
Do Interleukin-1 and Interleukin-6 Antagonists Hold Any Place in the Treatment of Atherosclerotic Cardiovascular Disease and Related Co-Morbidities? An Overview of Available Clinical Evidence

Abstract
:1. Introduction
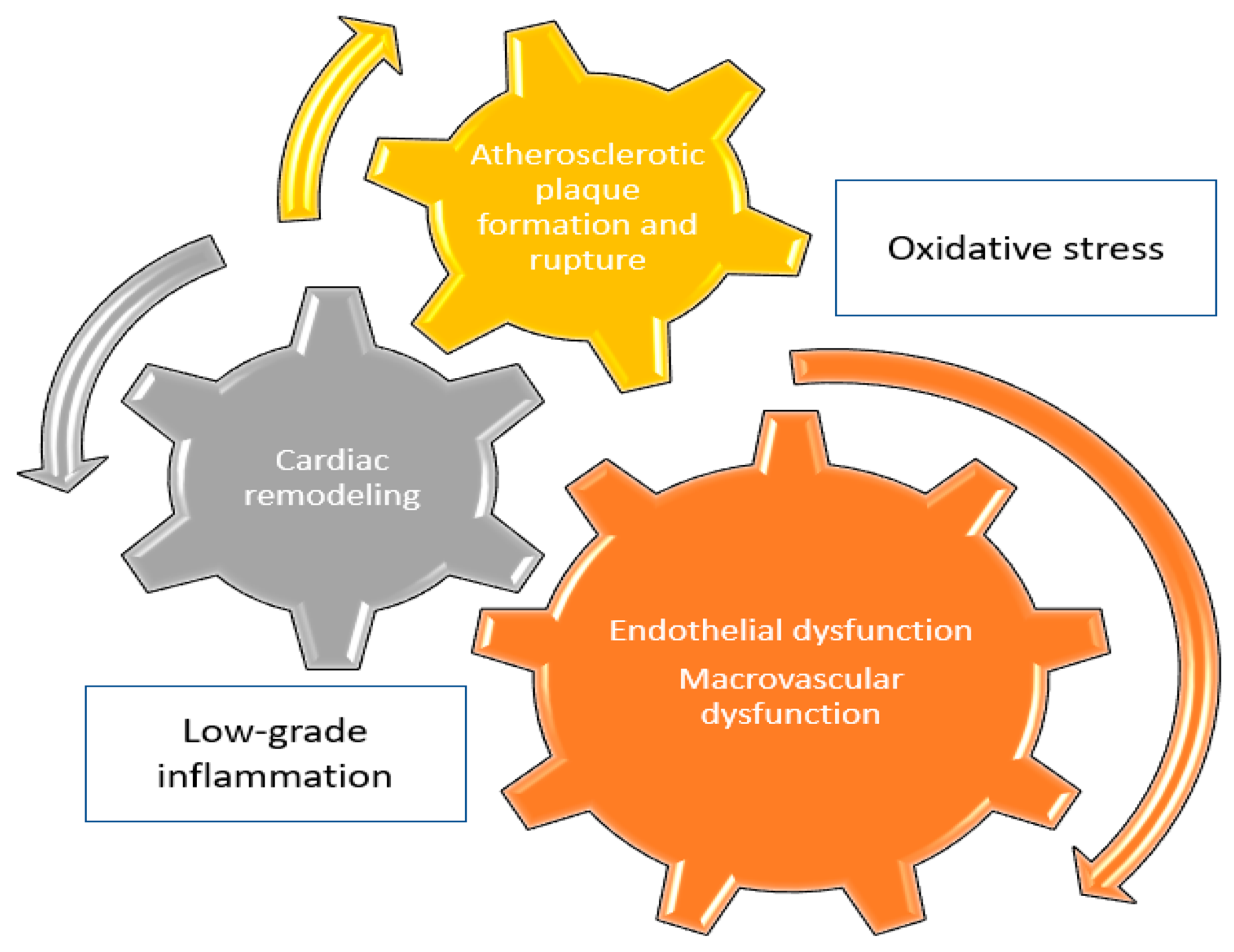
2. Inflammation & Cardiovascular Disease
2.1. The Role of Interleukin-1
2.1.1. Atherosclerosis
2.1.2. Major Adverse Cardiovascular Events
2.1.3. Peripheral Artery Disease
2.1.4. Arterial Hypertension
2.2. The Role of Interleukin-6
2.2.1. Atherosclerosis
2.2.2. Major Adverse Cardiovascular Events
2.2.3. Peripheral Artery Disease
2.2.4. Arterial Hypertension
3. IL-1 and IL-6 Antagonists for the Treatment of CVD
3.1. IL-1 Antagonists
- Anakinra
- Canakinumab
- Rilonacept
3.2. IL-6 Antagonists
- Tocilizumab
- Sarilumab
- Ziltivekimab
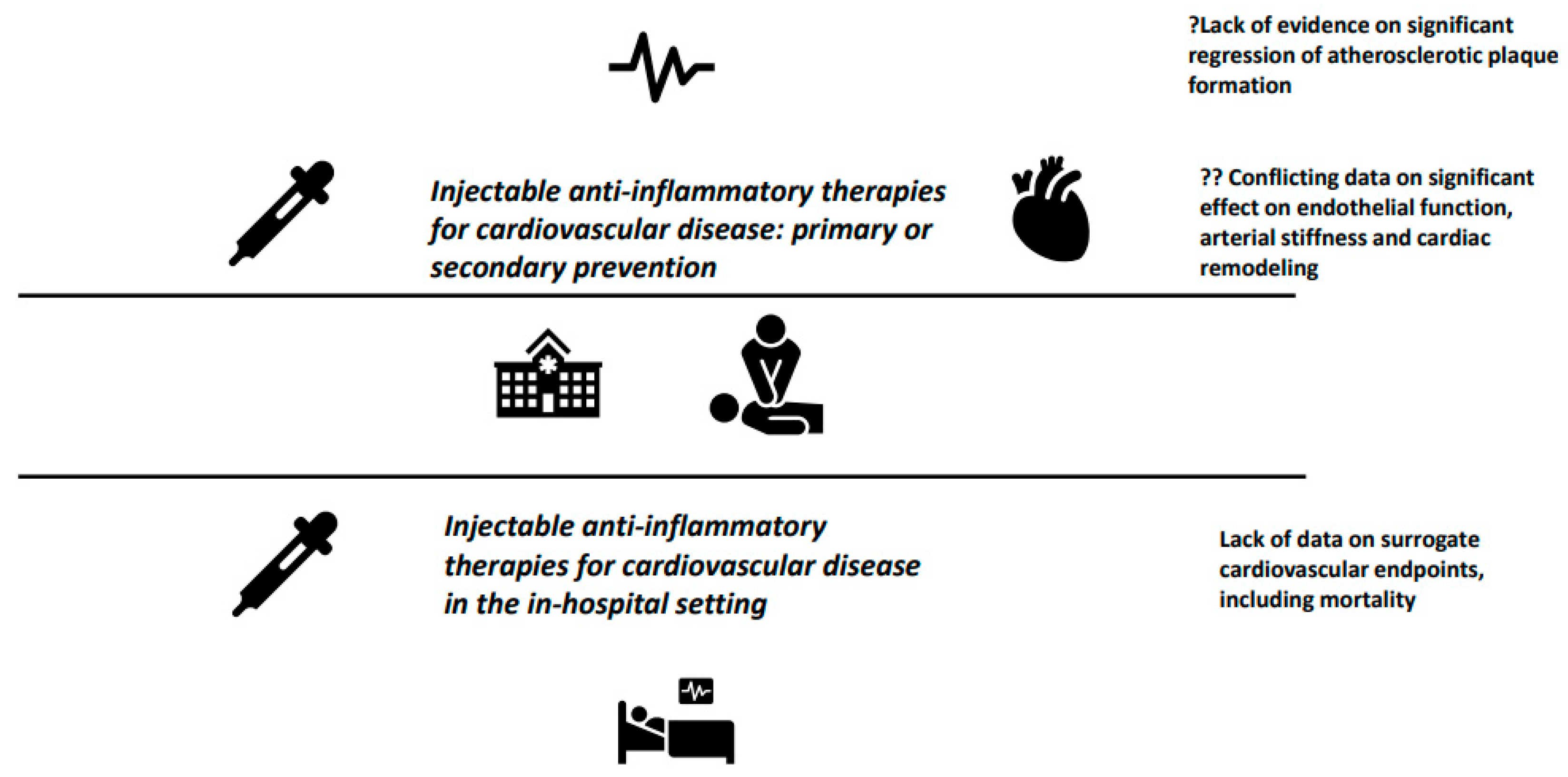
4. Future Perspectives and Concluding Remarks
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Available online: https://www.cdc.gov/nchs/fastats/leading-causes-of-death.htm (accessed on 1 January 2023).
- Available online: https://ec.europa.eu/eurostat/statistics-explained/index.php?title=Causes_of_death_statistics (accessed on 1 January 2023).
- Raggi, P.; Genest, J.; Giles, J.T.; Rayner, K.J.; Dwivedi, G.; Beanlands, R.S.; Gupta, M. Role of inflammation in the pathogenesis of atherosclerosis and therapeutic interventions. Atherosclerosis 2018, 276, 98–108. [Google Scholar] [CrossRef] [PubMed]
- Ruparelia, N.; Choudhury, R. Inflammation and atherosclerosis: What is on the horizon? Heart 2020, 106, 80–85. [Google Scholar] [CrossRef] [PubMed]
- Liberale, L.; Badimon, L.; Montecucco, F.; Lüscher, T.F.; Libby, P.; Camici, G.G. Inflammation, Aging, and Cardiovascular Disease: JACC Review Topic of the Week. J. Am. Coll. Cardiol. 2022, 79, 837–847. [Google Scholar] [CrossRef] [PubMed]
- Sproston, N.R.; Ashworth, J.J. Role of C-Reactive Protein at Sites of Inflammation and Infection. Front. Immunol. 2018, 9, 754. [Google Scholar] [CrossRef]
- Emerging Risk Factors Collaboration Kaptoge, S.; Di Angelantonio, E.; Lowe, G.; Pepys, M.B.; Thompson, S.G.; Collins, R.; Danesh, J. C-reactive protein concentration and risk of coronary heart disease, stroke, and mortality: An individual participant meta-analysis. Lancet 2010, 375, 132–140. [Google Scholar] [CrossRef]
- Li, Y.; Zhong, X.; Cheng, G.; Zhao, C.; Zhang, L.; Hong, Y.; Wan, Q.; He, R.; Wang, Z. Hs-CRP and all-cause, cardiovascular, and cancer mortality risk: A meta-analysis. Atherosclerosis 2017, 259, 75–82. [Google Scholar] [CrossRef]
- Hansson, G.K.; Libby, P.; Tabas, I. Inflammation and plaque vulnerability. J. Intern. Med. 2015, 278, 483–493. [Google Scholar] [CrossRef]
- Lo Gullo, A.; Mandraffino, G.; Imbalzano, E.; Mamone, F.; Aragona, C.O.; D’Ascola, A.; Loddo, S.; Cinquegrani, A.; Alibrandi, A.; Mormina, E.; et al. Toll-like receptor 3 and interleukin 1β expression in CD34+ cells from patients with rheumatoid arthritis: Association with inflammation and vascular involvement. Clin. Exp. Rheumatol. 2014, 32, 922–929. [Google Scholar]
- Ikonomidis, I.; Andreotti, F.; Economou, E.; Stefanadis, C.; Toutouzas, P.; Nihoyannopoulos, P. Increased proinflammatory cytokines in patients with chronic stable angina and their reduction by aspirin. Circulation 1999, 100, 793–798. [Google Scholar] [CrossRef]
- Herder, C.; de Las Heras Gala, T.; Carstensen-Kirberg, M.; Huth, C.; Zierer, A.; Wahl, S.; Sudduth-Klinger, J.; Kuulasmaa, K.; Peretz, D.; Ligthart, S.; et al. Circulating Levels of Interleukin 1-Receptor Antagonist and Risk of Cardiovascular Disease: Meta-Analysis of Six Population-Based Cohorts. Arterioscler. Thromb. Vasc. Biol. 2017, 37, 1222–1227. [Google Scholar] [CrossRef]
- Sun, Y.; Pavey, H.; Wilkinson, I.; Fisk, M. Role of the IL-33/ST2 axis in cardiovascular disease: A systematic review and meta-analysis. PLoS ONE 2021, 16, e0259026. [Google Scholar] [CrossRef] [PubMed]
- Naka, K.K.; Bechlioullis, A.; Marini, A.; Sionis, D.; Vakalis, K.; Triantis, G.; Wilkins, L.; Rogus, J.; Kornman, K.S.; Witztum, J.L.; et al. Interleukin-1 genotypes modulate the long-term effect of lipoprotein(a) on cardiovascular events: The Ioannina Study. J. Clin. Lipidol. 2018, 12, 338–347. [Google Scholar] [CrossRef] [PubMed]
- Hoel, H.; Ueland, T.; Knudsen, A.; Kjær, A.; Michelsen, A.E.; Sagen, E.L.; Halvorsen, B.; Yndestad, A.; Nielsen, S.D.; Aukrust, P.; et al. Soluble Markers of Interleukin 1 Activation as Predictors of First-Time Myocardial Infarction in HIV-Infected Individuals. J. Infect. Dis. 2020, 221, 506–509. [Google Scholar] [CrossRef] [PubMed]
- Fiotti, N.; Giansante, C.; Ponte, E.; Delbello, C.; Calabrese, S.; Zacchi, T.; Dobrina, A.; Guarnieri, G. Atherosclerosis and inflammation. Patterns of cytokine regulation in patients with peripheral arterial disease. Atherosclerosis 1999, 145, 51–60. [Google Scholar] [CrossRef]
- Andreozzi, G.M.; Martini, R.; Cordova, R.; D’Eri, A.; Salmistraro, G.; Mussap, M.; Plebani, M. Circulating levels of cytokines (IL-6 and IL-1beta) in patients with intermittent claudication, at rest, after maximal exercise treadmill test and during restore phase. Could they be progression markers of the disease? Int. Angiol. 2007, 26, 245–252. [Google Scholar]
- Jayedi, A.; Rahimi, K.; Bautista, L.E.; Nazarzadeh, M.; Zargar, M.S.; Shab-Bidar, S. Inflammation markers and risk of developing hypertension: A meta-analysis of cohort studies. Heart 2019, 105, 686–692. [Google Scholar] [CrossRef]
- Kim, S.K.; Kim, K.S.; Lee, Y.S.; Park, S.H.; Choe, J.Y. Arterial stiffness and proinflammatory cytokines in fibromyalgia syndrome. Clin. Exp. Rheumatol. 2010, 28 (Suppl. S63), S71–S77. [Google Scholar]
- Tuttolomondo, A.; Pecoraro, R.; Buttà, C.; Di Raimondo, D.; Ferrante, A.; Della Corte, V.; Ciccia, F.; Bellia, C.; Giardina, A.; Raffa, A.; et al. Arterial stiffness indexes and serum cytokine levels in seronegative spondyloarthritis: Relationships between stiffness markers and metabolic and immunoinflammatory variables. Scand. J. Rheumatol. 2015, 44, 474–479. [Google Scholar] [CrossRef]
- Tyrrell, D.J.; Goldstein, D.R. Ageing and atherosclerosis: Vascular intrinsic and extrinsic factors and potential role of IL-6. Nat. Rev. Cardiol. 2021, 18, 58–68. [Google Scholar] [CrossRef]
- Du, W.; Wong, C.; Song, Y.; Shen, H.; Mori, D.; Rotllan, N.; Price, N.; Dobrian, A.D.; Meng, H.; Kleinstein, S.H.; et al. Age-associated vascular inflammation promotes monocytosis during atherogenesis. Aging Cell. 2016, 15, 766–777. [Google Scholar] [CrossRef]
- Song, Y.; Shen, H.; Schenten, D.; Shan, P.; Lee, P.J.; Goldstein, D.R. Aging enhances the basal production of IL-6 and CCL2 in vascular smooth muscle cells. Arterioscler. Thromb. Vasc. Biol. 2012, 32, 103–109. [Google Scholar] [CrossRef]
- Huber, S.A.; Sakkinen, P.; Conze, D.; Hardin, N.; Tracy, R. Interleukin-6 exacerbates early atherosclerosis in mice. Arterioscler. Thromb. Vasc. Biol. 1999, 19, 2364–2367. [Google Scholar] [CrossRef]
- Zhang, B.; Li, X.L.; Zhao, C.R.; Pan, C.L.; Zhang, Z. Interleukin-6 as a Predictor of the Risk of Cardiovascular Disease: A Meta-Analysis of Prospective Epidemiological Studies. Immunol Investig. 2018, 47, 689–699. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Liu, W.; Xie, J. Circulating interleukin-6 levels and cardiovascular and all-cause mortality in the elderly population: A meta-analysis. Arch. Gerontol. Geriatr. 2017, 73, 257–262. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Cen, K.; Sun, W.; Feng, B. Predictive Value of Blood Interleukin-6 Level in Patients with Acute Coronary Syndrome: A Meta-analysis. Immunol. Investig. 2021, 50, 964–976. [Google Scholar] [CrossRef] [PubMed]
- Papadopoulos, A.; Palaiopanos, K.; Björkbacka, H.; Peters, A.; de Lemos, J.A.; Seshadri, S.; Dichgans, M.; Georgakis, M.K. Circulating Interleukin-6 Levels and Incident Ischemic Stroke: A Systematic Review and Meta-analysis of Prospective Studies. Neurology 2022, 98, e1002–e1012. [Google Scholar] [CrossRef] [PubMed]
- Whiteley, W.; Jackson, C.; Lewis, S.; Lowe, G.; Rumley, A.; Sandercock, P.; Wardlaw, J.; Dennis, M.; Sudlow, C. Inflammatory markers and poor outcome after stroke: A prospective cohort study and systematic review of interleukin-6. PLoS Med. 2009, 6, e1000145. [Google Scholar] [CrossRef]
- Chen, J.; Han, L.; Xu, X.; Tang, H.; Wang, H.; Wei, B. Serum biomarkers VEGF-C and IL-6 are associated with severe human Peripheral Artery Stenosis. J. Inflamm. 2015, 12, 50. [Google Scholar] [CrossRef]
- Danielsson, P.; Truedsson, L.; Eriksson, K.F.; Norgren, L. Inflammatory markers and IL-6 polymorphism in peripheral arterial disease with and without diabetes mellitus. Vasc. Med. 2005, 10, 191–198. [Google Scholar] [CrossRef]
- Tzoulaki, I.; Murray, G.D.; Lee, A.J.; Rumley, A.; Lowe, G.D.; Fowkes, F.G. Inflammatory, haemostatic, and rheological markers for incident peripheral arterial disease: Edinburgh Artery Study. Eur. Heart J. 2007, 28, 354–362. [Google Scholar] [CrossRef]
- Ueki, Y.; Miura, T.; Miyashita, Y.; Ebisawa, S.; Motoki, H.; Izawa, A.; Koyama, J.; Ikeda, U. Inflammatory Cytokine Levels After Endovascular Therapy in Patients with Peripheral Artery Disease. Angiology 2017, 68, 734–740. [Google Scholar] [CrossRef] [PubMed]
- Cheang, I.; Zhu, X.; Lu, X.; Yue, X.; Tang, Y.; Gao, R.; Liao, S.; Yao, W.; Zhou, Y.; Zhang, H.; et al. Associations of Inflammation with Risk of Cardiovascular and All-Cause Mortality in Adults with Hypertension: An Inflammatory Prognostic Scoring System. J. Inflamm. Res. 2022, 15, 6125–6136. [Google Scholar] [CrossRef] [PubMed]
- Abbate, A.; Van Tassell, B.W.; Biondi-Zoccai, G.; Kontos, M.C.; Grizzard, J.D.; Spillman, D.W.; Oddi, C.; Roberts, C.S.; Melchior, R.D.; Mueller, G.H.; et al. Effects of interleukin-1 blockade with anakinra on adverse cardiac remodeling and heart failure after acute myocardial infarction [from the Virginia Commonwealth University-Anakinra Remodeling Trial (2) (VCU-ART2) pilot study]. Am. J. Cardiol. 2013, 111, 1394–1400. [Google Scholar] [CrossRef]
- Ikonomidis, I.; Pavlidis, G.; Katsimbri, P.; Andreadou, I.; Triantafyllidi, H.; Tsoumani, M.; Varoudi, M.; Vlastos, D.; Makavos, G.; Kostelli, G.; et al. Differential effects of inhibition of interleukin 1 and 6 on myocardial, coronary and vascular function. Clin. Res. Cardiol. 2019, 108, 1093–1101. [Google Scholar] [CrossRef] [PubMed]
- Ikonomidis, I.; Tzortzis, S.; Andreadou, I. Increased benefit of interleukin-1 inhibition on vascular function, myocardial deformation, and twisting in patients with coronary artery disease and coexisting rheumatoid arthritis. Circ. Cardiovasc. Imaging 2014, 7, 619–628. [Google Scholar] [CrossRef] [PubMed]
- Morton, A.C.; Rothman, A.M.; Greenwood, J.P. The effect of interleukin-1 receptor antagonist therapy on markers of inflammation in non-ST elevation acute coronary syndromes: The MRC-ILA Heart Study. Eur Heart J. 2015, 36, 377–384. [Google Scholar] [CrossRef]
- Abbate, A.; Trankle, C.R.; Buckley, L.F.; Lipinski, M.J.; Appleton, D.; Kadariya, D.; Canada, J.M.; Carbone, S.; Roberts, C.S.; Abouzaki, N.; et al. Interleukin-1 Blockade Inhibits the Acute Inflammatory Response in Patients with ST-Segment-Elevation Myocardial Infarction. J. Am. Heart Assoc. 2020, 9, e014941. [Google Scholar] [CrossRef]
- Vasan, R.S.; Sullivan, L.M.; Roubenoff, R. Inflammatory markers and risk of heart failure in elderly subjects without prior myocardial infarction: The Framingham Heart Study. Circulation 2003, 107, 1486–1491. [Google Scholar] [CrossRef]
- Mann, D.L. Innate immunity and the failing heart: The cytokine hypothesis revisited. Circ. Res. 2015, 116, 1254–1268. [Google Scholar] [CrossRef]
- Mihalick, V.; Wohlford, G.; Talasaz, A.H.; Kim, F.; Canada, J.M.; Carbone, S.; Kadariya, D.; Billingsley, H.; Trankle, C. Patient Perceptions of Exertion and Dyspnea with Interleukin-1 Blockade in Patients With Recently Decompensated Systolic Heart Failure. Am. J. Cardiol. 2022, 174, 61–67. [Google Scholar] [CrossRef]
- Van Tassell, B.W.; Canada, J.; Carbone, S.; Trankle, C.; Buckley, L.; Erdle, C.O.; Abouzaki, N.A.; Dixon, D.; Kadariya, D.; Christopher, S.; et al. Interleukin-1 Blockade in Recently Decompensated Systolic Heart Failure: Results from REDHART (Recently Decompensated Heart Failure Anakinra Response Trial). Circ. Heart Fail. 2017, 10, e004373. [Google Scholar] [CrossRef]
- Van Tassell, B.W.; Trankle, C.R.; Canada, J.M.; Carbone, S.; Buckley, L.; Kadariya, D.; Del Buono, M.G.; Billingsley, H.; Wohlford, G.; Viscusi, M.; et al. IL-1 Blockade in Patients with Heart Failure with Preserved Ejection Fraction. Circ. Heart Fail. 2018, 11, e005036. [Google Scholar] [CrossRef] [PubMed]
- Soon, E.; Holmes, A.M.; Treacy, C.M. Elevated levels of inflammatory cytokines predict survival in idiopathic and familial pulmonary arterial hypertension. Circulation 2010, 122, 920–927. [Google Scholar] [CrossRef]
- Trankle, C.R.; Canada, J.M.; Kadariya, D. IL-1 Blockade Reduces Inflammation in Pulmonary Arterial Hypertension and Right Ventricular Failure: A Single-Arm, Open-Label, Phase IB/II Pilot Study. Am. J. Respir. Crit. Care Med. 2019, 199, 381–384. [Google Scholar] [CrossRef] [PubMed]
- Mostafa, T.M.; Hegazy, S.K.; Elshebini, E.M.; Saif, D.S.; Elabd, A.H. A comparative study on the anti-inflammatory effect of angiotensin-receptor blockers & statins on rheumatoid arthritis disease activity. Indian J. Med. Res. 2020, 152, 393–400. [Google Scholar] [CrossRef] [PubMed]
- Poznyak, A.V.; Bharadwaj, D.; Prasad, G.; Grechko, A.V.; Sazonova, M.A.; Orekhov, A.N. Anti-Inflammatory Therapy for Atherosclerosis: Focusing on Cytokines. Int. J. Mol. Sci. 2021, 22, 7061. [Google Scholar] [CrossRef] [PubMed]
- Ridker, P.M.; Everett, B.M.; Thuren, T.; MacFadyen, J.G.; Chang, W.H.; Ballantyne, C.; Fonseca, F.; Nicolau, J.; Koenig, W.; Anker, S.D.; et al. Antiinflammatory Therapy with Canakinumab for Atherosclerotic Disease. N. Engl. J. Med. 2017, 377, 1119–1131. [Google Scholar] [CrossRef] [PubMed]
- Everett, B.M.; MacFadyen, J.G.; Thuren, T.; Libby, P.; Glynn, R.J.; Ridker, P.M. Inhibition of Interleukin-1β and Reduction in Atherothrombotic Cardiovascular Events in the CANTOS Trial. J. Am. Coll. Cardiol. 2020, 76, 1660–1670. [Google Scholar] [CrossRef] [PubMed]
- Everett, B.M.; Cornel, J.H.; Lainscak, M.; Anker, S.D.; Abbate, A.; Thuren, T.; Libby, P.; Glynn, R.J.; Ridker, P.M. Anti-Inflammatory Therapy with Canakinumab for the Prevention of Hospitalization for Heart Failure. Circulation 2019, 139, 1289–1299. [Google Scholar] [CrossRef]
- Russell, K.S.; Yates, D.P.; Kramer, C.M.; Feller, A.; Mahling, P.; Colin, L.; Clough, T.; Wang, T.; LaPerna, L.; Patel, A.; et al. A randomized, placebo-controlled trial of canakinumab in patients with peripheral artery disease. Vasc. Med. 2019, 24, 414–421. [Google Scholar] [CrossRef]
- Maedler, K.; Sergeev, P.; Ris, F.; Oberholzer, J.; Joller-Jemelka, H.I.; Spinas, G.A.; Kaiser, N.; Halban, P.A.; Donath, M.Y. Glucose-induced beta cell production of IL-1beta contributes to glucotoxicity in human pancreatic islets. J. Clin. Investig. 2002, 110, 851–860, Erratum in J. Clin. Investig. 2017, 127, 1589. [Google Scholar] [CrossRef]
- Larsen, C.M.; Faulenbach, M.; Vaag, A.; Vølund, A.; Ehses, J.A.; Seifert, B.; Mandrup-Poulsen, T.; Donath, M.Y. Interleukin-1-receptor antagonist in type 2 diabetes mellitus. N. Engl. J. Med. 2007, 356, 1517–1526. [Google Scholar] [CrossRef] [PubMed]
- Howard, C.; Noe, A.; Skerjanec, A.; Holzhauer, B.; Wernsing, M.; Ligueros-Saylan, M.; Thuren, T. Safety and tolerability of canakinumab, an IL-1β inhibitor, in type 2 diabetes mellitus patients: A pooled analysis of three randomised double-blind studies. Cardiovasc. Diabetol. 2014, 13, 94. [Google Scholar] [CrossRef] [PubMed]
- Choudhury, R.P.; Birks, J.S.; Mani, V.; Biasiolli, L.; Robson, M.D.; L’Allier, P.L.; Gingras, M.-A.; Alie, N.; McLaughlin, M.A.; Basson, C.T.; et al. Arterial Effects of Canakinumab in Patients with Atherosclerosis and Type 2 Diabetes or Glucose Intolerance. J. Am. Coll. Cardiol. 2016, 68, 1769–1780. [Google Scholar] [CrossRef]
- Klein, A.L.; Imazio, M.; Cremer, P.; Brucato, A.; Abbate, A.; Fang, F.; Insalaco, A.; LeWinter, M.; Lewis, B.S.; Lin, D.; et al. Phase 3 Trial of Interleukin-1 Trap Rilonacept in Recurrent Pericarditis. N. Engl. J. Med. 2021, 384, 31–41. [Google Scholar] [CrossRef]
- Ritschel, V.N.; Seljeflot, I.; Arnesen, H.; Halvorsen, S.; Weiss, T.; Eritsland, J.; Andersen, G. IL-6 signalling in patients with acute ST-elevation myocardial infarction. Results Immunol. 2013, 4, 8–13. [Google Scholar] [CrossRef]
- Westman, P.C.; Lipinski, M.J.; Luger, D.; Waksman, R.; Bonow, R.O.; Wu, E.; Epstein, S.E. Inflammation as a Driver of Adverse Left Ventricular Remodeling After Acute Myocardial Infarction. J. Am. Coll. Cardiol. 2016, 67, 2050–2060. [Google Scholar] [CrossRef]
- Giles, J.T.; Sattar, N.; Gabriel, S.; Ridker, P.M.; Gay, S.; Warne, C.; Musselman, D.; Brockwell, L.; Shittu, E.; Klearman, M.; et al. Cardiovascular Safety of Tocilizumab Versus Etanercept in Rheumatoid Arthritis: A Randomized Controlled Trial. Arthritis Rheumatol. 2020, 72, 31–40. [Google Scholar] [CrossRef]
- McInnes, I.B.; Thompson, L.; Giles, J.T.; Bathon, J.M.; Salmon, J.; Beaulieu, A.D.; Codding, C.; Carlson, T.H.; Delles, C.; Lee, J.S.; et al. Effect of interleukin-6 receptor blockade on surrogates of vascular risk in rheumatoid arthritis: MEASURE, a randomised, placebo-controlled study. Ann. Rheum. Dis. 2015, 74, 694–702. [Google Scholar] [CrossRef]
- Lukas, C.; Redondin, M.; Pane, I.; Soubrier, M.; Houvenagel, E.; Sibilia, J.; Combe, B.; Morel, J. Cardiovascular events and change in cholesterol levels in patients with rheumatoid arthritis treated with tocilizumab: Data from the REGATE Registry. Clin. Exp. Rheumatol. 2021, 39, 501–507. [Google Scholar] [CrossRef]
- Hsieh, M.J.; Lee, C.H.; Tsai, M.L.; Kao, C.-F.; Lan, W.-C.; Huang, Y.-T.; Tseng, W.-Y.; Wen, M.-S.; Chang, S.-H. Biologic Agents Reduce Cardiovascular Events in Rheumatoid Arthritis Not Responsive to Tumour Necrosis Factor Inhibitors: A National Cohort Study. Can. J. Cardiol. 2020, 36, 1739–1746. [Google Scholar] [CrossRef]
- Castagné, B.; Viprey, M.; Martin, J.; Schott, A.M.; Cucherat, M.; Soubrier, M. Cardiovascular safety of tocilizumab: A systematic review and network meta-analysis. PLoS ONE 2019, 14, e0220178. [Google Scholar] [CrossRef]
- Singh, S.; Fumery, M.; Singh, A.G.; Singh, N.; Prokop, L.J.; Dulai, P.S.; Sandborn, W.J.; Curtis, J.R. Comparative Risk of Cardiovascular Events with Biologic and Synthetic Disease-Modifying Antirheumatic Drugs in Patients with Rheumatoid Arthritis: A Systematic Review and Meta-Analysis. Arthritis Care Res. (Hoboken) 2020, 72, 561–576. [Google Scholar] [CrossRef]
- Kobayashi, H.; Kobayashi, Y.; Giles, J.T.; Yoneyama, K.; Nakajima, Y.; Takei, M. Tocilizumab treatment increases left ventricular ejection fraction and decreases left ventricular mass index in patients with rheumatoid arthritis without cardiac symptoms: Assessed using 3.0 tesla cardiac magnetic resonance imaging. J. Rheumatol. 2014, 41, 1916–1921. [Google Scholar] [CrossRef]
- Yokoe, I.; Kobayashi, H.; Kobayashi, Y.; Yoneyama, K.; Kitamura, N.; Takei, M. Impact of tocilizumab on N-terminal pro-brain natriuretic peptide levels in patients with active rheumatoid arthritis without cardiac symptoms. Scand. J. Rheumatol. 2018, 47, 364–370. [Google Scholar] [CrossRef]
- Dubiel-Braszczok, B.; Nowak, K.; Owczarek, A.; Engelmann, M.; Gumkowska-Sroka, O.; Kotyla, P.J. Differential Impact of Biologic Therapy on Heart Function Biomarkers in Rheumatoid Arthritis Patients: Observational Study on Etanercept, Adalimumab, and Tocilizumab. Curr. Pharm. Des. 2022, 28, 2029–2037. [Google Scholar] [CrossRef]
- Orrem, H.L.; Nilsson, P.H.; Pischke, S.E.; Kleveland, O.; Yndestad, A.; Ekholt, K.; Damås, J.K.; Espevik, T.; Bendz, B.; Halvorsen, B.; et al. IL-6 Receptor Inhibition by Tocilizumab Attenuated Expression of C5a Receptor 1 and 2 in Non-ST-Elevation Myocardial Infarction. Front. Immunol. 2018, 9, 2035. [Google Scholar] [CrossRef]
- Helseth, R.; Kleveland, O.; Ueland, T.; Wiseth, R.; Damas, J.K.; Broch, K.; Michelsen, A.; Bendz, B.; Gullestad, L.; Aukrust, P.; et al. Tocilizumab increases citrullinated histone 3 in non-ST segment elevation myocardial infarction. Open Heart 2021, 8, e001492. [Google Scholar] [CrossRef]
- Holte, E.; Kleveland, O.; Ueland, T.; Kunszt, G.; Bratlie, M.; Broch, K.; Michelsen, A.; Bendz, B.; Amundsen, B.H.; Aakhus, S.; et al. Effect of interleukin-6 inhibition on coronary microvascular and endothelial function in myocardial infarction. Heart 2017, 103, 1521–1527. [Google Scholar] [CrossRef]
- Broch, K.; Anstensrud, A.K.; Woxholt, S.; Sharma, K.; Tøllefsen, I.M.; Bendz, B.; Aakhus, S.; Ueland, T.; Amundsen, B.H.; Damås, J.K.; et al. Randomized Trial of Interleukin-6 Receptor Inhibition in Patients with Acute ST-Segment Elevation Myocardial Infarction. J. Am. Coll. Cardiol. 2021, 77, 1845–1855. [Google Scholar] [CrossRef]
- Meyer, M.A.S.; Wiberg, S.; Grand, J.; Meyer, A.S.P.; Obling, L.E.R.; Frydland, M.; Thomsen, J.H.; Josiassen, J.; Møller, J.E.; Kjaergaard, J.; et al. Treatment Effects of Interleukin-6 Receptor Antibodies for Modulating the Systemic Inflammatory Response After Out-of-Hospital Cardiac Arrest (The IMICA Trial): A Double-Blinded, Placebo-Controlled, Single-Center, Randomized, Clinical Trial. Circulation 2021, 143, 1841–1851. [Google Scholar] [CrossRef] [PubMed]
- Gabay, C.; Burmester, G.R.; Strand, V.; Msihid, J.; Zilberstein, M.; Kimura, T.; van Hoogstraten, H.; Boklage, S.H.; Sadeh, J.; Graham, N.M.H.; et al. Sarilumab and adalimumab differential effects on bone remodelling and cardiovascular risk biomarkers, and predictions of treatment outcomes. Arthritis Res. Ther. 2020, 22, 70. [Google Scholar] [CrossRef] [PubMed]
- Ridker, P.M.; Devalaraja, M.; Baeres, F.M.M.; Engelmann, M.D.M.; Hovingh, G.K.; Ivkovic, M.; Lo, L.; Kling, D.; Pergola, P.; Raj, D.; et al. IL-6 inhibition with ziltivekimab in patients at high atherosclerotic risk (RESCUE): A double-blind, randomised, placebo-controlled, phase 2 trial. Lancet 2021, 397, 2060–2069. [Google Scholar] [CrossRef]
- Sethwala, A.M.; Goh, I.; Amerena, J.V. Combating Inflammation in Cardiovascular Disease. Heart Lung Circ. 2021, 30, 197–206. [Google Scholar] [CrossRef] [PubMed]
- Libby, P. Targeting Inflammatory Pathways in Cardiovascular Disease: The Inflammasome, Interleukin-1, Interleukin-6 and Beyond. Cells 2021, 10, 951. [Google Scholar] [CrossRef]
- Grebe, A.; Hoss, F.; Latz, E. NLRP3 Inflammasome and the IL-1 Pathway in Atherosclerosis. Circ. Res. 2018, 122, 1722–1740. [Google Scholar] [CrossRef]
- Ridker, P.M. Anticytokine Agents: Targeting Interleukin Signaling Pathways for the Treatment of Atherothrombosis. Circ. Res. 2019, 124, 437–450. [Google Scholar] [CrossRef]
- Tardif, J.C.; Kouz, S.; Waters, D.D.; Bertrand, O.F.; Diaz, R.; Maggioni, A.P.; Pinto, F.J.; Ibrahim, R.; Gamra, H.; Kiwan, G.S.; et al. Efficacy and Safety of Low-Dose Colchicine after Myocardial Infarction. N. Engl. J. Med. 2019, 381, 2497–2505. [Google Scholar] [CrossRef]
- Nidorf, S.M.; Fiolet, A.T.L.; Mosterd, A.; Eikelboom, J.W.; Schut, A.; Opstal, T.S.J.; The, S.H.K.; Xu, X.-F.; Ireland, M.A.; Lenderink, T.; et al. Colchicine in Patients with Chronic Coronary Disease. N. Engl. J. Med. 2020, 383, 1838–1847. [Google Scholar] [CrossRef]
- Ridker, P.M.; Everett, B.M.; Pradhan, A.; MacFadyen, J.G.; Solomon, D.H.; Zaharris, E.; Mam, V.; Hasan, A.; Rosenberg, Y.; Iturriaga, E.; et al. Low-Dose Methotrexate for the Prevention of Atherosclerotic Events. N. Engl. J. Med. 2019, 380, 752–762. [Google Scholar] [CrossRef]
- Nishiga, M.; Wang, D.W.; Han, Y.; Lewis, D.B.; Wu, J.C. COVID-19 and cardiovascular disease: From basic mechanisms to clinical perspectives. Nat. Rev. Cardiol. 2020, 17, 543–558. [Google Scholar] [CrossRef]
- Alkan, A.; Ugurlu, S. Canakinumab might be Protective against Severe COVID-19 for Patients with Autoinflammatory Disorders. Mediterr. J. Rheumatol. 2022, 33, 237–240. [Google Scholar] [CrossRef] [PubMed]
- Gasparyan, A.Y.; Kitas, G.D. Hyperinflammation due to COVID-19 and the Targeted Use of Interleukin-1 Inhibitors. Mediterr. J. Rheumatol. 2022, 33, 173–175. [Google Scholar] [CrossRef] [PubMed]
- Ridker, P.M.; Howard, C.P.; Walter, V.; Everett, B.; Libby, P.; Hensen, J.; Thuren, T. Effects of interleukin-1β inhibition with canakinumab on hemoglobin A1c, lipids, C-reactive protein, interleukin-6, and fibrinogen: A phase IIb randomized, placebo-controlled trial. Circulation 2012, 126, 2739–2748. [Google Scholar] [CrossRef] [PubMed]
- Gabay, C.; McInnes, I.B.; Kavanaugh, A.; Tuckwell, K.; Klearman, M.; Pulley, J.; Sattar, N. Comparison of lipid and lipid-associated cardiovascular risk marker changes after treatment with tocilizumab or adalimumab in patients with rheumatoid arthritis. Ann. Rheum. Dis. 2016, 75, 1806–1812. [Google Scholar] [CrossRef]
- Emery, P.; Rondon, J.; Parrino, J.; Lin, Y.; Pena-Rossi, C.; Van Hoogstraten, H.; Graham, N.M.H.; Liu, N.; Paccaly, A.; Wu, R.; et al. Safety and tolerability of subcutaneous sarilumab and intravenous tocilizumab in patients with rheumatoid arthritis. Rheumatology 2019, 58, 849–858. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Study | Type of Study | Treatment Duration | Study Population | Utilized IL-1 Antagonist | Comparator | Main Findings |
|---|---|---|---|---|---|---|
| Anakinra | ||||||
| Abbate et al., 2013 [35] | Randomized controlled trial | 14 days | 10 patients with ST-segment elevation acute myocardial infarction | Anakinra 100 mg once daily | Placebo | Anakinra compared to placebo resulted in:
|
| Ikonomidis et al., 2014 [37] | Randomized controlled trial | 3 h | 60 patients with RA and coronary artery disease (CAD), 20 patients with RA without CAD and 30 healthy controls | Anakinra 100 mg as a single dose | Anakinra compared to placebo resulted in:
| |
| Morton et al., 2015 [38] | Randomized controlled trial | 14 days | 182 patients with non-ST elevation acute coronary syndrome | Anakinra 100 mg once daily | Placebo | Anakinra compared to placebo resulted in:
|
| Abbate et al., 2020 [39] | Randomized controlled trial | 14 days | 99 patients with non-ST segment elevation acute myocardial infarction | Anakinra 100 mg once or twice daily | Placebo | Anakinra compared to placebo resulted in:
|
| Van Tassell et al., 2017 [43] & Mihalick et al., 2022 [42] | Randomized controlled trial | 2–12 weeks | 60 patients with recently decompensated heart failure | Anakinra 100 mg once daily for 2 weeks or for 12 weeks | Placebo | Anakinra compared to placebo resulted in:
|
| Van Tassell et al., 2018 [44] | Randomized controlled trial | 12 weeks | 31 patients with heart failure with preserved left ventricular ejection fraction | Anakinra 100 mg once daily for 12 weeks | Placebo | Anakinra compared to placebo resulted in:
|
| Canakinumab | ||||||
| Ridker et al., 2017 [49] | Randomized controlled trial | 48 months | 10,061 patients with prior myocardial infarction and residual inflammatory risk | Canakinumab 50, 150 or 300 mg, every 3 months | Placebo | Canakinumab compared to placebo resulted in:
|
| Russell et al., 2019 [52] | Randomized controlled trial | 12 months | 38 patients with symptomatic peripheral artery disease | Canakinumab 150 mg once monthly | Placebo | Canakinumab compared to placebo resulted in:
|
| Choudhury et al., 2016 [56] | Randomized controlled trial | 12 months | 189 patients with atherosclerotic disease and either type 2 diabetes or impaired glucose tolerance | Canakinumab 150 mg once monthly | Placebo | Canakinumab compared to placebo resulted in:
|
| Study | Type of Study | Treatment Duration | Study Population | Utilized IL-6 Antagonist | Comparator | Main Findings |
|---|---|---|---|---|---|---|
| Tocilizumab | ||||||
| Giles et al., 2020 [60] | Randomized controlled trial | 3.2 years | 3080 patients with seropositive, active rheumatoid arthritis | Tocilizumab 8 mg/kg/month | Etanercept 50 mg/week | No statistical difference between tocilizumab and etanercept across a number of surrogate cardiovascular endpoints |
| McInnes et al., 2015 [61] | Randomized controlled trial | 24 weeks | 132 patients with seropositive rheumatoid arthritis | Tocilizumab 8 mg/kg/month + methotrexate | Placebo + methotrexate | Tocilizumab compared to placebo resulted in:
|
| Holte et al., 2017 [71] | Randomized controlled trial | Single dose of tocilizumab or placebo prior to coronary angiography | 117 patients with non-ST segment elevation myocardial infarction | Tocilizumab 280 mg at a single dose | Placebo | Tocilizumab compared to placebo resulted in a:
|
| Broch et al., 2021 [72] | Randomized controlled trial | Single dose of tocilizumab or placebo prior to coronary angiography | 199 patients with ST-segment elevation myocardial infarction | Tocilizumab 280 mg at a single dose | Placebo | Tocilizumab compared to placebo resulted in a:
|
| Meyer et al., 2021 [73] | Randomized controlled trial | Single dose of tocilizumab | 80 comatose with out-of-hospital cardiac arrest | Tocilizumab 8 mg/kg at a single dose | Placebo | Tocilizumab compared to placebo resulted in a:
|
| Ziltivekimab | ||||||
| Ridker et al., 2021 [75] | Randomized controlled trial | 24 weeks | 66 patients with moderate to severe chronic kidney disease and residual inflammatory risk | Ziltivekimab 7.5 mg, 15 mg or 30 mg every 4 weeks | Placebo | Ziltivekimab compared to placebo resulted in a:
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dimosiari, A.; Patoulias, D.; Kitas, G.D.; Dimitroulas, T. Do Interleukin-1 and Interleukin-6 Antagonists Hold Any Place in the Treatment of Atherosclerotic Cardiovascular Disease and Related Co-Morbidities? An Overview of Available Clinical Evidence. J. Clin. Med. 2023, 12, 1302. https://doi.org/10.3390/jcm12041302
Dimosiari A, Patoulias D, Kitas GD, Dimitroulas T. Do Interleukin-1 and Interleukin-6 Antagonists Hold Any Place in the Treatment of Atherosclerotic Cardiovascular Disease and Related Co-Morbidities? An Overview of Available Clinical Evidence. Journal of Clinical Medicine. 2023; 12(4):1302. https://doi.org/10.3390/jcm12041302
Chicago/Turabian StyleDimosiari, Athina, Dimitrios Patoulias, George D. Kitas, and Theodoros Dimitroulas. 2023. "Do Interleukin-1 and Interleukin-6 Antagonists Hold Any Place in the Treatment of Atherosclerotic Cardiovascular Disease and Related Co-Morbidities? An Overview of Available Clinical Evidence" Journal of Clinical Medicine 12, no. 4: 1302. https://doi.org/10.3390/jcm12041302