
Clinical Trial for the Safety and Feasibility of Pedicle Screws Coated with a Fibroblast Growth Factor-2-Apatite Composite Layer for Posterior Cervical Fusion Surgery
 , ,
, ,
Abstract
:1. Introduction
2. Methods
Trial Protocol
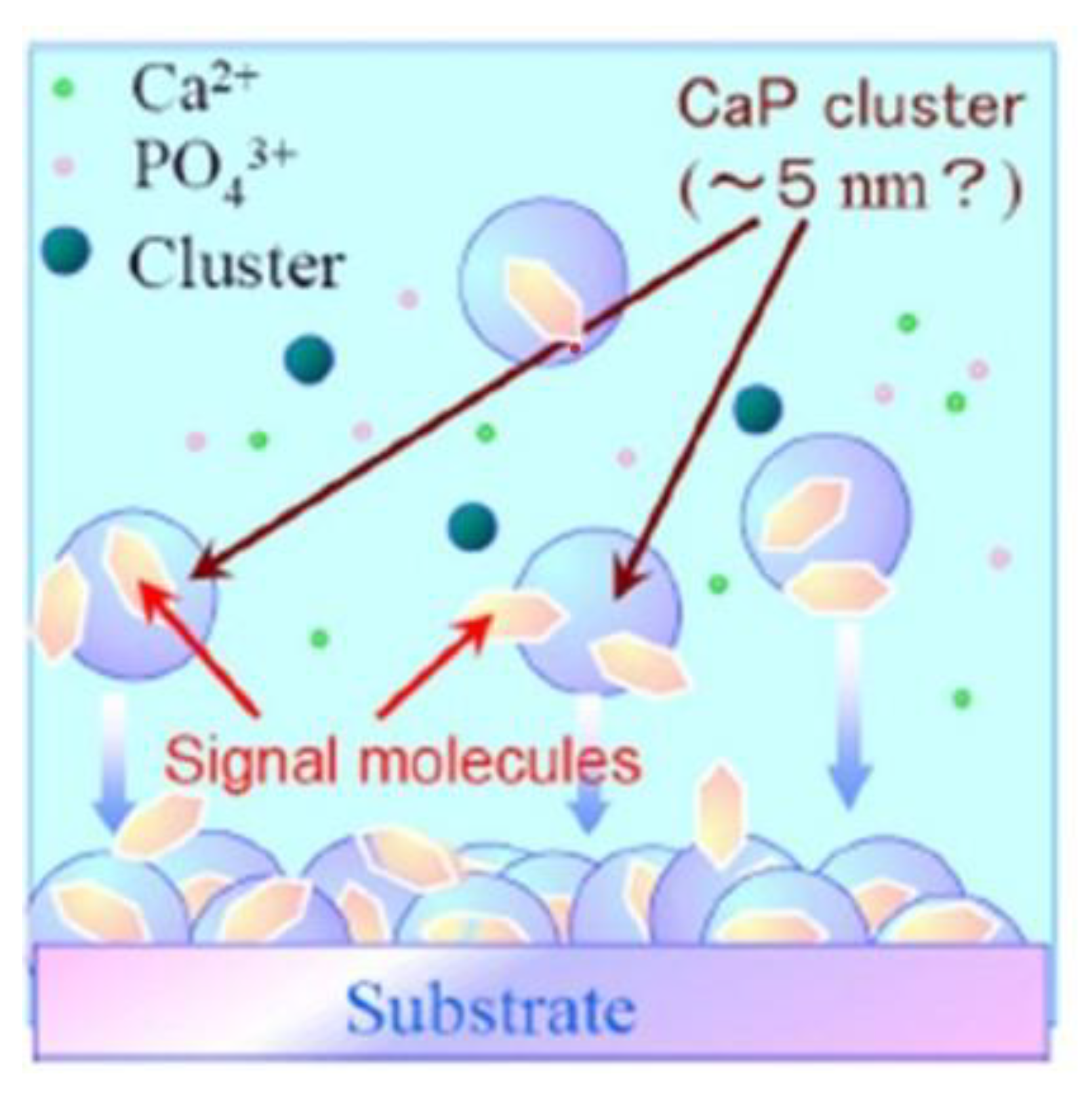
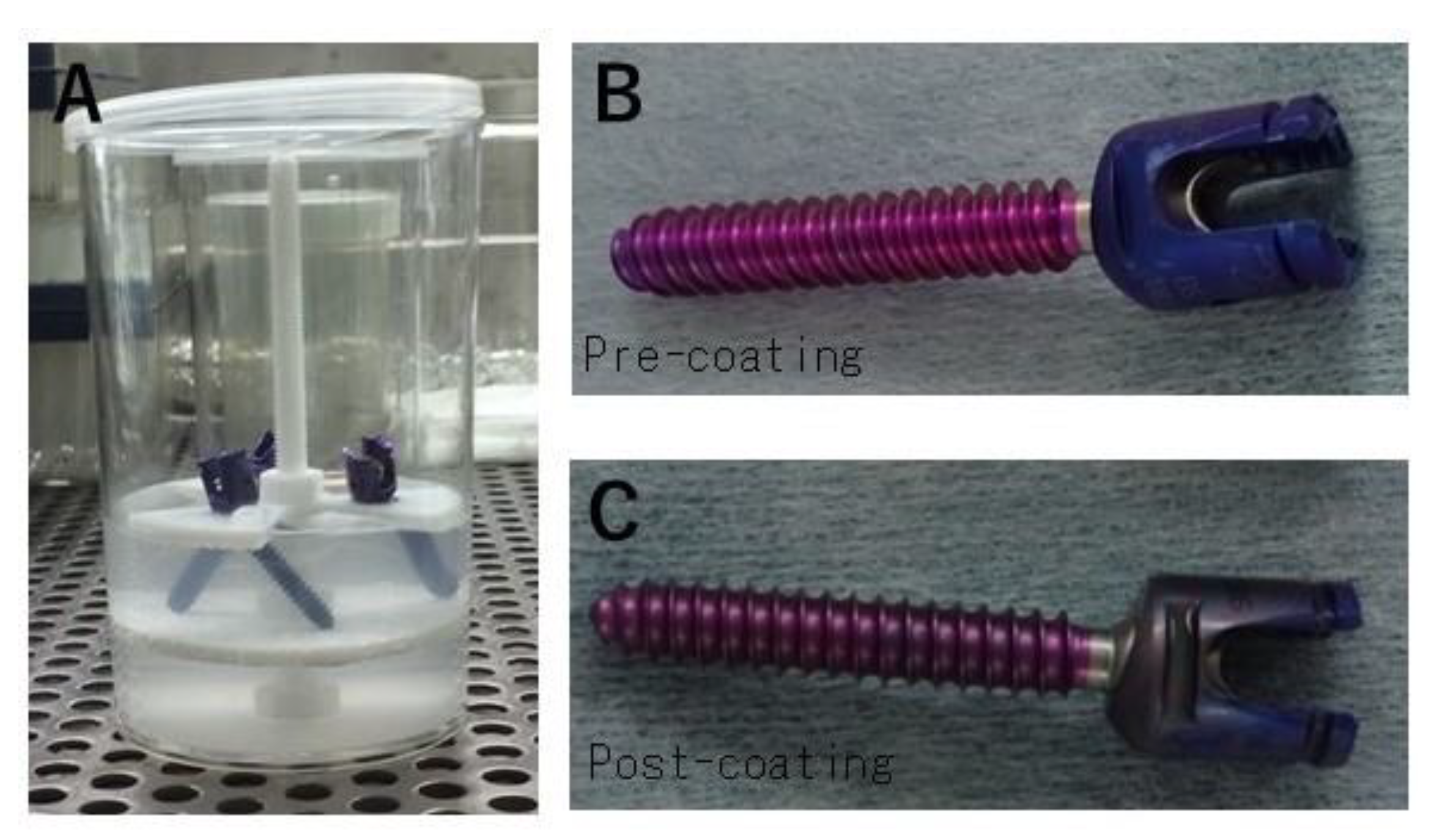
Ap-FGF Coating
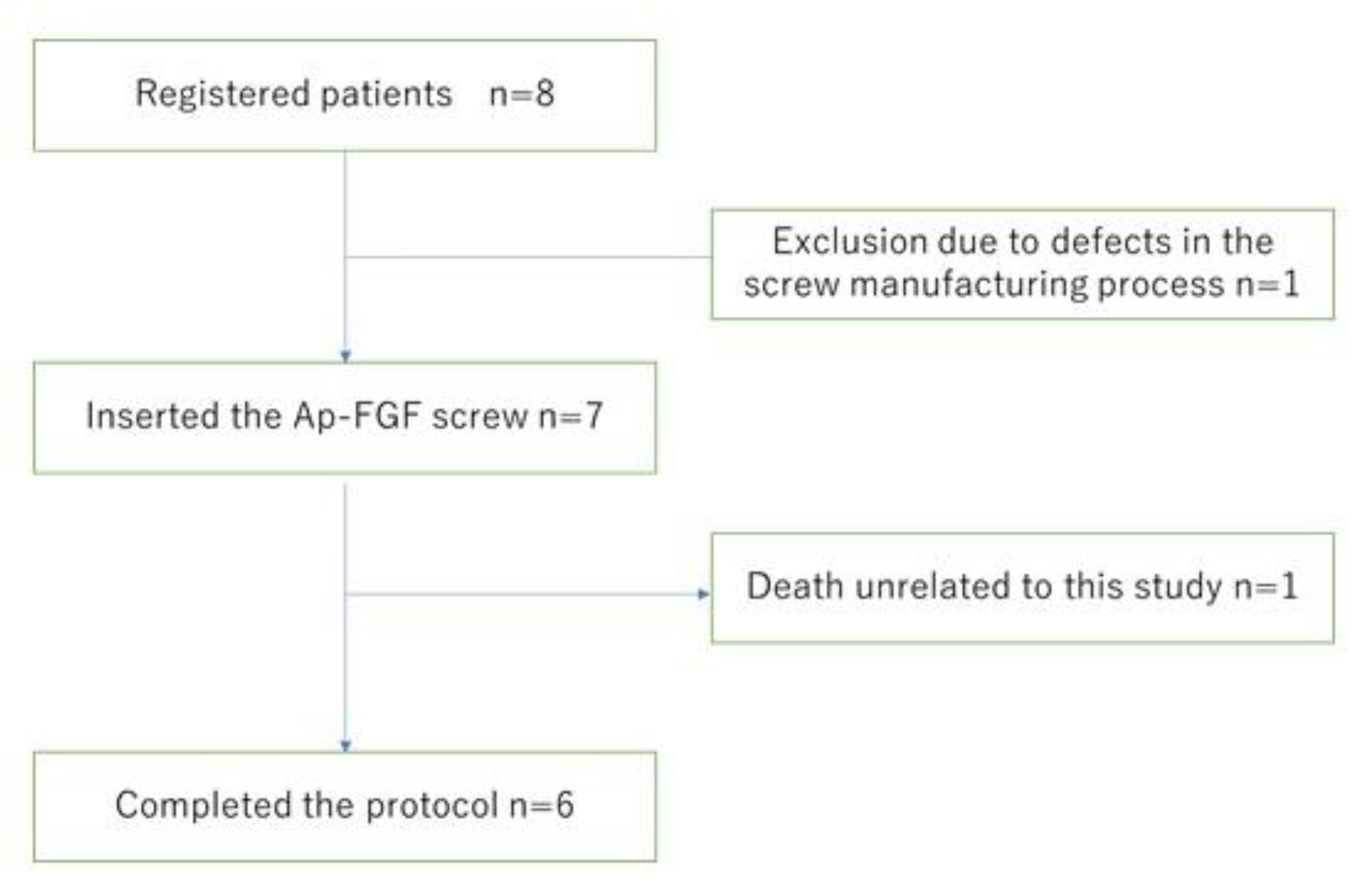
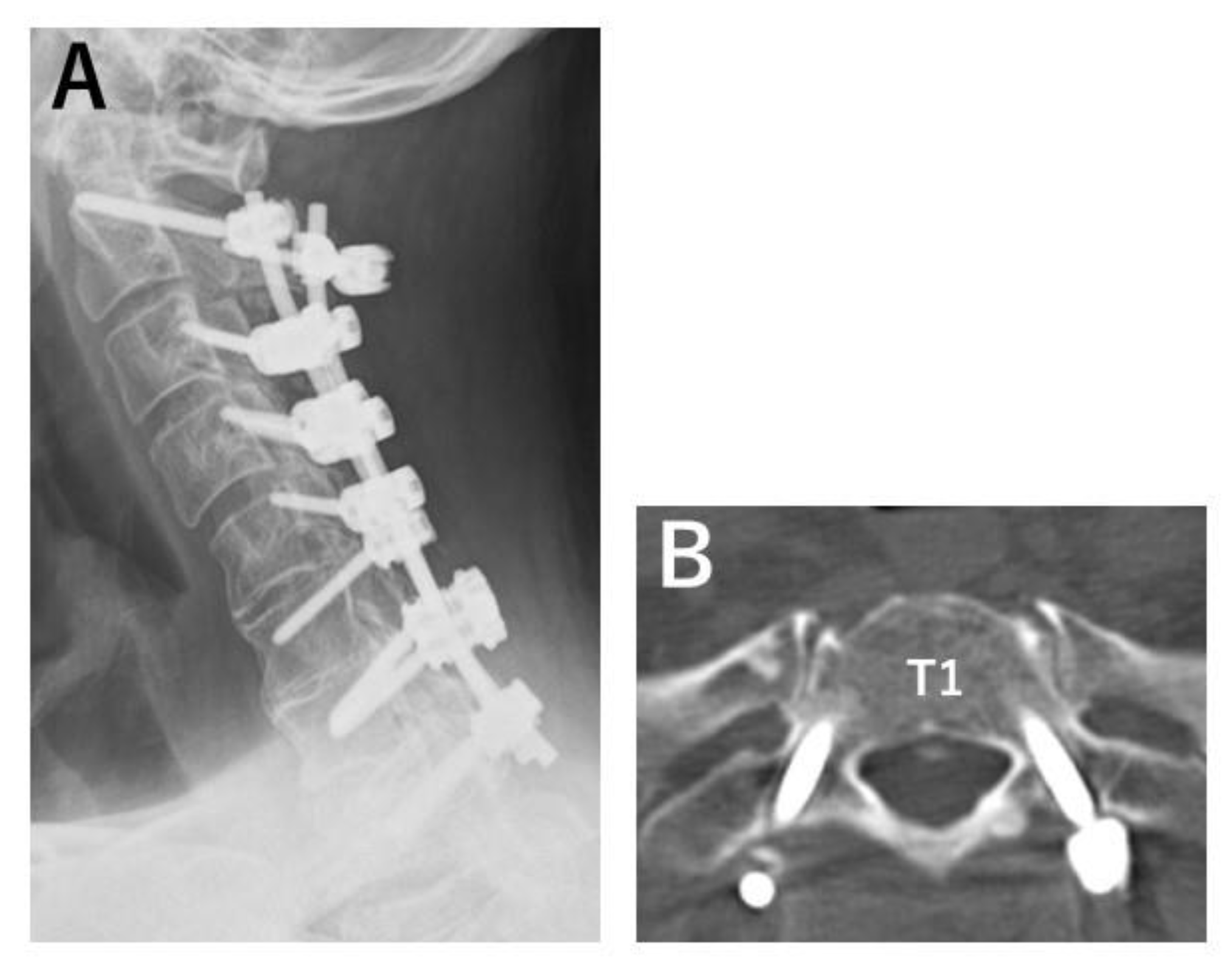
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Karczewski, D.; Pumberger, M.; Müller, M.; Andronic, O.; Perka, C.; Winkler, T. Implications for diagnosis and treatment of peri-spinal implant infections from experiences in periprosthetic joint infections-a literature comparison and review. J. Spine Surg. 2020, 6, 800–813. [Google Scholar] [CrossRef] [PubMed]
- Prinz, V.; Vajkoczy, P. Surgical revision strategies for postoperative spinal implant infections (PSII). J. Spine Surg. 2020, 6, 777–784. [Google Scholar] [CrossRef] [PubMed]
- Daldal, I.; Senkoylu, A. Strategies of management of deep spinal infection: From irrigation and debridement to vacuum-assisted closure treatment. Ann. Transl. Med. 2020, 8, 33. [Google Scholar] [CrossRef] [PubMed]
- Peng, C.W.; Chou, B.T.; Bendo, J.A.; Spivak, J.M. Vertebral artery injury in cervical spine surgery: Anatomical considerations, management, and preventive measures. Spine J. 2009, 9, 70–76. [Google Scholar] [CrossRef]
- Hicks, J.M.; Singla, A.; Shen, F.H.; Arlet, V. Complications of pedicle screw fixation in scoliosis surgery: A systematic review. Spine 2010, 35, E465–E470. [Google Scholar] [CrossRef]
- Lall, R.; Patel, N.J.; Resnick, D.K. A review of complications associated with craniocervical fusion surgery. Neurosurgery 2010, 67, 1396–1402, discussion 1402–1403. [Google Scholar] [CrossRef]
- Elliott, R.E.; Tanweer, O.; Boah, A.; Morsi, A.; Ma, T.; Frempong-Boadu, A.; Smith, M.L. Comparison of screw malposition and vertebral artery injury of C2 pedicle and transarticular screws: Meta-analysis and review of the literature. J. Spinal Disord. Tech. 2014, 27, 305–315. [Google Scholar] [CrossRef]
- Hitchon, P.W.; Moritani, T.; Woodroffe, R.W.; Abode-Iyamah, K.; El Tecle, N.E.; Noeller, J.; Elwy, R.K.; Nourski, K.V. C5 palsy following posterior decompression and instrumentation in cervical stenosis: Single center experience and review. Clin. Neurol. Neurosurg. 2018, 174, 29–35. [Google Scholar] [CrossRef]
- Young, P.M.; Berquist, T.H.; Bancroft, L.W.; Peterson, J.J. Complications of spinal instrumentation. Radiographics 2007, 27, 775–789. [Google Scholar] [CrossRef]
- Rankine, J.J. The postoperative spine. Semin. Musculoskelet. Radiol. 2014, 18, 300–308. [Google Scholar] [CrossRef]
- Marie-Hardy, L.; Pascal-Moussellard, H.; Barnaba, A.; Bonaccorsi, R.; Scemama, C. Screw loosening in posterior spine fusion: Prevalence and risk factors. Glob. Spine J. 2020, 10, 598–602. [Google Scholar] [CrossRef] [Green Version]
- Verla, T.; Xu, D.S.; Davis, M.J.; Reece, E.M.; Kelly, M.; Nunez, M.; Winocour, S.J.; Ropper, A.E. Failure in cervical spinal fusion and current management modalities. Semin. Plast. Surg. 2021, 35, 10–13. [Google Scholar] [CrossRef] [PubMed]
- Rometsch, E.; Spruit, M.; Zigler, J.E.; Menon, V.K.; Ouellet, J.A.; Mazel, C.; Härtl, R.; Espinoza, K.; Kandziora, F. Screw-related complications after instrumentation of the osteoporotic spine: A systematic literature review with meta-analysis. Glob. Spine J. 2020, 10, 69–88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karakaşlı, A.; Sekik, E.; Karaarslan, A.; Kızmazoğlu, C.; Havıtçıoğlu, H. Are pedicular screws and lateral hook screws more resistant against pullout than conventional spinal hooks and screws in terminal vertebral segment fixation? Eklem Hastalik. Cerrahisi 2016, 27, 22–28. [Google Scholar] [CrossRef]
- Matsukawa, K.; Yato, Y.; Kato, T.; Imabayashi, H.; Asazuma, T.; Nemoto, K. Cortical bone trajectory for lumbosacral fixation: Penetrating S-1 endplate screw technique: Technical note. J. Neurosurg. Spine 2014, 21, 203–209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giavaresi, G.; Fini, M.; Giardino, R.; Salamanna, F.; Sartori, M.; Borsari, V.; Spriano, S.; Bellini, C.M.; Brayda-Bruno, M. In vivo preclinical evaluation of the influence of osteoporosis on the anchorage of different pedicle screw designs. Eur. Spine J. 2011, 20, 1289–1296. [Google Scholar] [CrossRef] [Green Version]
- Bokov, A.; Pavlova, S.; Bulkin, A.; Aleynik, A.; Mlyavykh, S. Potential contribution of pedicle screw design to loosening rate in patients with degenerative diseases of the lumbar spine: An observational study. World J. Orthop. 2021, 12, 310–319. [Google Scholar] [CrossRef]
- Liu, M.Y.; Tsai, T.T.; Lai, P.L.; Hsieh, M.K.; Chen, L.H.; Tai, C.L. Biomechanical comparison of pedicle screw fixation strength in synthetic bones: Effects of screw shape, core/thread profile and cement augmentation. PLoS ONE 2020, 15, e0229328. [Google Scholar] [CrossRef] [PubMed]
- Ehresman, J.; Pennington, Z.; Elsamadicy, A.A.; Hersh, A.; Lubelski, D.; Lehner, K.; Cottrill, E.; Schilling, A.; Lakomkin, N.; Ahmed, A.K.; et al. Fenestrated pedicle screws for thoracolumbar instrumentation in patients with poor bone quality: Case series and systematic review of the literature. Clin. Neurol. Neurosurg. 2021, 206, 106675. [Google Scholar] [CrossRef]
- Upasani, V.V.; Farnsworth, C.L.; Tomlinson, T.; Chambers, R.C.; Tsutsui, S.; Slivka, M.A.; Mahar, A.T.; Newton, P.O. Pedicle screw surface coatings improve fixation in nonfusion spinal constructs. Spine 2009, 34, 335–343. [Google Scholar] [CrossRef]
- Ohe, M.; Moridaira, H.; Inami, S.; Takeuchi, D.; Nohara, Y.; Taneichi, H. Pedicle screws with a thin hydroxyapatite coating for improving fixation at the bone-implant interface in the osteoporotic spine: Experimental study in a porcine model. J. Neurosurg. Spine 2018, 28, 679–687. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Ito, A.; Li, X.; Sogo, Y.; Oyane, A. Signal molecules–calcium phosphate coprecipitation and its biomedical application as a functional coating. Biofabrication 2011, 3, 022001. [Google Scholar] [CrossRef] [PubMed]
- Mutsuzaki, H.; Ito, A.; Sakane, M.; Sogo, Y.; Oyane, A.; Ebihara, Y.; Ichinose, N.; Ochiai, N. Calcium phosphate coating formed in infusion fluid mixture to enhance fixation strength of titanium screws. J. Mater. Sci. Mater. Med. 2007, 18, 1799–1808. [Google Scholar] [CrossRef] [PubMed]
- Mutsuzaki, H.; Ito, A.; Sogo, Y.; Sakane, M.; Oyane, A.; Ochiai, N. Enhanced wound healing associated with Sharpey’s fiber-like tissue formation around FGF-2-apatite composite layers on percutaneous titanium screws in rabbits. Arch. Orthop. Trauma Surg. 2012, 132, 113–121. [Google Scholar] [CrossRef] [Green Version]
- Fujii, K.; Ito, A.; Mutsuzaki, H.; Murai, S.; Sogo, Y.; Hara, Y.; Yamazaki, M. Reducing the risk of impaired bone apposition to titanium screws with the use of fibroblast growth factor-2-apatite composite layer coating. J. Orthop. Surg. Res. 2017, 12, 1. [Google Scholar] [CrossRef] [Green Version]
- Mutsuzaki, H.; Ito, A.; Sakane, M.; Sogo, Y.; Oyane, A.; Ochiai, N. Fibroblast growth factor-2-apatite composite layers on titanium screw to reduce pin tract infection rate. J. Biomed. Mater. Res. B Appl. Biomater. 2008, 86, 365–374. [Google Scholar] [CrossRef]
- Imagama, S.; Ogino, R.; Ueno, S.; Murayama, N.; Takemoto, N.; Shimmyo, Y.; Kadoshima, T.; Tamura, S.; Kuroda, M.; Matsuyama, Y.; et al. Systemic treatment with a novel basic fibroblast growth factor mimic small-molecule compound boosts functional recovery after spinal cord injury. PLoS ONE 2020, 15, e0236050. [Google Scholar] [CrossRef]
- Paciaroni, M.; Bogousslavsky, J. Trafermin for stroke recovery: Is it time for another randomized clinical trial? Expert Opin. Biol. Ther. 2011, 11, 1533–1541. [Google Scholar] [CrossRef]
- Nagashima, K.; Koda, M.; Abe, T.; Kumagai, H.; Miura, K.; Fujii, K.; Noguchi, H.; Funayama, T.; Miyamoto, T.; Mannoji, C.; et al. Implant failure of pedicle screws in long-segment posterior cervical fusion is likely to occur at C7 and is avoidable by concomitant C6 or T1 buttress pedicle screws. J. Clin. Neurosci. 2019, 63, 106–109. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Inclusion criteria
|
Exclusion criteria
|
| Pt. No. | Age | Sex | Main Disease | Comorbidities |
|---|---|---|---|---|
| 1 | 59 | M | OPLL | DM |
| 2 | 61 | M | OPLL | |
| 3 | 61 | M | OPLL | DM |
| 4 | 64 | M | CSM | RA |
| 5 | 52 | M | OPLL | DM, HT, HL |
| 6 | 74 | M | OPLL | CKD, HT |
| 7 | 48 | M | CSM | dystonia |
| 8 | 58 | M | OPLL | Liver dysfunction |
| Adverse Events (AE) | No. of Patients | Note |
|---|---|---|
| Severe AE | ||
| Death | 1 | rapture of AAA |
| AE | ||
| Laboratory data abnormalities | ||
| CPK elevation | 7 | |
| Liver dysfunction | 4 | |
| Amylase elevation | 1 | |
| Neurological | ||
| C5 palsy | 1 | recovered |
| Others | ||
| Urticaria | 1 | |
| Pneumonia | 1 | |
| Gonitis purulenta | 1 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nagashima, K.; Hara, Y.; Mutsuzaki, H.; Totoki, Y.; Okano, E.; Mataki, K.; Matsumoto, Y.; Yanagisawa, Y.; Noguchi, H.; Sogo, Y.; et al. Clinical Trial for the Safety and Feasibility of Pedicle Screws Coated with a Fibroblast Growth Factor-2-Apatite Composite Layer for Posterior Cervical Fusion Surgery. J. Clin. Med. 2023, 12, 947. https://doi.org/10.3390/jcm12030947
Nagashima K, Hara Y, Mutsuzaki H, Totoki Y, Okano E, Mataki K, Matsumoto Y, Yanagisawa Y, Noguchi H, Sogo Y, et al. Clinical Trial for the Safety and Feasibility of Pedicle Screws Coated with a Fibroblast Growth Factor-2-Apatite Composite Layer for Posterior Cervical Fusion Surgery. Journal of Clinical Medicine. 2023; 12(3):947. https://doi.org/10.3390/jcm12030947
Chicago/Turabian StyleNagashima, Katsuya, Yuki Hara, Hirotaka Mutsuzaki, Yasukazu Totoki, Eriko Okano, Kentaro Mataki, Yukei Matsumoto, Yohei Yanagisawa, Hiroshi Noguchi, Yu Sogo, and et al. 2023. "Clinical Trial for the Safety and Feasibility of Pedicle Screws Coated with a Fibroblast Growth Factor-2-Apatite Composite Layer for Posterior Cervical Fusion Surgery" Journal of Clinical Medicine 12, no. 3: 947. https://doi.org/10.3390/jcm12030947