
Predicting Heart Failure in Patients with Atrial Fibrillation: A Report from the Prospective COOL-AF Registry
 ,
, 
Abstract
:1. Introduction
2. Methods
2.1. Study Protocol
2.2. Data Collection
2.3. Study Outcomes
2.4. Statistical Analysis
2.5. Model Development
2.6. Model Validation
3. Results
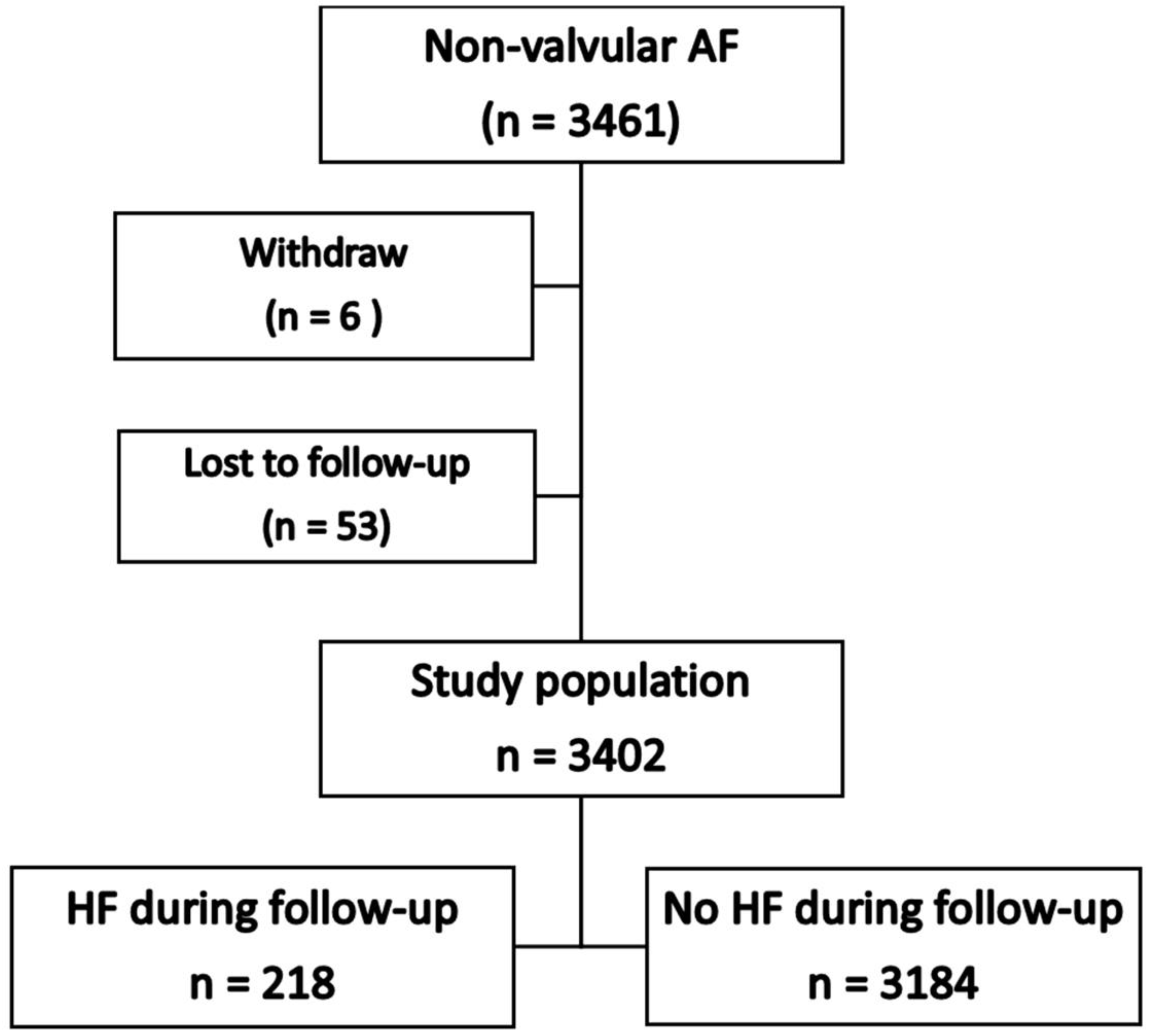
3.1. Type of Heart Failure at Baseline and During Follow-Up
3.2. Univariable and Multivariable Analysis
3.3. Model Development
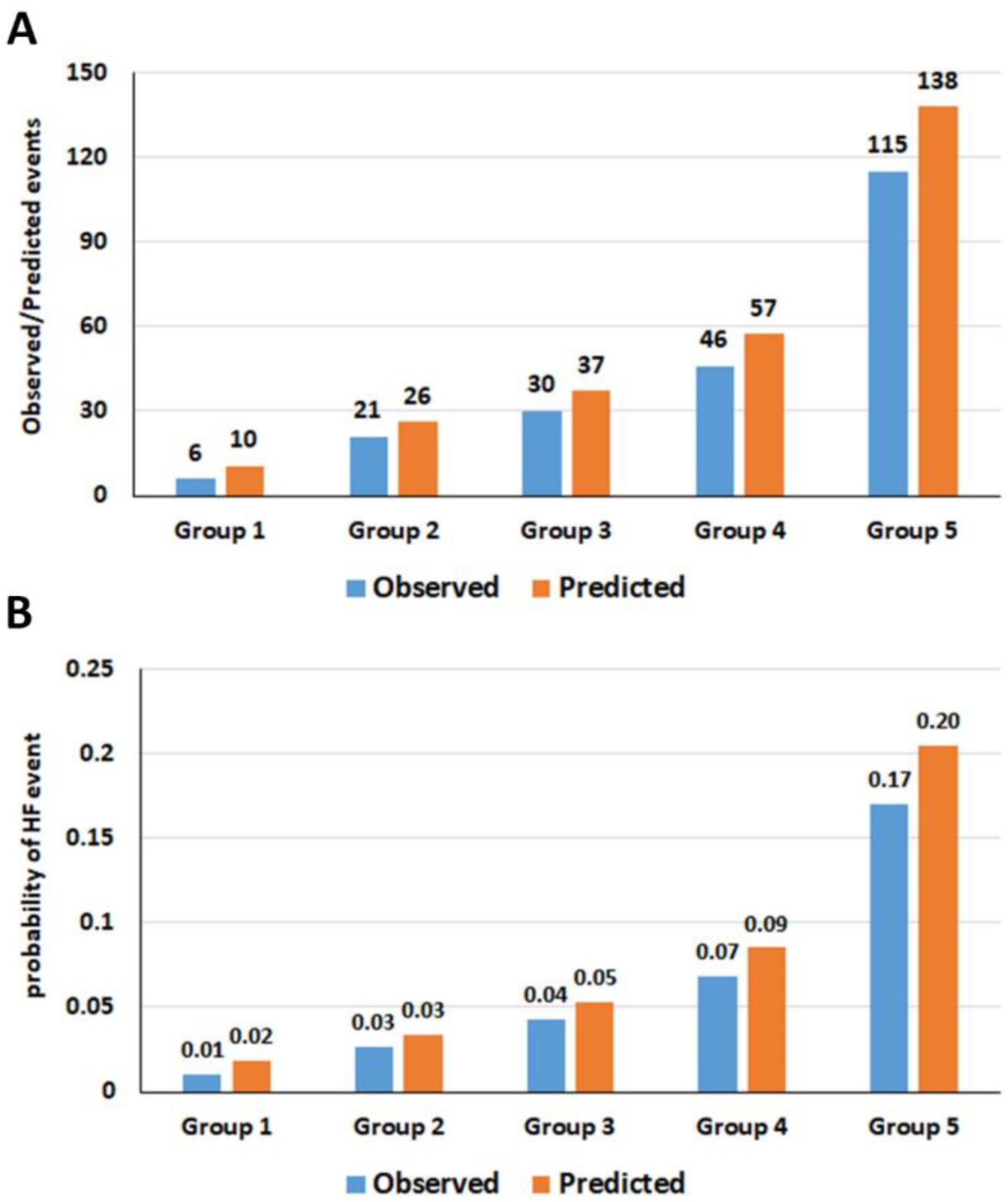
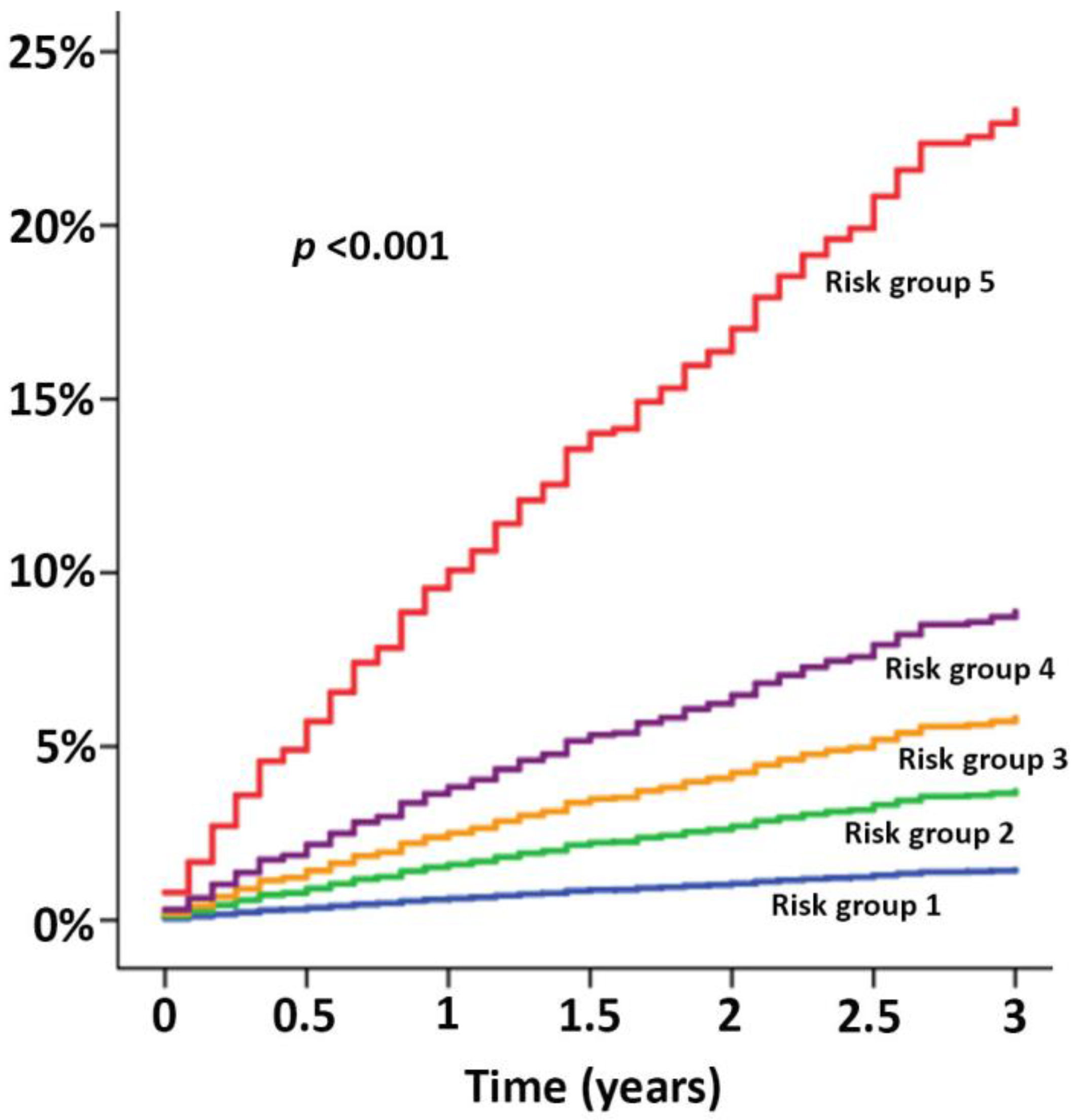
3.4. Model Validation
3.5. Simplified HF Prediction Score
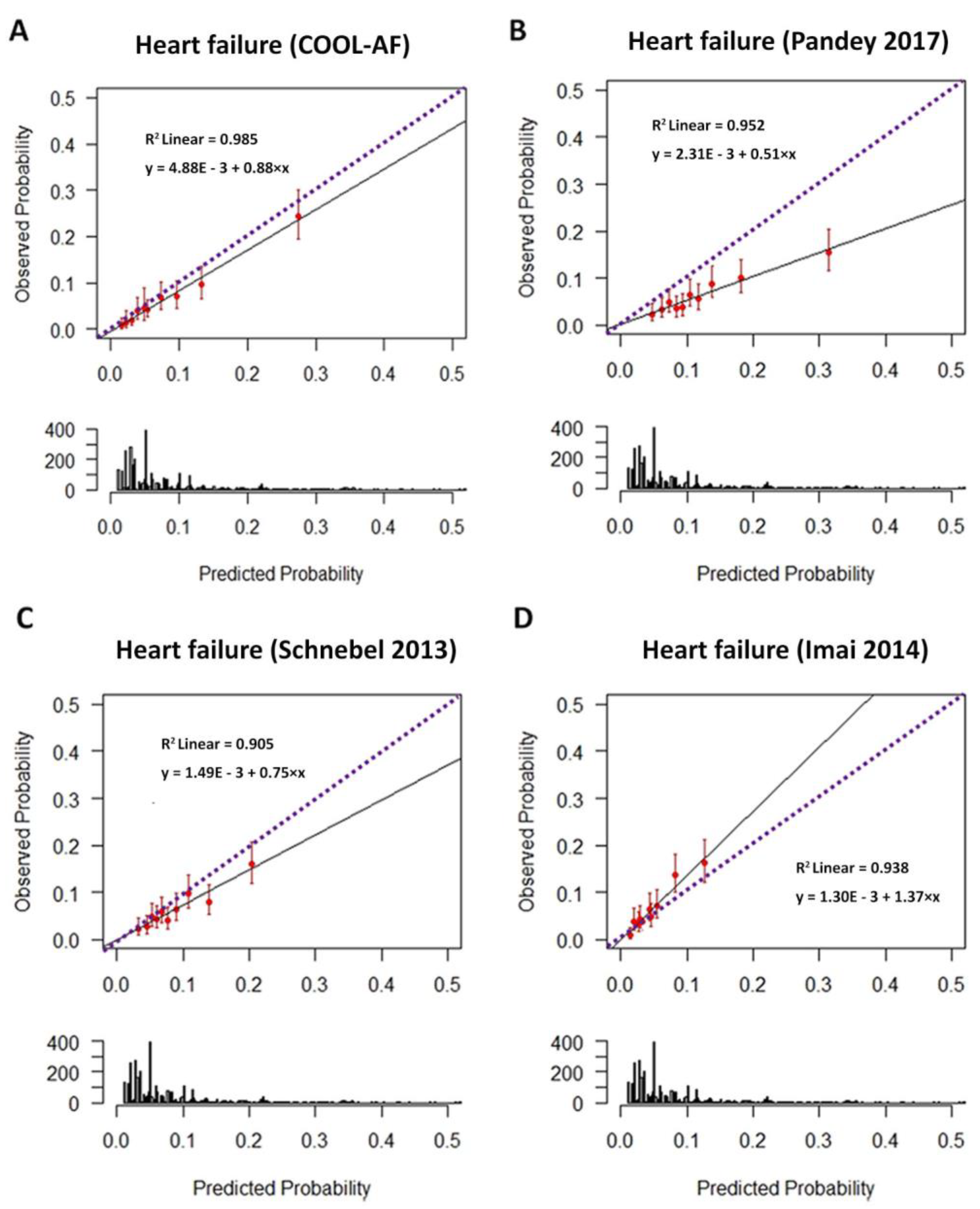
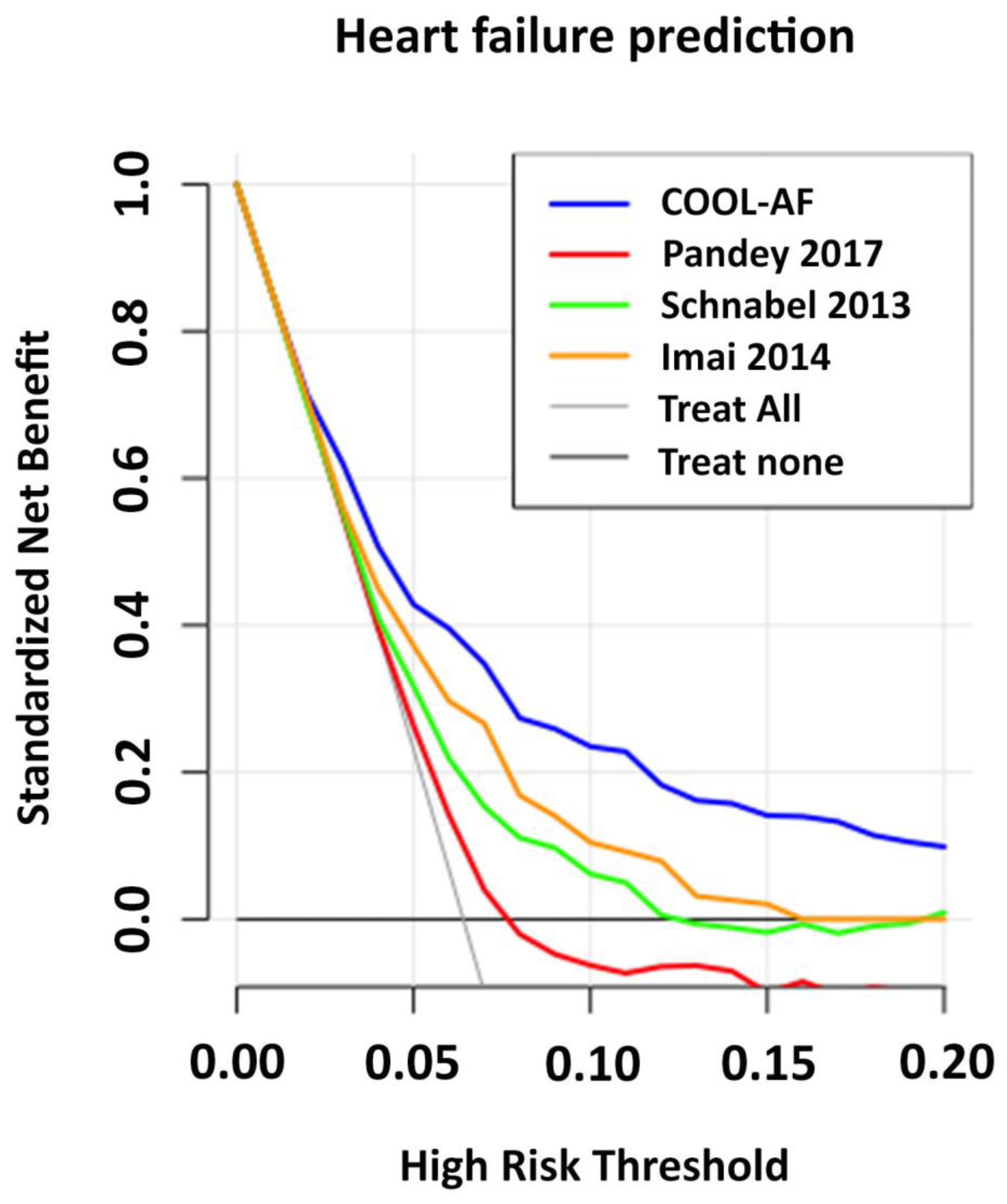
3.6. Comparisons of COOL-AF Predictive Model with Previous Studies
3.7. Additional Analysis to Identify Preventive Strategies to Reduce HF Risk
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Lee, J.Z.; Cha, Y.M. Atrial fibrillation and heart failure: A contemporary review of current management approaches. Heart Rhythm. O2 2021, 2, 762–770. [Google Scholar] [CrossRef] [PubMed]
- Carlisle, M.A.; Fudim, M.; DeVore, A.D.; Piccini, J.P. Heart Failure and Atrial Fibrillation, Like Fire and Fury. JACC Heart Fail. 2019, 7, 447–456. [Google Scholar] [CrossRef] [PubMed]
- Al-Khatib, S.M.; Benjamin, E.J.; Albert, C.M.; Alonso, A.; Chauhan, C.; Chen, P.S.; Curtis, A.B.; Desvigne-Nickens, P.; Ho, J.E.; Lam, C.S.P.; et al. Advancing Research on the Complex Interrelations Between Atrial Fibrillation and Heart Failure: A Report From a US National Heart, Lung, and Blood Institute Virtual Workshop. Circulation 2020, 141, 1915–1926. [Google Scholar] [CrossRef] [PubMed]
- Bassand, J.P.; Accetta, G.; Camm, A.J.; Cools, F.; Fitzmaurice, D.A.; Fox, K.A.; Goldhaber, S.Z.; Goto, S.; Haas, S.; Hacke, W.; et al. Two-year outcomes of patients with newly diagnosed atrial fibrillation: Results from GARFIELD-AF. Eur. Heart J. 2016, 37, 2882–2889. [Google Scholar] [CrossRef] [PubMed]
- Ogawa, H.; Hamatani, Y.; Doi, K.; Tezuka, Y.; An, Y.; Ishii, M.; Iguchi, M.; Masunaga, N.; Esato, M.; Chun, Y.H.; et al. Sex-Related Differences in the Clinical Events of Patients With Atrial Fibrillation- The Fushimi AF Registry. Circ. J. 2017, 81, 1403–1410. [Google Scholar] [CrossRef]
- Krittayaphong, R.; Boonyapiphat, T.; Wongvipaporn, C.; Sairat, P.; Investigators, C.-A. Age-Related Clinical Outcomes of Patients with Non-Valvular Atrial Fibrillation: Insights from the COOL-AF Registry. Clin. Interv. Aging 2021, 16, 707–719. [Google Scholar] [CrossRef]
- Piccini, J.P.; Simon, D.N.; Steinberg, B.A.; Thomas, L.; Allen, L.A.; Fonarow, G.C.; Gersh, B.; Hylek, E.; Kowey, P.R.; Reiffel, J.A.; et al. Differences in Clinical and Functional Outcomes of Atrial Fibrillation in Women and Men: Two-Year Results From the ORBIT-AF Registry. JAMA Cardiol. 2016, 1, 282–291. [Google Scholar] [CrossRef] [PubMed]
- Tsigkas, G.; Apostolos, A.; Despotopoulos, S.; Vasilagkos, G.; Kallergis, E.; Leventopoulos, G.; Mplani, V.; Davlouros, P. Heart failure and atrial fibrillation: New concepts in pathophysiology, management, and future directions. Heart Fail Rev. 2022, 27, 1201–1210. [Google Scholar] [CrossRef]
- Nielsen, P.B.; Larsen, T.B.; Gorst-Rasmussen, A.; Skjoth, F.; Lip, G.Y. Beta-Blockers in Atrial Fibrillation Patients With or Without Heart Failure: Association With Mortality in a Nationwide Cohort Study. Circ. Heart Fail. 2016, 9, e002597. [Google Scholar] [CrossRef]
- Sohns, C.; Zintl, K.; Zhao, Y.; Dagher, L.; Andresen, D.; Siebels, J.; Wegscheider, K.; Sehner, S.; Boersma, L.; Merkely, B.; et al. Impact of Left Ventricular Function and Heart Failure Symptoms on Outcomes Post Ablation of Atrial Fibrillation in Heart Failure: CASTLE-AF Trial. Circ. Arrhythmia Electrophysiol. 2020, 13, e008461. [Google Scholar] [CrossRef] [PubMed]
- Potpara, T.S.; Lip, G.Y.H.; Blomstrom-Lundqvist, C.; Boriani, G.; Van Gelder, I.C.; Heidbuchel, H.; Hindricks, G.; Camm, A.J. The 4S-AF Scheme (Stroke Risk; Symptoms; Severity of Burden; Substrate): A Novel Approach to In-Depth Characterization (Rather than Classification) of Atrial Fibrillation. Thromb. Haemost. 2021, 121, 270–278. [Google Scholar] [CrossRef]
- Lip, G.Y.H. The ABC pathway: An integrated approach to improve AF management. Nat. Rev. Cardiol. 2017, 14, 627–628. [Google Scholar] [CrossRef] [PubMed]
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomstrom-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.A.; Dilaveris, P.E.; et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association of Cardio-Thoracic Surgery (EACTS). Eur. Heart J. 2020, 42, 373–498. [Google Scholar] [CrossRef]
- Chao, T.F.; Joung, B.; Takahashi, Y.; Lim, T.W.; Choi, E.K.; Chan, Y.H.; Guo, Y.; Sriratanasathavorn, C.; Oh, S.; Okumura, K.; et al. 2021 Focused Update Consensus Guidelines of the Asia Pacific Heart Rhythm Society on Stroke Prevention in Atrial Fibrillation: Executive Summary. Thromb. Haemost. 2022, 122, 20–47. [Google Scholar] [CrossRef] [PubMed]
- Pandey, A.; Kim, S.; Moore, C.; Thomas, L.; Gersh, B.; Allen, L.A.; Kowey, P.R.; Mahaffey, K.W.; Hylek, E.; Peterson, E.D.; et al. Predictors and Prognostic Implications of Incident Heart Failure in Patients With Prevalent Atrial Fibrillation. JACC Heart Fail. 2017, 5, 44–52. [Google Scholar] [CrossRef]
- Schnabel, R.B.; Rienstra, M.; Sullivan, L.M.; Sun, J.X.; Moser, C.B.; Levy, D.; Pencina, M.J.; Fontes, J.D.; Magnani, J.W.; McManus, D.D.; et al. Risk assessment for incident heart failure in individuals with atrial fibrillation. Eur. J. Heart Fail. 2013, 15, 843–849. [Google Scholar] [CrossRef] [PubMed]
- Imai, K.; Okura, H.; Tamada, T.; Fukuhara, K.; Koyama, T.; Kume, T.; Hayashida, A.; Kawamoto, T.; Neishi, Y.; Yoshida, K. Prediction of congestive heart failure in patients with non valvular atrial fibrillation. Intern. Med. 2014, 53, 7–12. [Google Scholar] [CrossRef] [PubMed]
- Hicks, K.A.; Tcheng, J.E.; Bozkurt, B.; Chaitman, B.R.; Cutlip, D.E.; Farb, A.; Fonarow, G.C.; Jacobs, J.P.; Jaff, M.R.; Lichtman, J.H.; et al. 2014 ACC/AHA Key Data Elements and Definitions for Cardiovascular Endpoint Events in Clinical Trials: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Data Standards (Writing Committee to Develop Cardiovascular Endpoints Data Standards). J. Am. Coll. Cardiol. 2015, 66, 403–469. [Google Scholar] [CrossRef] [PubMed]
- Wolff, R.F.; Moons, K.G.M.; Riley, R.D.; Whiting, P.F.; Westwood, M.; Collins, G.S.; Reitsma, J.B.; Kleijnen, J.; Mallett, S.; Groupdagger, P. PROBAST: A Tool to Assess the Risk of Bias and Applicability of Prediction Model Studies. Ann. Intern. Med. 2019, 170, 51–58. [Google Scholar] [CrossRef]
- Van Calster, B.; McLernon, D.J.; van Smeden, M.; Wynants, L.; Steyerberg, E.W. Calibration: The Achilles heel of predictive analytics. BMC Med. 2019, 17, 230. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Riley, R.D.; Ensor, J.; Snell, K.I.; Debray, T.P.; Altman, D.G.; Moons, K.G.; Collins, G.S. External validation of clinical prediction models using big datasets from e-health records or IPD meta-analysis: Opportunities and challenges. BMJ 2016, 353, i3140. [Google Scholar] [CrossRef] [PubMed]
- Brier, G.W. Verification of forecasts expressed in terms of probability. Mon. Weather. Rev. 1950, 78, 1–3. [Google Scholar] [CrossRef]
- Tzoulaki, I.; Liberopoulos, G.; Ioannidis, J.P. Use of reclassification for assessment of improved prediction: An empirical evaluation. Int. J. Epidemiol. 2011, 40, 1094–1105. [Google Scholar] [CrossRef] [PubMed]
- Vickers, A.J.; Van Calster, B.; Steyerberg, E.W. A simple, step-by-step guide to interpreting decision curve analysis. Diagn. Progn. Res. 2019, 3, 18. [Google Scholar] [CrossRef]
- Krisai, P.; Johnson, L.S.B.; Moschovitis, G.; Benz, A.; Ramasundarahettige, C.; McIntyre, W.F.; Wong, J.A.; Conen, D.; Sticherling, C.; Connolly, S.J.; et al. Incidence and Predictors of Heart Failure in Patients with Atrial Fibrillation. CJC Open 2021, 3, 1482–1489. [Google Scholar] [CrossRef]
- Xu, H.X.; Zhu, Y.M.; Hua, Y.; Huang, Y.H.; Lu, Q. Association between atrial fibrillation and heart failure with different ejection fraction categories and its influence on outcomes. Acta Cardiol. 2020, 75, 423–432. [Google Scholar] [CrossRef]
- Mentz, R.J.; Roessig, L.; Greenberg, B.H.; Sato, N.; Shinagawa, K.; Yeo, D.; Kwok, B.W.; Reyes, E.B.; Krum, H.; Pieske, B.; et al. Heart Failure Clinical Trials in East and Southeast Asia: Understanding the Importance and Defining the Next Steps. JACC Heart Fail. 2016, 4, 419–427. [Google Scholar] [CrossRef] [PubMed]
- Lip, G.Y.H.; Banerjee, A.; Boriani, G.; Chiang, C.E.; Fargo, R.; Freedman, B.; Lane, D.A.; Ruff, C.T.; Turakhia, M.; Werring, D.; et al. Antithrombotic Therapy for Atrial Fibrillation: CHEST Guideline and Expert Panel Report. Chest 2018, 154, 1121–1201. [Google Scholar] [CrossRef] [PubMed]
- Essien, U.R.; Kim, N.; Hausmann, L.R.M.; Mor, M.K.; Good, C.B.; Magnani, J.W.; Litam, T.M.A.; Gellad, W.F.; Fine, M.J. Disparities in Anticoagulant Therapy Initiation for Incident Atrial Fibrillation by Race/Ethnicity Among Patients in the Veterans Health Administration System. JAMA Netw. Open 2021, 4, e2114234. [Google Scholar] [CrossRef] [PubMed]
- Oh, S.; Goto, S.; Accetta, G.; Angchaisuksiri, P.; Camm, A.J.; Cools, F.; Haas, S.; Kayani, G.; Koretsune, Y.; Lim, T.W.; et al. Vitamin K antagonist control in patients with atrial fibrillation in Asia compared with other regions of the world: Real-world data from the GARFIELD-AF registry. Int. J. Cardiol. 2016, 223, 543–547. [Google Scholar] [CrossRef] [PubMed]
- Johnson, L.S.B.; Oldgren, J.; Barrett, T.W.; McNaughton, C.D.; Wong, J.A.; McIntyre, W.F.; Freeman, C.L.; Murphy, L.; Engstrom, G.; Ezekowitz, M.; et al. LVS-HARMED Risk Score for Incident Heart Failure in Patients With Atrial Fibrillation Who Present to the Emergency Department: Data from a World-Wide Registry. J. Am. Heart Assoc. 2021, 10, e017735. [Google Scholar] [CrossRef] [PubMed]
- Swerdel, J. Predictive Modeling of Incident Heart Failure in Subjects with Newly Diagnosed Atrial Fibrillation. Ph.D. Thesis, Rutgers University-School of Graduate Studies, New Brunswick, NJ, USA, 2019. [Google Scholar] [CrossRef]
- Yang, H.; Negishi, K.; Otahal, P.; Marwick, T.H. Clinical prediction of incident heart failure risk: A systematic review and meta-analysis. Open Heart 2015, 2, e000222. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | All (n = 3402) | Heart Failure during Follow-Up (n = 218) | No Heart Failure during Follow-Up (n = 3184) | p-Value |
|---|---|---|---|---|
| Age (years) | 67.4 ± 11.3 | 70.3 ± 10.8 | 67.2 ± 11.3 | <0.001 * |
| Female gender | 1422 (41.8%) | 106 (48.6%) | 1316 (41.3%) | 0.035 * |
| Time after diagnosis of AF (years) | 3.4 ± 4.3 | 3.9 ±5.1 | 3.3 ± 4.3 | 0.097 |
| Atrial fibrillation | 0.177 | |||
| Paroxysmal | 1148 (33.7%) | 61 (28.0%) | 1087 (34.1%) | |
| Persistent | 643 (18.9%) | 45 (20.6%) | 598 (18.8%) | |
| Permanent | 1611 (47.4%) | 122 (51.4%) | 1499 (47.1%) | |
| Symptomatic AF | 2618 (77.0%) | 165 (75.7%) | 2453 (77.0%) | 0.646 |
| History of heart failure | 912 (26.8%) | 115 (52.8%) | 797 (25.0%) | <0.001 * |
| History of CAD | 547 (16.1%) | 73 (33.5%) | 474 (14.9%) | <0.001 * |
| CIED | 341 (10.0%) | 37 (17.0%) | 304 (9.5%) | <0.001 * |
| History of ischemic stroke/TIA | 592 (17.4%) | 37 (17.0%) | 555 (17.4%) | 0.863 |
| Hypertension | 2328 (68.4%) | 177 (81.2%) | 2151 (67.6%) | <0.001 * |
| Diabetes mellitus | 839 (24.7%) | 97 (44.5%) | 742 (23.3%) | <0.001 * |
| Smoking | 678 (19.9%) | 59 (27.1%) | 619 (19.4%) | 0.006 * |
| Dyslipidemia | 1915 (56.3%) | 146 (67.0%) | 1769 (55.6%) | 0.001 * |
| Renal replacement therapy | 40 (1.2%) | 10 (4.6%) | 30 (0.9%) | <0.001 * |
| Dementia | 29 (0.9%) | 3 (1.4%) | 26 (0.8%) | 0.385 |
| History of bleeding | 323 (9.5%) | 28 (12.8%) | 295 (9.3%) | 0.081 |
| CHA2DS2-VASc score | <0.001 * | |||
| Low risk | 287 (8.4%) | 3 (1.4%) | 284 (8.9%) | |
| Intermediate risk | 546 (16.0%) | 16 (7.3%) | 530 (16.6%) | |
| High risk | 2569 (75.5%) | 199 (91.3%) | 2370 (74.4%) | |
| HAS-BLED score | <0.001 * | |||
| 0 | 490 (14.4%) | 15 (6.9%) | 475 (14.9%) | |
| 1–2 | 2373 (69.8%) | 130 (59.6%) | 2243 (70.4%) | |
| ≥3 | 539 (15.8%) | 73 (33.5%) | 466 (14.6%) | |
| CKD | 2051 (60.3%) | 161 (73.9%) | 1890 (59.4%) | <0.001 * |
| Anemia | 1286 (37.8%) | 120 (55.0%) | 1166 (36.6%) | <0.001 * |
| LVEF < 50% | 618 (18.2%) | 72 (33.0%) | 546 (17.1%) | <0.001 * |
| Antiplatelet | 890 (26.2%) | 87 (39.9%) | 803 (25.2%) | <0.001 * |
| Anticoagulant | 2566 (75.4%) | 168 (77.1%) | 2398 (75.3%) | 0.561 |
| Warfarin | 2338 (68.7%) | 159 (72.9%) | 2179 (68.4%) | 0.166 |
| NOACs | 228 (6.7%) | 9 (4.1%) | 219 (6.9%) | 0.116 |
| Beta blocker | 2476 (72.8%) | 165 (75.7%) | 2311 (72.6%) | 0.319 |
| CCB | 934 (27.5%) | 65 (29.8%) | 869 (27.3%) | 0.419 |
| Digitalis | 539 (15.8%) | 39 (17.9%) | 500 (15.7%) | 0.392 |
| MRA | 280 (8.2%) | 27 (12.4%) | 253 (7.9%) | 0.021 * |
| Statin | 2012 (59.1%) | 156 (71.6%) | 1856 (58.3%) | <0.001 * |
| ACEI/ARB | 1555 (45.7%) | 119 (54.6%) | 1436 (45.1%) | 0.007 * |
| Variable | Univariate Analysis | Multivariable Analysis | ||
|---|---|---|---|---|
| HR (95% CI) | p-Value | HR (95% CI) | p-Value | |
| Age ≥ 65 | 1.82 (1.35–2.46) | <0.001 * | 1.69 (1.24–2.31) | 0.001 * |
| Female gender | 1.34 (1.02–1.74) | 0.033 * | 1.77 (1.29–2.43) | <0.001 * |
| Atrial fibrillation | ||||
| Paroxysmal | Reference | 0.064 | ||
| Persistent | 1.36 (0.92–1.99) | 0.122 | ||
| Permanent | 1.44 (1.06–1.97) | 0.021 * | ||
| Symptomatic AF | 0.95 (0.70–1.29) | 0.737 | ||
| History of heart failure | 2.94 (2.25–3.84) | <0.001 * | 2.36 (1.76–3.17) | <0.001 * |
| History of CAD | 2.69 (2.03–3.57) | <0.001 * | 1.68 (1.25–2.27) | 0.001 * |
| CIED | 1.66 (1.17–2.37) | 0.005 * | 1.55 (1.08–2.23) | 0.018 * |
| History of ischemic stroke/TIA | 1.00 (0.70–1.43) | 0.998 | ||
| Diabetes mellitus | 2.50 (1.91–3.27) | <0.001 * | 2.02 (1.53–2.66) | <0.001 * |
| Hypertension | 1.97 (1.40–2.77) | <0.001 * | 1.46 (1.02–2.08) | 0.038 * |
| Smoking | 1.39 (1.03–1.87) | 0.031 * | 1.74 (1.23–2.47) | 0.002 * |
| Dyslipidemia | 1.62 (1.22–2.16) | 0.001 * | ||
| Renal replacement therapy | 4.89 (2.59–9.22) | <0.001 * | 4.20 (2.19–8.04) | <0.001 * |
| Dementia | 1.57 (0.50–4.91) | 0.437 | ||
| History of bleeding | 1.35 (0.91–2.01) | 0.138 | ||
| History of bleeding | 1.30 (0.87–1.95) | 0.198 | ||
| CKD | 1.91 (1.41–2.58) | <0.001 * | ||
| Anemia | 2.12 (1.63–2.77) | <0.001 * | ||
| LVEF < 50% | 2.36 (1.78–3.12) | <0.001 * | 1.77 (1.29–2.44) | <0.001 * |
| Antiplatelet | 1.79 (1.36–2.34) | <0.001 * | ||
| Anticoagulant | 1.15 (0.84–1.58) | 0.378 | ||
| Warfarin | 1.27 (0.94–1.72) | 0.115 | ||
| NOACs | 0.61 (0.31–1.18) | 0.142 | ||
| Beta blocker | 1.17 (0.86–1.60) | 0.315 | ||
| CCB | 1.16 (0.87–1.55) | 0.321 | ||
| Digitalis | 1.13 (0.80–1.60) | 0.489 | ||
| MRA | 1.63 (1.09–2.44) | 0.017 * | ||
| Statin | 1.82 (1.36–2.45) | <0.001 * | ||
| ACEI/ARB | 1.43 (1.09–1.87) | 0.009 * | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Krittayaphong, R.; Chichareon, P.; Komoltri, C.; Sairat, P.; Lip, G.Y.H. Predicting Heart Failure in Patients with Atrial Fibrillation: A Report from the Prospective COOL-AF Registry. J. Clin. Med. 2023, 12, 1265. https://doi.org/10.3390/jcm12041265
Krittayaphong R, Chichareon P, Komoltri C, Sairat P, Lip GYH. Predicting Heart Failure in Patients with Atrial Fibrillation: A Report from the Prospective COOL-AF Registry. Journal of Clinical Medicine. 2023; 12(4):1265. https://doi.org/10.3390/jcm12041265
Chicago/Turabian StyleKrittayaphong, Rungroj, Ply Chichareon, Chulalak Komoltri, Poom Sairat, and Gregory Y. H. Lip. 2023. "Predicting Heart Failure in Patients with Atrial Fibrillation: A Report from the Prospective COOL-AF Registry" Journal of Clinical Medicine 12, no. 4: 1265. https://doi.org/10.3390/jcm12041265