) | 8 (23.5) | |
| Grade 3 | 6 (14.0) | 1 (11.1) | 5 (14.7) | |
| Grade 4 | 6 (14.0) | 1 (11.1) | 5 (14.7) | |
| Grade 5 | 12 (27.9) | 4 (44.4) | 8 (23.5) | |
| Poor-grade SAH (WFNS4–5) | 18 (41.9) | 5 (55.6) | 13 (38.2) | 0.349 |
| Modified Fisher scale—no. (%) | 0.558 | |||
| Grade 1 | 8 (18.6) | 1 (11.1) | 7 (20.6) | |
| Grade 2 | 5 (11.6) | 2 (22.2) | 3 (8.8) | |
| Grade 3 | 9 (20.9) | 1 (11.1) | 8 (23.5) | |
| Grade 4 | 21 (48.8) | 5 (55.6) | 16 (47.1) | |
| IVH | 26 (60.5) | 7 (77.8) | 19 (55.9) | 0.296 |
| ICH | 15 (34.9) | 4 (44.4) | 11 (32.4) | 0.499 |
| Acute hydrocephalus | 27 (62.8) | 8 (88.9) | 19 (55.9) | 0.069 |
| All (n = 70) | VKA (n = 15) | Controls (n = 55) | p-Value | |
|---|---|---|---|---|
| Demographics | ||||
| Age—yrs.—median (Q1–Q3) | 73.0 (65.0–76.8) | 73.0 (66.4–76.6) | 73.0 (63.8 - 77.6) | 0.869 |
| Sex—Female/Male- no. (%) | 38 (54.3)/32 (45.7) | 8 (53.3)/7 (46.7) | 30 (54.5)/25 (45.5) | 0.933 |
| Comorbidity—no. (%) | ||||
| Hypertension | 39 (55.7) | 13 (86.7) | 26 (47.3) | 0.006 |
| Smoking | 17 (24.3) | 3 (20.0) | 14 (25.5) | 0.662 |
| Diabetes type 2 | 6 (8.6) | 3 (20.0) | 3 (5.5) | 0.074 |
| Coronary artery disease | 3 (4.3) | 3 (20.0) | 0 (0) | 0.001 |
| Coagulation status on admission | ||||
| INR—median (Q1–Q3) | 1.1 (1.0–1.2) | 2.2 (1.4–3.0) | 1.1 (1.0–1.1) | <0.001 |
| Thrombocyte count (103/µL)—median (Q1–Q3) | 241.0 (194.5–278.0) | 221.0 (171.0–260.0) | 242.0 (208.3–290.5) | 0.169 |
| Aneurysm location—no. (%) | ||||
| Acomm | 23 (32.9) | 5 (33.3) | 18 (32.7) | 0.094 |
| MCA | 16 (22.9) | 2 (13.3) | 14 (25.5) | |
| ICA (incl. Pcomm) | 14 (20.0) | 1 (6.7) | 13 (23.6) | |
| Others | 17 (24.3) | 7 (46.7) | 10 (18.2) | |
| Ant. circulation | 53 (75.7) | 8 (53.3) | 45 (81.8) | 0.023 |
| Max. diameter (mm)—median (Q1–Q3) | 6.0 (4.0–8.0) | 6.2 (4.5–9.0) | 6.0 (4.0–8.0) | 0.873 |
| Aneurysm occlusion—no. (%) | ||||
| Clipping/Endovascular | 23 (32.9)/47 (67.1) | 3 (20.0)/12 (80.0) | 20 (36.4)/35 (63.6) | 0.232 |
| Hemorrhage severity | ||||
| WFNS grade—no. (%) | 0.331 | |||
| Grade 1 | 23 (32.9) | 6 (40.0) | 17 (30.9) | |
| Grade 2 | 9 (12.9) | 1 (6.7) | 8 (14.5) | |
| Grade 3 | 10 (14.3) | 0 (0) | 10 (18.2) | |
| Grade 4 | 12 (17.1) | 3 (20.0) | 9 (16.4) | |
| Grade 5 | 16 (22.9) | 5 (33.3) | 11 (20.0) | |
| Poor-grade SAH (WFNS4–5) | 28 (40.0) | 8 (53.3) | 20 (36.4) | 0.234 |
| Modified Fisher scale—no. (%) | 0.528 | |||
| Grade 1 | 11 (15.7) | 2 (13.3) | 9 (16.4) | |
| Grade 2 | 5 (7.1) | 2 (13.3) | 3 (5.5) | |
| Grade 3 | 17 (24.3) | 2 (13.3) | 15 (23.3) | |
| Grade 4 | 37 (52.9) | 9 (60.0) | 28 (50.9) | |
| IVH | 40 (57.1) | 11 (73.3) | 29 (52.7) | 0.153 |
| ICH | 22 (31.4) | 5 (33.3) | 17 (30.9) | 0.858 |
| Acute hydrocephalus | 46 (65.7) | 12 (80.0) | 34 (61.8) | 0.189 |
| All (n = 43) | DOAC (n = 9) | Controls (n = 34) | p-Value | |
|---|---|---|---|---|
| ICU-related complications | ||||
| Mechanical ventilation—no. (%) | 28 (65.1) | 9 (100) | 19 (55.9) | 0.014 |
| Sepsis—no. (%) | 3 (7.0) | 2 (22.2) | 1 (2.9) | 0.043 |
| DCI occurrence—no. (%) | 15 (34.9%) | 2 (22.2) | 13 (38.2) | 0.370 |
| Clinical outcome | ||||
| In-hospital mortality—no. (%) | 7 (16.3) | 3 (33.3) | 4 (11.8) | 0.119 |
| GOS 12 months—no. (%) | 0.892 | |||
| Good recovery | 10 (23.3) | 2 (22.2) | 8 (23.5) | |
| Moderate disability | 8 (18.6) | 1 (11.1) | 7 (20.6) | |
| Severe disability | 14 (32.6) | 3 (33.3) | 11 (32.4) | |
| Vegetative state | 1 (2.3) | 0 (0) | 1 (2.9) | |
| Dead | 10 (23.3) | 3 (33.3) | 7 (20.6) | |
| Unfavorable outcome (GOS1–3) | 25 (58.1) | 6 (66.7) | 19 (55.9) | 0.560 |
| All (n = 70) | VKA (n = 15) | Controls (n = 55) | p-Value | |
| ICU-related complications | ||||
| Mechanical ventilation—no. (%) | 50 (71.4) | 38 (69.1) | 12 (80.0) | 0.407 |
| Sepsis—no. (%) | 9 (12.9) | 7 (12.7) | 2 (13.3) | 0.950 |
| DCI occurrence—no. (%) | 21 (30.0) | 17 (30.9) | 4 (26.7) | 0.751 |
| Clinical outcome | ||||
| In hospital mortality—no. (%) | 19 (27.1) | 3 (20.0) | 16 (29.1) | 0.483 |
| GOS 12 months—no. (%) | 0.907 | |||
| Good recovery | 22 (31.4) | 3 (20.0) | 19 (34.5) | |
| Moderate disability | 11 (15.7) | 1 (6.7) | 10 (18.2) | |
| Severe disability | 13 (18.6) | 6 (40.0) | 7 (12.7) | |
| Vegetative state | 3 (4.3) | 1 (6.7) | 2 (3.6) | |
| Dead | 21 (30.0) | 4 (26.7) | 17 (30.9) | |
| Unfavorable outcome (GOS1–3) | 37 (52.9) | 11 (73.3) | 26 (47.3) | 0.073 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Veldeman, M.; Rossmann, T.; Weiss, M.; Conzen-Dilger, C.; Korja, M.; Hoellig, A.; Virta, J.J.; Satopää, J.; Luostarinen, T.; Clusmann, H.; et al. Aneurysmal Subarachnoid Hemorrhage in Hospitalized Patients on Anticoagulants—A Two Center Matched Case-Control Study. J. Clin. Med. 2023, 12, 1476. https://doi.org/10.3390/jcm12041476
Veldeman M, Rossmann T, Weiss M, Conzen-Dilger C, Korja M, Hoellig A, Virta JJ, Satopää J, Luostarinen T, Clusmann H, et al. Aneurysmal Subarachnoid Hemorrhage in Hospitalized Patients on Anticoagulants—A Two Center Matched Case-Control Study. Journal of Clinical Medicine. 2023; 12(4):1476. https://doi.org/10.3390/jcm12041476
Chicago/Turabian StyleVeldeman, Michael, Tobias Rossmann, Miriam Weiss, Catharina Conzen-Dilger, Miikka Korja, Anke Hoellig, Jyri J. Virta, Jarno Satopää, Teemu Luostarinen, Hans Clusmann, and et al. 2023. "Aneurysmal Subarachnoid Hemorrhage in Hospitalized Patients on Anticoagulants—A Two Center Matched Case-Control Study" Journal of Clinical Medicine 12, no. 4: 1476. https://doi.org/10.3390/jcm12041476