
Stent Thrombosis and Restenosis with Contemporary Drug-Eluting Stents: Predictors and Current Evidence
 , , and
, , and
Abstract
:1. Introduction
2. Evolution of Drug-Eluting Stents
- -
- Stent platform: contemporary DES are made to shorten the time it takes for the stented artery segment to heal, which is what caused first-generation DES to have a higher risk of very late ST than BMS [7,8]. The first-generation DES were built on a platform of stainless steel (iron, nickel, and chromium) with struts that were 130–150 μm thick. Cobalt chromium (CoCr) and platinum chromium (PtCr), two different metallic alloys, were used in newer-generation DES to achieve thinner stent struts (<100 μm), reduce strut-related changes in shear stress, and enable faster and thorough endothelial strut coverage while maintaining an adequate radial strength [9,10,11]. Additionally, the number of connectors and crowns has been shrinking in newer-generation stents, and contemporary DES have 2–3 connectors and 6–7 crowns with improved deliverability, flexibility, and conformability without any trade-off in radial and longitudinal strength [12].
- -
- Polymer coating on the stent surface acts as a drug carrier and enables effective and controlled drug release at the arterial stented site. However, once the anti-proliferative medication has entirely been released, the polymeric material is no longer needed. Over time, the persistence of polymer coating may cause inflammatory responses within the arterial wall, impairing the stented artery’s ability to heal [13]. To overcome these issues, contemporary DES contain more biocompatible durable fluorinated or biodegradable polymers (made of lactic or glycolic acids which fully resorb by hydrolysis after the completion of drug release). A further iteration has been developed with polymer-free DES (PF-DES), which release the anti-proliferative drug directly from the stent surface without the need for a polymeric carrier.
- -
- The anti-proliferative drug released from the polymer or stent surface prevents VSMC proliferation, minimizing the growth of neointimal tissue inside the stent. On first-generation DES platforms, paclitaxel and sirolimus were introduced. By binding to the tubulin component of microtubules, paclitaxel suppresses their detachment from centrosomes, blocking the cell cycle. Sirolimus instead inhibits the mammalian target of rapamycin (mTOR), which prevents the advancement of the cell cycle, cell migration, and protein synthesis. It has repeatedly been demonstrated that sirolimus-eluting DES have a stronger anti-restenotic efficacy than paclitaxel-eluting DES [14]. This might be because sirolimus has a larger therapeutic index and distinct tissue kinetics than other drugs. Accordingly, the -limus family of drugs (which differ from each other in structure, molecular weight, potency, and lipophilicity) are used in newer-generation DES.
2.1. Durable-Polymer Drug-Eluting Stents
2.2. Biodegradable Polymer Drug-Eluting Stents
2.3. Polymer-Free Drug-Eluting Stents
3. Bioresorbable Scaffolds
4. Risk Factors of Stent Thrombosis and In-Stent Restenosis with Contemporary DES
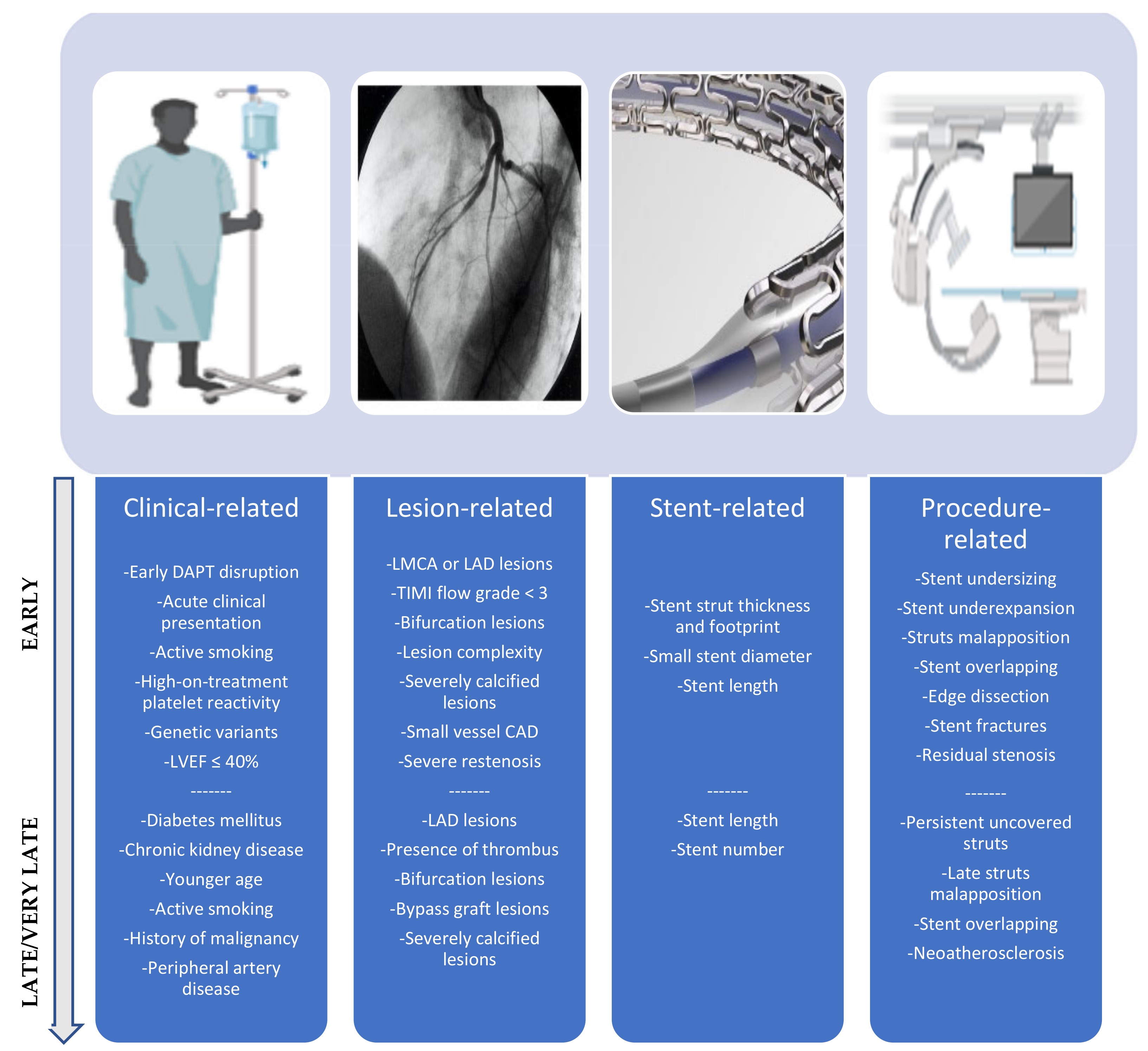
4.1. Stent Thrombosis
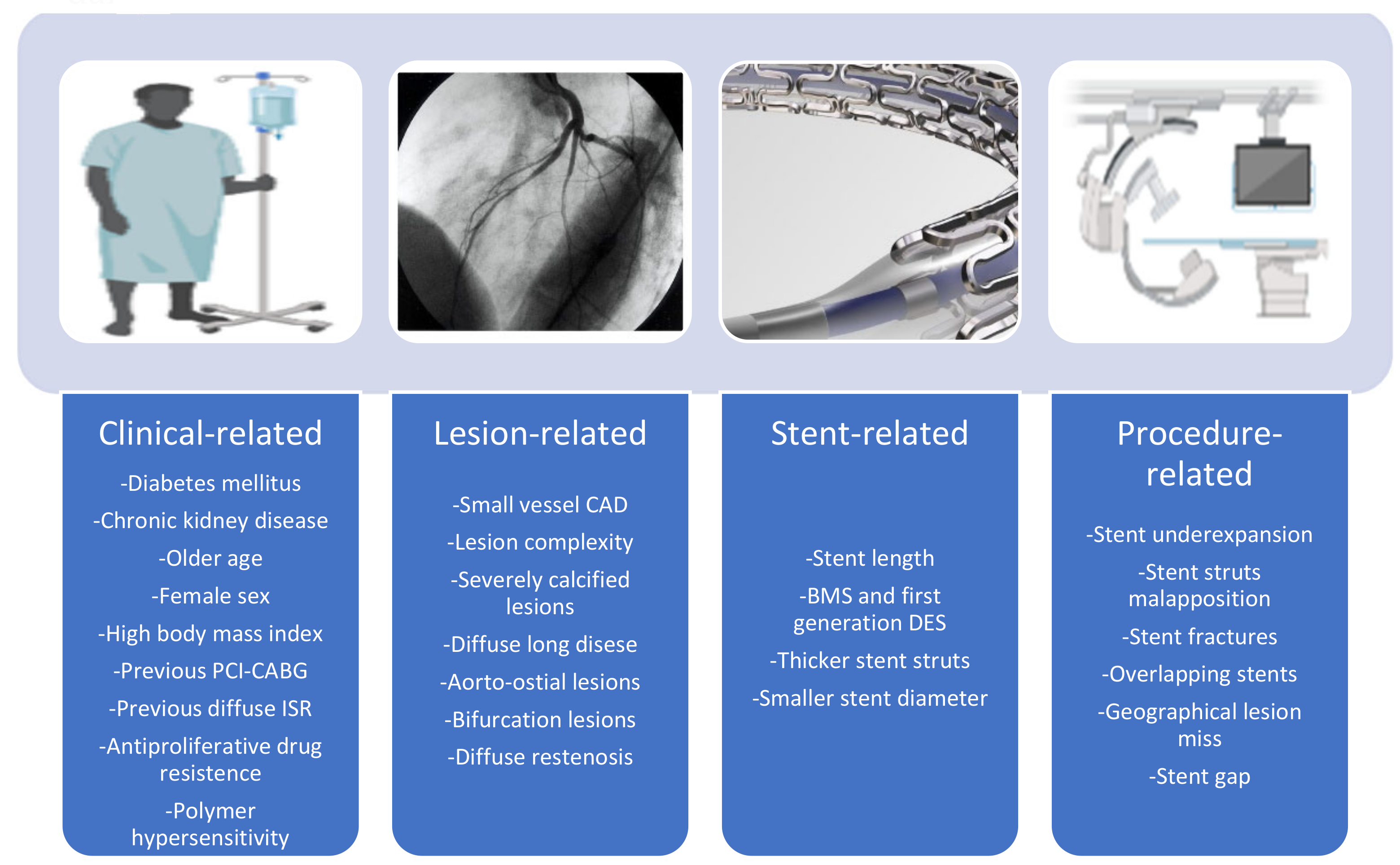
4.2. In-Stent Restenosis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Morice, M.C.; Serruys, P.W.; Sousa, J.E.; Fajadet, J.; Ban Hayashi, E.; Perin, M.; Colombo, A.; Schuler, G.; Barragan, P.; Guagliumi, G.; et al. Randomized Study with the Sirolimus-Coated Bx Velocity Balloon-Expandable Stent in the Treatment of Patients with de Novo Native Coronary Artery Lesions. A randomized comparison of a sirolimus-eluting stent with a standard stent for coronary revascularization. N. Engl. J. Med. 2002, 346, 1773–1780. [Google Scholar] [CrossRef]
- Moses, J.W.; Leon, M.B.; Popma, J.J.; Fitzgerald, P.J.; Holmes, D.R.; O’Shaughnessy, C.; Caputo, R.P.; Kereiakes, D.J.; Williams, D.O.; Teirstein, P.S.; et al. Sirolimus-eluting stents versus standard stents in patients with stenosis in a native coronary artery. N. Engl. J. Med. 2003, 349, 1315–1323. [Google Scholar] [CrossRef]
- Stone, G.W.; Ellis, S.G.; Cox, D.A.; Hermiller, J.; O’Shaughnessy, C.; Mann, J.T.; Turco, M.; Caputo, R.; Bergin, P.; Greenberg, J.; et al. A polymer-based, paclitaxel-eluting stent in patients with coronary artery disease. N. Engl. J. Med. 2004, 350, 221–231. [Google Scholar] [CrossRef]
- Stettler, C.; Wandel, S.; Allemann, S.; Kastrati, A.; Morice, M.C.; Schömig, A.; Pfisterer, M.E.; Stone, G.W.; Leon, M.B.; de Lezo, J.S.; et al. Outcomes associated with drug-eluting and bare-metal stents: A collaborative network meta-analysis. Lancet 2007, 370, 937–948. [Google Scholar] [CrossRef]
- Stefanini, G.G.; Byrne, R.A.; Windecker, S.; Kastrati, A. State of the art: Coronary artery stents—Past, present and future. EuroIntervention 2017, 13, 706–716. [Google Scholar] [CrossRef]
- Byrne, R.A.; Stone, G.W.; Ormiston, J.; Kastrati, A. Coronary balloon angioplasty, stents, and scaffolds. Lancet 2017, 390, 781–792. [Google Scholar] [CrossRef]
- Camenzind, E.; Steg, P.G.; Wijns, W. Stent thrombosis late after implantation of first-generation drug-eluting stents: A cause for concern. Circulation 2007, 115, 1440–1455. [Google Scholar] [CrossRef]
- Nordmann, A.J.; Briel, M.; Bucher, H.C. Mortality in randomized controlled trials comparing drug-eluting vs. bare metal stents in coronary artery disease: A meta-analysis. Eur. Heart J. 2006, 27, 2784–2814. [Google Scholar] [CrossRef]
- Kastrati, A.; Mehilli, J.; Dirschinger, J.; Dotzer, F.; Schühlen, H.; Neumann, F.J.; Fleckenstein, M.; Pfafferott, C.; Seyfarth, M.; Schömig, A. Intracoronary stenting and angiographic results: Strut thickness effect on restenosis outcome (ISAR-STEREO) trial. Circulation 2001, 103, 2816–2821. [Google Scholar] [CrossRef]
- Stone, G.W.; Rizvi, A.; Newman, W.; Mastali, K.; Wang, J.C.; Caputo, R.; Doostzadeh, J.; Cao, S.; Simonton, C.A.; Sudhir, K.; et al. Everolimus-eluting versus paclitaxel-eluting stents in coronary artery disease. N. Engl. J. Med. 2010, 362, 1663–1674. [Google Scholar] [CrossRef]
- Madhavan, M.V.; Howard, J.P.; Naqvi, A.; Ben-Yehuda, O.; Redfors, B.; Prasad, M.; Shahim, B.; Leon, M.B.; Bangalore, S.; Stone, G.W.; et al. Long-term follow-up after ultrathin vs. conventional 2nd-generation drug-eluting stents: A systematic review and meta-analysis of randomized controlled trials. Eur. Heart J. 2021, 42, 2643–2654. [Google Scholar] [CrossRef]
- Iannaccone, M.; Gatti, P.; Barbero, U.; Bassignana, A.; Gallo, D.; de Benedictis, M.; Helft, G.; Morbiducci, U.; Doronzo, B.; D’Ascenzo, F. Impact of strut thickness and number of crown and connectors on clinical outcomes on patients treated with second-generation drug eluting stent. Catheter. Cardiovasc. Interv. 2020, 96, 1417–1422. [Google Scholar] [CrossRef]
- Joner, M.; Finn, A.V.; Farb, A.; Mont, E.K.; Kolodgie, F.D.; Ladich, E.; Kutys, R.; Skorija, K.; Gold, H.K.; Virmani, R. Pathology of drug-eluting stents in humans: Delayed healing and late thrombotic risk. J. Am. Coll. Cardiol. 2006, 48, 193–202. [Google Scholar] [CrossRef]
- Morice, M.C.; Colombo, A.; Meier, B.; Serruys, P.; Tamburino, C.; Guagliumi, G.; Sousa, E.; Stoll, H.P.; REALITY Trial Investigators. Sirolimus- vs. paclitaxel-eluting stents in de novo coronary artery lesions: The REALITY trial: A randomized controlled trial. JAMA 2006, 295, 895–904. [Google Scholar] [CrossRef]
- Kandzari, D.E.; Mauri, L.; Popma, J.J.; Turco, M.A.; Gurbel, P.A.; Fitzgerald, P.J.; Leon, M.B. Late-term clinical outcomes with zotarolimus- and sirolimus-eluting stents. 5-year follow-up of the ENDEAVOR III (A Randomized Controlled Trial of the Medtronic Endeavor Drug [ABT-578] Eluting Coronary Stent System Versus the Cypher Sirolimus-Eluting Coronary Stent System in De Novo Native Coronary Artery Lesions). JACC Cardiovasc. Interv. 2011, 4, 543–550. [Google Scholar] [CrossRef]
- Kelly, C.R.; Teirstein, P.S.; Meredith, I.T.; Farah, B.; Dubois, C.L.; Feldman, R.L.; Dens, J.; Hagiwara, N.; Rabinowitz, A.; Carrié, D.; et al. Long-Term Safety and Efficacy of Platinum Chromium Everolimus-Eluting Stents in Coronary Artery Disease: 5-Year Results from the PLATINUM Trial. JACC Cardiovasc. Interv. 2017, 10, 2392–2400. [Google Scholar] [CrossRef]
- Hassan, S.; Ali, M.N.; Ghafoor, B. Evolutionary perspective of drug eluting stents: From thick polymer to polymer free approach. J. Cardiothorac Surg. 2022, 17, 65. [Google Scholar] [CrossRef]
- Kommineni, N.; Saka, R.; Khan, W.; Domb, A.J. Non-polymer drug-eluting coronary stents. Drug Deliv. Transl. Res. 2018, 8, 903–917. [Google Scholar] [CrossRef]
- Testa, L.; Latib, A.; Montone, R.A.; Colombo, A.; Bedogni, F. Coronary Bioresorbable Vascular Scaffold Use in the Treatment of Coronary Artery Disease. Circ. Cardiovasc. Interv. 2016, 9, e003978; Erratum in Circ. Cardiovasc. Interv. 2016, 9, e000018. [Google Scholar] [CrossRef]
- Polimeni, A.; Anadol, R.; Münzel, T.; Indolfi, C.; De Rosa, S.; Gori, T. Long-term outcome of bioresorbable vascular scaffolds for the treatment of coronary artery disease: A meta-analysis of RCTs. BMC Cardiovasc. Disord. 2017, 17, 147. [Google Scholar] [CrossRef] [Green Version]
- Polimeni, A.; Anadol, R.; Münzel, T.; Geyer, M.; De Rosa, S.; Indolfi, C.; Gori, T. Bioresorbable vascular scaffolds for percutaneous treatment of chronic total coronary occlusions: A meta-analysis. BMC Cardiovasc. Disord. 2019, 19, 59. [Google Scholar] [CrossRef]
- Polimeni, A.; Weissner, M.; Schochlow, K.; Ullrich, H.; Indolfi, C.; Dijkstra, J.; Anadol, R.; Münzel, T.; Gori, T. Incidence, Clinical Presentation, and Predictors of Clinical Restenosis in Coronary Bioresorbable Scaffolds. JACC Cardiovasc. Interv. 2017, 10, 1819–1827. [Google Scholar] [CrossRef]
- Dimitriadis, Z.; Polimeni, A.; Anadol, R.; Geyer, M.; Weissner, M.; Ullrich, H.; Münzel, T.; Gori, T. Procedural Predictors for Bioresorbable Vascular Scaffold Thrombosis: Analysis of the Individual Components of the “PSP” Technique. J. Clin. Med. 2019, 8, 93. [Google Scholar] [CrossRef]
- Gori, T.; Weissner, M.; Gönner, S.; Wendling, F.; Ullrich, H.; Ellis, S.; Anadol, R.; Polimeni, A.; Münzel, T. Characteristics, Predictors, and Mechanisms of Thrombosis in Coronary Bioresorbable Scaffolds: Differences Between Early and Late Events. JACC Cardiovasc. Interv. 2017, 10, 2363–2371. [Google Scholar] [CrossRef]
- Anadol, R.; Lorenz, L.; Weissner, M.; Ullrich, H.; Polimeni, A.; Münzel, T.; Gori, T. Characteristics and outcome of patients with complex coronary lesions treated with bioresorbable scaffolds: Three-year follow-up in a cohort of consecutive patients. EuroIntervention 2018, 14, e1011–e1019. [Google Scholar] [CrossRef]
- Stefanini, G.G.; Alfonso, F.; Barbato, E.; Byrne, R.A.; Capodanno, D.; Colleran, R.; Escaned, J.; Giacoppo, D.; Kunadian, V.; Lansky, A.; et al. Management of myocardial revascularisation failure: An expert consensus document of the EAPCI. EuroIntervention 2020, 16, e875–e890. [Google Scholar] [CrossRef]
- Giustino, G.; Colombo, A.; Camaj, A.; Yasumura, K.; Mehran, R.; Stone, G.W.; Kini, A.; Sharma, S.K. Coronary In-Stent Restenosis: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2022, 80, 348–372. [Google Scholar] [CrossRef]
- Polimeni, A.; Sorrentino, S.; Spaccarotella, C.; Mongiardo, A.; Sabatino, J.; De Rosa, S.; Gori, T.; Indolfi, C. Stent Thrombosis After Percutaneous Coronary Intervention: From Bare-Metal to the Last Generation of Drug-Eluting Stents. Interv. Cardiol. Clin. 2022, 11, 465–473. [Google Scholar] [CrossRef]
- Nicolas, J.; Pivato, C.A.; Chiarito, M.; Beerkens, F.; Cao, D.; Mehran, R. Evolution of drug-eluting coronary stents: A back-and-forth journey from the bench-to-bedside. Cardiovasc. Res. 2022, 118, cvac105. [Google Scholar] [CrossRef]
- Polimeni, A.; Sorrentino, S.; Spaccarotella, C.; Mongiardo, A.; Sabatino, J.; De Rosa, S.; Gori, T.; Indolfi, C. Stent Thrombosis After Percutaneous Coronary Intervention: From Bare-Metal to the Last Generation of Drug-Eluting Stents. Cardiol. Clin. 2020, 38, 639–647. [Google Scholar] [CrossRef]
- Condello, F.; Sturla, M.; Terzi, R.; Polimeni, A.; Stefanini, G.G. Walking the Line with Ticagrelor: Meta-Analysis Comparing the Safety and Efficacy of Ticagrelor Monotherapy after a Short Course of Ticagrelor-Based Dual Antiplatelet Therapy versus Standard Therapy in Complex Percutaneous Coronary Intervention. J. Clin. Med. 2021, 10, 5506. [Google Scholar] [CrossRef]
- Sorrentino, S.; Salerno, N.; Leo, I.; Polimeni, A.; Sabatino, J.; Spaccarotella, C.A.M.; Mongiardo, A.; De Rosa, S.; Indolfi, C. New Antithrombotic Strategies and Coronary Stent Technologies for Patients at High Bleeding Risk Undergoing Percutaneous Coronary Intervention. Curr. Vasc. Pharmacol. 2022, 20, 37–45. [Google Scholar] [CrossRef]
- Cutlip, D.E.; Windecker, S.; Mehran, R.; Boam, A.; Cohen, D.J.; van Es, G.A.; Steg, P.G.; Morel, M.A.; Mauri, L.; Vranckx, P.; et al. Clinical end points in coronary stent trials: A case for standardized definitions. Circulation 2007, 115, 2344–2351. [Google Scholar] [CrossRef]
- Yang, Y.X.; Liu, Y.; Li, X.W.; Lu, P.J.; Wang, J.; Li, C.P.; Gao, J. Clinical outcomes after percutaneous coronary intervention for early versus late and very late stent thrombosis: A systematic review and meta-analysis. J. Thromb. Thrombolysis 2021, 51, 682–692. [Google Scholar] [CrossRef]
- Gori, T.; Polimeni, A.; Indolfi, C.; Räber, L.; Adriaenssens, T.; Münzel, T. Predictors of stent thrombosis and their implications for clinical practice. Nat. Rev. Cardiol. 2019, 16, 243–256. [Google Scholar] [CrossRef]
- Park, K.W.; Hwang, S.J.; Kwon, D.A.; Oh, B.H.; Park, Y.B.; Chae, I.H.; Gwon, H.C.; Park, S.J.; Seung, K.B.; Ahn, T.; et al. Characteristics and predictors of drug-eluting stent thrombosis: Results from the multicenter ‘Korea Stent Thrombosis (KoST)’ registry. Circ. J. 2011, 75, 1626–1632. [Google Scholar] [CrossRef]
- Généreux, P.; Rutledge, D.R.; Palmerini, T.; Caixeta, A.; Kedhi, E.; Hermiller, J.B.; Wang, J.; Krucoff, M.W.; Jones-McMeans, J.; Sudhir, K.; et al. Stent Thrombosis and Dual Antiplatelet Therapy Interruption with Everolimus-Eluting Stents: Insights From the Xience V Coronary Stent System Trials. Circ. Cardiovasc. Interv. 2015, 8, e001362. [Google Scholar] [CrossRef]
- van Werkum, J.W.; Heestermans, A.A.; Zomer, A.C.; Kelder, J.C.; Suttorp, M.J.; Rensing, B.J.; Koolen, J.J.; Brueren, B.R.; Dambrink, J.H.; Hautvast, R.W.; et al. Predictors of coronary stent thrombosis: The Dutch Stent Thrombosis Registry. J. Am. Coll. Cardiol. 2009, 53, 1399–1409. [Google Scholar] [CrossRef]
- Geisler, T.; Zürn, C.; Simonenko, R.; Rapin, M.; Kraibooj, H.; Kilias, A.; Bigalke, B.; Stellos, K.; Schwab, M.; May, A.E.; et al. Early but not late stent thrombosis is influenced by residual platelet aggregation in patients undergoing coronary interventions. Eur. Heart J. 2010, 31, 59–66. [Google Scholar] [CrossRef]
- Waksman, R.; Kirtane, A.J.; Torguson, R.; Cohen, D.J.; Ryan, T.; Räber, L.; Applegate, R.; Waxman, S.; Gordon, P.; Kaneshige, K.; et al. Correlates and outcomes of late and very late drug-eluting stent thrombosis: Results from DESERT (International Drug-Eluting Stent Event Registry of Thrombosis). JACC Cardiovasc. Interv. 2014, 7, 1093–1102. [Google Scholar] [CrossRef] [Green Version]
- Kuramitsu, S.; Ohya, M.; Shinozaki, T.; Otake, H.; Horie, K.; Kawamoto, H.; Yamanaka, F.; Natsuaki, M.; Shiomi, H.; Nakazawa, G.; et al. Risk Factors and Long-Term Clinical Outcomes of Second-Generation Drug-Eluting Stent Thrombosis. Circ. Cardiovasc. Interv. 2019, 12, e007822. [Google Scholar] [CrossRef]
- Harmsze, A.M.; van Werkum, J.W.; Ten Berg, J.M.; Zwart, B.; Bouman, H.J.; Breet, N.J.; van ‘t Hof, A.W.; Ruven, H.J.; Hackeng, C.M.; Klungel, O.H.; et al. CYP2C19*2 and CYP2C9*3 alleles are associated with stent thrombosis: A case-control study. Eur. Heart J. 2010, 31, 3046–3053. [Google Scholar] [CrossRef]
- Park, K.W.; Park, J.J.; Kang, J.; Jeon, K.H.; Kang, S.H.; Han, J.K.; Lee, S.E.; Yang, H.M.; Lee, H.Y.; Kang, H.J.; et al. Paraoxonase 1 gene polymorphism does not affect clopidogrel response variability but is associated with clinical outcome after PCI. PLoS ONE 2013, 8, e52779. [Google Scholar] [CrossRef]
- Nakatani, S.; Nishino, M.; Taniike, M.; Makino, N.; Kato, H.; Egami, Y.; Shutta, R.; Tanouchi, J.; Yamada, Y. Initial findings of impact of strut width on stent coverage and apposition of sirolimus-eluting stents assessed by optical coherence tomography. Catheter Cardiovasc. Interv. 2013, 81, 776–781. [Google Scholar] [CrossRef]
- Grundeken, M.J.; Beijk, M.A. A Narrative Review of Ultrathin-strut Drug-eluting Stents: The Thinner the Better? Heart Int. 2021, 15, 84–93. [Google Scholar] [CrossRef]
- Taglieri, N.; Bruno, A.G.; Ghetti, G.; Marrozzini, C.; Saia, F.; Galié, N.; Palmerini, T. Target Lesion Failure with Current Drug-Eluting Stents: Evidence from a Comprehensive Network Meta-Analysis. JACC Cardiovasc. Interv. 2020, 13, 2868–2878. [Google Scholar] [CrossRef]
- Lou, Y.; Yu, Y.; Xi, Z.; Gao, Y.; Liu, W.; Nie, X. Five-Year Outcomes of Biodegradable Polymer Drug-Eluting Stents Versus Second-Generation Durable Polymer Drug-Eluting Stents: A Meta-Analysis of Randomized Controlled Trials. Cardiovasc. Drugs Ther. 2019, 33, 557–566. [Google Scholar] [CrossRef]
- Adriaenssens, T.; Ughi, G.J.; Dubois, C.; De Cock, D.; Onsea, K.; Bennett, J.; Wiyono, S.; Sinnaeve, P.; Coosemans, M.; Ferdinande, B.; et al. STACCATO (Assessment of Stent sTrut Apposition and Coverage in Coronary ArTeries with Optical coherence tomography in patients with STEMI, NSTEMI and stable/unstable angina undergoing everolimus vs. biolimus A9-eluting stent implantation): A randomised controlled trial. EuroIntervention 2016, 11, e1619–e1626. [Google Scholar] [CrossRef]
- Barlis, P.; Regar, E.; Serruys, P.W.; Dimopoulos, K.; van der Giessen, W.J.; van Geuns, R.J.; Ferrante, G.; Wandel, S.; Windecker, S.; van Es, G.A.; et al. An optical coherence tomography study of a biodegradable vs. durable polymer-coated limus-eluting stent: A LEADERS trial sub-study. Eur. Heart J. 2010, 31, 165–176. [Google Scholar] [CrossRef]
- Otaegui Irurueta, I.; González Sucarrats, S.; Barrón Molina, J.L.; Pérez de Prado, A.; Massotti, M.; Carmona Ramírez, M.Á.; Martí, G.; Bellera, N.; Serra, B.; Serra, V.; et al. Can an ultrathin strut stent design and a polymer free, proendothelializing probucol matrix coating improve early strut healing? The FRIENDLY-OCT trial. An intra-patient randomized study with OCT, evaluating early strut coverage of a novel probucol coated polymer-free and ultra-thin strut sirolimus-eluting stent compared to a biodegradable polymer sirolimus-eluting stent. Int. J. Cardiol. 2022, 360, 13–20. [Google Scholar] [CrossRef]
- He, Y.; Wang, R.; Liu, J.; Li, F.; Li, J.; Li, C.; Zhou, J.; Zhao, Z.; Yang, W.; Mou, F.; et al. A Randomized Comparison of the Healing Response Between the Firehawk Stent and the Xience Stent in Patients with ST-Segment Elevation Myocardial Infarction at 6 Months of Follow-Up (TARGET STEMI OCT China Trial): An Optical Coherence Tomography Study. Front. Cardiovasc. Med. 2022, 9, 895167. [Google Scholar] [CrossRef]
- Saito, A.; Dai, Z.; Ono, M.; Kanie, T.; Takaoka, Y.; Mizuno, A.; Komiyama, N.; Asano, T. The relationship between coronary stent strut thickness and the incidences of clinical outcomes after drug-eluting stent implantation: A systematic review and meta-regression analysis. Catheter Cardiovasc. Interv. 2022, 99, 575–582. [Google Scholar] [CrossRef]
- Souteyrand, G.; Amabile, N.; Mangin, L.; Chabin, X.; Meneveau, N.; Cayla, G.; Vanzetto, G.; Barnay, P.; Trouillet, C.; Rioufol, G.; et al. Mechanisms of stent thrombosis analysed by optical coherence tomography: Insights from the national PESTO French registry. Eur. Heart J. 2016, 37, 1208–1216. [Google Scholar] [CrossRef]
- Adriaenssens, T.; Joner, M.; Godschalk, T.C.; Malik, N.; Alfonso, F.; Xhepa, E.; De Cock, D.; Komukai, K.; Tada, T.; Cuesta, J.; et al. Optical Coherence Tomography Findings in Patients with Coronary Stent Thrombosis: A Report of the PRESTIGE Consortium (Prevention of Late Stent Thrombosis by an Interdisciplinary Global European Effort). Circulation 2017, 136, 1007–1021. [Google Scholar] [CrossRef]
- Taniwaki, M.; Radu, M.D.; Zaugg, S.; Amabile, N.; Garcia-Garcia, H.M.; Yamaji, K.; Jørgensen, E.; Kelbæk, H.; Pilgrim, T.; Caussin, C.; et al. Mechanisms of Very Late Drug-Eluting Stent Thrombosis Assessed by Optical Coherence Tomography. Circulation 2016, 133, 650–660. [Google Scholar] [CrossRef]
- Kitahara, H.; Okada, K.; Kimura, T.; Yock, P.G.; Lansky, A.J.; Popma, J.J.; Yeung, A.C.; Fitzgerald, P.J.; Honda, Y. Impact of Stent Size Selection on Acute and Long-Term Outcomes After Drug-Eluting Stent Implantation in De Novo Coronary Lesions. Circ. Cardiovasc. Interv. 2017, 10, e004795. [Google Scholar] [CrossRef]
- Räber, L.; Mintz, G.S.; Koskinas, K.C.; Johnson, T.W.; Holm, N.R.; Onuma, Y.; Radu, M.D.; Joner, M.; Yu, B.; Jia, H.; et al. Part 1: Guidance and optimization of coronary interventions. An expert consensus document of the European Association of Percutaneous Cardiovascular Interventions. Eur. Heart J. 2018, 39, 3281–3300. [Google Scholar] [CrossRef]
- Won, H.; Shin, D.H.; Kim, B.K.; Mintz, G.S.; Kim, J.S.; Ko, Y.G.; Choi, D.; Jang, Y.; Hong, M.K. Optical coherence tomography derived cut-off value of uncovered stent struts to predict adverse clinical outcomes after drug-eluting stent implantation. Int. J. Cardiovasc. Imaging 2013, 29, 1255–1263. [Google Scholar] [CrossRef]
- Jinnouchi, H.; Sakakura, K.; Yanase, T.; Ugata, Y.; Tsukui, T.; Taniguchi, Y.; Yamamoto, K.; Seguchi, M.; Wada, H.; Fujita, H. Impact of stent edge dissection detected by optical coherence tomography after current-generation drug-eluting stent implantation. PLoS ONE 2021, 16, e0259693. [Google Scholar] [CrossRef]
- Prati, F.; Romagnoli, E.; Burzotta, F.; Limbruno, U.; Gatto, L.; La Manna, A.; Versaci, F.; Marco, V.; Di Vito, L.; Imola, F.; et al. Clinical Impact of OCT Findings During PCI: The CLI-OPCI II Study. JACC Cardiovasc. Imaging 2015, 8, 1297–1305. [Google Scholar] [CrossRef] [Green Version]
- Choi, S.Y.; Witzenbichler, B.; Maehara, A.; Lansky, A.J.; Guagliumi, G.; Brodie, B.; Kellett, M.A., Jr.; Dressler, O.; Parise, H.; Mehran, R.; et al. Intravascular ultrasound findings of early stent thrombosis after primary percutaneous intervention in acute myocardial infarction: A Harmonizing Outcomes with Revascularization and Stents in Acute Myocardial Infarction (HORIZONS-AMI) substudy. Circ. Cardiovasc. Interv. 2011, 4, 239–247. [Google Scholar] [CrossRef]
- Gao, L.; Lee, S.; Kim, C.J.; Minami, Y.; Ong, D.S.; Soeda, T.; Lowe, H.; Choi, S.Y.; Lerman, A.; Lee, J.; et al. Incidence and Morphological Predictors of Intrastent Coronary Thrombus After Drug-Eluting Stent Implantation (from a Multicenter Registry). Am. J. Cardiol. 2016, 117, 369–375. [Google Scholar] [CrossRef]
- Hong, Y.J.; Jeong, M.H.; Choi, Y.H.; Song, J.A.; Kim, D.H.; Lee, K.H.; Yamanaka, F.; Lee, M.G.; Park, K.H.; Sim, D.S.; et al. Impact of tissue prolapse after stent implantation on short- and long-term clinical outcomes in patients with acute myocardial infarction: An intravascular ultrasound analysis. Int. J. Cardiol. 2013, 166, 646–651. [Google Scholar] [CrossRef]
- Kan, J.; Ge, Z.; Zhang, J.J.; Liu, Z.Z.; Tian, N.L.; Ye, F.; Li, S.J.; Qian, X.S.; Yang, S.; Chen, M.X.; et al. Incidence and Clinical Outcomes of Stent Fractures on the Basis of 6555 Patients and 16,482 Drug-Eluting Stents From 4 Centers. JACC Cardiovasc. Interv. 2016, 9, 1115–1123. [Google Scholar] [CrossRef]
- Gori, T.; Polimeni, A.; Indolfi, C.; Räber, L.; Adriaenssens, T.; Münzel, T. Reply to ‘Relationship between stent fracture and thrombosis’. Nat. Rev. Cardiol. 2020, 17, 64–65. [Google Scholar] [CrossRef]
- Otsuka, F.; Byrne, R.A.; Yahagi, K.; Mori, H.; Ladich, E.; Fowler, D.R.; Kutys, R.; Xhepa, E.; Kastrati, A.; Virmani, R.; et al. Neoatherosclerosis: Overview of histopathologic findings and implications for intravascular imaging assessment. Eur. Heart J. 2015, 36, 2147–2159. [Google Scholar] [CrossRef]
- Madhavan, M.V.; Kirtane, A.J.; Redfors, B.; Généreux, P.; Ben-Yehuda, O.; Palmerini, T.; Benedetto, U.; Biondi-Zoccai, G.; Smits, P.C.; von Birgelen, C.; et al. Stent-Related Adverse Events >1 Year After Percutaneous Coronary Intervention. J. Am. Coll. Cardiol. 2020, 75, 590–604. [Google Scholar] [CrossRef]
- Alfonso, F.; Coughlan, J.J.; Giacoppo, D.; Kastrati, A.; Byrne, R.A. Management of in-stent restenosis. EuroIntervention 2022, 18, e103–e123. [Google Scholar] [CrossRef]
- Moussa, I.D.; Mohananey, D.; Saucedo, J.; Stone, G.W.; Yeh, R.W.; Kennedy, K.F.; Waksman, R.; Teirstein, P.; Moses, J.W.; Simonton, C. Trends and Outcomes of Restenosis After Coronary Stent Implantation in the United States. J. Am. Coll. Cardiol. 2020, 76, 1521–1531. [Google Scholar] [CrossRef]
- Kastrati, A.; Cassese, S. In-Stent Restenosis in the United States: Time to Enrich its Treatment Armamentarium. J. Am. Coll. Cardiol. 2020, 76, 1532–1535. [Google Scholar] [CrossRef]
- Cassese, S.; Byrne, R.A.; Tada, T.; Pinieck, S.; Joner, M.; Ibrahim, T.; King, L.A.; Fusaro, M.; Laugwitz, K.L.; Kastrati, A. Incidence and predictors of restenosis after coronary stenting in 10,004 patients with surveillance angiography. Heart 2014, 100, 153–159. [Google Scholar] [CrossRef]
- Tamez, H.; Secemsky, E.A.; Valsdottir, L.R.; Moussa, I.D.; Song, Y.; Simonton, C.A.; Gibson, C.M.; Popma, J.J.; Yeh, R.W. Long-term outcomes of percutaneous coronary intervention for in-stent restenosis among Medicare beneficiaries. EuroIntervention 2021, 17, e380–e387. [Google Scholar] [CrossRef]
- Buchanan, K.D.; Torguson, R.; Rogers, T.; Xu, L.; Gai, J.; Ben-Dor, I.; Suddath, W.O.; Satler, L.F.; Waksman, R. In-Stent Restenosis of Drug-Eluting Stents Compared with a Matched Group of Patients with De Novo Coronary Artery Stenosis. Am. J. Cardiol. 2018, 121, 1512–1518. [Google Scholar] [CrossRef]
- Wang, H.; Wang, Q.; Hu, J.; Zhang, R.; Gao, T.; Rong, S.; Dong, H. Global research trends in in-stent neoatherosclerosis: A CiteSpace-based visual analysis. Front. Cardiovasc. Med. 2022, 9, 1025858. [Google Scholar] [CrossRef]
- Indolfi, C.; Iaconetti, C.; Gareri, C.; Polimeni, A.; De Rosa, S. Non-coding RNAs in vascular remodeling and restenosis. Vasc. Pharmacol. 2019, 114, 49–63. [Google Scholar] [CrossRef]
- Iaconetti, C.; Polimeni, A.; Sorrentino, S.; Sabatino, J.; Pironti, G.; Esposito, G.; Curcio, A.; Indolfi, C. Inhibition of miR-92a increases endothelial proliferation and migration in vitro as well as reduces neointimal proliferation in vivo after vascular injury. Basic Res. Cardiol. 2012, 107, 296. [Google Scholar] [CrossRef]
- Iaconetti, C.; De Rosa, S.; Polimeni, A.; Sorrentino, S.; Gareri, C.; Carino, A.; Sabatino, J.; Colangelo, M.; Curcio, A.; Indolfi, C. Down-regulation of miR-23b induces phenotypic switching of vascular smooth muscle cells in vitro and in vivo. Cardiovasc. Res. 2015, 107, 522–533. [Google Scholar] [CrossRef]
- Nakano, M.; Otsuka, F.; Yahagi, K.; Sakakura, K.; Kutys, R.; Ladich, E.R.; Finn, A.V.; Kolodgie, F.D.; Virmani, R. Human autopsy study of drug-eluting stents restenosis: Histomorphological predictors and neointimal characteristics. Eur. Heart J. 2013, 34, 3304–3313. [Google Scholar] [CrossRef]
- Chieffo, A.; Foglieni, C.; Nodari, R.L.; Briguori, C.; Sangiorgi, G.; Latib, A.; Montorfano, M.; Airoldi, F.; Michev, I.; Carlino, M.; et al. Histopathology of clinical coronary restenosis in drug-eluting versus bare metal stents. Am. J. Cardiol. 2009, 104, 1660–1667. [Google Scholar] [CrossRef]
- Ali, Z.A.; Roleder, T.; Narula, J.; Mohanty, B.D.; Baber, U.; Kovacic, J.C.; Mintz, G.S.; Otsuka, F.; Pan, S.; Virmani, R.; et al. Increased thin-cap neoatheroma and periprocedural myocardial infarction in drug-eluting stent restenosis: Multimodality intravascular imaging of drug-eluting and bare-metal stents. Circ. Cardiovasc. Interv. 2013, 6, 507–517. [Google Scholar] [CrossRef] [Green Version]
- Song, L.; Mintz, G.S.; Yin, D.; Yamamoto, M.H.; Chin, C.Y.; Matsumura, M.; Kirtane, A.J.; Parikh, M.A.; Moses, J.W.; Ali, Z.A.; et al. Characteristics of early versus late in-stent restenosis in second-generation drug-eluting stents: An optical coherence tomography study. EuroIntervention 2017, 13, 294–302. [Google Scholar] [CrossRef]
- Chen, Z.; Matsumura, M.; Mintz, G.S.; Noguchi, M.; Fujimura, T.; Usui, E.; Seike, F.; Hu, X.; Jin, G.; Li, C.; et al. Prevalence and Impact of Neoatherosclerosis on Clinical Outcomes After Percutaneous Treatment of Second-Generation Drug-Eluting Stent Restenosis. Circ. Cardiovasc. Interv. 2022, 15, e011693. [Google Scholar] [CrossRef]
- Hu, W.; Jiang, J. Hypersensitivity and in-stent restenosis in coronary stent materials. Front. Bioeng. Biotechnol. 2022, 10, 1003322. [Google Scholar] [CrossRef]
- Zeng, M.; Yan, X.; Wu, W. Risk factors for revascularization and in-stent restenosis in patients with triple-vessel disease after second-generation drug-eluting stent implantation: A retrospective analysis. BMC Cardiovasc. Disord. 2021, 21, 446. [Google Scholar] [CrossRef]
- Zheng, C.; Kang, J.; Park, K.W.; Han, J.K.; Yang, H.M.; Kang, H.J.; Koo, B.K.; Kim, H.S. The Predictors of Target Lesion Revascularization and Rate of In-Stent Restenosis in the Second-Generation Drug-Eluting Stent Era. J. Interv. Cardiol. 2019, 2019, 3270132. [Google Scholar] [CrossRef]
- Park, D.W.; Yun, S.C.; Lee, J.Y.; Kim, W.J.; Kang, S.J.; Lee, S.W.; Kim, Y.H.; Lee, C.W.; Kim, J.J.; Park, S.W.; et al. C-reactive protein and the risk of stent thrombosis and cardiovascular events after drug-eluting stent implantation. Circulation 2009, 120, 1987–1995. [Google Scholar] [CrossRef]
- Lightell, D.J., Jr.; Woods, T.C. Relative resistance to Mammalian target of rapamycin inhibition in vascular smooth muscle cells of diabetic donors. Ochsner J. 2013, 13, 56–60. [Google Scholar]
- Khan, A.A.; Dangas, G.D. The quest for a “diabetic” stent. Catheter. Cardiovasc. Interv. 2018, 91, 892–893. [Google Scholar] [CrossRef]
- Romaguera, R.; Salinas, P.; Gomez-Lara, J.; Brugaletta, S.; Gómez-Menchero, A.; Romero, M.A.; García-Blas, S.; Ocaranza, R.; Bordes, P.; Kockar, M.J.; et al. Amphilimus- vs. zotarolimus-eluting stents in patients with diabetes mellitus and coronary artery disease: The SUGAR trial. Eur. Heart J. 2022, 43, 1320–1330. [Google Scholar] [CrossRef]
- Pepe, M.; Napoli, G.; Carulli, E.; Moscarelli, M.; Forleo, C.; Nestola, P.L.; Biondi-Zoccai, G.; Giordano, A.; Favale, S. Autoimmune diseases in patients undergoing percutaneous coronary intervention: A risk factor for in-stent restenosis? Atherosclerosis 2021, 333, 24–31. [Google Scholar] [CrossRef]
- Li, M.; Hou, J.; Gu, X.; Weng, R.; Zhong, Z.; Liu, S. Incidence and risk factors of in-stent restenosis after percutaneous coronary intervention in patients from southern China. Eur. J. Med. Res. 2022, 27, 12. [Google Scholar] [CrossRef]
- Sanz-Sanchez, J.; Chiarito, M.; Gill, G.S.; van der Heijden, L.C.; Pina, Y.; Cortese, B.; Alfonso, F.; von Birgelen, C.; Gil, J.L.D.; Waksman, R.; et al. Small Vessel Coronary Artery Disease: Rationale for Standardized Definition and Critical Appraisal of the Literature. J. Soc. Cardiovasc. Angiogr. Interv. 2022, 1, 100403. [Google Scholar] [CrossRef]
- Buiten, R.A.; Ploumen, E.H.; Zocca, P.; Doggen, C.J.M.; van der Heijden, L.C.; Kok, M.M.; Danse, P.W.; Schotborgh, C.E.; Scholte, M.; de Man, F.H.A.F.; et al. Outcomes in Patients Treated with Thin-Strut, Very Thin-Strut, or Ultrathin-Strut Drug-Eluting Stents in Small Coronary Vessels: A Prespecified Analysis of the Randomized BIO-RESORT Trial. JAMA Cardiol. 2019, 4, 659–669. [Google Scholar] [CrossRef]
- Sanz Sánchez, J.; Chiarito, M.; Cortese, B.; Moretti, A.; Pagnotta, P.; Reimers, B.; Stefanini, G.G.; Ferrante, G. Drug-Coated balloons vs. drug-eluting stents for the treatment of small coronary artery disease: A meta-analysis of randomized trials. Catheter. Cardiovasc. Interv. 2021, 98, 66–75. [Google Scholar] [CrossRef]
- Généreux, P.; Madhavan, M.V.; Mintz, G.S.; Maehara, A.; Palmerini, T.; Lasalle, L.; Xu, K.; McAndrew, T.; Kirtane, A.; Lansky, A.J.; et al. Ischemic outcomes after coronary intervention of calcified vessels in acute coronary syndromes. Pooled analysis from the HORIZONS-AMI (Harmonizing Outcomes with Revascularization and Stents in Acute Myocardial Infarction) and ACUITY (Acute Catheterization and Urgent Intervention Triage Strategy) TRIALS. J. Am. Coll. Cardiol. 2014, 63, 1845–1854. [Google Scholar] [CrossRef]
- Barbato, E.; Shlofmitz, E.; Milkas, A.; Shlofmitz, R.; Azzalini, L.; Colombo, A. State of the art: Evolving concepts in the treatment of heavily calcified and undilatable coronary stenoses—From debulking to plaque modification, a 40-year-long journey. EuroIntervention 2017, 13, 696–705. [Google Scholar] [CrossRef]
- Latib, A.; Mussardo, M.; Ielasi, A.; Tarsia, G.; Godino, C.; Al-Lamee, R.; Chieffo, A.; Airoldi, F.; Carlino, M.; Montorfano, M.; et al. Long-term outcomes after the percutaneous treatment of drug-eluting stent restenosis. JACC Cardiovasc. Interv. 2011, 4, 155–164. [Google Scholar] [CrossRef]
- Albiero, R.; Burzotta, F.; Lassen, J.F.; Lefèvre, T.; Banning, A.P.; Chatzizisis, Y.S.; Johnson, T.W.; Ferenc, M.; Pan, M.; Daremont, O.; et al. Treatment of coronary bifurcation lesions, part I: Implanting the first stent in the provisional pathway. The 16th expert consensus document of the European Bifurcation Club. EuroIntervention 2022, 18, e362–e376. [Google Scholar] [CrossRef]
- Lassen, J.F.; Albiero, R.; Johnson, T.W.; Burzotta, F.; Lefèvre, T.; Iles, T.L.; Pan, M.; Banning, A.P.; Chatzizisis, Y.S.; Ferenc, M.; et al. Treatment of coronary bifurcation lesions, part II: Implanting two stents. The 16th expert consensus document of the European Bifurcation Club. EuroIntervention 2022, 18, 457–470. [Google Scholar] [CrossRef]
- Jaffe, R.; Halon, D.A.; Shiran, A.; Rubinshtein, R. Percutaneous treatment of aorto-ostial coronary lesions: Current challenges and future directions. Int. J. Cardiol. 2015, 186, 61–66. [Google Scholar] [CrossRef]
- Weiss, A.J.; Lorente-Ros, M.; Correa, A.; Barman, N.; Tamis-Holland, J.E. Recent Advances in Stent Technology: Do They Reduce Cardiovascular Events? Curr. Atheroscler. Rep. 2022, 24, 731–744, Erratum in Curr. Atheroscler. Rep. 2022, 24, 745. [Google Scholar] [CrossRef]
- Koppara, T.; Cheng, Q.; Yahagi, K.; Mori, H.; Sanchez, O.D.; Feygin, J.; Wittchow, E.; Kolodgie, F.D.; Virmani, R.; Joner, M. Thrombogenicity and early vascular healing response in metallic biodegradable polymer-based and fully bioabsorbable drug-eluting stents. Circ. Cardiovasc. Interv. 2015, 8, e002427. [Google Scholar] [CrossRef]
- Lupi, A.; Schaffer, A.; Bongo, A.S. Should ultrathin strut drug eluting stents be considered the new benchmark for novel coronary stents approval? The complex interplay between stent strut thickness, polymeric carriers and antiproliferative drugs. J. Thorac. Dis. 2018, 10, 678–681. [Google Scholar] [CrossRef]
- Kong, M.G.; Han, J.K.; Kang, J.H.; Zheng, C.; Yang, H.M.; Park, K.W.; Kang, H.J.; Koo, B.K.; Chae, I.H.; Kim, H.S.; et al. Clinical outcomes of long stenting in the drug-eluting stent era: Patient-level pooled analysis from the GRAND-DES registry. EuroIntervention 2021, 16, 1318–1325. [Google Scholar] [CrossRef]
- Zhang, X.; Yang, L.; Ju, H.; Zhang, F.; Wu, J.; He, B.; Chen, Y. Prevalence and prognosis of coronary stent gap detected by multi-detector CT: A follow-up study. Eur. Radiol. 2012, 22, 1896–1903. [Google Scholar] [CrossRef]
- Shlofmitz, E.; Iantorno, M.; Waksman, R. Restenosis of Drug-Eluting Stents: A New Classification System Based on Disease Mechanism to Guide Treatment and State-of-the-Art Review. Circ. Cardiovasc. Interv. 2019, 12, e007023, Erratum in Circ. Cardiovasc. Interv. 2019, 12, e000044. [Google Scholar] [CrossRef]
- Mehran, R.; Dangas, G.; Abizaid, A.S.; Mintz, G.S.; Lansky, A.J.; Satler, L.F.; Pichard, A.D.; Kent, K.M.; Stone, G.W.; Leon, M.B. Angiographic patterns of in-stent restenosis: Classification and implications for long-term outcome. Circulation 1999, 100, 1872–1878. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Endeavor | Xience | Promus | Resolute | |
|---|---|---|---|---|
| Platform material | CoCr | CoCr | PtCr | CoCr |
| Strut thickness (μm) | 91 | 81 | 81 | 91 |
| Polymer material | MPC/LMA/HPMA/3-MPMA | PBMA/PVDF-HFP | PBMA/PVDF-HFP | PBMA/PHMA/PVP/PVA |
| Coating distribution | Circumferential | Circumferential | Circumferential | Circumferential |
| Polymer thickness (μm) | 4.8 | 8 | 8 | 4.8 |
| Drug released | Zotarolimus | Everolimus | Everolimus | Zotarolimus |
| Synergy | Synergy Megatron | BioMatrix/Nobori | Ultimaster | COMBO | Orsiro | MiStent | BioMime | Supraflex | Yukon Choice PC | Firehawk | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Platform material | PtCr | PtCr | Stainless steel | CoCr | Stainless steel | CoCr | CoCr | CoCr | CoCr | Stainless steel | CoCr |
| Strut thickness (μm) | 74 | 89 | 120 | 80 | 100 | 60 | 64 | 65 | 60 | 87 | 86 |
| Polymer material | PLGA | PLGA | PDLLA | PDLLA-PCL | PDLLA/PLGA | PLLA | PLGA | PLLA/PLGA | PLLA/PLCL/PVP | PDLLA | PDLLA |
| Coating distribution | Abluminal | Abluminal | Abluminal | Abluminal | Abluminal | Circumferential | Circumferential | Circumferential | Circumferential | Abluminal | Abluminal |
| Polymer thickness (μm) | 4 | 10 | 15 | 5 | 7 | 15 | 2 | 4–5 | 5 | 10 | |
| Drug released | Everolimus | Everolimus | Biolimus A9 | Sirolimus | Sirolimus | Sirolimus | Sirolimus | Sirolimus | Sirolimus | Sirolimus | Sirolimus |
| Additional features | Circumferential coating of anti-CD34 antibodies | Silicon carbide additional coating | Microporous PEARL surface for better endothelial cell adhesion |
| BioFreedom Ultra | Cre8 | Coroflex ISAR NEO | |
|---|---|---|---|
| Platform material | CoCr | CoCr | CoCr |
| Strut thickness (μm) | 84 | 70–80 | 55–65 |
| Drug released | Biolimus A9 | Amphilimus | Sirolimus |
| Surface modification technique | Abluminal microporous surface coating | Abluminal Reservoir-based coating | Abluminal microporous surface coating |
| Additional features | BioInducer surface (<0.3 μm) covalently bonded to the CoCr platform to limit risk of allergic reaction and platelet adhesion | Probucol as matrix-builder and is a highly lipophilic, lipid-lowering agent with antioxidant effects |
| Device | Backbone | Coating | Strut Thickness (μm) | Eluted Drug | Bioresorption Time (Months) |
|---|---|---|---|---|---|
| Bioresorbable polymer | |||||
| Absorb BVS | PLLA | PDLLA | 157 | Everolimus | 24–48 |
| DESolve Nx | PLLA | Polylactide-based | 150 | Novolimus | 24 |
| DESolve Cx | PLLA | Polylactide-based | 120 | Novolimus | 24 |
| Fantom | DAT-PC | DAT-PC | 125 | Sirolimus | 36 |
| Bioresorbable metal | |||||
| DREAMS 1G | Magnesium alloy | PLGA | 125 | Paclitaxel | 9–12 |
| Magmaris | Magnesium alloy | PLLA | 150 | Sirolimus | 9–12 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Condello, F.; Spaccarotella, C.; Sorrentino, S.; Indolfi, C.; Stefanini, G.G.; Polimeni, A. Stent Thrombosis and Restenosis with Contemporary Drug-Eluting Stents: Predictors and Current Evidence. J. Clin. Med. 2023, 12, 1238. https://doi.org/10.3390/jcm12031238
Condello F, Spaccarotella C, Sorrentino S, Indolfi C, Stefanini GG, Polimeni A. Stent Thrombosis and Restenosis with Contemporary Drug-Eluting Stents: Predictors and Current Evidence. Journal of Clinical Medicine. 2023; 12(3):1238. https://doi.org/10.3390/jcm12031238
Chicago/Turabian StyleCondello, Francesco, Carmen Spaccarotella, Sabato Sorrentino, Ciro Indolfi, Giulio G. Stefanini, and Alberto Polimeni. 2023. "Stent Thrombosis and Restenosis with Contemporary Drug-Eluting Stents: Predictors and Current Evidence" Journal of Clinical Medicine 12, no. 3: 1238. https://doi.org/10.3390/jcm12031238