
Immediate Effects of Myofascial Release Treatment on Lumbar Microcirculation: A Randomized, Placebo-Controlled Trial
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design Overview
2.2. Setting and Participants
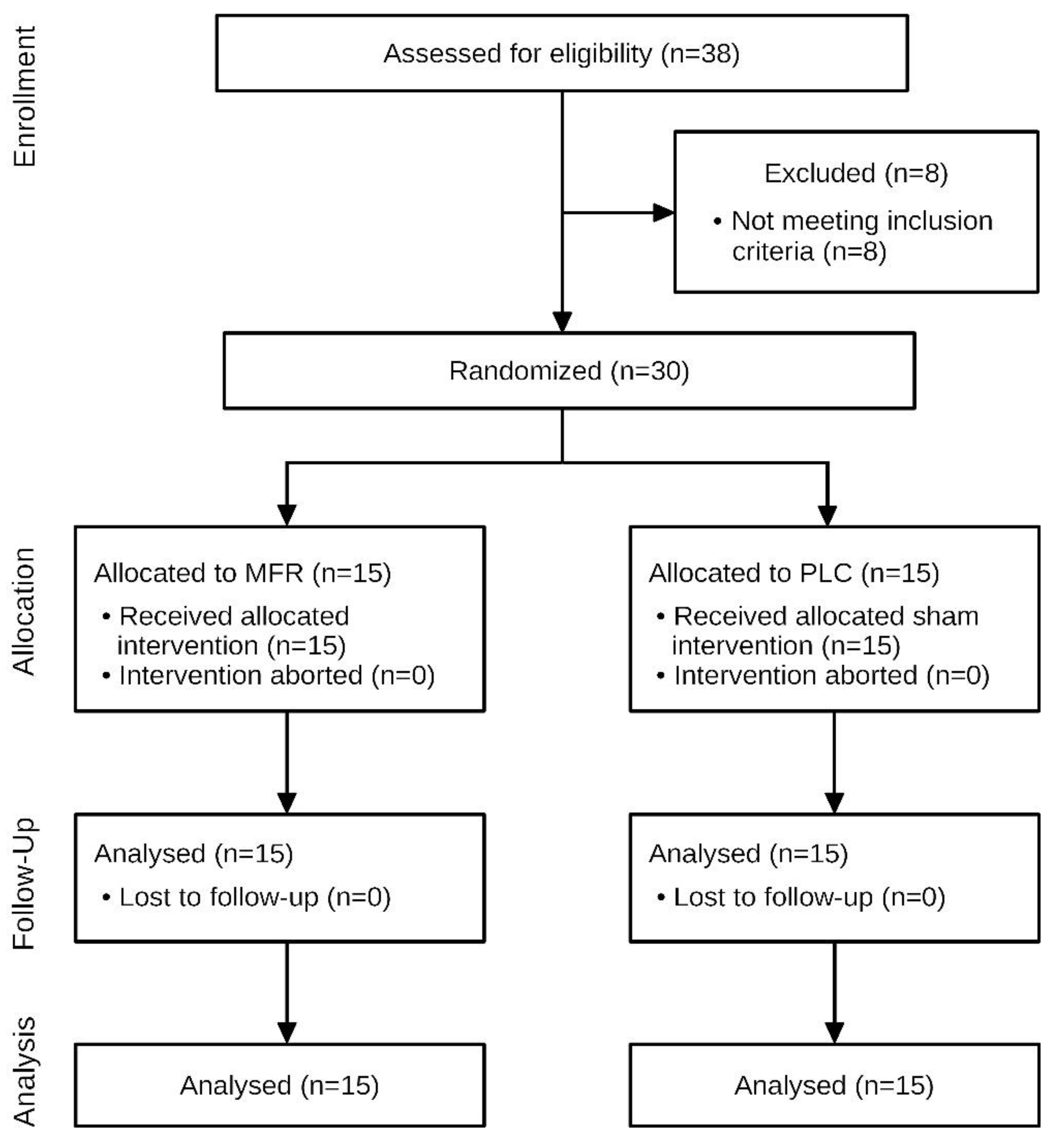
2.3. Randomization and Interventions
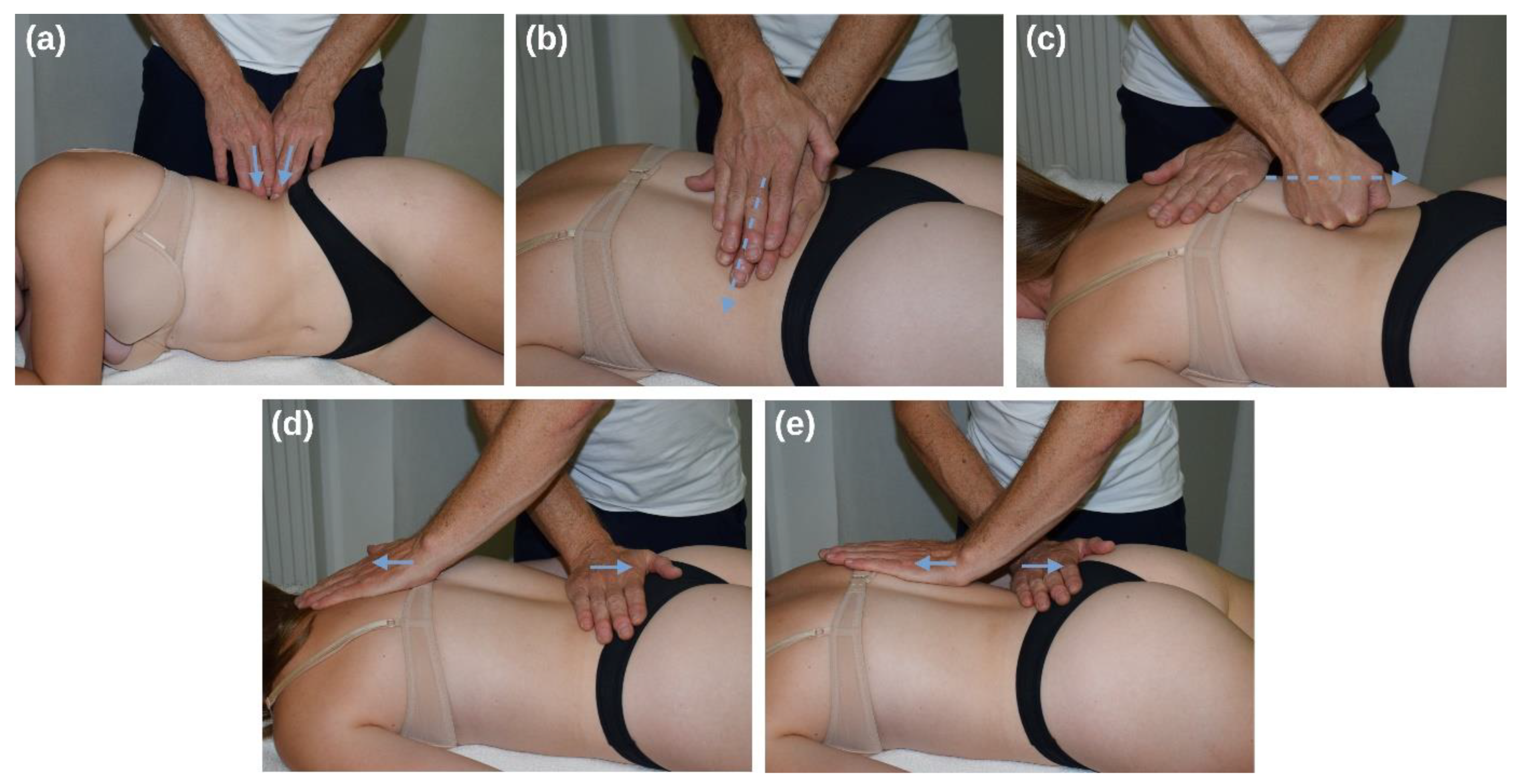
2.3.1. Myofascial Release Intervention
2.3.2. Control Group
2.4. Outcomes
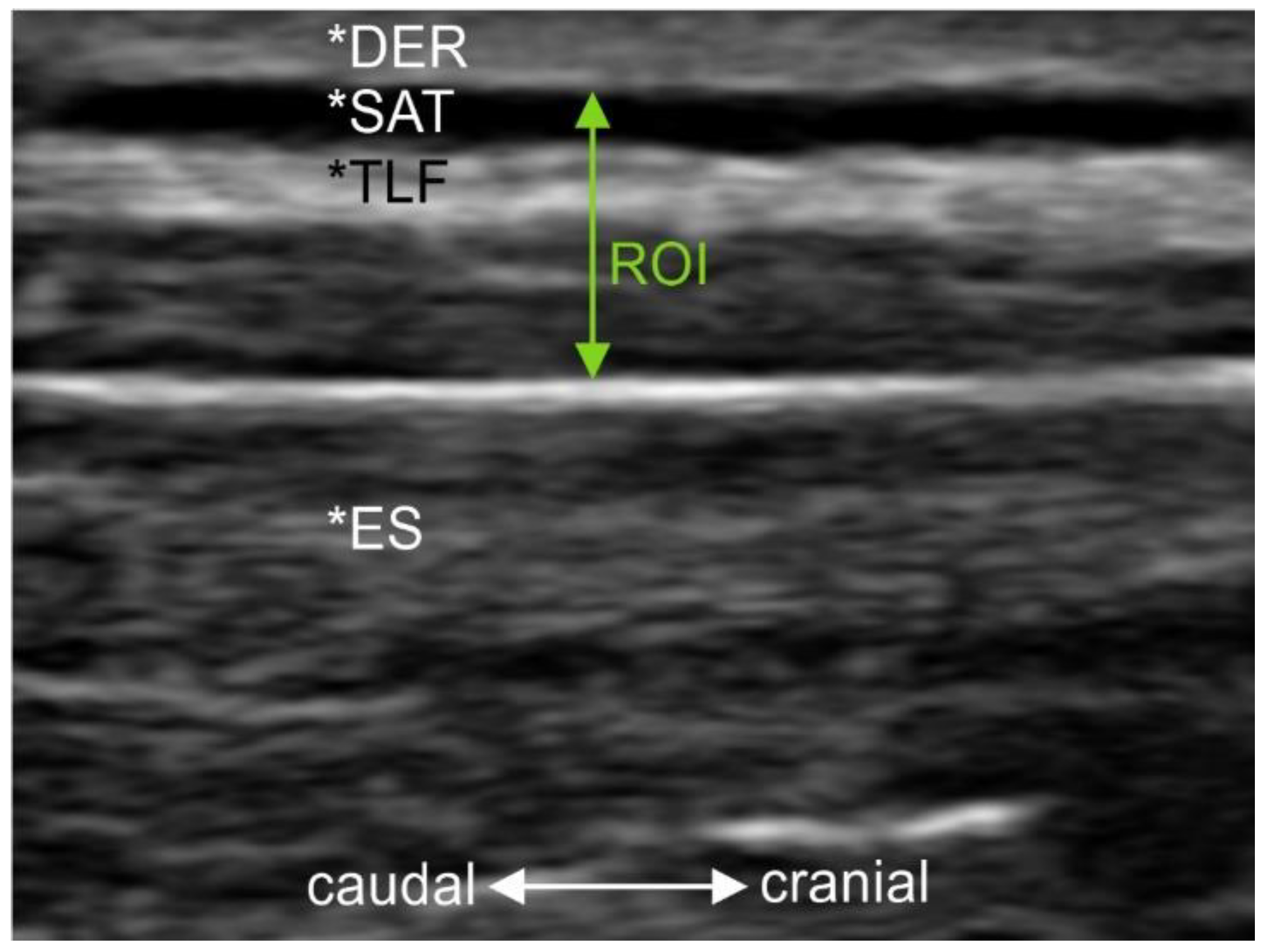
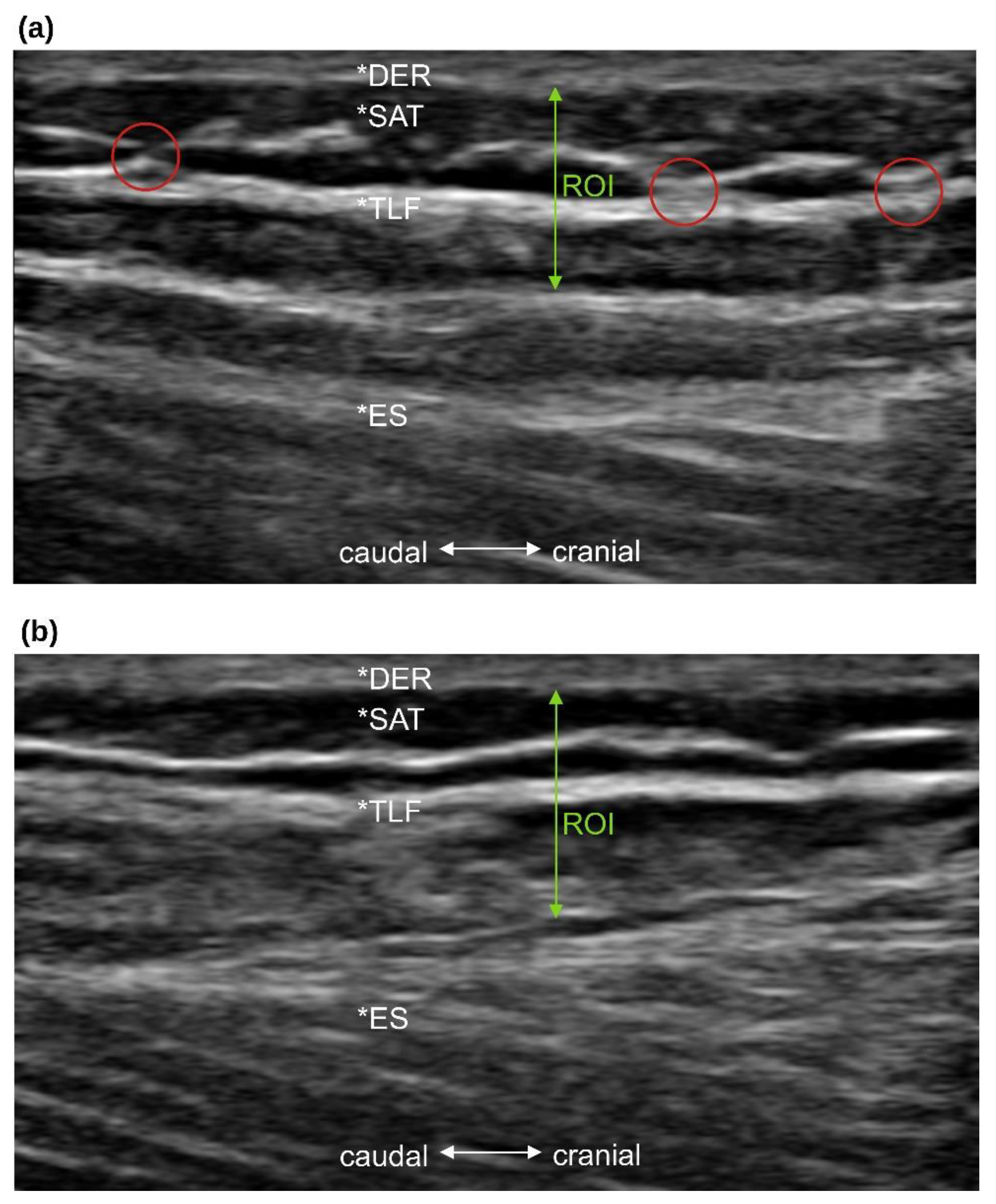
2.4.1. Thoracolumbar Fascia Morphology
2.4.2. Blood Flow Measurements
2.5. Statistics
3. Results
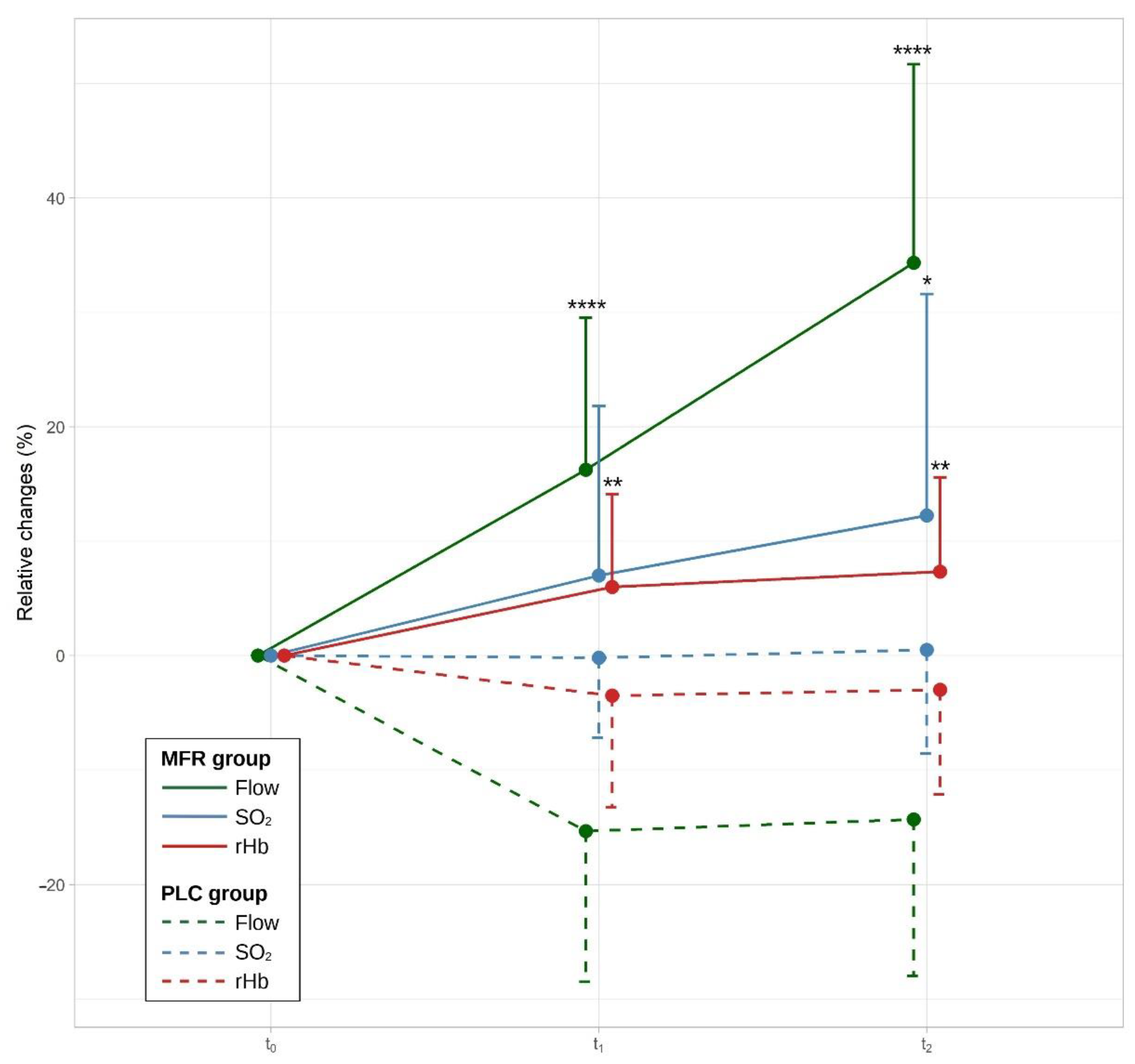
3.1. Primary Objective: Difference between Myofascial Release Treatment and Placebo Intervention
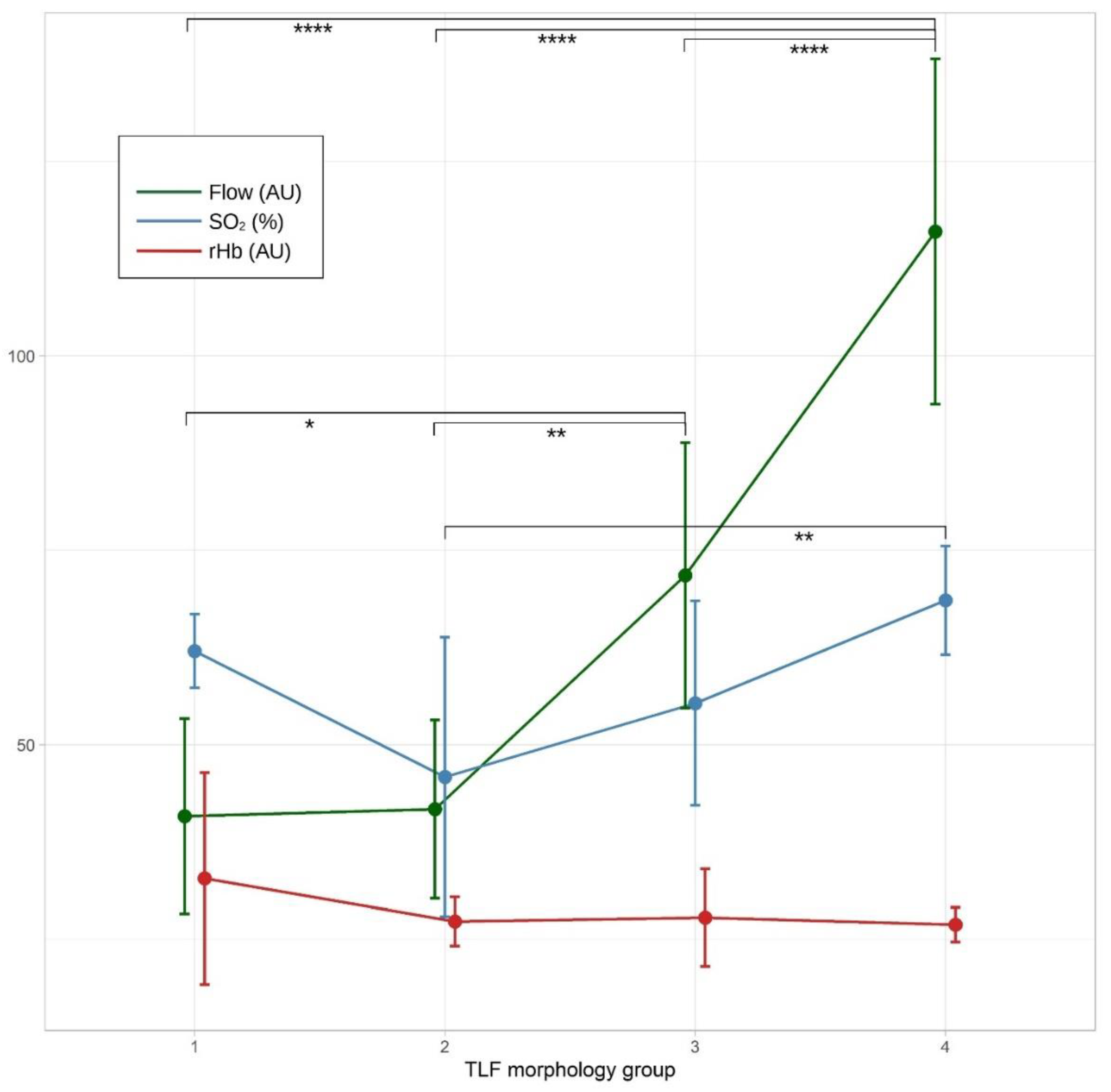
3.2. Secondary Objectives: Influence of Thoracolumbar Fascia Morphology and Physical Activity on Microcirculation in Lumbar Tissue and Their Correlations
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Willard, F.H.; Vleeming, A.; Schuenke, M.D.; Danneels, L.; Schleip, R. The Thoracolumbar Fascia: Anatomy, Function and Clinical Considerations. J. Anat. 2012, 221, 507–536. [Google Scholar] [CrossRef] [PubMed]
- Langevin, H.M.; Fox, J.R.; Koptiuch, C.; Badger, G.J.; Greenan-Naumann, A.C.; Bouffard, N.A.; Konofagou, E.E.; Lee, W.-N.; Triano, J.J.; Henry, S.M. Reduced Thoracolumbar Fascia Shear Strain in Human Chronic Low Back Pain. BMC Musculoskelet. Disord. 2011, 12, 203. [Google Scholar] [CrossRef]
- Schleip, R.; Gabbiani, G.; Wilke, J.; Naylor, I.; Hinz, B.; Zorn, A.; Jäger, H.; Breul, R.; Schreiner, S.; Klingler, W. Fascia Is Able to Actively Contract and May Thereby Influence Musculoskeletal Dynamics: A Histochemical and Mechanographic Investigation. Front. Physiol. 2019, 10, 336. [Google Scholar] [CrossRef] [PubMed]
- Brandl, A.; Egner, C.; Schleip, R. Immediate Effects of Myofascial Release on the Thoracolumbar Fascia and Osteopathic Treatment for Acute Low Back Pain on Spine Shape Parameters: A Randomized, Placebo-Controlled Trial. Life 2021, 11, 845. [Google Scholar] [CrossRef] [PubMed]
- Mense, S. Innervation of the Thoracolumbar Fascia. Eur. J. Transl. Myol. 2019, 29, 151–158. [Google Scholar] [CrossRef]
- Tesarz, J.; Hoheisel, U.; Wiedenhöfer, B.; Mense, S. Sensory Innervation of the Thoracolumbar Fascia in Rats and Humans. Neuroscience 2011, 194, 302–308. [Google Scholar] [CrossRef] [PubMed]
- Fede, C.; Petrelli, L.; Guidolin, D.; Porzionato, A.; Pirri, C.; Fan, C.; De Caro, R.; Stecco, C. Evidence of a New Hidden Neural Network into Deep Fasciae. Sci. Rep. 2021, 11, 12623. [Google Scholar] [CrossRef]
- Wilke, J.; Schleip, R.; Klingler, W.; Stecco, C. The Lumbodorsal Fascia as a Potential Source of Low Back Pain: A Narrative Review. BioMed Res. Int. 2017, 2017, 5349620. [Google Scholar] [CrossRef]
- Wilke, J.; Schleip, R.; Yucesoy, C.A.; Banzer, W. Not Merely a Protective Packing Organ? A Review of Fascia and Its Force Transmission Capacity. J. Appl. Physiol. 2018, 124, 234–244. [Google Scholar] [CrossRef]
- Wilke, J.; Macchi, V.; De Caro, R.; Stecco, C. Fascia Thickness, Aging and Flexibility: Is There an Association? J. Anat. 2019, 234, 43–49. [Google Scholar] [CrossRef] [Green Version]
- Li, W.; Ahn, A.C. Subcutaneous Fascial Bands—A Qualitative and Morphometric Analysis. PLoS ONE 2011, 6, e23987. [Google Scholar] [CrossRef] [PubMed]
- Vleeming, A.; Schuenke, M.D.; Danneels, L.; Willard, F.H. The Functional Coupling of the Deep Abdominal and Paraspinal Muscles: The Effects of Simulated Paraspinal Muscle Contraction on Force Transfer to the Middle and Posterior Layer of the Thoracolumbar Fascia. J. Anat. 2014, 225, 447–462. [Google Scholar] [CrossRef]
- Pavan, P.G.; Stecco, A.; Stern, R.; Stecco, C. Painful Connections: Densification versus Fibrosis of Fascia. Curr. Pain Headache Rep. 2014, 18, 441. [Google Scholar] [CrossRef]
- Corey, S.M.; Vizzard, M.A.; Bouffard, N.A.; Badger, G.J.; Langevin, H.M. Stretching of the Back Improves Gait, Mechanical Sensitivity and Connective Tissue Inflammation in a Rodent Model. PLoS ONE 2012, 7, e29831. [Google Scholar] [CrossRef]
- Bishop, J.H.; Fox, J.R.; Maple, R.; Loretan, C.; Badger, G.J.; Henry, S.M.; Vizzard, M.A.; Langevin, H.M. Ultrasound Evaluation of the Combined Effects of Thoracolumbar Fascia Injury and Movement Restriction in a Porcine Model. PLoS ONE 2016, 11, e0147393. [Google Scholar] [CrossRef] [PubMed]
- Hoheisel, U.; Rosner, J.; Mense, S. Innervation Changes Induced by Inflammation of the Rat Thoracolumbar Fascia. Neuroscience 2015, 300, 351–359. [Google Scholar] [CrossRef] [PubMed]
- Tong, M.H.; Mousavi, S.J.; Kiers, H.; Ferreira, P.; Refshauge, K.; van Dieën, J. Is There a Relationship between Lumbar Proprioception and Low Back Pain? A Systematic Review with Meta-Analysis. Arch. Phys. Med. Rehabil. 2017, 98, 120–136. [Google Scholar] [CrossRef]
- Langevin, H.M.; Stevens-Tuttle, D.; Fox, J.R.; Badger, G.J.; Bouffard, N.A.; Krag, M.H.; Wu, J.; Henry, S.M. Ultrasound Evidence of Altered Lumbar Connective Tissue Structure in Human Subjects with Chronic Low Back Pain. BMC Musculoskelet. Disord. 2009, 10, 151. [Google Scholar] [CrossRef]
- Langevin, H.M.; Bishop, J.; Maple, R.; Badger, G.J.; Fox, J.R. Effect of Stretching on Thoracolumbar Fascia Injury and Movement Restriction in a Porcine Model. Am. J. Phys. Med. Rehabil. 2018, 97, 187–191. [Google Scholar] [CrossRef]
- De Coninck, K.; Hambly, K.; Dickinson, J.W.; Passfield, L. Measuring the Morphological Characteristics of Thoracolumbar Fascia in Ultrasound Images: An Inter-Rater Reliability Study. BMC Musculoskelet. Disord. 2018, 19, 180. [Google Scholar] [CrossRef]
- Adamietz, B.; Schönberg, S.O.; Reiser, M.; Uder, M.; Frank, A.; Strecker, R.; Weiß, C.; Heiss, R. Visualization of the Epimysium and Fascia Thoracolumbalis at the Lumbar Spine Using MRI. Radiologe 2021, 61, 49–53. [Google Scholar] [CrossRef]
- Calanni, L.; Zampella, C.; Micheletti, P.; Greco, D.; Negro, M.; D’Antona, G. Correlation between Patellar Tendon Mechanical Properties and Oxygenation Detection by Near Infrared Spectroscopy in Males. Muscle Ligaments Tendons J. 2021, 11, 54–61. [Google Scholar] [CrossRef]
- Wezenbeek, E.; Willems, T.; Mahieu, N.; De Muynck, M.; Vanden Bossche, L.; Steyaert, A.; De Clercq, D.; Witvrouw, E. The Role of the Vascular and Structural Response to Activity in the Development of Achilles Tendinopathy: A Prospective Study. Am. J. Sports Med. 2018, 46, 947–954. [Google Scholar] [CrossRef] [PubMed]
- Hotta, K.; Behnke, B.J.; Arjmandi, B.; Ghosh, P.; Chen, B.; Brooks, R.; Maraj, J.J.; Elam, M.L.; Maher, P.; Kurien, D.; et al. Daily Muscle Stretching Enhances Blood Flow, Endothelial Function, Capillarity, Vascular Volume and Connectivity in Aged Skeletal Muscle. J. Physiol. 2018, 596, 1903–1917. [Google Scholar] [CrossRef] [PubMed]
- Schleip, R. Fascial Plasticity—A New Neurobiological Explanation: Part 1. J. Bodyw. Mov. Ther. 2003, 7, 11–19. [Google Scholar] [CrossRef]
- Schleip, R. Fascial Plasticity—A New Neurobiological Explanation Part 2. J. Bodyw. Mov. Ther. 2003, 7, 104–116. [Google Scholar] [CrossRef]
- Ajimsha, M.S.; Al-Mudahka, N.R.; Al-Madzhar, J.A. Effectiveness of Myofascial Release: Systematic Review of Randomized Controlled Trials. J. Bodyw. Mov. Ther. 2015, 19, 102–112. [Google Scholar] [CrossRef] [PubMed]
- Wu, Z.; Wang, Y.; Ye, X.; Chen, Z.; Zhou, R.; Ye, Z.; Huang, J.; Zhu, Y.; Chen, G.; Xu, X. Myofascial Release for Chronic Low Back Pain: A Systematic Review and Meta-Analysis. Front. Med. 2021, 8, 697986. [Google Scholar] [CrossRef]
- Stecco, A.; Stern, R.; Fantoni, I.; De Caro, R.; Stecco, C. Fascial Disorders: Implications for Treatment. PM&R 2016, 8, 161–168. [Google Scholar] [CrossRef]
- Brandl, A.; Egner, C.; Schwarze, M.; Reer, R.; Schmidt, T.; Schleip, R. Immediate Effects of Instrument-Assisted Soft Tissue Mobilization on Hydration Content in Lumbar Myofascial Tissues: A Quasi-Experiment. J. Clin. Med. 2023, 12, 1009. [Google Scholar] [CrossRef]
- Meltzer, K.R.; Cao, T.V.; Schad, J.F.; King, H.; Stoll, S.T.; Standley, P.R. In Vitro Modeling of Repetitive Motion Injury and Myofascial Release. J. Bodyw. Mov. Ther. 2010, 14, 162–171. [Google Scholar] [CrossRef]
- Tozzi, P. A Unifying Neuro-Fasciagenic Model of Somatic Dysfunction—Underlying Mechanisms and Treatment—Part I. J. Bodyw. Mov. Ther. 2015, 19, 310–326. [Google Scholar] [CrossRef] [PubMed]
- Zegarra-Parodi, R.; Pazdernik, V.K.; Roustit, M.; Park, P.Y.S.; Degenhardt, B.F. Effects of Pressure Applied during Standardized Spinal Mobilizations on Peripheral Skin Blood Flow: A Randomised Cross-over Study. Man. Ther. 2016, 21, 220–226. [Google Scholar] [CrossRef] [PubMed]
- Portillo-Soto, A.; Eberman, L.E.; Demchak, T.J.; Peebles, C. Comparison of Blood Flow Changes with Soft Tissue Mobilization and Massage Therapy. J. Altern. Complement. Med. 2014, 20, 932–936. [Google Scholar] [CrossRef] [PubMed]
- World Medical Association. World Medical Association Declaration of Helsinki: Ethical Principles for Medical Research Involving Human Subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Lang, A.-G.; Buchner, A. G*Power 3: A Flexible Statistical Power Analysis Program for the Social, Behavioral, and Biomedical Sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Bundesärztekammer (BÄK); Kassenärztliche Bundesvereinigung (KBV); Arbeitsgemeinschaft der Wissenschaftlichen Medizinischen Fachgesellschaften (AWMF). Nationale VersorgungsLeitlinie Nicht-Spezifischer Kreuzschmerz—Langfassung; 2. Auflage; Bundesärztekammer; Kassenärztliche Bundesvereinigung; Arbeitsgemeinschaft der Wissenschaftlichen Medizinischen Fachgesellschaften: Berlin, Germany, 2017. [Google Scholar]
- Meh, K.; Jurak, G.; Sorić, M.; Rocha, P.; Sember, V. Validity and Reliability of IPAQ-SF and GPAQ for Assessing Sedentary Behaviour in Adults in the European Union: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 4602. [Google Scholar] [CrossRef]
- Chen, Y.-H.; Chai, H.-M.; Shau, Y.-W.; Wang, C.-L.; Wang, S.-F. Increased Sliding of Transverse Abdominis during Contraction after Myofascial Release in Patients with Chronic Low Back Pain. Man. Ther. 2016, 23, 69–75. [Google Scholar] [CrossRef]
- Wong, C.K. Strain Counterstrain: Current Concepts and Clinical Evidence. Man. Ther. 2012, 17, 2–8. [Google Scholar] [CrossRef]
- Arguisuelas, M.D.; Lison, J.F.; Domenech-Fernandez, J.; Martinez-Hurtado, I.; Coloma, P.S.; Sanchez-Zuriaga, D. Effects of Myofascial Release in Erector Spinae Myoelectric Activity and Lumbar Spine Kinematics in Non-Specific Chronic Low Back Pain: Randomized Controlled Trial. Clin. Biomech 2019, 63, 27–33. [Google Scholar] [CrossRef]
- Stokes, M.; Hides, J.; Elliott, J.; Kiesel, K.; Hodges, P. Rehabilitative Ultrasound Imaging of the Posterior Paraspinal Muscles. J. Orthop. Sports Phys. Ther. 2007, 37, 581–595. [Google Scholar] [CrossRef] [PubMed]
- Almazán-Polo, J.; López-López, D.; Romero-Morales, C.; Rodríguez-Sanz, D.; Becerro-de-Bengoa-Vallejo, R.; Losa-Iglesias, M.E.; Bravo-Aguilar, M.; Calvo-Lobo, C. Quantitative Ultrasound Imaging Differences in Multifidus and Thoracolumbar Fasciae between Athletes with and without Chronic Lumbopelvic Pain: A Case-Control Study. J. Clin. Med. 2020, 9, 2647. [Google Scholar] [CrossRef] [PubMed]
- Wezenbeek, E.; Willems, T.M.; Mahieu, N.; Van Caekenberghe, I.; Witvrouw, E.; De Clercq, D. Is Achilles Tendon Blood Flow Related to Foot Pronation? Scand. J. Med. Sci. Sports 2017, 27, 1970–1977. [Google Scholar] [CrossRef] [PubMed]
- Fleiss, J.L. Reliability of Measurement. In Design and Analysis of Clinical Experiments; John Wiley & Sons: Hoboken, NJ, USA, 2011; pp. 1–32. [Google Scholar]
- Cohen, J. A Power Primer. Psychol. Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef]
- Brandl, A.; Egner, C.; Reer, R.; Schmidt, T.; Schleip, R. Associations between Deformation of the Thoracolumbar Fascia and Activation of the Erector Spinae and Multifidus Muscle in Patients with Acute Low Back Pain and Healthy Controls: A Matched Pair Case-Control Study. Life 2022, 12, 1735. [Google Scholar] [CrossRef]
- Zullo, A.; Mancini, F.P.; Schleip, R.; Wearing, S.; Klingler, W. Fibrosis: Sirtuins at the Checkpoints of Myofibroblast Differentiation and Profibrotic Activity. Wound Repair Regen. 2021, 29, 650–666. [Google Scholar] [CrossRef]
- Ubbink, R.; Bettink, M.A.W.; Janse, R.; Harms, F.A.; Johannes, T.; Münker, F.M.; Mik, E.G. A Monitor for Cellular Oxygen METabolism (COMET): Monitoring Tissue Oxygenation at the Mitochondrial Level. J Clin Monit Comput 2017, 31, 1143–1150. [Google Scholar] [CrossRef]
- Ritschl, L.M.; Schmidt, L.H.; Fichter, A.M.; Hapfelmeier, A.; Wolff, K.-D.; Mücke, T. Multimodal Analysis Using Flowmeter Analysis, Laser-Doppler Spectrophotometry, and Indocyanine Green Videoangiography for the Detection of Venous Compromise in Flaps in Rats. J. Cranio-Maxillofac. Surg. 2018, 46, 905–915. [Google Scholar] [CrossRef]
- Sinhorim, L.; dos Santos Amorim, M.; Ortiz, M.E.; Bittencourt, E.B.; Bianco, G.; da Silva, F.C.; Horewicz, V.V.; Schleip, R.; Reed, W.R.; Mazzardo-Martins, L.; et al. Potential Nociceptive Role of the Thoracolumbar Fascia: A Scope Review Involving In Vivo and Ex Vivo Studies. J. Clin. Med. 2021, 10, 4342. [Google Scholar] [CrossRef]
- Latimer, J.; Lee, M.; Adams, R.; Moran, C.M. An Investigation of the Relationship between Low Back Pain and Lumbar Posteroanterior Stiffness. J. Manip. Physiol. Ther. 1996, 19, 587–591. [Google Scholar]
- Kędra, A.; Plandowska, M.; Kędra, P.; Czaprowski, D. Physical Activity and Low Back Pain in Children and Adolescents: A Systematic Review. Eur. Spine J. 2021, 30, 946–956. [Google Scholar] [CrossRef] [PubMed]
- Wakker, J.; Kratzer, W.; Schmidberger, J.; Graeter, T.; Boretzki, S.; Schulze, J.; Uhlemann, S.; Heizelmann, A.; Stumpf, S.; Jäger, H.; et al. Elasticity Standard Values of the Thoracolumbar Fascia Assessed with Acoustic Radiation Force Impulse Elastography on Healthy Volunteers: A Cross Section Study. J. Bodyw. Mov. Ther. 2021, 26, 530–537. [Google Scholar] [CrossRef] [PubMed]
- Santos, T.S.; Oliveira, K.K.B.; Martins, L.V.; Vidal, A.P.C. Effects of Manual Therapy on Body Posture: Systematic Review and Meta-Analysis. Gait Posture 2022, 96, 280–294. [Google Scholar] [CrossRef] [PubMed]
- Deng, H.B.; Macfarlane, D.J.; Thomas, G.N.; Lao, X.Q.; Jiang, C.Q.; Cheng, K.K.; Lam, T.H. Reliability and Validity of the IPAQ-Chinese: The Guangzhou Biobank Cohort Study. Med. Sci. Sports Exerc. 2008, 40, 303–307. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Baseline Characteristics | Participants (n = 30) Mean ± SD |
|---|---|
| Gender (men/women) | 15/15 |
| Age (years) | 40.5 ± 14.1 |
| Height (m) | 1.73 ± 0.1 |
| Weight (kg) | 69.0 ± 11.5 |
| BMI (kg/m2) | 23.0 ± 3.2 |
| Physical activity (IPAQ) | |
| High, n (%) | 11 (36) |
| Moderate, n (%) | 12 (40) |
| Low, n (%) | 7 (23) |
| 95% Confidence Interval of Mean | ||||||
|---|---|---|---|---|---|---|
| Outcome | Time | Group | n | Mean ± SD | Lower Bound | Upper Bound |
| Flow | t1 | MFR | 15 | 16.20 ± 13.30 | 8.84 | 23.56 |
| PLC | 15 | −15.40 ± 16.10 | −22.68 | −8.12 | ||
| t2 | MFR | 15 | 34.40 ± 17.40 | 24.79 | 44.01 | |
| PLC | 15 | −14.30 ± 13.70 | −21.87 | −6.73 | ||
| SO2 | t1 | MFR | 15 | 6.78 ± 14.80 | −1.42 | 14.98 |
| PLC | 15 | −0.19 ± 7.00 | −4.06 | 3.68 | ||
| t2 | MFR | 15 | 12.20 ± 19.40 | 1.50 | 22.90 | |
| PLC | 15 | 0.51 ± 9.08 | −4.52 | 5.54 | ||
| rHb | t1 | MFR | 15 | 6.56 ± 8.11 | 2.10 | 11.08 |
| PLC | 15 | −3.51 ± 9.74 | −8.91 | 1.89 | ||
| t2 | MFR | 15 | 7.33 ± 8.24 | 2.76 | 11.90 | |
| PLC | 15 | −3.00 ± 9.14 | −8.06 | 2.06 | ||
| 95% Confidence Interval of Mean | |||||
|---|---|---|---|---|---|
| TLF Groups | Mean (AU) | Lower Bound | Upper Bound | p (Adj.) | |
| 1 (n = 5) | 2 (n = 7) | 0.91 | −26.7 | 28.5 | 1 |
| 1 (n = 5) | 3 (n = 9) | 31.0 | 4.66 | 57.3 | 0.0167 |
| 1 (n = 5) | 4 (n = 9) | 75.2 | 48.9 | 102 | <0.0001 |
| 2 (n = 7) | 3 (n = 9) | 30.1 | 6.28 | 53.8 | 0.0093 |
| 2 (n = 7) | 4 (n = 9) | 74.3 | 50.5 | 98.1 | <0.0001 |
| 3 (n = 9) | 4 (n = 9) | 44.2 | 22.0 | 66.5 | <0.0001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brandl, A.; Egner, C.; Reer, R.; Schmidt, T.; Schleip, R. Immediate Effects of Myofascial Release Treatment on Lumbar Microcirculation: A Randomized, Placebo-Controlled Trial. J. Clin. Med. 2023, 12, 1248. https://doi.org/10.3390/jcm12041248
Brandl A, Egner C, Reer R, Schmidt T, Schleip R. Immediate Effects of Myofascial Release Treatment on Lumbar Microcirculation: A Randomized, Placebo-Controlled Trial. Journal of Clinical Medicine. 2023; 12(4):1248. https://doi.org/10.3390/jcm12041248
Chicago/Turabian StyleBrandl, Andreas, Christoph Egner, Rüdiger Reer, Tobias Schmidt, and Robert Schleip. 2023. "Immediate Effects of Myofascial Release Treatment on Lumbar Microcirculation: A Randomized, Placebo-Controlled Trial" Journal of Clinical Medicine 12, no. 4: 1248. https://doi.org/10.3390/jcm12041248