
Soft-Tissue Augmentation around Dental Implants with a Connective Tissue Graft (CTG) and Xenogeneic Collagen Matrix (CMX)—5-Year Follow-Up


Abstract
:1. Introduction
- The augmentation procedure of gingiva does not improve the thickness of the soft tissues in the aesthetic area in a 5-year observation.
- The non-inferiority of the Geistlich Mucograft (Geistlich Pharma AG, Wolhusen, Switzerland) to the connective tissue graft in a gingiva augmentation procedure in a 5-year observation.
2. Materials and Methods
2.1. Study Design
Patients Randomization
- (a)
- G2a: CMX before Geistlich Mucograft, 15 implants in 13 patients (11 patients with single, 2 patients with double implants);
- (b)
- G2b: CTG before a connective tissue graft from the palate (CTG); 15 implants in 14 patients (13 patients with single and 1 patient with double implants).
- (a)
- G3a: CMX after Geistlich Mucograft; 15 implants in 12 patients (9 patients with single, 3 patients with double implants)
- (b)
- G3b: CTG with a connective tissue graft from the palate (CTG); 15 implants in 13 patients (11 patients with single, 2 patients with double implants).
2.2. Inclusion and Exclusion Criteria
- missing single or double teeth in the anterior area of their upper or lower jaw, with a proper interarch relationship (incisors, canines and first premolar), ridge width (bucco–lingual) greater than 5 mm at its narrowest point and minimum height of keratinized gingiva of 2 mm buccally;
- no previous soft-tissue augmentation procedure at the experimental site.
- implants placed with an insertion torque of 35 Ncm or less;
- irradiation in the head and neck area; untreated periodontitis;
- poor oral hygiene (plaque score API 20%, bleeding score 10%);
- poor motivation;
- fresh post-extraction sockets.
2.3. Surgical Procedures
2.4. Measurement of Marginal Bone Loss (MBL)
2.5. Soft-Tissue Measurement
2.6. Clinical Outcome
2.7. Follow-Up
2.8. Primary and Secondary Endpoints
2.9. Statistical Analysis
3. Results
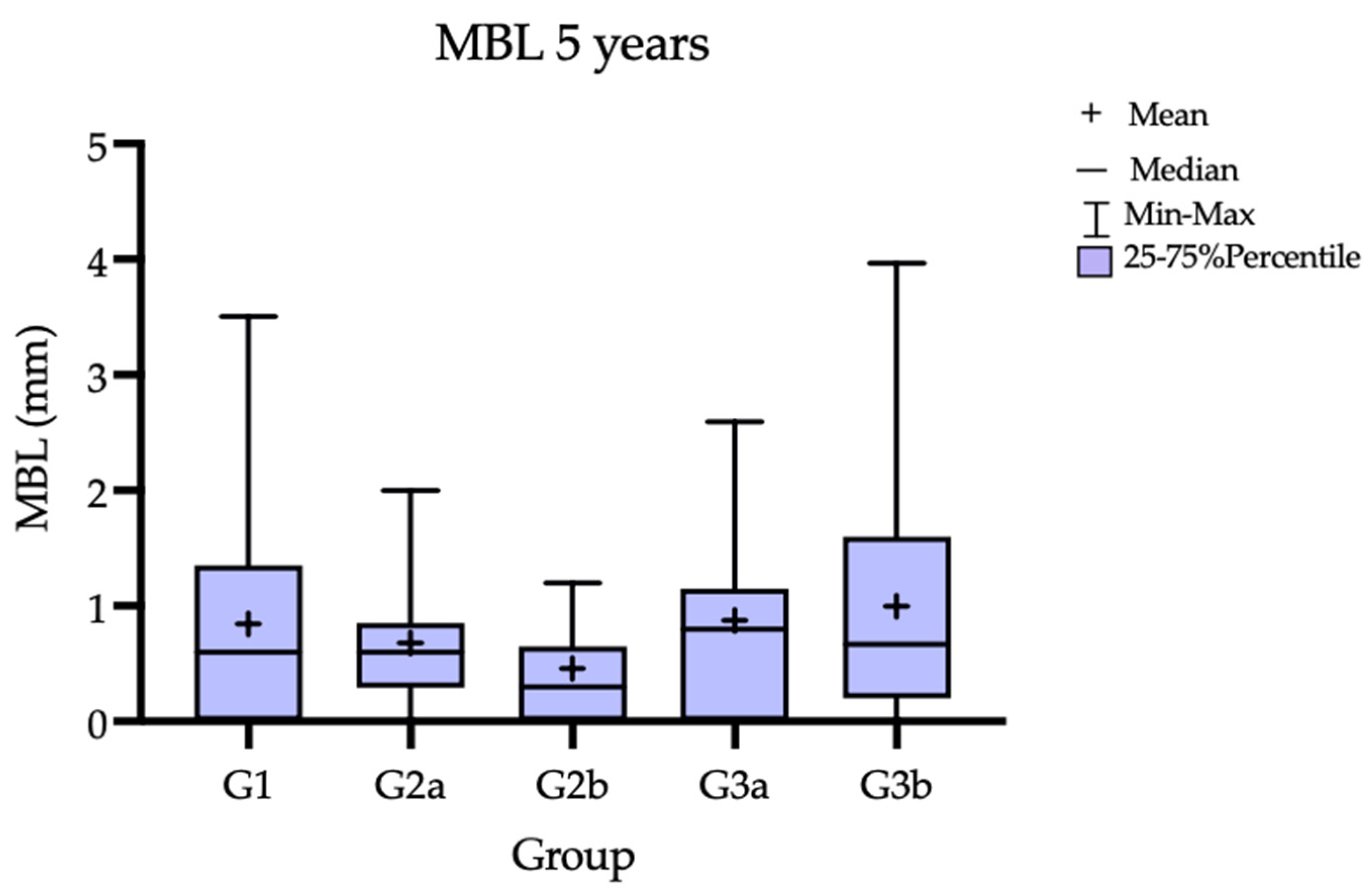
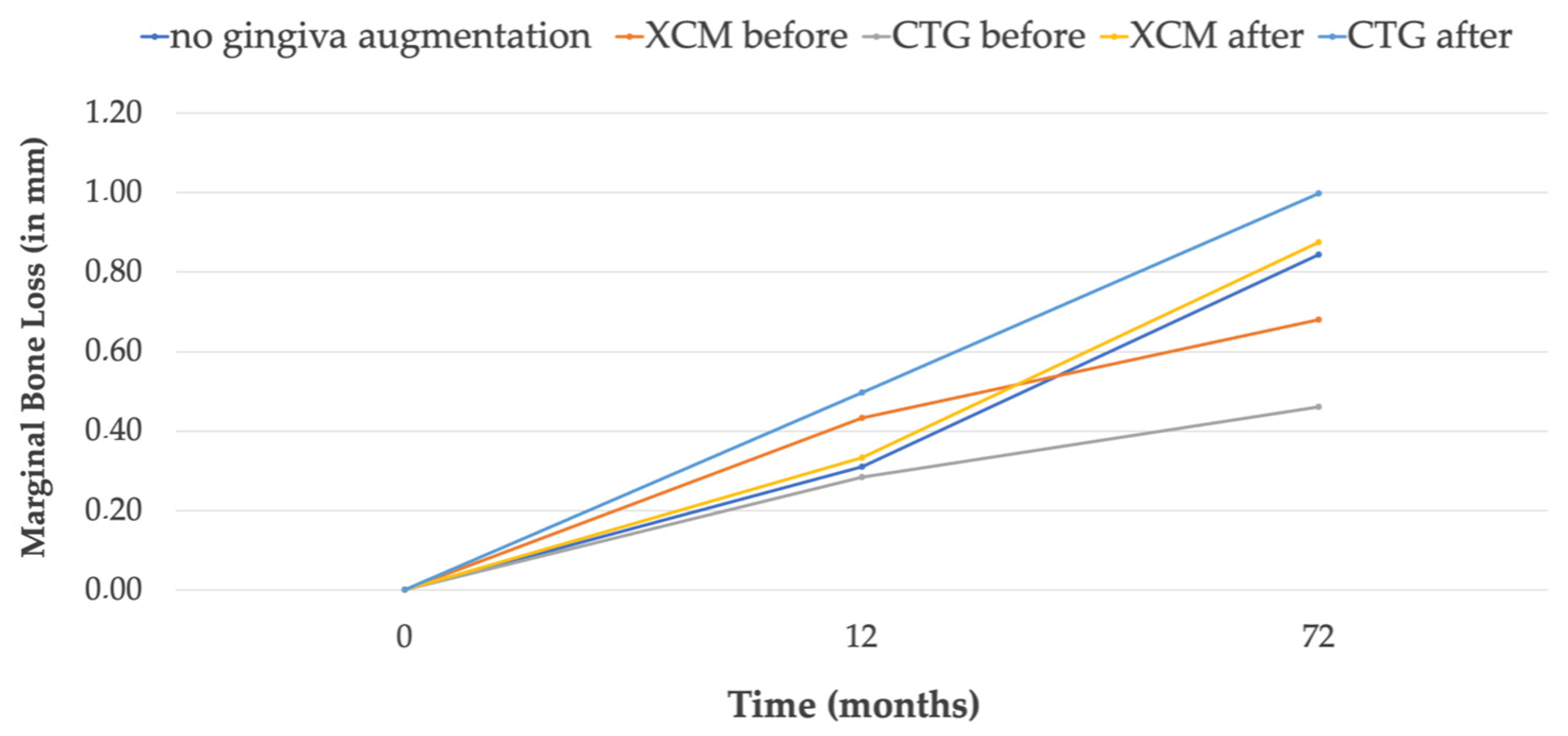
3.1. Marginal Bone Loss
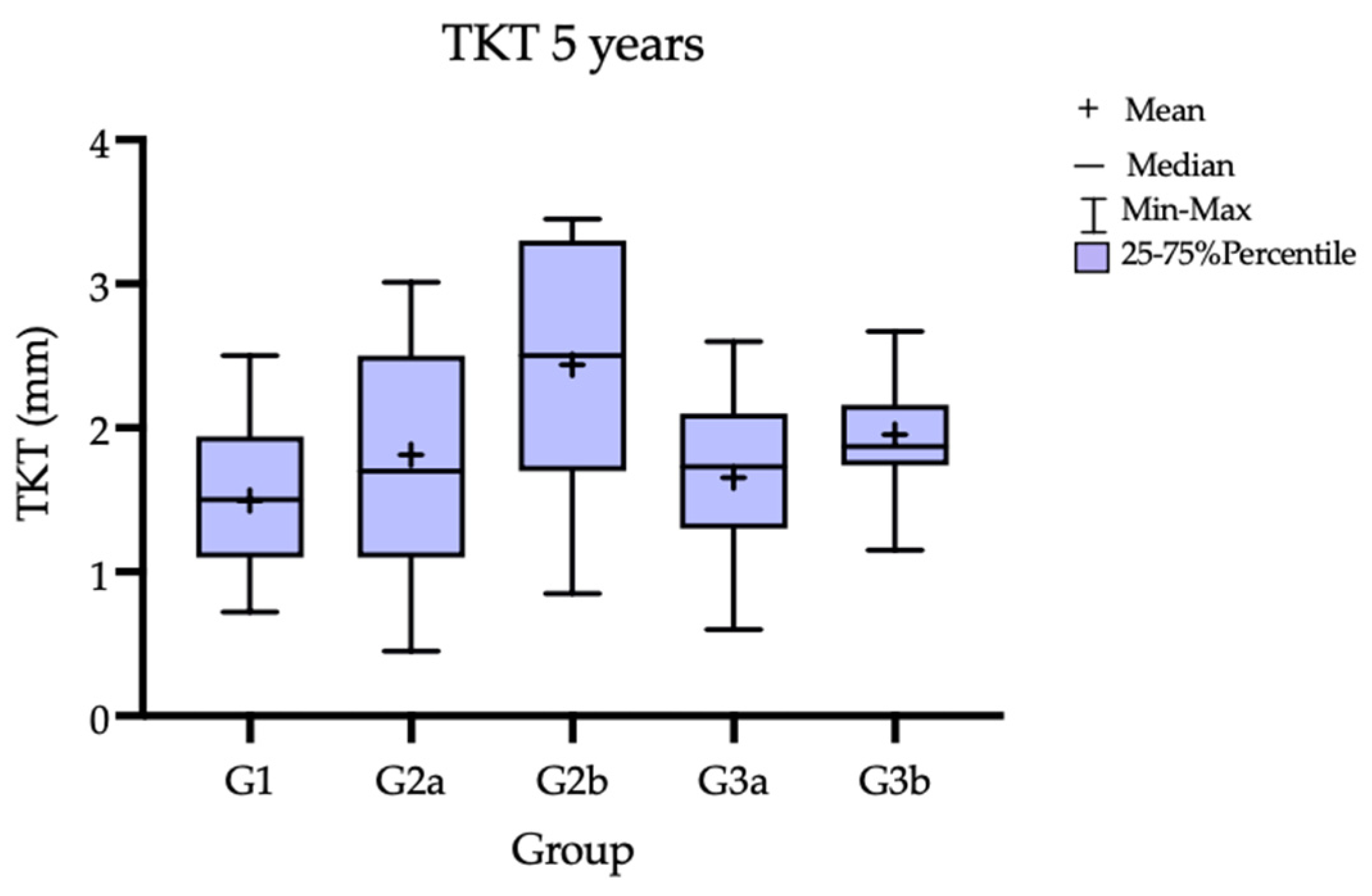
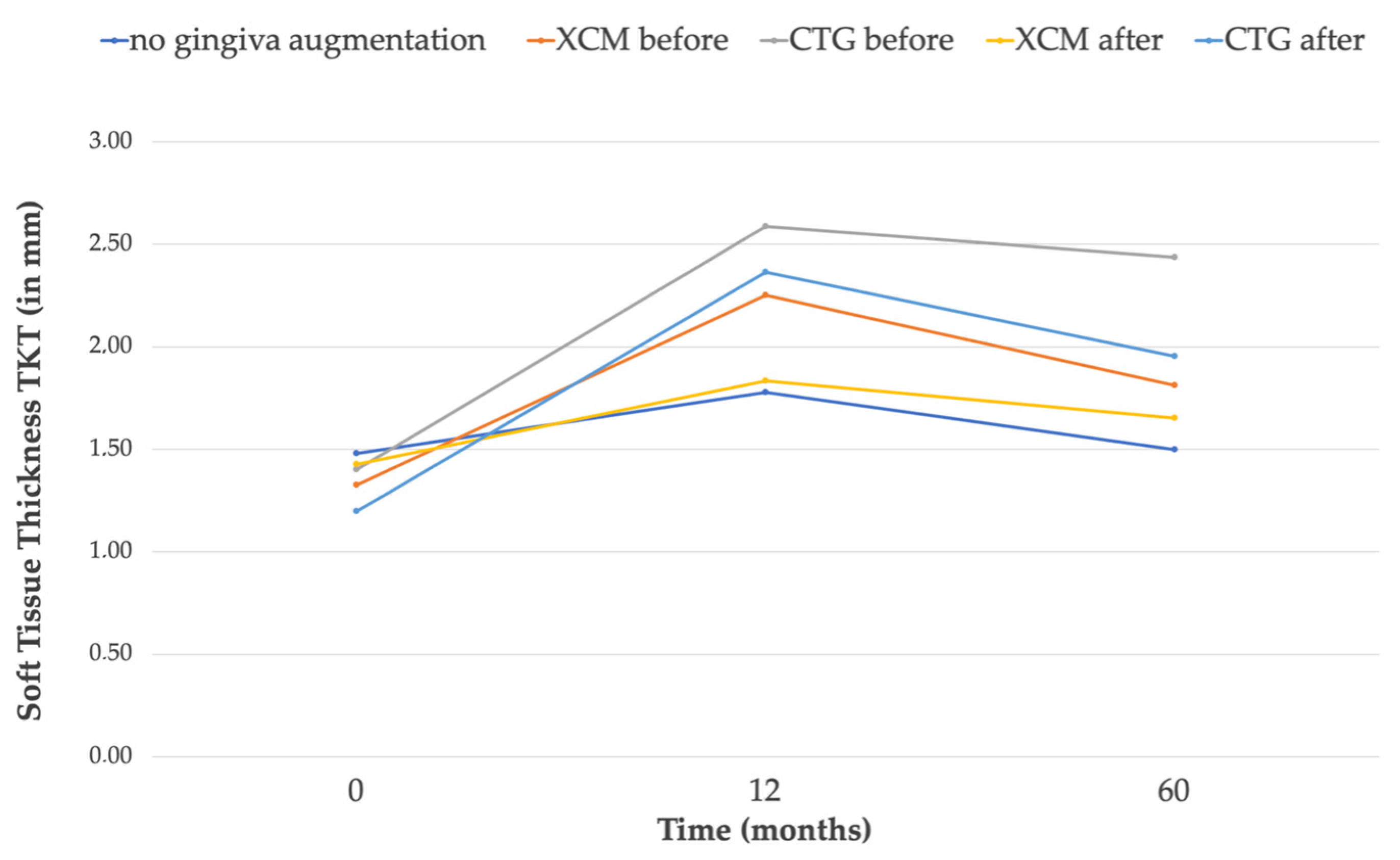
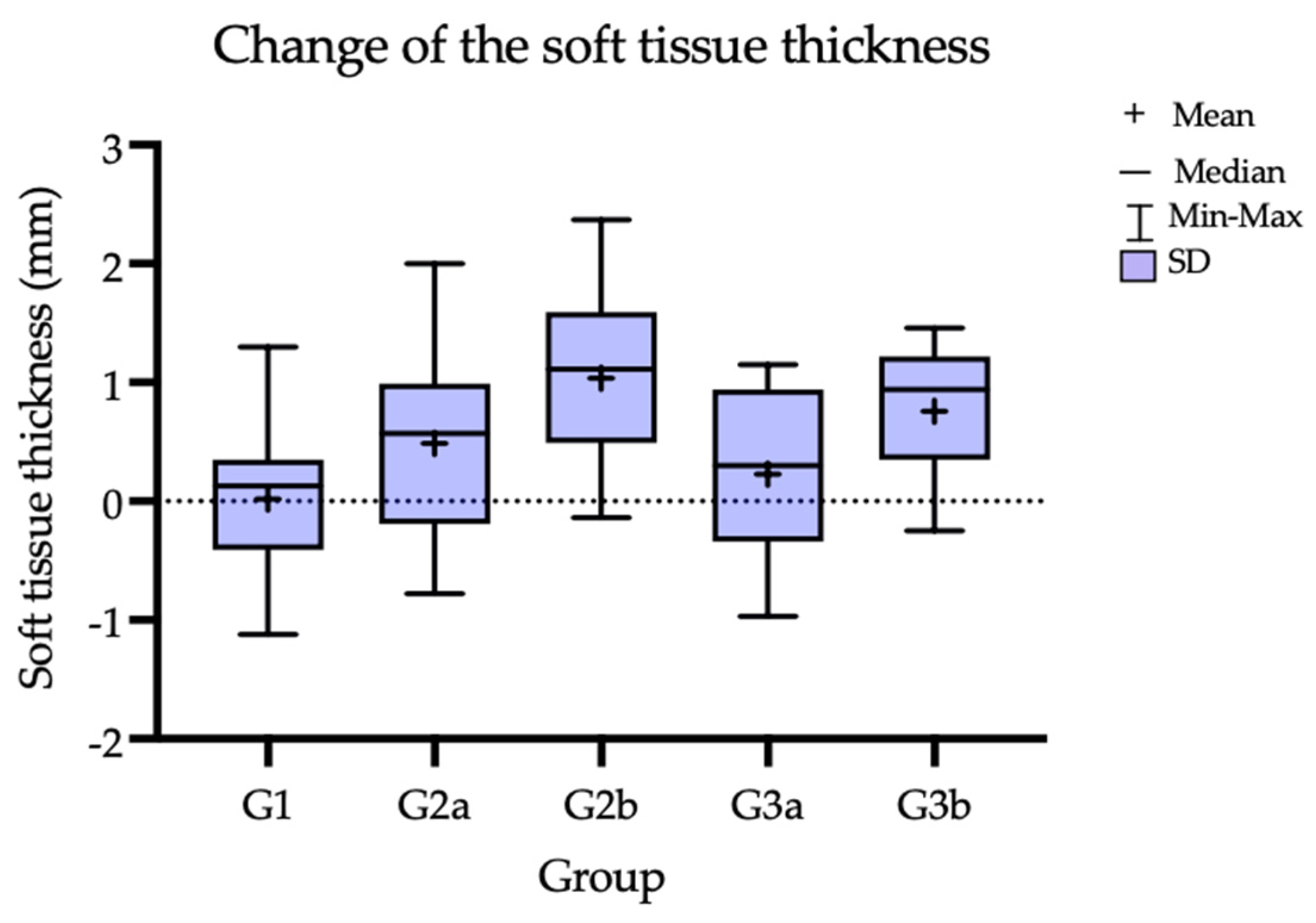
3.2. Soft-Tissue Volume
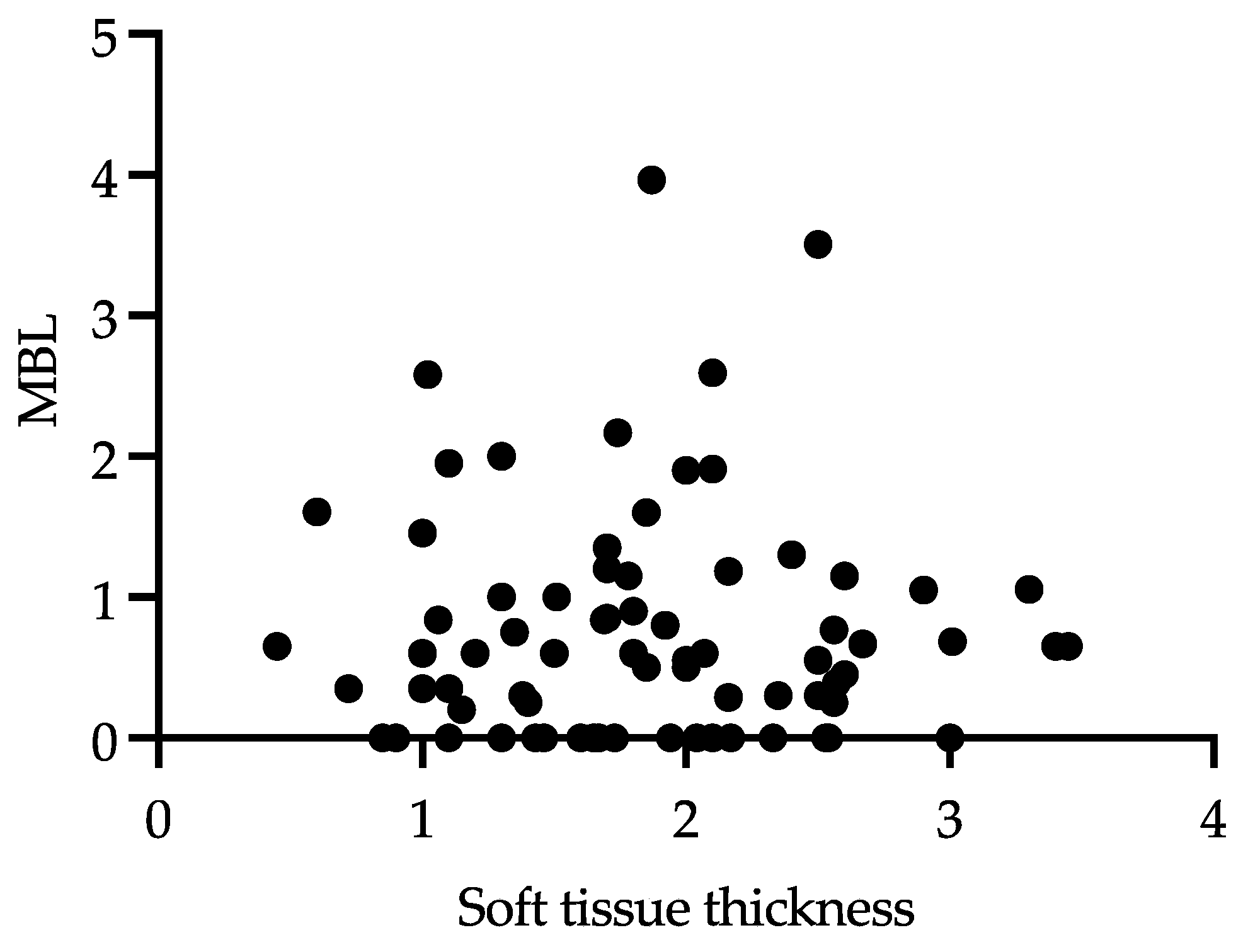
3.3. Correlation between MBL and Keratinized Soft-Tissue Thickness TKT
3.4. Clinical Outcomes
4. Discussion
- The first research hypothesis was rejected. In all the groups, a nominal gain of tissue thickness was observed comparing the baseline to 5 Y post-operation. Statistically significant differences in soft-tissue thickness gain were found between G1 vs. G2b (no gingival augmentation vs. CTG before), G1 vs. G3b (no augmentation vs. CTG after) and for G2b vs. G3a (CTG before vs. CMX after).
- The second hypothesis of the non-inferiority of the Geistlich Mucograft compared to the connective tissue grafts in the augmentation gingiva could not be verified. Although the CMX material showed good results in comparison to the control, a statistically significant difference to the CTG, in terms of thickness gain, was observed, with the CTG being superior. When comparing the baseline to the 5 Y thickness, the results were ranked in order of the smallest to the largest tissue gain: no augmentation (0.018 mm) < CMX after (0.226 mm) < CMX before (0.486 mm) < CTG after (0.76 mm) < CTG before (1.035 mm).
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Linkevicius, T.; Apse, P.; Grybauskas, S.; Puisys, A. The influence of soft tissue thickness on crestal bone changes around implants: A 1-year prospective controlled clinical trial. Int. J. Oral Maxillofac. Implant. 2009, 24, 712–719. [Google Scholar]
- Bhat, P.; Thakur, S.; Kulkarni, S. The influence of soft tissue biotype on the marginal bone changes around dental implants: A 1-year prospective clinico-radiological study. J. Indian Soc. Periodontol. 2015, 19, 640–644. [Google Scholar] [CrossRef]
- Lissek, M.; Boeker, M.; Happe, A. How thick is the oral mucosa around implants after augmentation with different materials: A systematic review of the effectiveness of substitute matrices in comparison to connective tissue grafts. Int. J. Mol. Sci. 2020, 21, 5043. [Google Scholar] [CrossRef] [PubMed]
- Scharf, D.R.; Tarnow, D.P. Modified roll technique for localized alveolar ridge augmentation. Int. J. Periodontics Restor. Dent. 1992, 12, 415–425. [Google Scholar] [CrossRef]
- Langer, B.; Calagna, L. The subepithelial connective tissue graft. J. Prosthet. Dent. 1980, 44, 363–367. [Google Scholar] [CrossRef] [PubMed]
- Puzio, M.; Hadzik, J.; Błaszczyszyn, A.; Gedrange, T.; Dominiak, M. Soft tissue augmentation around dental implants with connective tissue graft (CTG) and xenogenic collagen matrix (XCM). 1-year randomized control trail. Ann. Anat. 2020, 230, 151484. [Google Scholar] [CrossRef]
- Puzio, M.; Błaszczyszyn, A.; Hadzik, J.; Dominiak, M. Ultrasound assessment of soft tissue augmentation around implants in the aesthetic zone using a connective tissue graft and xenogeneic collagen matrix—1-year randomised follow-up. Ann. Anat. 2018, 217, 129–141. [Google Scholar] [CrossRef] [PubMed]
- Derks, J.; Schaller, D.; Håkansson, J.; Wennström, J.L.; Tomasi, C.; Berglundh, T. Peri-implantitis—Onset and pattern of progression. J. Clin. Periodontol. 2016, 43, 383–388. [Google Scholar] [CrossRef]
- Agudio, G.; Chambrone, L.; Selvaggi, F.; Pini-Prato, G.P. Effect of gingival augmentation procedure (free gingival graft) on reducing the risk of non-carious cervical lesions: A 25- to 30-year follow-up study. J. Periodontol. 2019, 90, 1235–1243. [Google Scholar] [CrossRef]
- Bertl, K.; Spineli, L.M.; Mohandis, K.; Stavropoulos, A. Root coverage stability: A systematic overview of controlled clinical trials with at least 5 years of follow-up. Clin. Exp. Dent. Res. 2021, 7, 692–710. [Google Scholar] [CrossRef]
- Heitz-Mayfield, L.J.A. Peri-implant diseases: Diagnosis and risk indicators. J. Clin. Periodontol. 2008, 35, 292–304. [Google Scholar] [CrossRef]
- Hadzik, J.; Botzenhart, U.; Krawiec, M.; Gedrange, T.; Heinemann, F.; Vegh, A.; Dominiak, M. Comparative evaluation of the effectiveness of the implantation in the lateral part of the mandible between short tissue level (TE) and bone level (BL) implant systems. Ann. Anat. 2017, 213, 78–82. [Google Scholar] [CrossRef] [PubMed]
- Bassetti, R.G.; Stähli, A.; Bassetti, M.A.; Sculean, A. Soft tissue augmentation procedures at second-stage surgery: A systematic review. Clin. Oral Investig. 2016, 20, 1369–1387. [Google Scholar] [CrossRef] [PubMed]
- Lindhe, J.; Meyle, J. Peri-implant diseases: Consensus Report of the Sixth European Workshop on Periodontology. J. Clin. Periodontol. 2008, 35, 282–285. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Souza, A.B.; Tormena, M.; Matarazzo, F.; Araújo, M.G. The influence of peri-implant keratinized mucosa on brushing discomfort and peri-implant tissue health. Clin. Oral Implant. Res. 2016, 27, 650–655. [Google Scholar] [CrossRef]
- Moraschini, V.; Luz, D.; Velloso, G.; Barboza, E.d.S.P. Quality assessment of systematic reviews of the significance of keratinized mucosa on implant health. Int. J. Oral Maxillofac. Surg. 2017, 46, 774–781. [Google Scholar] [CrossRef]
- Hadzik, J.; Kubasiewicz-Ross, P.; Nawrot-Hadzik, I.; Gedrange, T.; Pitułaj, A.; Dominiak, M. Short (6 mm) and Regular Dental Implants in the Posterior Maxilla-7-Years Follow-up Study. J. Clin. Med. 2021, 10, 940. [Google Scholar] [CrossRef]
- Santamaria, M.P.; Rossato, A.; Miguel, M.M.V.; Fonseca, M.B.; Bautista, C.R.G.; de Marco, A.C.; Mathias-Santamaria, I.F.; Ferreira Ferraz, L.F. Comparison of two types of xenogeneic matrices to treat single gingival recessions: A randomized clinical trial. J. Periodontol. 2022, 93, 709–720. [Google Scholar] [CrossRef]
- Huang, J.P.; Liu, J.M.; Wu, Y.M.; Dai, A.; Hu, H.J.; He, F.M.; Chen, Q.M.; Li, X.J.; Sun, P.; Ding, P.H. Clinical evaluation of xenogeneic collagen matrix versus free gingival grafts for keratinized mucosa augmentation around dental implants: A randomized controlled clinical trial. J. Clin. Periodontol. 2021, 48, 1293–1301. [Google Scholar] [CrossRef]
- Moraschini, V.; Guimarães, H.B.; Cavalcante, I.C.; Calasans-Maia, M.D. Clinical efficacy of xenogeneic collagen matrix in augmenting keratinized mucosa round dental implants: A systematic review and meta-analysis. Clin. Oral Investig. 2020, 24, 2163–2174. [Google Scholar] [CrossRef]
- Schmitt, C.M.; Moest, T.; Lutz, R.; Wehrhan, F.; Neukam, F.W.; Schlegel, K.A. Long-term outcomes after vestibuloplasty with a porcine collagen matrix (Mucograft®) versus the free gingival graft: A comparative prospective clinical trial. Clin. Oral Implant. Res. 2016, 27, e125–e133. [Google Scholar] [CrossRef] [PubMed]
- Galindo-Moreno, P.; León-Cano, A.; Ortega-Oller, I.; Monje, A.; O’valle, F.; Catena, A. Marginal bone loss as success criterion in implant dentistry: Beyond 2 mm. Clin. Oral Implant. Res. 2015, 26, e28–e34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Di Gianfilippo, R.; Valente, N.A.; Toti, P.; Wang, H.L.; Barone, A. Influence of implant mucosal thickness on early bone loss: A systematic review with meta-analysis. J. Periodontal Implant. Sci. 2020, 50, 209–225. [Google Scholar] [CrossRef] [PubMed]
- Wittneben, J.G.; Joda, T.; Weber, H.P.; Brägger, U. Screw retained vs. cement retained implant-supported fixed dental prosthesis. Periodontol. 2000 2017, 73, 141–151. [Google Scholar] [CrossRef]
- Sailer, I.; Mühlemann, S.; Zwahlen, M.; Hämmerle, C.H.F.; Schneider, D. Cemented and screw-retained implant reconstructions: A systematic review of the survival and complication rates. Clin. Oral Implant. Res. 2012, 23 (Suppl. S6), 163–201. [Google Scholar] [CrossRef]
- Fu, J.H.; Wang, H.L. Breaking the wave of peri-implantitis. Periodontol. 2000 2020, 84, 145–160. [Google Scholar] [CrossRef]
- Krawiec, M.; Olchowy, C.; Kubasiewicz-Ross, P.; Hadzik, J.; Dominiak, M. Role of implant loading time in the prevention of marginal bone loss after implant-supported restorations: A targeted review. Dent. Med. Probl. 2022, 59, 475–481. [Google Scholar] [CrossRef]
- Strauss, F.J.; Hämmerle, C.H.F.; Thoma, D.S. Short communication: Cemented implant reconstructions are associated with less marginal bone loss than screw-retained reconstructions at 3 and 5 years of loading. Clin. Oral Implant. Res. 2021, 32, 651–656. [Google Scholar] [CrossRef]
- Suárez-López del Amo, F.; Lin, G.-H.; Monje, A.; Galindo-Moreno, P.; Wang, H.-L. Influence of Soft Tissue Thickness on Peri-Implant Marginal Bone Loss: A Systematic Review and Meta-Analysis. J. Periodontol. 2016, 87, 690–699. [Google Scholar] [CrossRef]
- Puisys, A.; Linkevicius, T. The influence of mucosal tissue thickening on crestal bone stability around bone-level implants. A prospective controlled clinical trial. Clin. Oral Implant. Res. 2015, 26, 123–129. [Google Scholar] [CrossRef]
- Wiesner, G.; Esposito, M.; Worthington, H.; Schlee, M. Connective tissue grafts for thickening peri-implant tissues at implant placement. One-year results from an explanatory split-mouth randomised controlled clinical trial. Eur. J. Oral Implantol. 2010, 3, 27–35. [Google Scholar] [PubMed]
- Jepsen, S.; Berglundh, T.; Genco, R.; Aass, A.M.; Demirel, K.; Derks, J.; Figuero, E.; Giovannoli, J.L.; Goldstein, M.; Lambert, F.; et al. Primary prevention of peri-implantitis: Managing peri-implant mucositis. J. Clin. Periodontol. 2015, 42 (Suppl. S16), S152–S157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hadzik, J.; Kubasiewicz-Ross, P.; Gębarowski, T.; Waloszczyk, N.; Maciej, A.; Stolarczyk, A.; Gedrange, T.; Dominiak, M.; Szajna, E.; Simka, W. An Experimental Anodized Titanium Surface for Transgingival Dental Implant Elements—Preliminary Report. J. Funct. Biomater. 2023, 14, 34. [Google Scholar] [CrossRef] [PubMed]
- Kulakov, A.; Kogan, E.; Brailovskaya, T.; Vedyaeva, A.; Zharkov, N.; Krasilnikova, O.; Krasheninnikov, M.; Baranovskii, D.; Rasulov, T.; Klabukov, I. Mesenchymal stromal cells enhance vascularization and epithelialization within 7 days after gingival augmentation with collagen matrices in rabbits. Dent. J. 2021, 9, 101. [Google Scholar] [CrossRef]
- Fu, X.; Wang, Y.; Chen, B.; Tian, J.; Lin, Y.; Zhang, Y. Patient-reported outcome measures and clinical outcomes following peri-implant vestibuloplasty with a free gingival graft versus xenogeneic collagen matrix: A comparative prospective clinical study. Int. J. Implant Dent. 2021, 7, 69. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group Description | No Gingiva Augmentation | CMX Before | CTG Before | CMX After | CTG After | |
|---|---|---|---|---|---|---|
| Group | G1 | G2a | G2b | G3a | G3b | |
| MBL 5 years (in mm) | Min | 0 | 0 | 0 | 0 | 0 |
| Max | 3.5 | 2 | 1.2 | 2.6 | 3.7 | |
| Median: | 0.60 | 0.60 | 0.3 | 0.80 | 0.67 | |
| 25% Percentile: | 0 | 0.29 | 0 | 0 | 0.2 | |
| 75% Percentile: | 1.35 | 0.85 | 0.65 | 1.15 | 1.6 | |
| Range | 3.50 | 2.0 | 1.2 | 2.59 | 3.96 |
| Group Description | No Giginva Augmentation | CMX Before | CTG Before | CMX After | CTG After | |
|---|---|---|---|---|---|---|
| Group | G1 | G2a | G2b | G3a | G3b | |
| TKT (in mm) | Mean T0 | 1.48 | 1.326 | 1.4 | 1.426 | 1.2 |
| Mean 12 M | 1.776 | 2.25 | 2.587 | 1.835 | 2.36 | |
| Mean 60 M | 1.496 | 1.813 | 2.436 | 1.652 | 1.95 | |
| Mean change T0 vs. 60 M | 0.018 | 0.486 | 1.035 | 0.226 | 0.76 |
| Tukey’s Multiple Comparisons Test | Mean Diff. | 95.00% CI of Diff. | Significant | Summary | Adjusted p Value |
|---|---|---|---|---|---|
| G1 vs. G2a | −0.3167 | −0.9843 to 0.3510 | No | ns | 0.6697 |
| G1 vs. G2b | −0.94 | −1.608 to −0.2723 | Yes | ** | 0.0019 |
| G1 vs. G3a | −0.1560 | −0.8237 to 0.5117 | No | ns | 0.9643 |
| G1 vs. G3b | −0.4567 | −1.092 to 0.2110 | No | ns | 0.3149 |
| G2a vs. G2b | −0.6233 | −1.292 to 0.01230 | No | ns | 0.0782 |
| G2a vs. G2a | 0.1607 | −0.5070 to 0.8283 | No | ns | 0.9603 |
| G2a vs. G3b | −0.14 | −0.8077 to 0.50277 | No | ns | 0.9759 |
| G2b vs. G3a | 0.784 | 0.1163 to 1.452 | Yes | ** | 0.0136 |
| G2b vs. G3b | 0.4833 | −0.1843 to 1.151 | No | ns | 0.2606 |
| G3a vs. G3b | −0.3007 | −0.9683 to 0.3670 | No | ns | 0.7108 |
| Tukey’s Multiple Comparisons Test | Mean Diff. | 95.00% CI of Diff. | Significant | Summary | Adjusted p Value |
|---|---|---|---|---|---|
| G1 vs. G2a | −0.4693 | −1.155 to 0.2161 | No | ns | 0.3180 |
| G1 vs. G2b | −1.018 | −1.703 to −0.3325 | Yes | *** | 0.0008 |
| G1 vs. G3a | −0.2087 | −0.8941 to 0.4768 | No | ns | 0.9130 |
| G1 vs. G3b | −0.7387 | −1.424 to 0.05319 | Yes | * | 0.0284 |
| G2a vs. G2b | −0.5487 | −1.234 to 0.1368 | No | ns | 0.1769 |
| G2a vs. G2a | 0.2607 | −0.4248 to 0.9461 | No | ns | 0.8238 |
| G2a vs. G3b | −0.2693 | −0.9548 to 0.4161 | No | ns | 0.8058 |
| G2b vs. G3a | 0.8093 | 0.239 to 1.495 | Yes | ** | 0.0126 |
| G2b vs. G3b | 0.2793 | −0.4061 to 0.9648 | No | ns | 0.7842 |
| G3a vs. G3b | −0.5300 | −1.215 to 0.155 | No | ns | 0.2052 |
| No Gingiva Augmentation | CMX Before | CTG Before | CMX After | CTG After | |
|---|---|---|---|---|---|
| G1 | G2a | G2b | G3a | G3b | |
| Number of implants | 2 | 0 | 0 | 1 | 1 |
| Percentage of implants | 13% | 0% | 0% | 6.6% | 6.6% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hadzik, J.; Błaszczyszyn, A.; Gedrange, T.; Dominiak, M. Soft-Tissue Augmentation around Dental Implants with a Connective Tissue Graft (CTG) and Xenogeneic Collagen Matrix (CMX)—5-Year Follow-Up. J. Clin. Med. 2023, 12, 924. https://doi.org/10.3390/jcm12030924
Hadzik J, Błaszczyszyn A, Gedrange T, Dominiak M. Soft-Tissue Augmentation around Dental Implants with a Connective Tissue Graft (CTG) and Xenogeneic Collagen Matrix (CMX)—5-Year Follow-Up. Journal of Clinical Medicine. 2023; 12(3):924. https://doi.org/10.3390/jcm12030924
Chicago/Turabian StyleHadzik, Jakub, Artur Błaszczyszyn, Tomasz Gedrange, and Marzena Dominiak. 2023. "Soft-Tissue Augmentation around Dental Implants with a Connective Tissue Graft (CTG) and Xenogeneic Collagen Matrix (CMX)—5-Year Follow-Up" Journal of Clinical Medicine 12, no. 3: 924. https://doi.org/10.3390/jcm12030924