
Sepsis-Associated Delirium: A Narrative Review

 , , , , , ,
, , , , , ,
Abstract
:1. Introduction
2. Epidemiology
2.1. Subsyndromal Delirium
2.2. Clinical Phenotypes of Delirium in the ICU
2.3. SAD
2.4. COVID-19-Associated Delirium
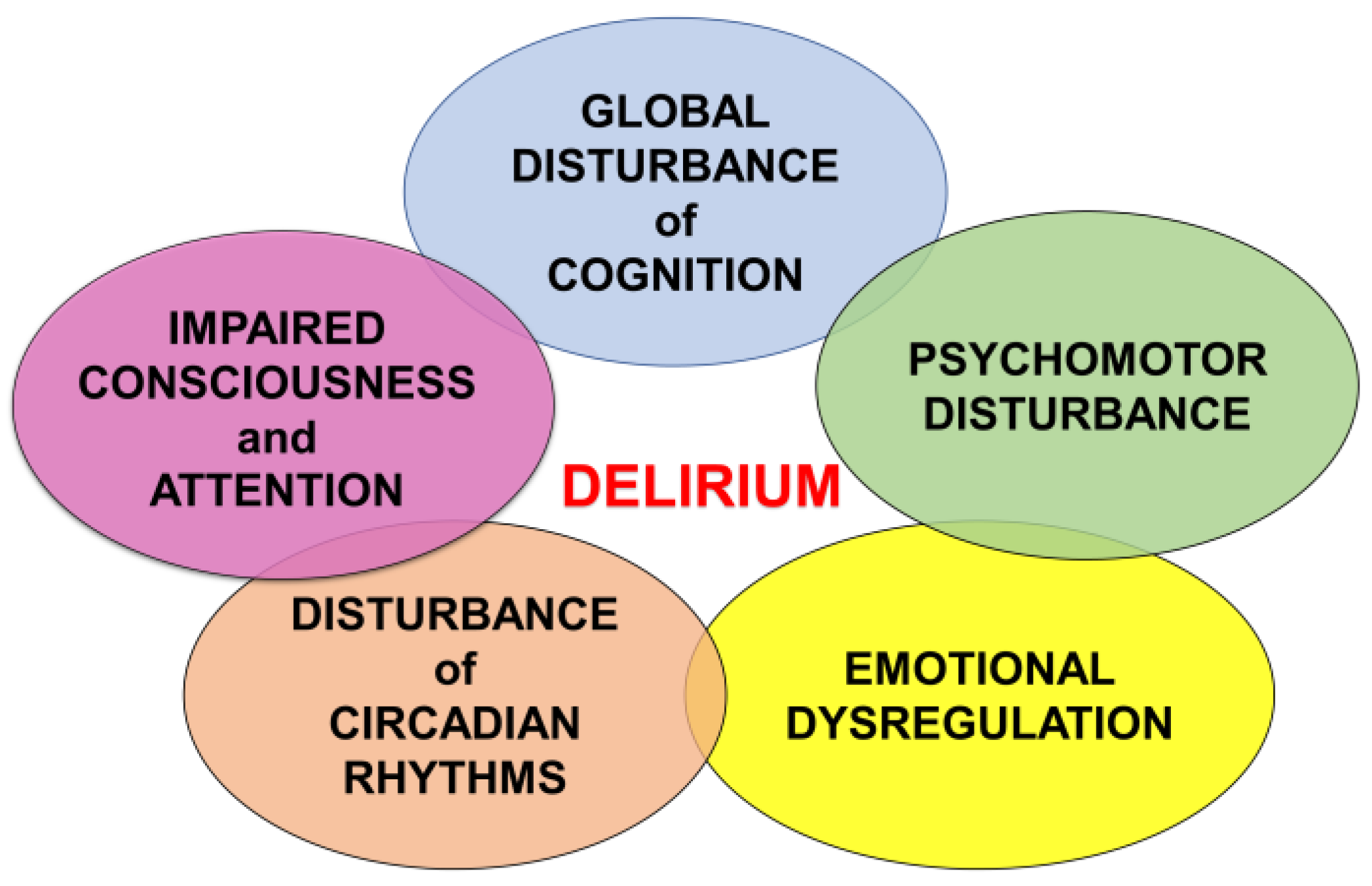
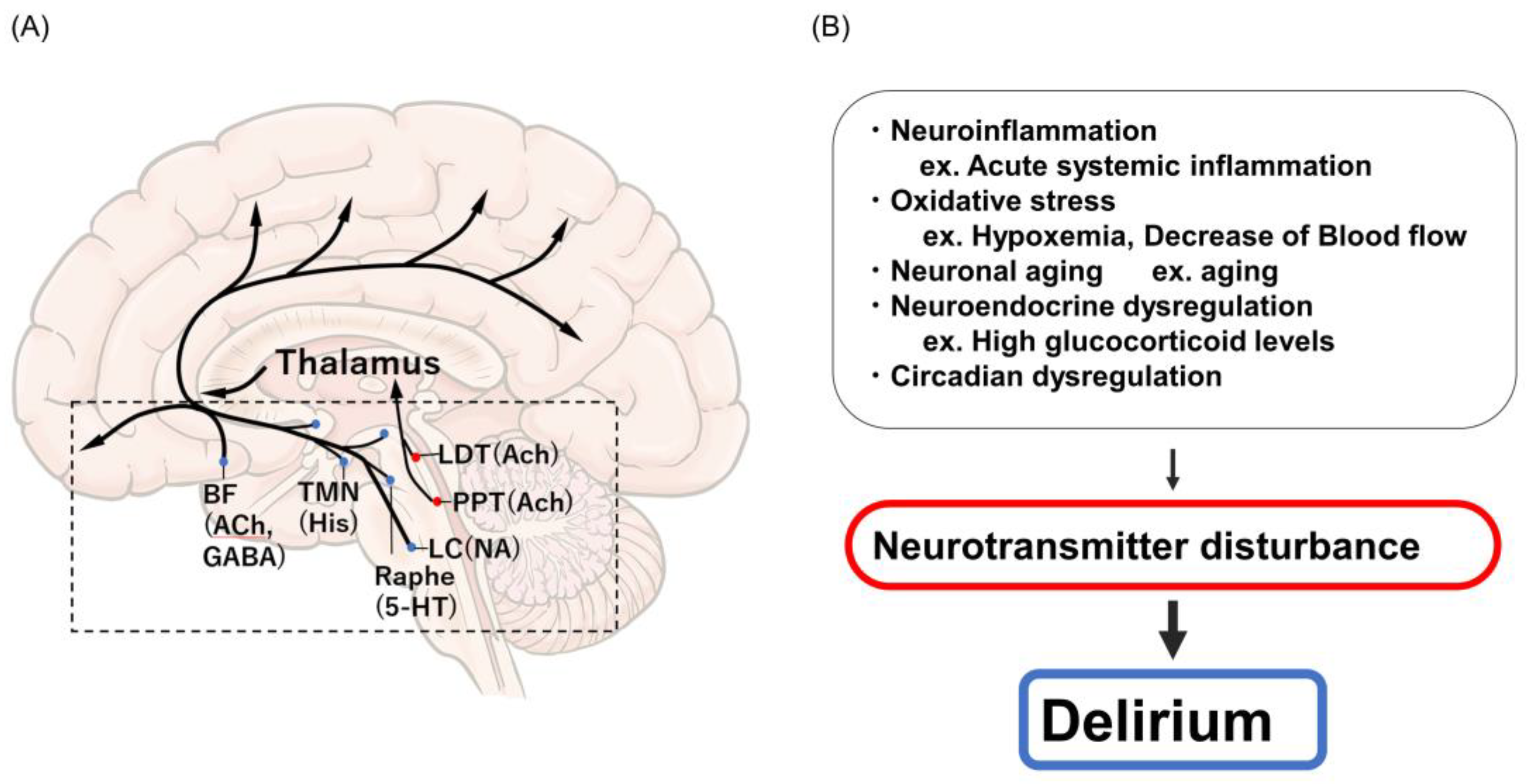
3. Etiology and Pathophysiology of Delirium
4. Etiology and Pathophysiology of SAD
5. Risk Factors and Predictive Indicators of SAD
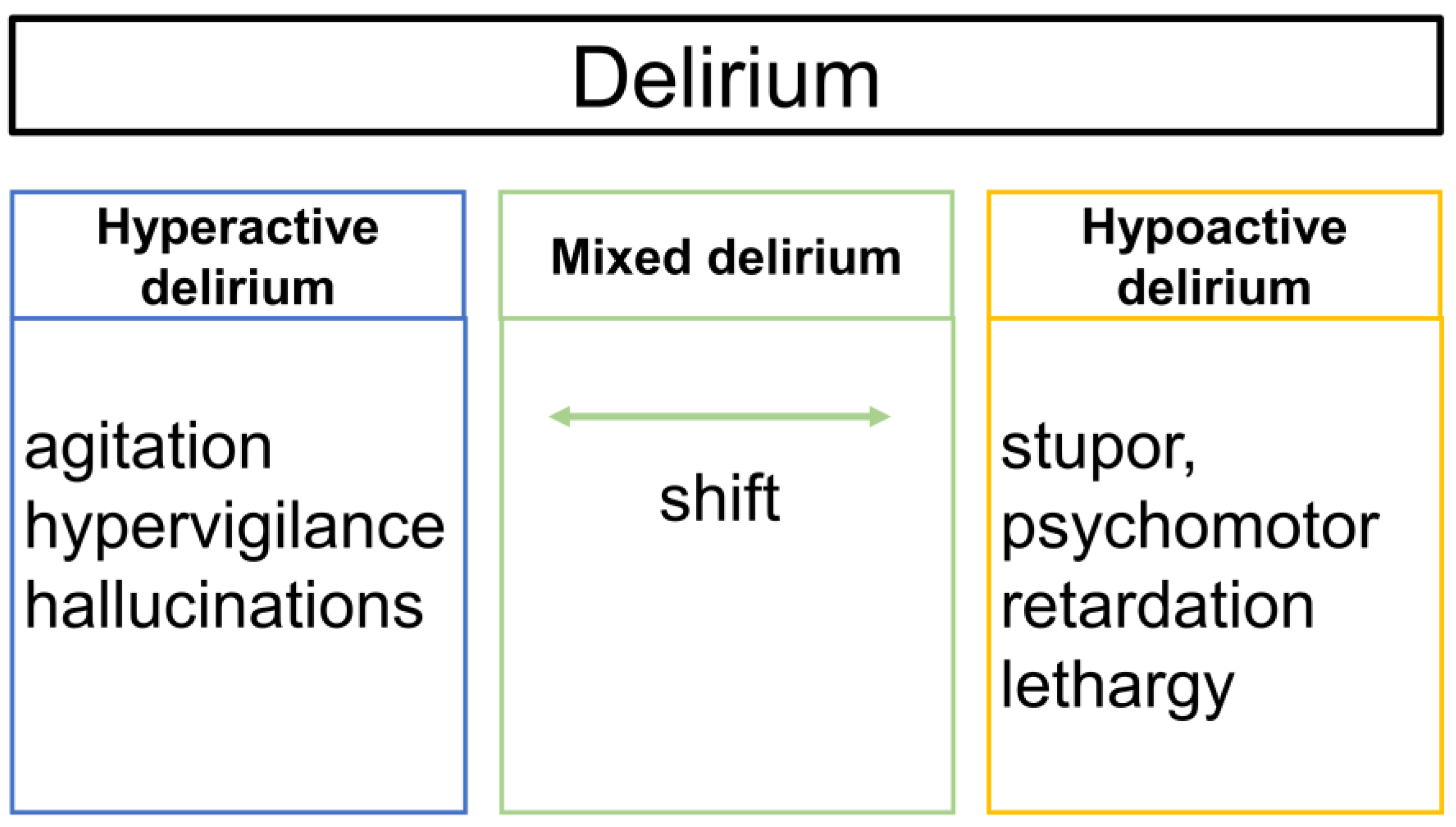
6. Subtypes of Delirium
7. Diagnosis and Severity Evaluation
8. Prevention and Treatment of SAD
8.1. Non-Pharmacological Approach
8.2. Pharmacological Approach
9. Prognosis of SAD
10. Delirium in Patients with COVID-19
11. Future Directions
12. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pisani, M.A.; Araujo, K.L.B.; Murphy, T.E. Association of Cumulative Dose of Haloperidol with Next-Day Delirium in Older Medical ICU Patients. Crit. Care Med. 2015, 43, 996–1002. [Google Scholar] [CrossRef]
- Wilcox, M.E.; Brummel, N.E.; Archer, K.; Ely, E.W.; Jackson, J.C.; Hopkins, R.O. Cognitive dysfunction in ICU patients: Risk factors, predictors, and rehabilitation interventions. Crit. Care Med. 2013, 41, S81–S98. [Google Scholar] [CrossRef] [PubMed]
- Pandharipande, P.P.; Ely, E.W.; Arora, R.C.; Balas, M.C.; Boustani, M.A.; La Calle, G.H.; Cunningham, C.; Devlin, J.W.; Elefante, J.; Han, J.H.; et al. The intensive care delirium research agenda: A multinational, interprofessional perspective. Intensive Care Med. 2017, 43, 1329–1339. [Google Scholar] [CrossRef] [PubMed]
- Atterton, B.; Paulino, M.C.; Povoa, P.; Martin-Loeches, I. Sepsis Associated Delirium. Medicina 2020, 56, 240. [Google Scholar] [CrossRef] [PubMed]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.-D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef] [PubMed]
- Sharshar, T.; Annane, D.; De La Grandmaison, G.L.; Brouland, J.P.; Hopkinson, N.; Gray, F. The Neuropathology of Septic Shock. Brain Pathol. 2004, 14, 21–33. [Google Scholar] [CrossRef]
- Sonneville, R.; De Montmollin, E.; Poujade, J.; Garrouste-Orgeas, M.; Souweine, B.; Darmon, M.; Mariotte, E.; Argaud, L.; Barbier, F.; Goldgran-Toledano, D.; et al. Potentially modifiable factors contributing to sepsis-associated encephalopathy. Intensive Care Med. 2017, 43, 1075–1084. [Google Scholar] [CrossRef]
- Salluh, J.; Wang, H.; Schneider, E.B.; Nagaraja, N.; Yenokyan, G.; Damluji, A.; Serafim, R.B.; Stevens, R.D. Outcome of delirium in critically ill patients: Systematic review and meta-analysis. BMJ 2015, 350, h2538. [Google Scholar] [CrossRef]
- Maclullich, A.M.J.; Anand, A.; Davis, D.; Jackson, T.; Barugh, A.J.; Hall, R.J.; Ferguson, K.J.; Meagher, D.J.; Cunningham, C. New horizons in the pathogenesis, assessment and management of delirium. Age Ageing 2013, 42, 667–674. [Google Scholar] [CrossRef]
- Gibb, K.; Seeley, A.; Quinn, T.; Siddiqi, N.; Shenkin, S.; Rockwood, K.; Davis, D. The consistent burden in published estimates of delirium occurrence in medical inpatients over four decades: A systematic review and meta-analysis study. Age Ageing 2020, 49, 352–360. [Google Scholar] [CrossRef] [Green Version]
- Pendlebury, S.T.; Lovett, N.G.; Smith, S.C.; Dutta, N.; Bendon, C.; Lloyd-Lavery, A.; Mehta, Z.; Rothwell, P. Observational, longitudinal study of delirium in consecutive unselected acute medical admissions: Age-specific rates and associated factors, mortality and re-admission. BMJ Open 2015, 5, e007808. [Google Scholar] [CrossRef] [PubMed]
- Brummel, N.E.; Boehm, L.M.; Girard, T.D.; Pandharipande, P.P.; Jackson, J.C.; Hughes, C.G.; Patel, M.B.; Han, J.H.; Vasilevskis, E.E.; Thompson, J.L.; et al. Subsyndromal Delirium and Institutionalization Among Patients with Critical Illness. Am. J. Crit. Care 2017, 26, 447–455. [Google Scholar] [CrossRef] [PubMed]
- Girard, T.D.; Thompson, J.L.; Pandharipande, P.P.; Brummel, N.; Jackson, J.C.; Patel, M.B.; Hughes, C.G.; Chandrasekhar, R.; Pun, B.T.; Boehm, L.M.; et al. Clinical phenotypes of delirium during critical illness and severity of subsequent long-term cognitive impairment: A prospective cohort study. Lancet Respir. Med. 2018, 6, 213–222. [Google Scholar] [CrossRef] [PubMed]
- Shao, S.-C.; Lai, C.-C.; Chen, Y.-H.; Chen, Y.-C.; Hung, M.-J.; Liao, S.-C. Prevalence, incidence and mortality of delirium in patients with COVID-19: A systematic review and meta-analysis. Age Ageing 2021, 50, 1445–1453. [Google Scholar] [CrossRef]
- Maldonado, J.R. Delirium pathophysiology: An updated hypothesis of the etiology of acute brain failure. Int. J. Geriatr. Psychiatry 2018, 33, 1428–1457. [Google Scholar] [CrossRef]
- Grover, S.; Avasthi, A. Clinical Practice Guidelines for Management of Delirium in Elderly. Indian, J. Psychiatry 2018, 60, S329–S340. [Google Scholar] [CrossRef]
- Hshieh, T.T.; Fong, T.G.; Marcantonio, E.R.; Inouye, S.K. Cholinergic Deficiency Hypothesis in Delirium: A Synthesis of Current Evidence. J. Gerontol. Ser. A 2008, 63, 764–772. [Google Scholar] [CrossRef]
- Kwatra, M.M. Delirium in Older Persons. N. Engl. J. Med. 2006, 354, 1157–1165. [Google Scholar]
- Inouye, S.K.; Ferrucci, L. Elucidating the Pathophysiology of Delirium and the Interrelationship of Delirium and Dementia. J. Gerontol. Ser. A 2006, 61, 1277–1280. [Google Scholar] [CrossRef]
- Wilson, J.E.; Mart, M.F.; Cunningham, C.; Shehabi, Y.; Girard, T.D.; MacLullich, A.M.; Slooter, A.J.C.; Ely, E.W. Delirium. Nat. Rev. Dis. Primers 2020, 6, 90. [Google Scholar] [CrossRef]
- Pinho, C.; Cruz, S.; Santos, A.; Abelha, F.J. Postoperative delirium: Age and low functional reserve as independent risk factors. J. Clin. Anesthesia 2016, 33, 507–513. [Google Scholar] [CrossRef] [PubMed]
- De Rooij, S.E.; van Munster, B.C.; Korevaar, J.C.; Levi, M. Cytokines and acute phase response in delirium. J. Psychosom. Res. 2007, 62, 521–525. [Google Scholar] [CrossRef] [PubMed]
- Beloosesky, Y.; Hendel, D.; Weiss, A.; Hershkovitz, A.; Grinblat, J.; Pirotsky, A.; Barak, V. Cytokines and C-Reactive Protein Production in Hip-Fracture-Operated Elderly Patients. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2007, 62, 420–426. [Google Scholar] [CrossRef] [PubMed]
- Berr, C.; Balansard, B.; Arnaud, J.; Roussel, A.-M.; Alpérovitch, A.; EVA Study Group. Cognitive Decline Is Associated with Systemic Oxidative Stress: The EVA Study. J. Am. Geriatr. Soc. 2000, 48, 1285–1291. [Google Scholar] [CrossRef]
- MacLullich, A.M.; Ferguson, K.J.; Miller, T.; de Rooij, S.E.; Cunningham, C. Unravelling the pathophysiology of delirium: A focus on the role of aberrant stress responses. J. Psychosom. Res. 2008, 65, 229–238. [Google Scholar] [CrossRef]
- Maldonado, J.R. Neuropathogenesis of delirium: Review of current etiologic theories and common pathways. Am. J. Geriatr. Psychiatry 2013, 21, 1190–1222. [Google Scholar] [CrossRef]
- Brown, R.; Basheer, R.; McKenna, J.; Strecker, R.E.; McCarley, R. Control of Sleep and Wakefulness. Physiol. Rev. 2012, 92, 1087–1187. [Google Scholar] [CrossRef]
- Chung, H.Y.; Wickel, J.; Brunkhorst, F.M.; Geis, C. Sepsis-Associated Encephalopathy: From Delirium to Dementia? J. Clin. Med. 2020, 9, 703. [Google Scholar] [CrossRef]
- Sharshar, T.; Polito, A.; Checinski, A.; Stevens, R.D. Septic-associated encephalopathy-everything starts at a microlevel. Crit. Care 2010, 14, 199. [Google Scholar] [CrossRef]
- Ebersoldt, M.; Sharshar, T.; Annane, D. Sepsis-associated delirium. Intensive Care Med. 2007, 33, 941–950. [Google Scholar] [CrossRef]
- Eidelman, L.A.; Putterman, D.; Putterman, C.; Sprung, C.L. The spectrum of septic encephalopathy. Definitions, etiologies, and mortalities. JAMA 1996, 275, 470–473. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.-N.; Wang, X.-T.; Ai, Y.-H.; Guo, Q.-L.; Huang, L.; Liu, Z.-Y.; Yao, B. Epidemiological features and risk factors of sepsis-associated encephalopathy in intensive care unit patients: 2008–2011. Chin. Med. J. 2012, 125, 828–831. [Google Scholar] [PubMed]
- Kim, Y.; Jin, Y.; Jin, T.; Lee, S.M. Risk factors and outcomes of sepsis-associated delirium in intensive care unit patients: A secondary data analysis. Intensive Crit. Care Nurs. 2020, 59, 102844. [Google Scholar] [CrossRef]
- Spronk, P.E.; Riekerk, B.; Hofhuis, J.; Rommes, J.H. Occurrence of delirium is severely underestimated in the ICU during daily care. Intensive Care Med. 2009, 35, 1276–1280. [Google Scholar] [CrossRef] [PubMed]
- la Cour, K.N.; Andersen-Ranberg, N.C.; Weihe, S.; Poulsen, L.M.; Mortensen, C.B.; Kjer, C.K.W.; Collet, M.O.; Estrup, S.; Mathiesen, O. Distribution of delirium motor subtypes in the intensive care unit: A systematic scoping review. Crit. Care 2022, 26, 53. [Google Scholar] [CrossRef] [PubMed]
- Devlin, J.W.; Fong, J.J.; Schumaker, G.; O’Connor, H.; Ruthazer, R.; Garpestad, E. Use of a validated delirium assessment tool improves the ability of physicians to identify delirium in medical intensive care unit patients. Crit. Care Med. 2007, 35, 2721–2724. [Google Scholar] [CrossRef]
- Devlin, J.W.; Skrobik, Y.; Gélinas, C.; Needham, D.M.; Slooter, A.J.C.; Pandharipande, P.; Watson, P.L.; Weinhouse, G.L.; Nunnally, M.E.; Rochwerg, B.; et al. Clinical Practice Guidelines for the Prevention and Management of Pain, Agitation/Sedation, Delirium, Immobility, and Sleep Disruption in Adult Patients in the ICU. Crit. Care Med. 2018, 46, e825–e873. [Google Scholar] [CrossRef]
- Chen, T.-J.; Chung, Y.-W.; Chang, H.-C.; Chen, P.-Y.; Wu, C.-R.; Hsieh, S.-H.; Chiu, H.-Y. Diagnostic accuracy of the CAM-ICU and ICDSC in detecting intensive care unit delirium: A bivariate meta-analysis. Int. J. Nurs. Stud. 2021, 113, 103782. [Google Scholar] [CrossRef]
- Khan, B.A.; Perkins, A.J.; Gao, S.; Hui, S.L.; Campbell, N.L.; Farber, M.O.; Chlan, L.L.; Boustani, M.A. The Confusion Assessment Method for the ICU-7 Delirium Severity Scale: A Novel Delirium Severity Instrument for Use in the ICU. Crit. Care Med. 2017, 45, 851–857. [Google Scholar] [CrossRef]
- Wiegand, T.L.T.; Rémi, J.; Dimitriadis, K. Electroencephalography in delirium assessment: A scoping review. BMC Neurol. 2022, 22, 86. [Google Scholar] [CrossRef]
- Non-Invasive Eye Tracking for the Diagnosis of Delirium on ICU (CONfuSED); National Library of Medicine: Bethesda, MD, USA, 2020.
- Zaal, I.J.; Devlin, J.W.; Peelen, L.M.; Slooter, A.J.C. A Systematic Review of Risk Factors for Delirium in the ICU. Crit. Care Med. 2015, 43, 40–47. [Google Scholar] [CrossRef]
- Schaller, S.J.; Anstey, M.; Blobner, M.; Edrich, T.; Grabitz, S.D.; Gradwohl-Matis, I.; Heim, M.; Houle, T.; Kurth, T.; Latronico, N.; et al. Early, goal-directed mobilisation in the surgical intensive care unit: A randomised controlled trial. Lancet 2016, 388, 1377–1388. [Google Scholar] [CrossRef] [PubMed]
- Schweickert, W.D.; Pohlman, M.C.; Pohlman, A.S.; Nigos, C.; Pawlik, A.J.; Esbrook, C.L.; Spears, L.; Miller, M.; Franczyk, M.; Deprizio, D.; et al. Early physical and occupational therapy in mechanically ventilated, critically ill patients: A randomised controlled trial. Lancet 2009, 373, 1874–1882. [Google Scholar] [CrossRef]
- Pun, B.T.; Balas, M.C.; Barnes-Daly, M.A.; Thompson, J.L.; Aldrich, J.M.; Barr, J.; Byrum, D.; Carson, S.S.; Devlin, J.W.; Engel, H.J.; et al. Caring for Critically Ill Patients with the ABCDEF Bundle: Results of the ICU Liberation Collaborative in Over 15,000 Adults. Crit. Care Med. 2019, 47, 3–14. [Google Scholar] [CrossRef]
- Faustino, T.N.; Suzart, N.A.; dos Santos Rabelo, R.N.; Santos, J.L.; Batista, G.S.; de Freitas, Y.S.; Saback, D.A.; Sales, N.M.M.D.; Barreto, B.B.; Gusmao-Flores, D. Effectiveness of combined non-pharmacological interventions in the prevention of delirium in critically ill patients: A randomized clinical trial. J. Crit. Care 2022, 68, 114–120. [Google Scholar] [CrossRef]
- Burry, L.D.; Cheng, W.; Williamson, D.R.; Adhikari, N.K.; Egerod, I.; Kanji, S.; Martin, C.M.; Hutton, B.; Rose, L. Pharmacological and non-pharmacological interventions to prevent delirium in critically ill patients: A systematic review and network meta-analysis. Intensive Care Med. 2021, 47, 943–960. [Google Scholar] [CrossRef] [PubMed]
- Kawazoe, Y.; Miyamoto, K.; Morimoto, T.; Yamamoto, T.; Fuke, A.; Hashimoto, A.; Koami, H.; Beppu, S.; Katayama, Y.; Itoh, M.; et al. Effect of Dexmedetomidine on Mortality and Ventilator-Free Days in Patients Requiring Mechanical Ventilation with Sepsis: A Randomized Clinical Trial. JAMA 2017, 317, 1321–1328. [Google Scholar] [CrossRef]
- Hughes, C.G.; Mailloux, P.T.; Devlin, J.W.; Swan, J.T.; Sanders, R.D.; Anzueto, A.; Jackson, J.C.; Hoskins, A.S.; Pun, B.T.; Orun, O.M.; et al. Dexmedetomidine or Propofol for Sedation in Mechanically Ventilated Adults with Sepsis. N. Engl. J. Med. 2021, 384, 1424–1436. [Google Scholar] [CrossRef] [PubMed]
- Khaing, K.; Nair, B.R. Melatonin for delirium prevention in hospitalized patients: A systematic review and meta-analysis. J. Psychiatr. Res. 2021, 133, 181–190. [Google Scholar] [CrossRef]
- Needham, D.M.; Colantuoni, E.; Dinglas, V.D.; Hough, C.L.; Wozniak, A.W.; Jackson, J.C.; Morris, P.P.E.; Mendez-Tellez, P.A.; Ely, P.E.W.; Hopkins, P.R.O. Rosuvastatin versus placebo for delirium in intensive care and subsequent cognitive impairment in patients with sepsis-associated acute respiratory distress syndrome: An ancillary study to a randomised controlled trial. Lancet Respir. Med. 2016, 4, 203–212. [Google Scholar] [CrossRef] [PubMed]
- Reade, M.C.; Eastwood, G.M.; Bellomo, R.; Bailey, M.; Bersten, A.; Cheung, B.; Davies, A.; Delaney, A.; Ghosh, A.; van Haren, F.; et al. Effect of Dexmedetomidine Added to Standard Care on Ventilator-Free Time in Patients with Agitated Delirium: A Randomized Clinical Trial. JAMA 2016, 315, 1460–1468. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Inoue, S.; Hatakeyama, J.; Kondo, Y.; Hifumi, T.; Sakuramoto, H.; Kawasaki, T.; Taito, S.; Nakamura, K.; Unoki, T.; Kawai, Y.; et al. Post-intensive care syndrome: Its pathophysiology, prevention, and future directions. Acute Med. Surg. 2019, 6, 233–246. [Google Scholar] [CrossRef]
- Pandharipande, P.P.; Girard, T.D.; Jackson, J.C.; Morandi, A.; Thompson, J.L.; Pun, B.T. Long-Term Cognitive Impairment after Critical Illness. N. Engl. J. Med. 2013, 369, 1306–1316. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.M.; Fan, E. ICU-acquired weakness: What is preventing its rehabilitation in critically ill patients? BMC Med. 2012, 10, 115. [Google Scholar] [CrossRef]
- Altman, M.T.; Knauert, M.P.; Murphy, T.E.; Ahasic, A.M.; Chauhan, Z.; Pisani, M.A. Association of intensive care unit delirium with sleep disturbance and functional disability after critical illness: An observational cohort study. Ann. Intensive Care 2018, 8, 63. [Google Scholar] [CrossRef]
- Jackson, J.C.; Pandharipande, P.P.; Girard, T.D.; Brummel, N.E.; Thompson, J.L.; Hughes, C.G.; Pun, B.T.; Vasilevskis, E.; Morandi, A.; Shintani, A.K.; et al. Depression, post-traumatic stress disorder, and functional disability in survivors of critical illness in the BRAIN-ICU study: A longitudinal cohort study. Lancet Respir. Med. 2014, 2, 369–379. [Google Scholar] [CrossRef] [PubMed]
- Bieber, E.D.; Philbrick, K.L.; Shapiro, J.B.; Karnatovskaia, L.V. Psychiatry’s role in the prevention of post-intensive care mental health impairment: Stakeholder survey. BMC Psychiatry 2022, 22, 198. [Google Scholar] [CrossRef]
- Kotfis, K.; Williams Roberson, S.; Wilson, J.E.; Dabrowski, W.; Pun, B.T.; Ely, E.W. COVID-19: ICU delirium management during SARS-CoV-2 pandemic. Crit. Care 2020, 24, 176. [Google Scholar] [CrossRef]
- Pun, B.T.; Badenes, R.; La Calle, G.H.; Orun, O.M.; Chen, W.; Raman, R.; Simpson, B.-G.K.; Wilson-Linville, S.; Olmedillo, B.H.; de la Cueva, A.V.; et al. Prevalence and risk factors for delirium in critically ill patients with COVID-19 (COVID-D): A multicentre cohort study. Lancet Respir. Med. 2021, 9, 239–250. [Google Scholar] [CrossRef]
- Ostuzzi, G.; Gastaldon, C.; Papola, D.; Fagiolini, A.; Dursun, S.; Taylor, D.; Corre, C.U.; Barbui, C. Pharmacological treatment of hyperactive delirium in people with COVID-19: Rethinking conventional approaches. Adv. Psychopharmacol. 2020, 10, 2045125320942703. [Google Scholar] [CrossRef] [PubMed]
- Hawkins, M.; Sockalingam, S.; Bonato, S.; Rajaratnam, T.; Ravindran, M.; Gosse, P.; Sheehan, K.A. A rapid review of the pathoetiology, presentation, and management of delirium in adults with COVID-19. J. Psychosom. Res. 2020, 141, 110350. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, M.; Helfand, B.K.I.; Gou, R.Y.; Gartaganis, S.L.; Webb, M.; Moccia, J.M.; Bruursema, S.N.; Dokic, B.; McCulloch, B.; Ring, H.; et al. Delirium in Older Patients With COVID-19 Presenting to the Emergency Department. JAMA Netw. Open 2020, 3, e2029540. [Google Scholar] [CrossRef] [PubMed]
- Garcez, F.B.; Aliberti, M.J.R.; Poco, P.C.E.; Hiratsuka, M.; Takahashi, S.F.; Coelho, V.A. Delirium and Adverse Outcomes in Hospitalized Patients with COVID-19. J. Am. Geriatr. Soc. 2020, 68, 2440–2446. [Google Scholar] [CrossRef] [PubMed]
- Kandori, K.; Okada, Y.; Ishii, W.; Narumiya, H.; Maebayashi, Y.; Iizuka, R. Association between visitation restriction during the COVID-19 pandemic and delirium incidence among emergency admission patients: A single-center retrospective observational cohort study in Japan. J. Intensive Care 2020, 8, 90. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Risk Factors for SAD or SAE | |
|---|---|
| Background | Age ≥ 65 years |
| Cognitive dysfunction | |
| Long-term use of psychoactive drugs | |
| History of chronic alcohol abuse | |
| Original disease | Staphylococcus aureus bacteremia |
| Neurological disease | |
| Laboratory tests | Decreased Alb |
| Renal failure | |
| Hypo-/hyperglycemia | |
| Hypernatremia | |
| Hypercapnia | |
| Physical examination | Tachypnea |
| Low level of consciousness | |
| Dependent activity and high nursing needs | |
| Use of vasopressors/inotropes |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tokuda, R.; Nakamura, K.; Takatani, Y.; Tanaka, C.; Kondo, Y.; Ohbe, H.; Kamijo, H.; Otake, K.; Nakamura, A.; Ishikura, H.; et al. Sepsis-Associated Delirium: A Narrative Review. J. Clin. Med. 2023, 12, 1273. https://doi.org/10.3390/jcm12041273
Tokuda R, Nakamura K, Takatani Y, Tanaka C, Kondo Y, Ohbe H, Kamijo H, Otake K, Nakamura A, Ishikura H, et al. Sepsis-Associated Delirium: A Narrative Review. Journal of Clinical Medicine. 2023; 12(4):1273. https://doi.org/10.3390/jcm12041273
Chicago/Turabian StyleTokuda, Rina, Kensuke Nakamura, Yudai Takatani, Chie Tanaka, Yutaka Kondo, Hiroyuki Ohbe, Hiroshi Kamijo, Kosuke Otake, Atsuo Nakamura, Hiroyasu Ishikura, and et al. 2023. "Sepsis-Associated Delirium: A Narrative Review" Journal of Clinical Medicine 12, no. 4: 1273. https://doi.org/10.3390/jcm12041273